
Abstract
Introduction
Various conditions—including infections, cancers, and trauma—can affect the oral cavity and neck. Contrast-enhanced CT plays an important role in diagnosing, staging, determining treatment efficacy, and conducting treatment follow-up in such conditions.1–3 However, many patients have metallic dental fillings or implants (hereinafter, called dental metals) that cause photon starvation in CT image acquisition. The resulting artifacts on CT images degrade image quality and make evaluation of neck diseases difficult. 4
Several techniques to reduce metal artifacts have been developed; examples include increased tube current, high tube voltage, thin collimation, additional scanning with gantry tilt, 4 and dual-energy scanning. 5 Even after imaging is complete, other strategies such as single-energy metal artifact reduction (SEMAR) can reduce metal artifacts in the image reconstruction step. 6 With this technique, the dental metals are segmented from the CT image, and then the sinogram and CT image data are corrected after a few back-projection and forward-projection steps. SEMAR has been reported to be able to reduce metal artifacts in oral regions in conventional hybrid iterative reconstruction (Hybrid IR) images.7–9
Deep learning has also been gaining wide attention in radiology. 10 Recent studies have shown that deep learning can be applied not only in imaging diagnosis, 11 but also in image processing. 12 Noise reduction is better with a deep learning reconstruction (DLR) algorithm than with Hybrid IR. 13 In the training process of DLR, deep learning is performed by using low-quality data and high-quality image as input and reference data, respectively. Because of the improved image quality, DLR is expected to spread widely into daily clinical practice. However, although DLR can also be used in combination with SEMAR, 14 no published reports have evaluated the quality of combined DLR-SEMAR images compared with DLR alone or with Hybrid IR–SEMAR.
In the present study, we investigated and compared DLR-SEMAR with DLR alone and with Hybrid IR–SEMAR for metal artifact reduction and the depiction of structures and of lesions in the oral cavity and oropharyngeal region for patients with metal fillings or implants.
Materials and Methods
This retrospective study was approved by our institutional review board, which waived the requirement for obtaining written informed consent.
Patients
We searched our institution’s picture archiving and communication system for all consecutive patients with dental metals who underwent contrast-enhanced helical 320-detector row CT (Aquilion One: Canon Medical Systems, Otawara, Japan) of the oral cavity and oropharyngeal regions. Between November 30, 2021, and January 28, 2022, 37 patients meeting those inclusion criteria were identified. Image sets from 5 patients whose imaging was performed in the arterial phase were selected and used for training purposes in the qualitative image analyses. Those images were also excluded from the final analyses. As a result, 32 patients (25 men, 7 women; mean age: 63 ± 15 years) were included in the final analyses.
These were the indications for CT examination: tumour of the oral cavity (n = 5), posttreatment surveillance for carcinoma of the oral cavity (n = 9), infection of the neck (n = 1), infection of the cheek (n = 1), posttreatment oropharyngeal carcinoma (n = 3), hypopharynx carcinoma (n = 1), posttreatment hypopharynx carcinoma (n = 1), posttreatment submandibular gland carcinoma (n = 1), posttreatment laryngeal carcinoma (n = 2), posttreatment parotid gland carcinoma (n = 1), posttreatment external auditory canal carcinoma (n = 2), nasal tumour (n = 1), posttreatment nasal tumour (n = 2), postoperative glottal carcinoma (n = 1), and postoperative pharyngeal carcinoma (n = 1).
CT Imaging
The CT imaging parameters used for the patients were: tube voltage, 120 kVp; tube current, automatic modulation with standard deviation (SD) set at 13.0; helical pitch, .8125:1; and gantry rotation time, .5 s. The volume and concentration of contrast were chosen based on body weight, with a maximal concentration of 370 mgImL−1 and a 100 mL upper limit for the total volume.
Based on the source data, images were reconstructed using these algorithms: for DLR, the AiCE body sharp standard (Canon Medical Systems); for Hybrid IR, the AIDR 3D enhanced standard, with FC03 reconstruction kernel (Canon Medical Systems) combined with SEMAR (Canon Medical Systems); and DLR combined with SEMAR. In reconstruction of DLR-SEMAR and Hybrid IR–SEMAR, DLR and Hybrid IR images, respectively were also reconstructed simultaneously. However, because there have already been reports which showed the better image of Hybrid IR-SEMAR compared with Hybrid IR, 9 we have omitted Hybrid IR from analyses. Field of view, at 200-250 mm, and slice thickness/interval, at 3/3 mm, were the same across the 3 image sets.
The CT images were anonymized and exported from the picture archiving and communication system in the Digital Imaging and Communications in Medicine format.
