
Abstract
Purpose
Retrospective review of splenic artery embolization (SAE) outcomes performed for blunt abdominal trauma.
Materials and Methods
11-year retrospective review at a large level-1 Canadian trauma centre. All patients who underwent SAE after blunt trauma were included. Technical success was defined as angiographic occlusion of the target vessel and clinical success was defined as successful non-operative management and splenic salvage on follow-up.
Results
138 patients were included of which 68.1% were male. The median age was 47 years (interquartile range (IQR) = 32.5 years). The most common mechanisms of injury were motor vehicle accidents (37.0%), mechanical falls (25.4%), and pedestrians hit by motor vehicles (10.9%). 70.3% of patients had American Association for the Surgery of Trauma (AAST) grade 4 injuries. Patients were treated with proximal SAE (n = 97), distal SAE (n = 23) or combined SAE (n = 18), and 68% were embolized with an Amplatzer plug. No significant differences were observed across all measures of hospitalization (Length of hospital stay: x2(2) = .358, P = .836; intensive care unit (ICU) stay: x2(2) = .390, P = .823; ICU stay post-procedure: x2(2) = 1.048, P = .592). Technical success and splenic salvage were achieved in 100% and 97.8% of patients, respectively. 7 patients (5%) had post-embolization complications and 7 patients (5%) died during hospital admission, but death was secondary to other injuries sustained in the trauma rather than complications related to splenic injury or its management.
Conclusion
We report that SAE as an adjunct to non-operative management of blunt splenic trauma can be performed safely and effectively with a high rate of clinical success.
Introduction
The spleen is the most commonly affected visceral organ in blunt abdominal trauma.1,2 Management of splenic trauma has evolved over the past three decades, with non-operative management and splenic salvage being increasingly favoured over surgical intervention in eligible patients.3,4 Splenic artery embolization (SAE) has been used as an adjunct to nonsurgical management of isolated blunt splenic injuries for several decades. 5 It was first described in 1981 by Sclafani 6 and became more widely used in the late 1990s. 5 Presently, non-operative management with SAE is considered standard of care for hemodynamically stable patients in many trauma centres worldwide. The decision on who to treat, when to treat, which embolic to use and where to deploy the chosen embolic has generated considerable debate and controversy over the intervening years.2,7
SAE can be performed distally or proximally depending on the injury pattern. Distal splenic artery embolization (DSAE) is preferred in cases of focal vascular injury (e.g. vessel truncation, pseudoaneurysm and focal extravasation) and proximal splenic artery embolization (PSAE) is preferred for cases where there is multi-focal splenic injury or when no focal angiographic abnormality is identified but CT has demonstrated injury.8,9 PSAE works by lowering the arterial pressure in the spleen, promoting haemostasis and stabilization of fracture clefts within splenic parenchyma. 10 Post PSAE perfusion to the spleen is maintained via collaterals. Collateral splenic perfusion not only prevents infarction but also helps avoid abscess formation and preserves immune function.8,9,11 In cases where there is both multifocal splenic injury and focal vascular injury such as a pseudoaneurysm or active extravasation, a combined splenic artery embolization (CSAE) can be performed where both the focal abnormality is selectively embolized followed by a proximal embolization which reduces the arterial pressure to the diffusely fractured spleen.
The aim of this study was to retrospectively evaluate the rate of splenic salvage in those who had undergone SAE for blunt abdominal trauma.
Methods and Materials
Ethics
Approval was provided by the Research Ethics Board of a large level-1 Canadian trauma centre (project identification number 4908), who determined that individual informed consent was not required for this retrospective analysis.
Patient Identification
This study covered an 11-year period from 1 January 2011 to 1 January 2022. Patients were identified through the Radiology Information System (RIS). Information including demographics, details of hospital stay, treatment and complications were obtained from a combination of RIS, Picture and Communications Archive (PACS) and the Electronic Medical Record (EMR). Splenic injuries were graded on computed tomography (CT) by 2 radiologists and any discrepancies were mediated by an independent interventional radiologist prior to inclusion. Splenic injuries were graded using the American Association for the Surgery of Trauma (AAST) 2018 classification. 12
Inclusion Criteria
All patients over the age of 16 who underwent SAE after blunt trauma were included. Patients were excluded if SAE was performed for non-traumatic reasons or if the mechanism of injury was penetrating. Complications were defined according to the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) classification system. 13 Potential complications included abscess, access site complications, vessel dissection and rebleeding.
Data Collection
Data collected included age, gender, time and date of procedure, length of hospital stay, length of intensive care stay (ICU), mechanism of injury, AAST grade, time to embolization, location of embolization, type of embolic material used, complications, need for rescue splenectomy and timing of splenectomy post SAE.
Embolization Definition
For the purposes of this manuscript, PSAE was defined as a large vessel occlusion proximal to the splenic hilum but distal to the dorsal pancreatic artery. DSAE was defined as embolization of selected splenic artery branches distal to the hilum. CSAE refers to a procedure where DSAE was performed for focal vascular lesion, followed by PSAE.
Outcome Definition
Technical success was defined as angiographic occlusion of the target artery at conclusion of the procedure. Clinical success was defined as splenic salvage after SAE.
Embolization Technique
All procedures were performed by one of 6 fellowship trained interventional radiologists, or a supervised clinical fellow. According to operator preference, embolization was performed using pushable coils (.018 or .035 Cook Nester or MicroNester, Cook Medical, Bloomington, USA), Amplatzer™ vascular plugs (Abbott Laboratories, Chicago, IL, USA), Microvascular plugs (Medronic, Dublin, Ireland), Cyanoacrylate (GluStitch Inc, Delta, BC, Canada) or Gelatin sponge.
Statistical Analysis
All statistical analysis were completed using SPSS (IBM SPSS Statistics for Windows, Version 28, Armonk, NY). Demographic characteristics were analysed using independent samples Median Test. Approximate P-values were reported based on chi-squared and corresponding degrees of freedom. Clinical characteristics were analysed using independent samples Kruskal–Wallis H test. Differences with a probability of .05 were considered statistically significant. Following a significant interaction, a series of Mann–Whitney tests were performed to ascertain which pairs of groups differ significantly from one another.
Results
Demographic and Clinical Characteristics for the Three SAE Groups. Values Reported as Median (Interquartile Range), Unless Specified Otherwise.