Quantitative Image Analyses
Quantitative image analyses were performed in ImageJ (https://imagej.nih.gov/ij/index.html). One radiologist with imaging experience of 2 years placed circular or ovoid regions of interest (ROIs) on the tongue (approximately 30 mm in diameter) at the level of the metal artifacts and on the medial pterygoid muscle (approximately 4 mm in diameter) at a level with no metal (Figure 1) under the supervision of a senior radiologist (with imaging experience of 12 years). In placing the ROIs, the copy-and-paste function was used to ensure that the ROI sizes and locations were the same for each reconstruction algorithm applied to a patient’s imaging data. ROIs were placed without reference to the measured values. After the ROIs were placed, mean CT attenuation for the tongue and SD of the CT attenuation for the medial pterygoid muscle, which is an indicator for image noise, were recorded. Axial enhanced CT images resulting from deep learning reconstruction (DLR) with single-energy metal artifact reduction (SEMAR). For the quantitative evaluation of these images from a 73-year-old man undergoing imaging for postoperative pharyngeal cancer follow-up, circular or oval regions of interest (ROIs) were placed (a) on the tongue at the slice where artifact is prominent, and (b) on the medial pterygoid muscle at the slice where metals are absent. The ROI on the tongue was approximately 30 mm in diameter. The ROI on the medial pterygoid muscle was approximately 4 mm in diameter.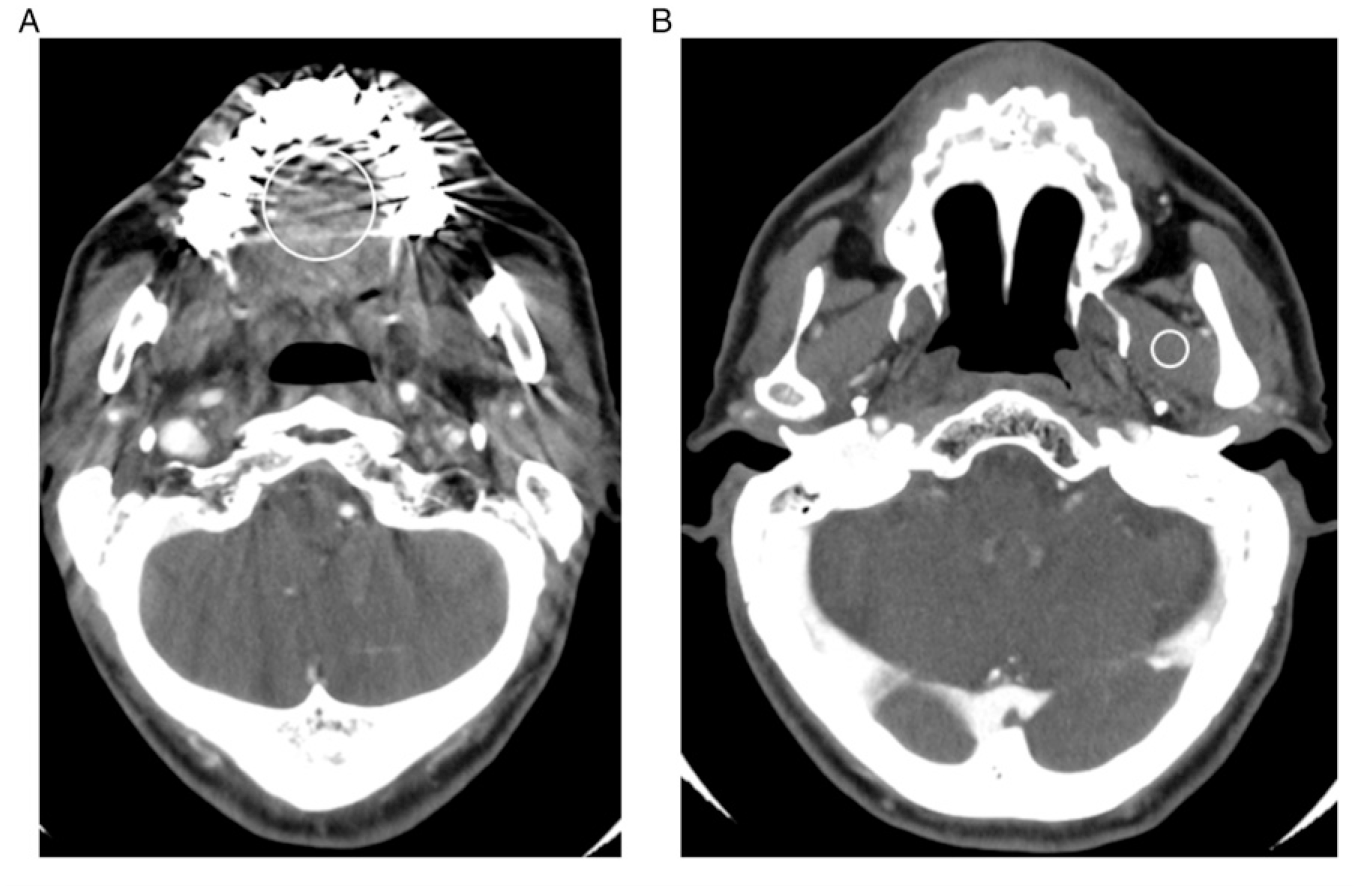
Qualitative Image Analyses (One-by-One and Side-by-Side)
The first radiologist randomized all image sets. In the qualitative image analyses, 2 other radiologists (readers 1 and 2, with 2 and 4 years of imaging experience respectively) used ImageJ to evaluate the image sets. To become familiar with the experiment and to prevent variability in the main evaluation, practice was done with the 5 cases taken in the arterial phase.
First, image sets were evaluated 1 at a time (one-by-one analysis), with the readers being blinded to the image reconstruction algorithm. Their independent evaluations of the image sets considered: ・depiction of structures (tongue apex, tongue root, tonsil, submandibular gland, parotid gland, and parapharyngeal space) (5, clear depiction; 4, slightly clear depiction; 3, slightly blurred; 2, moderately blurred; and 1, unrecognizable). ・artifacts (5, no artifacts; 4, less than mild artifacts; 3, mild artifacts; 2, more than mild artifacts; and 1, artifacts that hinder diagnosis). ・subjective image noise (5, almost no noise; 4, less than standard noise; 3, standard noise; 2, more than standard noise; and 1, severe noise). ・depiction of lesions (4, clear depiction; 3, slightly blurred; 2, moderately blurred; and 1, unrecognizable). For this evaluation, the locations of the lesions were indicated to the readers.
The Hybrid IR–SEMAR and DLR-SEMAR images were then evaluated side-by-side. For this evaluation, the position (left or right) of the reconstructions were randomly varied for each patient. The readers were blinded to the image reconstruction algorithms. Their independent evaluations of the images considered: ・artifacts (2, left image is clearly superior; 1, left image is slightly superior; 0, no difference; −1, left image is slightly inferior; and −2, left image is clearly inferior). ・overall image quality (2, left image is clearly superior; 1, left image is slightly superior; 0, no difference; −1, left image is slightly inferior; and −2, left image is clearly inferior).
Statistical Analysis
Statistical analyses were performed with EZR (version 1.55), a graphical user interface to the R software application (version 4.1.2: R Foundation for Statistical Computing, Vienna, Austria). 15
In the quantitative analyses of the reconstruction algorithms, the variance in CT attenuation of the tongue, which is regarded as an indicator of artifact,16,17 was compared using the Levene test. The SD for the CT attenuation of the pterygoid muscle, which is an indicator of image noise, was compared using the Wilcoxon signed rank test. In the one-by-one qualitative analyses of the algorithms, results were also compared using the Wilcoxon signed rank test. Because the foregoing comparisons were performed for multiple groups (that is, DLR-SEMAR vs DLR, and DLR-SEMAR vs Hybrid IR–SEMAR), the Bonferroni correction was performed, and a P value less than .025 (= .05/2) was considered to indicate a statistically significant difference. In the side-by-side qualitative analyses, the left and right positions of the reconstructions were de-randomized, and the scores were converted such that positive values denoted the superiority of DLR-SEMAR over Hybrid IR–SEMAR. Means and 95% confidence intervals of the scores were calculated, and a lower limit of the 95% confidence interval that exceeded zero was regarded as statistically significant superiority for DLR-SEMAR over Hybrid IR–SEMAR.
In the qualitative analyses, interobserver agreement between the 2 readers was evaluated using the Cohen weighted kappa.
RESULTS
Quantitative Image Analyses
Quantitative Image Analysis.
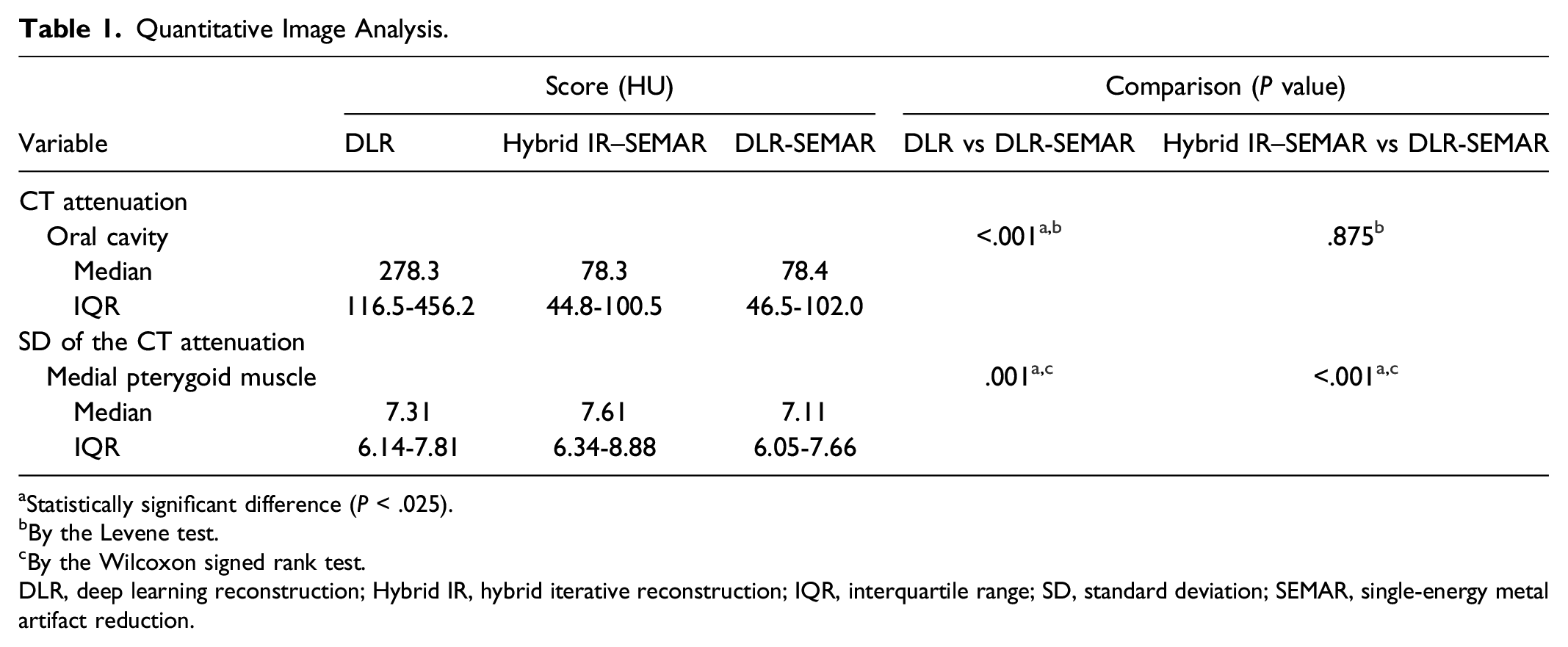
aStatistically significant difference (P < .025).