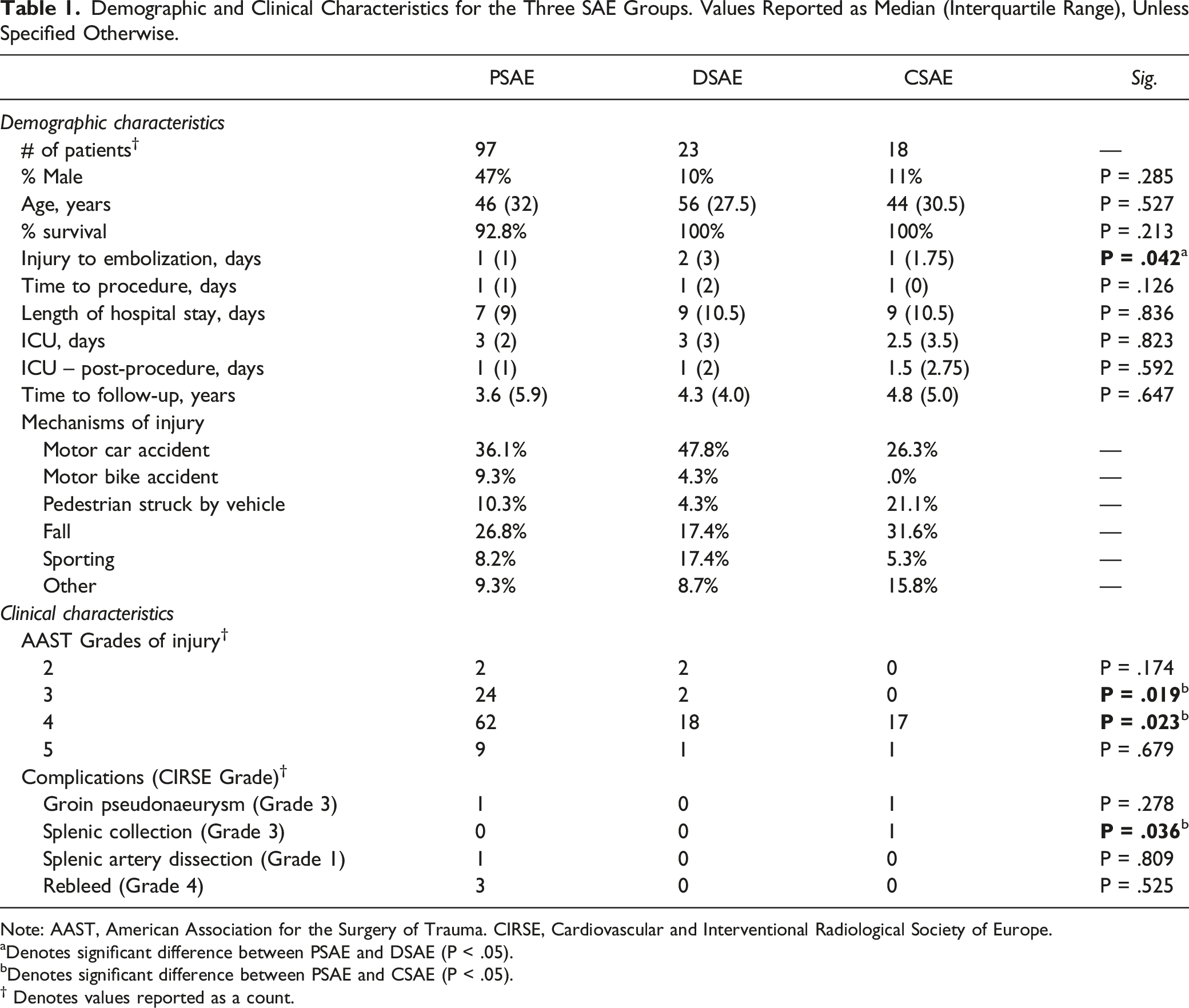
Note: AAST, American Association for the Surgery of Trauma. CIRSE, Cardiovascular and Interventional Radiological Society of Europe.
aDenotes significant difference between PSAE and DSAE (P < .05).
bDenotes significant difference between PSAE and CSAE (P < .05).
† Denotes values reported as a count.
Patient Demographics
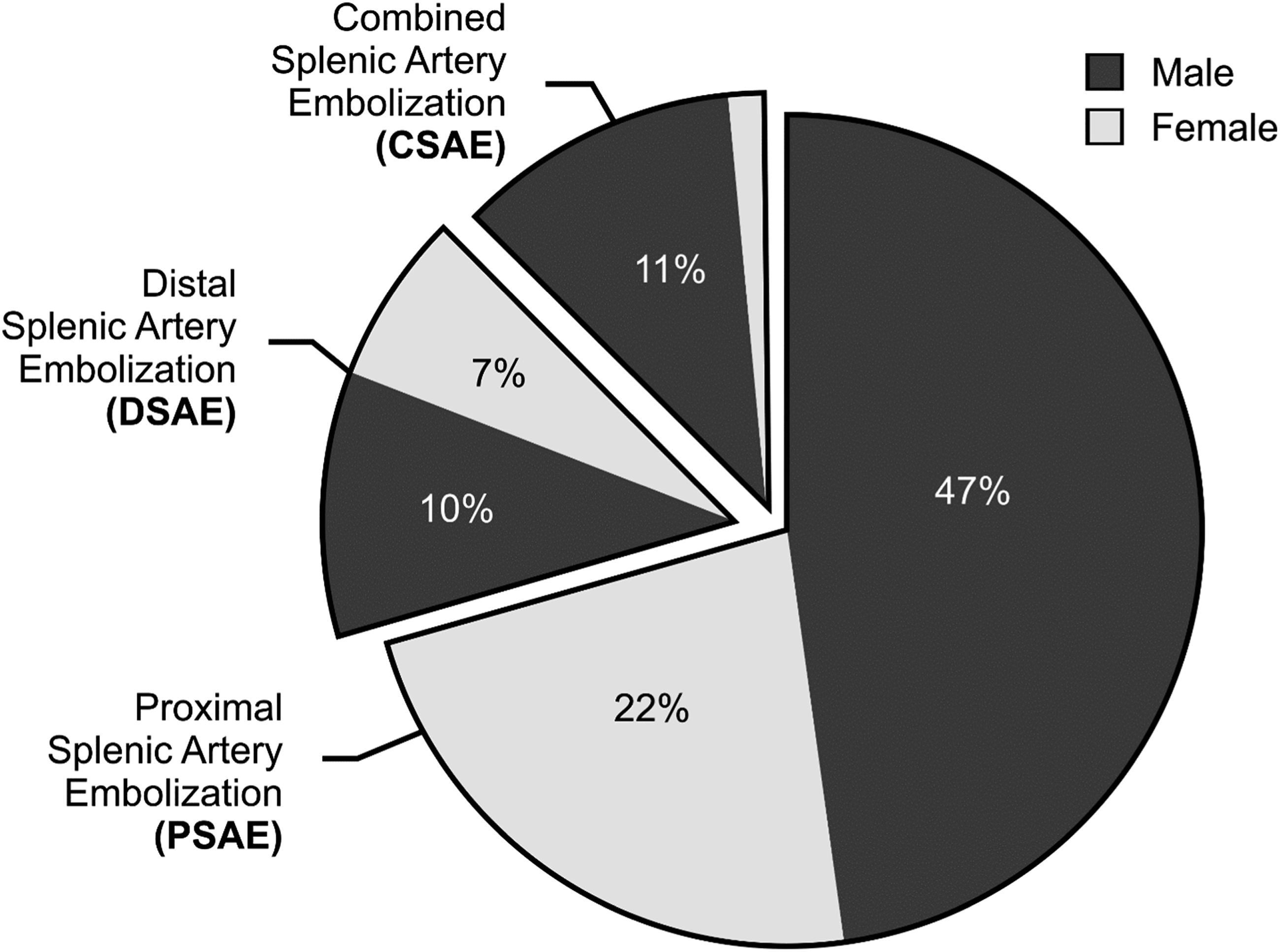
A total of 159 patients underwent splenic embolization in the defined study time, of which 138 had a history of blunt splenic trauma. 68.1% of total patients were male and the median age was 47 years (IQR = 32.5 years; range 16-94 years). 42.0% of embolizations were performed as emergency out of hours procedures. 8 embolizations were performed in 2011 while 15 were performed in 2021, with trends between these years shown in Figure 1. Patients had either PSAE (n = 97), DSAE (n = 23) or CSAE (n = 18) performed (see distribution of sex across groups in Figure 2). Number of splenic embolizations over an 11-year period. Distribution of gender across three splenic embolization treatment groups.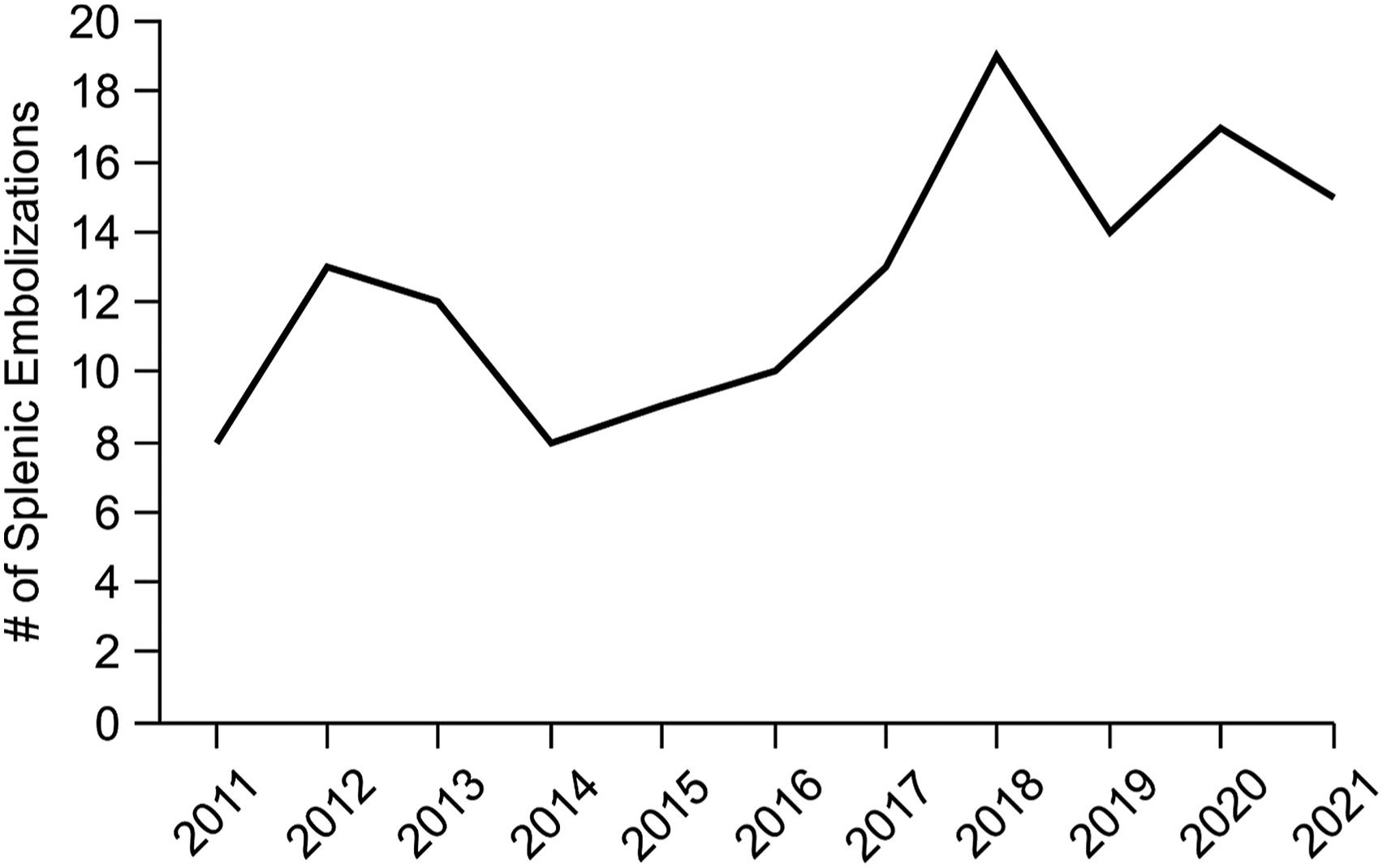
Hospitalization Time
No significant median differences were observed across all dependent measures of hospitalization time between the different categories of embolization (Length of hospital stay: x2(2) = .358, P = .836; ICU stay: x2(2) = .390, P = .823; ICU stay – post-procedure: x2(2) = 1.048, P = .592). In general, the median hospital stay was 7.5 days (IQR = 9.75 days). 91.3% (n = 126) were admitted to an Intensive care unit (ICU) during their stay. The median length of ICU admission was 3 days (IQR = 2 days). The median length of ICU stay post-procedure was 1 day (IQR = 1.75 days). An overview of the breakdown of hospitalization times across groups are presented in Table 1.