bBy the Levene test.
cBy the Wilcoxon signed rank test.
DLR, deep learning reconstruction; Hybrid IR, hybrid iterative reconstruction; IQR, interquartile range; SD, standard deviation; SEMAR, single-energy metal artifact reduction.
The SD of CT attenuation (indicator of image noise) in the medial pterygoid muscle was 7.31 for DLR, 7.61 for Hybrid IR–SEMAR, and 7.11 for DLR-SEMAR. The SD of CT attenuation in the medial pterygoid muscle was statistically significantly better with DLR-SEMAR than with DLR (P = .001) or with Hybrid IR–SEMAR (P < .001).
One-by-One Qualitative Image Analyses
One-by-One Qualitative Image Analysis.
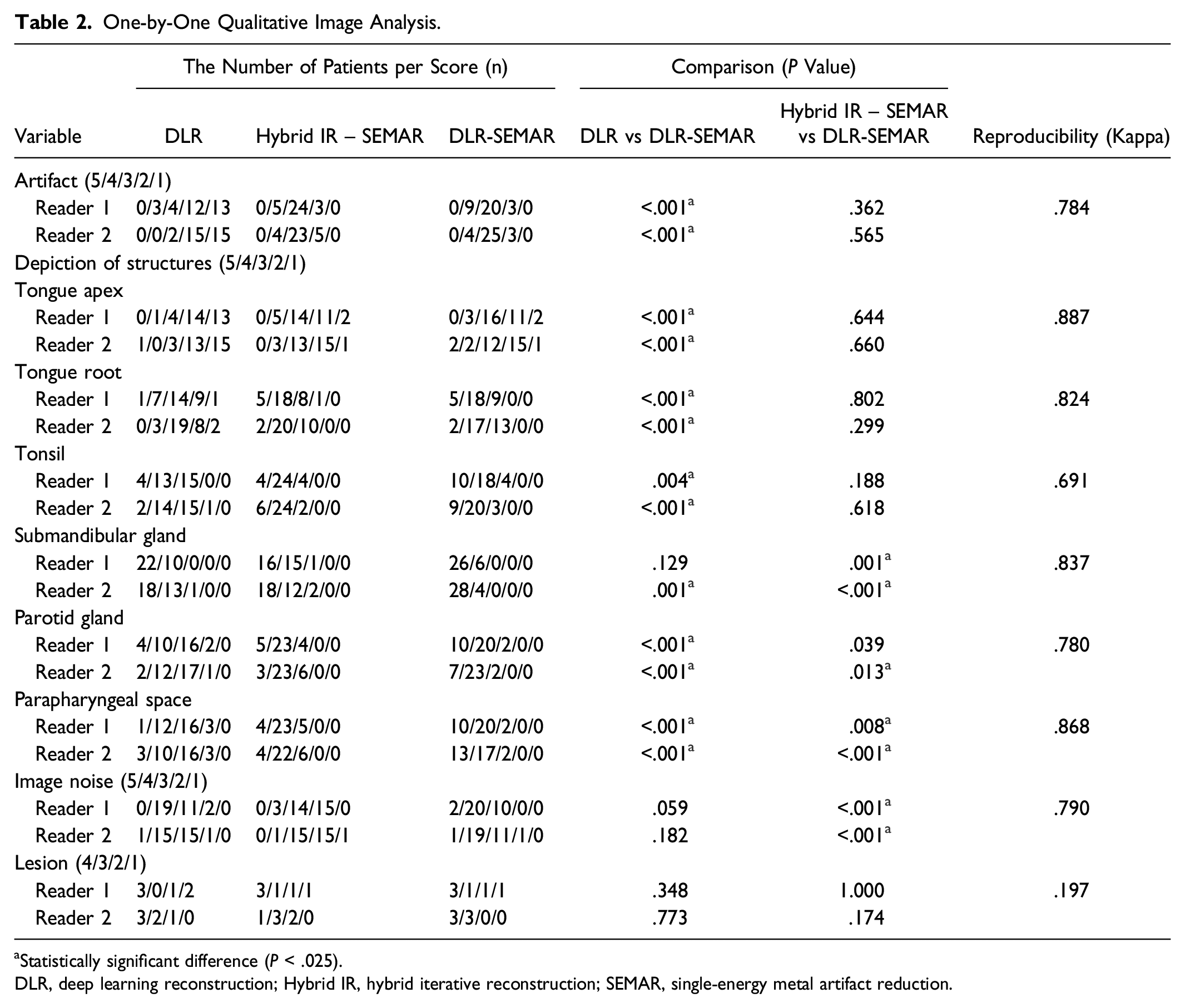
aStatistically significant difference (P < .025).