Mechanism and Grades of Injury
Figures 3 and 4 demonstrate the mechanism and grade of injury between the treatment groups, respectively. The most frequent mechanisms of injury were motor car accidents (37.0%), mechanical falls (25.4%) and pedestrians hit by motor vehicles (10.9%). Total number of injuries by mechanism across the three splenic embolization treatment groups. Distribution of grade of injuries across the three splenic embolization treatment groups based on the American Association for the Surgery of Trauma (AAST) scale.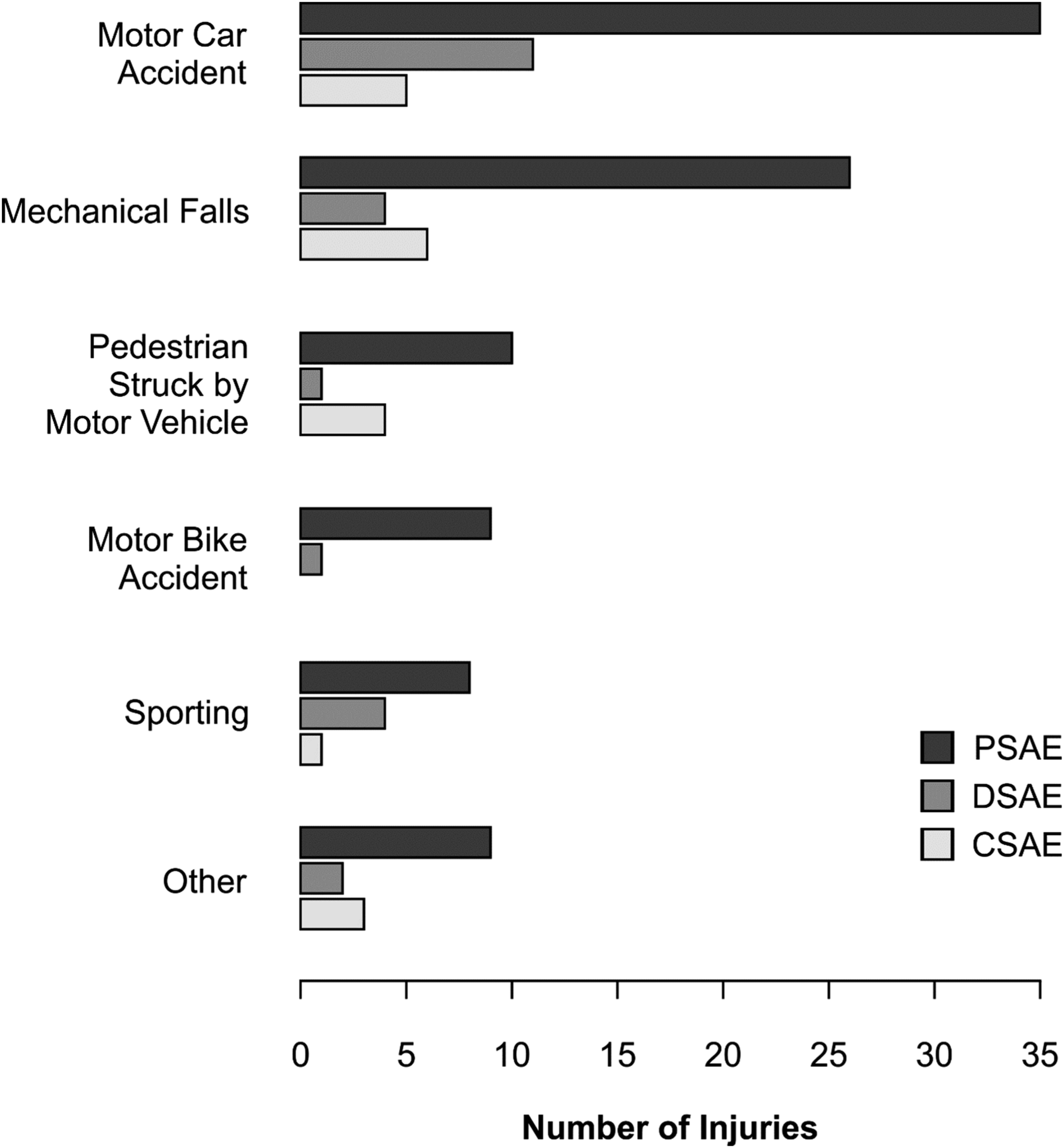
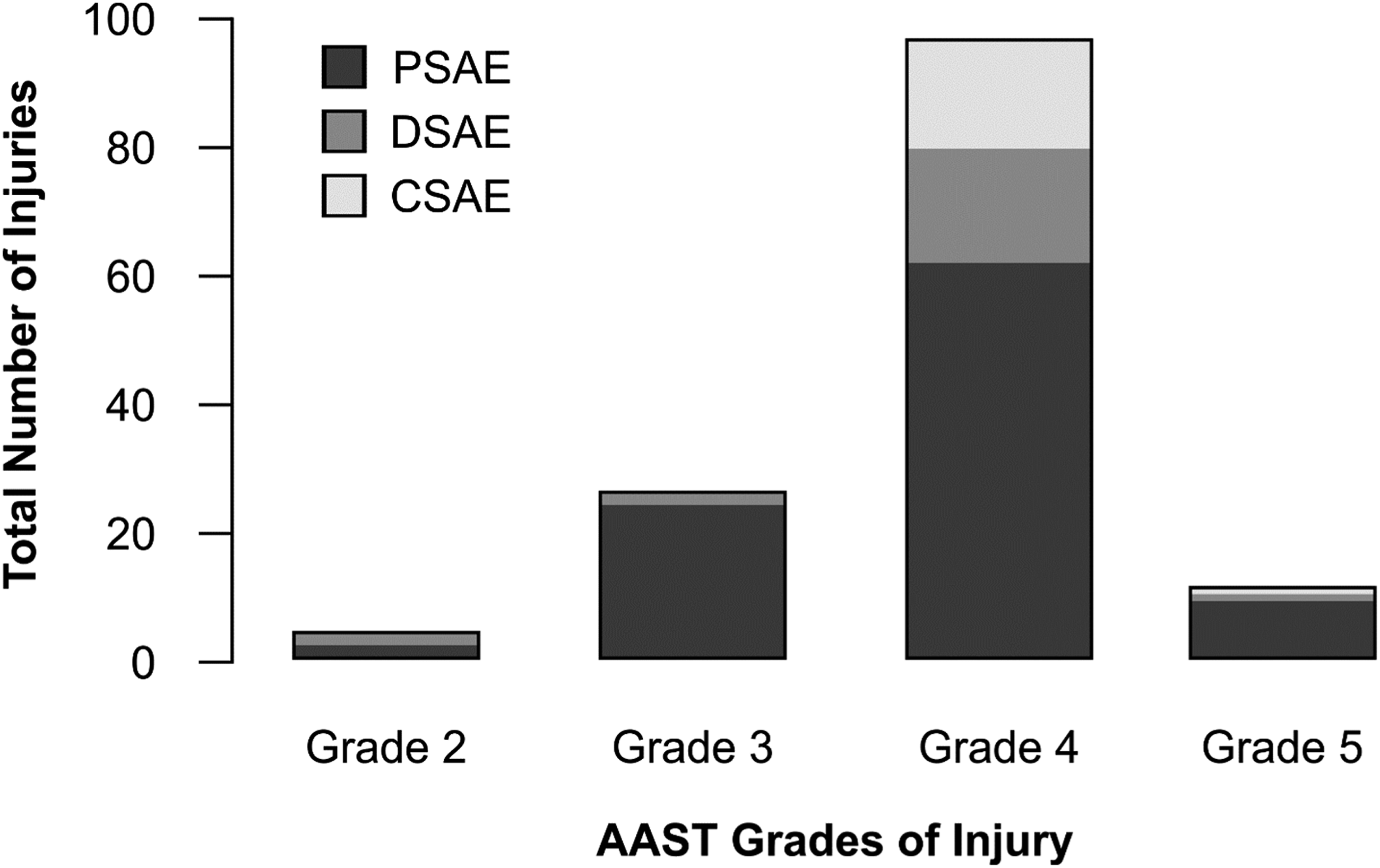
The majority of patients in each group had AAST grade 3 or grade 4 injuries, with 70.3% of all patients having AAST grade 4 injuries (Figure 4). Total number of patients admitted with blunt splenic trauma, and grade of spleen laceration, is described in Figure 5.
Time to Embolization