DLR, deep learning reconstruction; Hybrid IR, hybrid iterative reconstruction; SEMAR, single-energy metal artifact reduction.
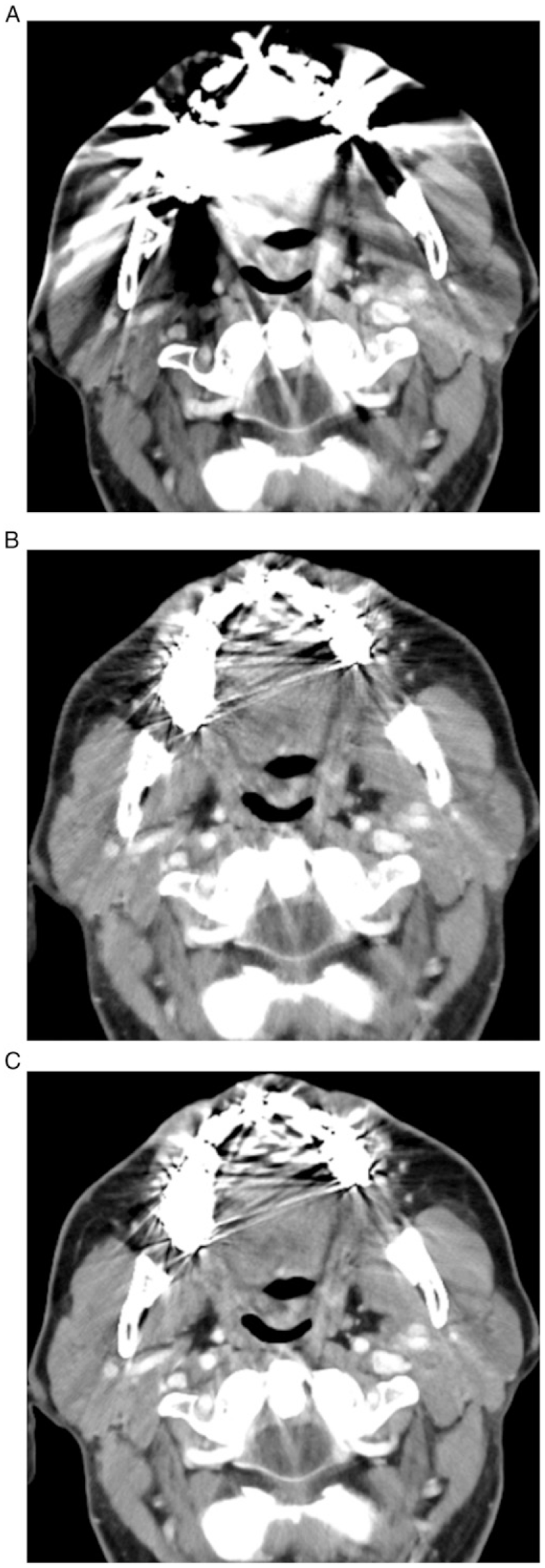
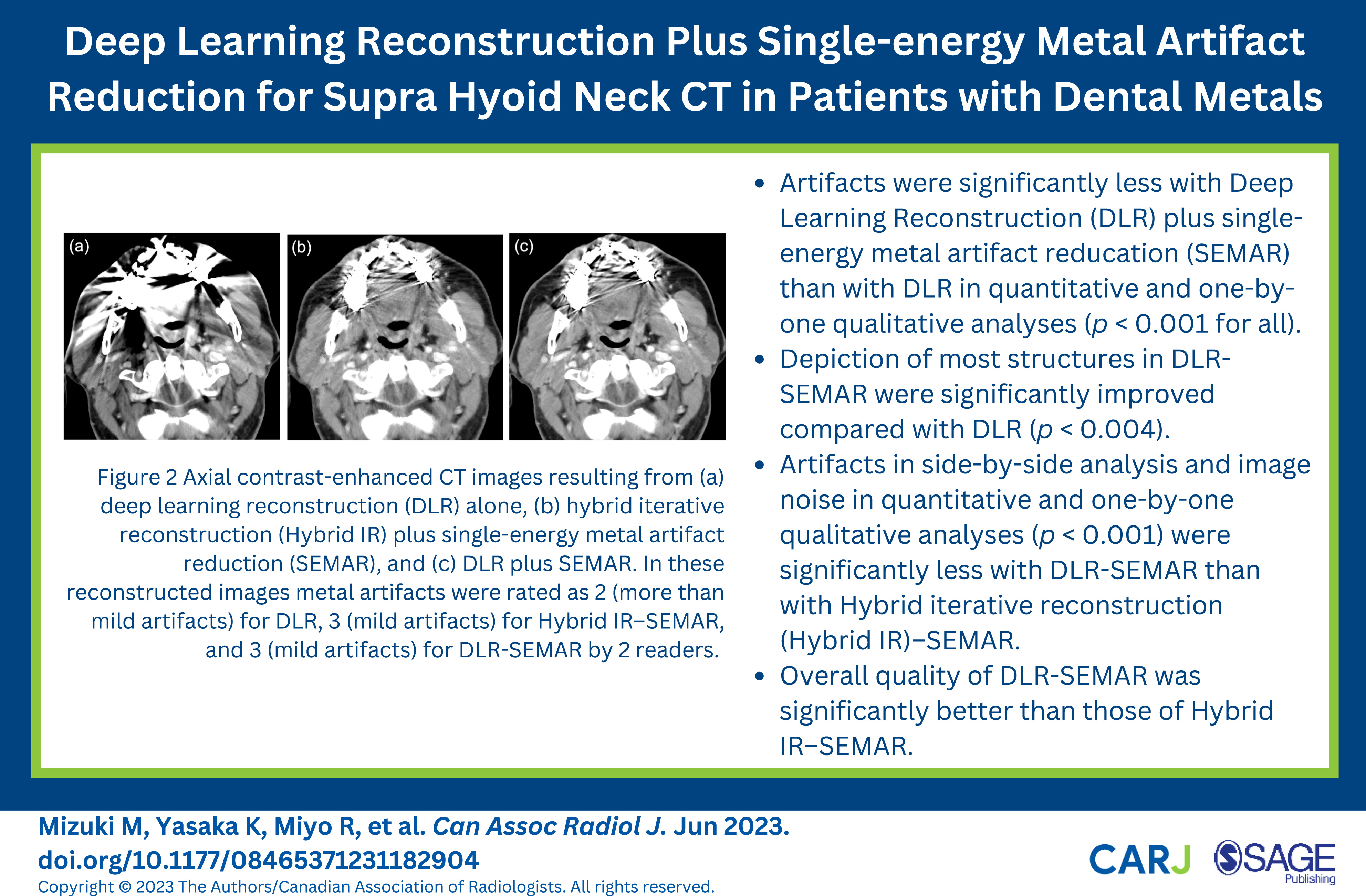
Axial contrast-enhanced CT images resulting from (a) deep learning reconstruction (DLR) alone, (b) hybrid iterative reconstruction (Hybrid IR) plus single-energy metal artifact reduction (SEMAR), and (c) DLR plus SEMAR. In these reconstructed images from a 70-year-old man. Metal artifacts were rated by reader 1 as 2 (more than mild artifacts) for DLR, 3 (mild artifacts) for Hybrid IR–SEMAR, and 3 (mild artifacts) for DLR-SEMAR. Reader 2 also rated the same images as 2 (more than mild artifacts), 3 (mild artifacts), and 3 (mild artifacts) respectively.
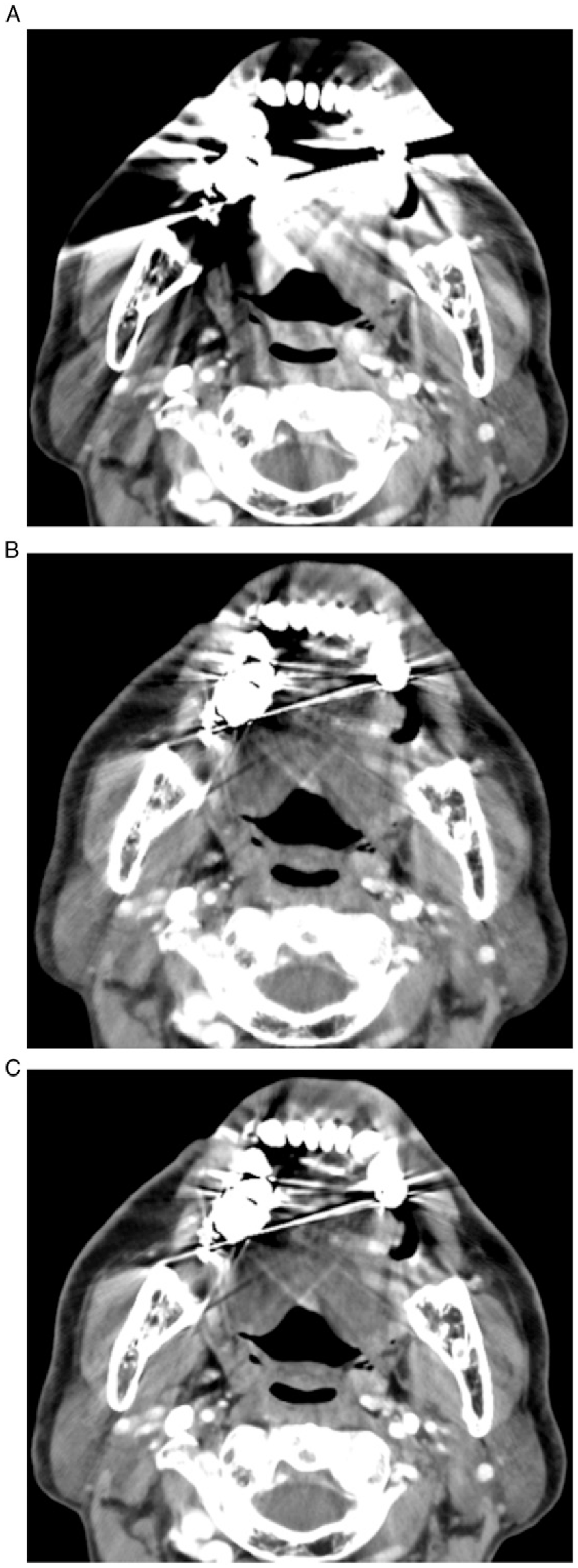
Axial contrast-enhanced CT images resulting from (a) deep learning reconstruction (DLR) alone, (b) hybrid iterative reconstruction (Hybrid IR) plus single-energy metal