The median length of time (days) from injury sustained to time of embolization was 1 day (i.e. within 24 hours, IQR = 1 day and range: 1–2 days). As shown in Table 1, there was a significant difference between the PSAE and DSAE groups in the interval between time of injury to embolization (x2(2) = 6.321, P = .042). Analysis indicates that the PSAE group (xmedian = 1 day, IQR = 1 day) had significantly less time elapsed between injury to procedure compared to the DSAE group (xmedian = 2 days, IQR = 3 days, P = .010). The median length of time (days) from presentation at the hospital to embolization was 1 day (i.e. within 24 hours, IQR = 1 day and range: 1-2 days). In this category, there was no significant difference in the time interval between the 2 groups (x2(2) = 4.146, P = .126). Total number of patients admitted with blunt splenic trauma.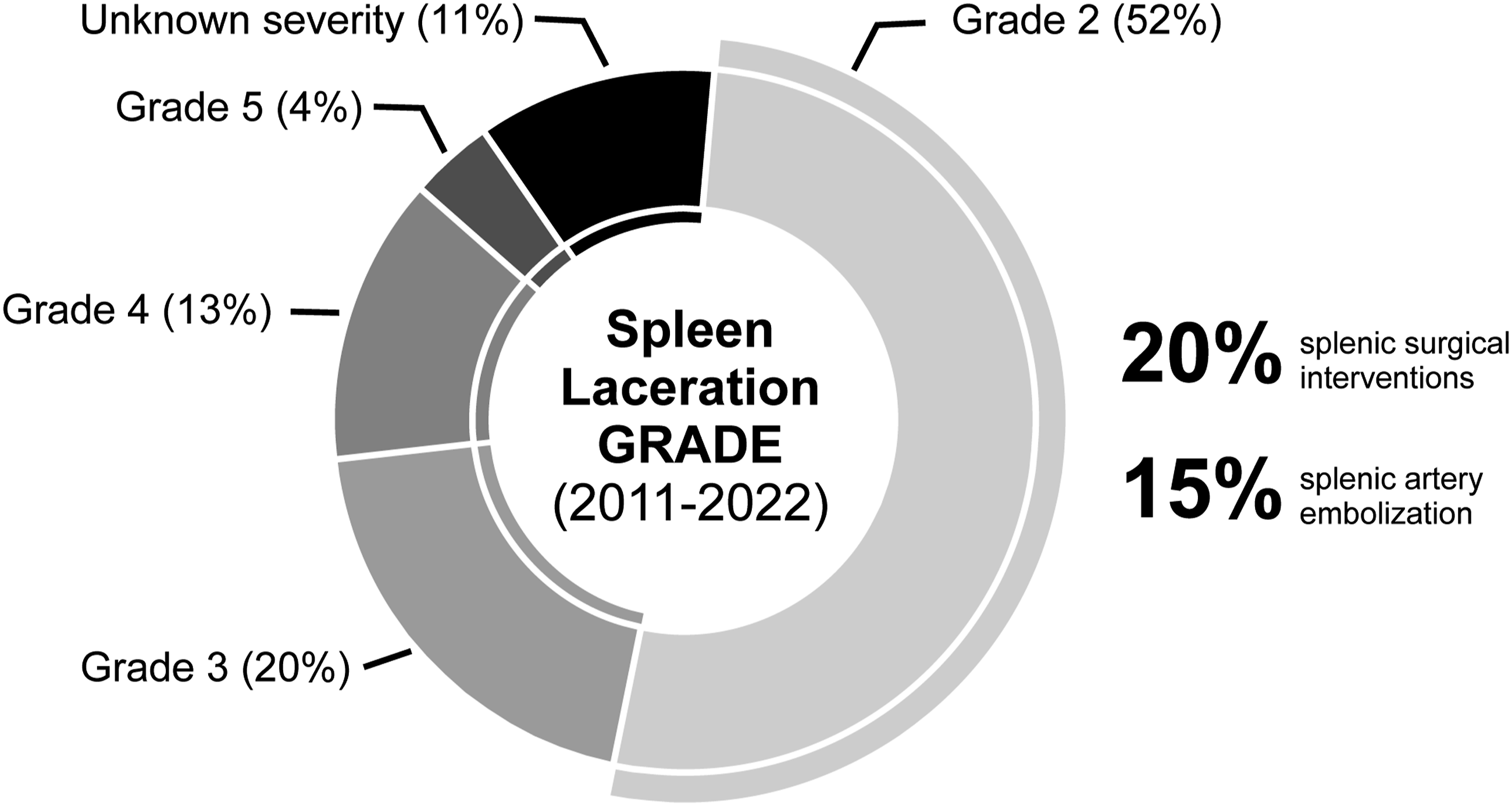
Choice of Embolic
Type or Combination of Embolic Used for PSAE and DSAE Groups. Values Reported as Percentages.