artifact reduction (SEMAR), and (c) DLR plus SEMAR. In these reconstructed images from a 75-year-old man with a left tongue cancer, metal artifacts were rated by reader 1 as 2 (more than mild artifacts) for DLR, 3 (mild artifacts) for Hybrid IR–SEMAR, and 3 (mild artifacts) for DLR-SEMAR. Reader 2 rated the same images as 2 (more than mild artifacts), 3 (mild artifacts), and 3 (mild artifacts) respectively.
The readers agreed that DLR-SEMAR was significantly superior to DLR in terms of artifact (P < .001), depiction of lingual apex (P < .001), root of tongue (P < .001), tonsil (P < .004), parotid gland (P < .001), and parapharyngeal space (P < .001). With respect to depiction of the submandibular gland, 1 reader found DLR-SEMAR to be statistically significantly better than DLR (P = .001); the other did not (P = .129).
The readers agreed that DLR-SEMAR was significantly superior to Hybrid IR–SEMAR in depiction of the submandibular gland (P < .001) and the parapharyngeal space (P < .008). One reader judged DLR-SEMAR to be statistically significantly better than Hybrid IR–SEMAR in depicting the parotid gland (P = .013). The readers also agreed that DLR-SEMAR was statistically significantly better than Hybrid IR–SEMAR for noise suppression (P < .001).
In the 32 patients, 6 lesions (2 tongue cancers, 1 oropharyngeal cancer, 1 hypopharyngeal cancer, 1 lymph node metastasis, 1 maxillary sinus cancer) were found. Although the differences between the reconstructions were not statistically significant, both readers judged that the depiction of lesions tended to be superior in DLR-SEMAR compared with DLR. One reader judged that depictions tended to be superior in DLR-SEMAR compared with Hybrid IR–SEMAR.
Side-by-Side Qualitative Image Analyses
Side-by-Side Qualitative Image Analysis (DLR-SEMAR vs Hybrid IR–SEMAR).
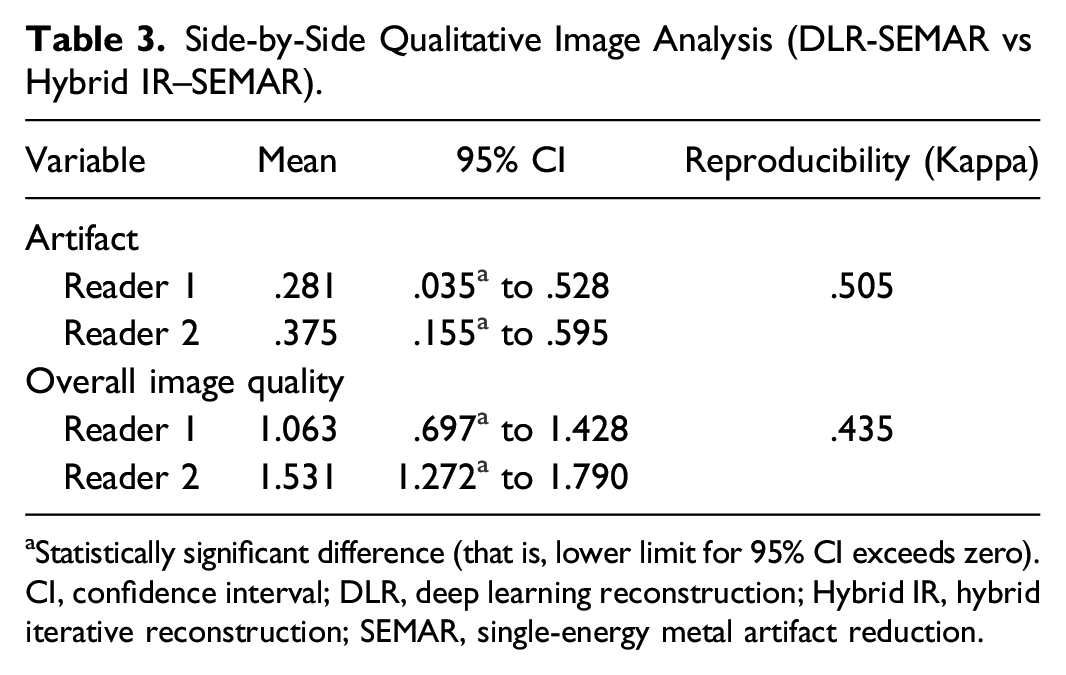
aStatistically significant difference (that is, lower limit for 95% CI exceeds zero).