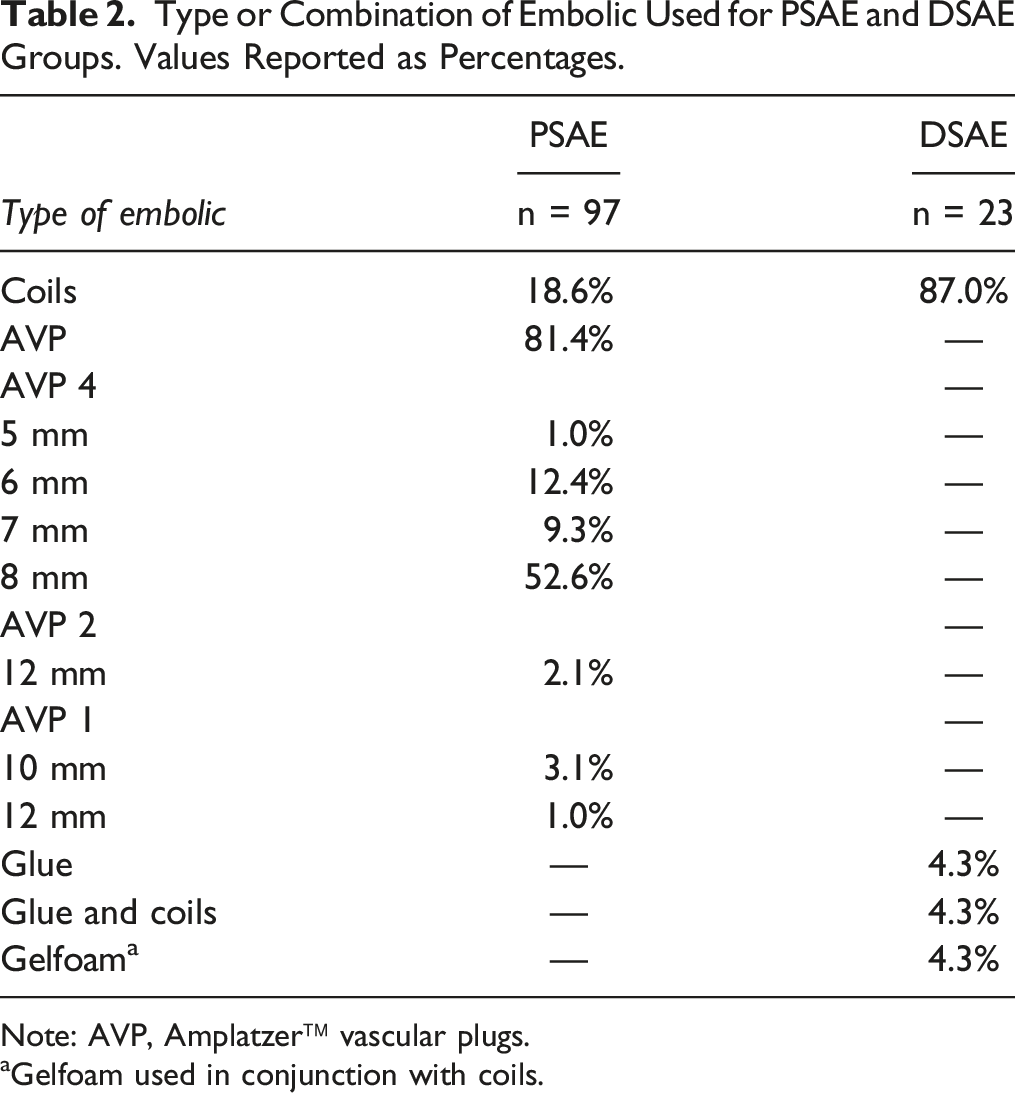
Note: AVP, Amplatzer™ vascular plugs.
aGelfoam used in conjunction with coils.
For CSAE, 14 of the 18 patients (77.7%) patients were treated with AVP (PSAE) and coils (DSAE). The remainder were treated with various other combinations ([1 AVP (PSAE) and Gelfoam (DSAE)], [1 Microvascular plug (PSAE) and coils (DSAE)], [1 Coils (PSAE) and Gelfoam (DSAE)], [1 Coils (PSAE) and coils (DSAE)]).
Outcomes
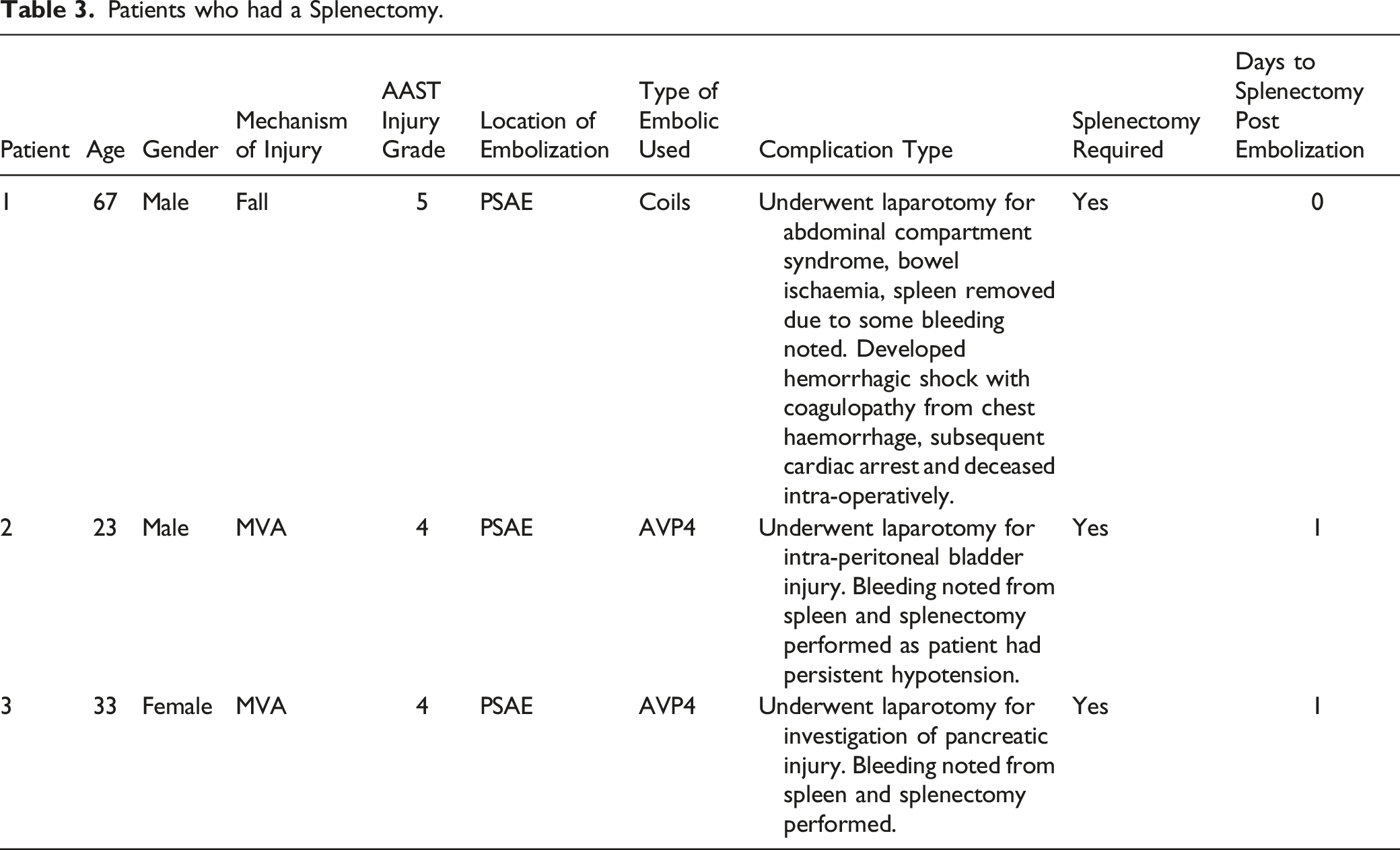
Patients who had a Splenectomy.
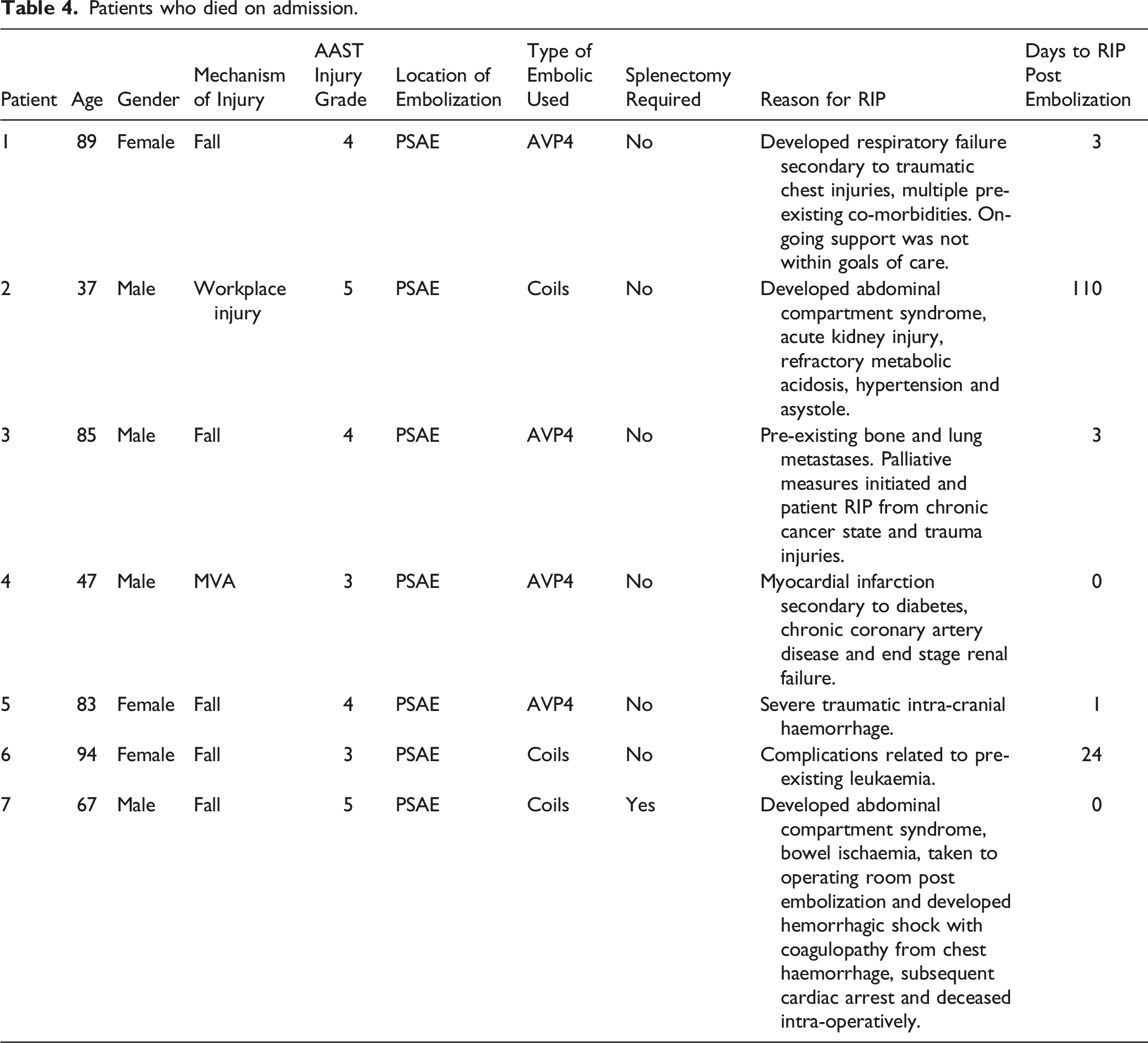
Patients who died on admission.