CI, confidence interval; DLR, deep learning reconstruction; Hybrid IR, hybrid iterative reconstruction; SEMAR, single-energy metal artifact reduction.
Discussion
Artifacts caused by dental metals often interfere with the evaluation of disease in CT examinations of the oral cavity and neck regions. Our study indicated that metal artifacts were significantly reduced and depictions of most structures were improved with DLR-SEMAR compared with DLR in patients with dental metals. In addition, compared with Hybrid IR–SEMAR, DLR-SEMAR showed less artifact (in side-by-side comparison) and image noise, resulting in improved overall quality and improved depiction of the submandibular gland and parapharyngeal space, which are relatively distant from oral metals.
Previous studies have reported that SEMAR reduces metal artifacts and improves image quality in Hybrid IR images of the oral cavity and neck regions.7–9 The present study makes it evident that SEMAR can also reduce metal artifacts in DLR reconstructions. We further found that the depiction of most structures is improved with the use of SEMAR in DLR reconstructions.
In the present study, we also compared artifact reduction in DLR-SEMAR and conventional Hybrid IR–SEMAR. Although the quantitative and one-by-one qualitative analyses demonstrated no significant differences in artifact for those reconstruction algorithms, the side-by-side qualitative analysis revealed a significant difference in artifact between DLR-SEMAR and Hybrid IR–SEMAR reconstructions. Those results indicate that, although the difference is not large, DLR-SEMAR is better than Hybrid IR–SEMAR in terms of artifact reduction.
Noise is also an important element of image quality. Image noise was found to be significantly reduced in DLR-SEMAR images compared with Hybrid IR–SEMAR images, which accords with a published systematic review reporting that the signal-to-noise ratio is significantly higher with DLR than with Hybrid IR. 13 Reduced image noise and artifacts would have resulted in significantly better depictions of the submandibular gland and parapharyngeal space, whose distances from oral metals are relatively large. In other words, the benefit of DLR-SEMAR over Hybrid IR–SEMAR would be most prominent in evaluating diseases of the submandibular gland and parapharyngeal space. Furthermore, image quality was significantly better overall with DLR-SEMAR reconstruction than with Hybrid IR–SEMAR reconstruction.
We also evaluated the depiction of lesions. Because lesions were few in number in our cohort (n = 6), no significant differences were observed; however, the depiction of lesions tended to be better in DLR-SEMAR images than in DLR or Hybrid IR–SEMAR images.
Our study has some limitations. First, most images were postoperative follow-up images. Few pre-treatment images were available, and the number of lesions present in the images was small. Because the evidence indicates that DLR-SEMAR is better than DLR and Hybrid IR in the depiction of some structures, we would expect to see a statistically significant difference in lesion detection rates between DLR-SEMAR and Hybrid IR–SEMAR in an analysis conducted using a larger number of pre-treatment cases. Second, no comparisons of image quality between DLR-SEMAR and Full IR plus SEMAR were performed. Kubo et al. reported that, compared with Hybrid IR, Full IR plus SEMAR is associated with significantly reduced metal artifact. 18 However, a serious concern associated with Full IR is that its reconstruction time when combined with SEMAR is reportedly 17.9 times that for Hybrid IR–SEMAR, 18 making the routine use of Full IR with SEMAR difficult in daily clinical practice. The comparison between DLR-SEMAR and Full IR with SEMAR would therefore have little practical value. Finally, because of the retrospective nature of the present study, the various materials used for the dental fillings could not be taken into consideration in the analyses.
Conclusions
In the present study, metal artifacts were significantly reduced and depiction of structures was improved in DLR-SEMAR images compared with DLR images reconstructed from CT imaging data in the oral cavity and neck regions. In addition, DLR-SEMAR images were found to be less noisy than Hybrid IR–SEMAR images, and artifacts were slightly less with DLR-SEMAR than with Hybrid IR–SEMAR, which was associated with improved overall image quality and better depiction of the submandibular gland and parapharyngeal space, which are relatively distant from oral metals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has received funding by JSPS KAKENHI Grant Number JP 18K15542.
Ethical Approval
This retrospective study was approved by our institutional review board, which waived the requirement for obtaining written informed consent.