Limitations
As a single centre study, our practice at a large regional trauma centre with tertiary and quaternary care services may not be reflective of how other hospitals are structurally designed but this review shows that high rates of splenic salvage are possible in the management of blunt splenic trauma. We acknowledge that the data collected is heavily skewed to PSAE with Amplatzer plugs, given the smaller numbers in the other groups. This bias may reduce the statistical reliability of our analysis. The number of complications such as splenic infarction may be underreported as patients were not routinely followed up with imaging unless they had specific symptoms that warranted a workup. It is reasonable to infer that small splenic infarcts that were clinically silent were not picked up in this analysis.
Discussion
This study affirms that there is a high rate (97.8%) of splenic salvage in patients who have SAE and is in keeping with rates previously described in the literature.7,14-16 Patients in this series who ended up with a splenectomy did so while being treated for other injuries that required a laparotomy. Splenic bleeding described as slow in the OR notes was incidentally identified during the laparotomy and it is difficult to know for certain if this bleeding would have been clinically significant in the absence of other injuries. All three patients who underwent splenectomy were treated with PSAE which in comparison to DSAE, does not directly stop arterial extravasation but rather decreases arterial pressure to the spleen and allows for clotting.
The majority of patients embolized had AAST grade 4 injuries (n = 97, 70.3%) and the decision on who and when to embolize was made in collaboration with the admitting trauma team. The standard of practice at our institution dictates that patients who are hemodynamically stable with significant splenic trauma (generally greater than, or equal to, grade 3) are considered for embolization and those who are hemodynamically unstable are considered for surgical management. The median time from the patient’s arrival at the hospital to performing splenic embolization was one day (i.e. within 24 hours), with 42% of these embolizations done as an emergency out of hours procedure. The Splenic Arterial Embolization to Avoid Splenectomy (SPLASH) trial, a recent multicentre randomized prospective clinical study, demonstrated that for hemodynamically stable patients with high grade splenic trauma, there was no significant difference in rates of splenic salvage and complications between immediate SAE and surveillance with SAE performed only if necessary. 16 Ultimately, this trial did not recommend one management strategy over another but concluded that both prophylactic angioembolization and surveillance were defensible strategies for patients with high grade splenic injuries. 17 The median length of hospitalization in this trial was significantly shorter for patients in the embolization group compared to the surveillance group. This would suggest that in resource restricted environments where the number of hospital beds per capita are limited, embolization would have advantages related to earlier patient discharge.
94 patients (68.1%) in our study were embolized with an Amplatzer™ plug, which to the best of our knowledge, is the largest case series demonstrating the successful use of these plugs as the primary embolic utilized for splenic embolization. Amplatzer™ plugs come in three varieties that are suitable for PSAE, the AVP, AVP II and the AVP-4. 18 The majority of patients (n = 88) in our study were treated with an AVP-4, some of the benefits being that it can be delivered through a 5 French catheter allowing for rapid and precise deployment. The largest diameter the AVP-4 comes in is 8 mm. The AVP and AVP II come in a wider variety of diameters and were generally used for treating larger splenic artery diameters, which require a 5 French sheath or a 6 French guiding catheter. 10 Only 2 of the 94 patients (2.1%) treated with Amplatzer™ plugs developed a rebleed, suggesting that these plugs offer a very effective and efficient alternative to coils for PSAE.
The overall complication rate in this study was 5%, which is consistent with recently published studies on splenic embolization.7,16 Of the 7 patients who died during hospital admission, none succumbed from splenic rupture or embolization related complications (Table 4) but rather to other injuries incurred in the trauma. We did not see any complications in the DSAE group, which is unusual and may be explained by the small number of patients in this cohort (n = 23, 16.6%). There was a statistically significant difference in the number of splenic collections in the CSAE group (n = 1) compared to the PSAE group (n = 0), however there was no significant difference in the overall rate of complication between the groups. A recent meta-analysis reported a doubled rate of complications in CSAE (58.8%) compared to PSAE (18.2%) or DSAE (28.7%) alone. 19 This discrepancy in our study compared to reported complication rates in the literature could be explained by our low use of Gelfoam, which was used in one DSAE case and two CSAE cases. It has been reported that the use of Gelfoam results in higher complication rates when compared to other embolics.20-23
Conclusion
Given the low rate of complications and high rate of clinical success, the use of embolization as an adjunct to non-operative management in splenic trauma is a reasonable and effective strategy. It validates the need for accessible interventional radiology services at trauma centres not just for pelvic trauma but for solid organ injury as well.
Supplemental Material
Supplemental Material - Retrospective Evaluation of Splenic Artery Embolization Outcomes in the Management of Blunt Splenic Trauma: A Single Centre Experience at a Large Level 1 Trauma Centre
Supplemental Material for Retrospective Evaluation of Splenic Artery Embolization Outcomes in the Management of Blunt Splenic Trauma: A Single Centre Experience at a Large Level 1 Trauma Centre by C O’Rourke, H McKee, DO Wijeyaratnam, J Bajwa, L Tremblay, and E David in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.