
Abstract
Introduction
Organ replacement programs are a cornerstone to health care, with transplantation offering improved overall survival and quality of life to most patients. Kidney transplantation is considered the gold-standard treatment for end-stage renal disease (ESRD). 1 This treatment can be sub-categorized into deceased and living-donor renal transplantations, with the latter offering the best outcomes in terms of allograft survival, consistent early function, and less aggressive immunosuppressive regiments.2,3 Surgeons have evolved their techniques over the years to increase donation rates, such as through living-donor paired-exchange programs and through the implementation of laparoscopic surgery, which offers a minimally invasive procedure with shorter recovery time for the donors.4,5
While the COVID-19 global pandemic initially resulted in the suspension of several Canadian renal transplant work-up and living-donor kidney transplant programs, hospital facilities have since optimized their approaches to return to a near normal frequency of transplants. 6 In 2021, a total of 2835 solid organ transplants were performed in Canada, with kidneys accounting for 59% (1673) of all transplantations. 7 This is not significantly changed in comparison to a total of 1790 kidney transplantations being performed in 2019 out of a total of 3053 solid organ transplants (59%). 7
Laparoscopic donor nephrectomy, though advantageous over open nephrectomy, poses several technical challenges such as limited surgical field of view. 8 In addition, anatomic variations must be taken into consideration when deciding upon which kidney to donate, as it can significantly impact both donor and recipient outcomes. As such, diagnostic imaging is fundamental to the preoperative assessment of potential living renal donors, with the overarching goal of helping our surgical colleagues establish suitable donor candidates. 9 CT angiography offers an established, minimally invasive, easily accessible, and relatively rapid method of donor evaluation.10,11 A detailed description of the renal parenchyma, renal vasculature anatomy, and urinary collecting system helps surgeons assess the technical feasibility of the transplantation, reduces surgical complications, and screens for co-morbidities. 11
The purpose of this study was to evaluate whether standardized template reporting for the preoperative assessment of potential living renal transplant donors improves the comprehensiveness of radiographic reports to meet the needs of urologists performing renal transplants.
Materials and Methods
Hospitals based in Ontario, Canada with an adult renal transplant program were invited to participate in the research study. REB exemption or approval for a quality initiative project was obtained at all institutions involved. Urologist and radiologist stakeholders from each of the Ontario renal transplant centres ratified a standardized reporting template for the evaluation of potential renal donors, with a reporting checklist for image interpretation based on established literature.12,13 Following the creation of this template, each institution reviewed and approved its use with slight variations in wording made per centre. The templates were then made available to radiologists through the institution’s transcription software or an established centralized template list. An example of the utilized standardized template can be found in Supplemental Appendix A. Utilization of the standardized report template was encouraged at each site, and compliance was reinforced through educational sessions, departmental meetings, short-term auditing, and reminders through emails and face-to-face interactions. Trainees were alerted to the template by the supervising radiologists at the beginning of their rotation.
Three centres (A, B, and C) were designated “intervention” groups. Centre D was the control group, given employment of a site-specific standardized template prior to study commencement. Reports of adults (age >18 years) undergoing evaluation for living renal transplant donation were retrospectively collected for analysis, with 100 consecutive CT scan reports per centre, pre- and post-implementation of standardized reporting. A fifth institution (Centre E) was added to the study as an ancillary institution as their renal transplant program is relatively new, with only 34 pre- and 14 post-implementation reports available at the time of publication. Additionally, long-term adherence to the standardized template was evaluated at the highest volume intervention institution. All reports for CT scans performed in a 12-month period following the first year of template implementation were evaluated for overall compliance to standardized reporting.
Each report was analyzed independently by an abdominal-imaging trained radiologist or radiology trainee (fellow or resident) at their respective institutions for thirteen outcome measures, including size characteristics (3D dimensions and maximum dimension), shape/parenchyma, scarring, calculi, renal cyst, renal mass, arterial anatomy (number of arteries, artery diameter, and distance to first branch), venous anatomy, presence of large lumbar veins, and collecting system characteristics. Each outcome variable was objectively measured as either “yes, discussed in the report” or “no, not discussed in the report.” The outcome variables for the left and right kidneys were evaluated separately.
The collected data from all institutions was exported into Microsoft Excel spreadsheet software (version 16.58, 2022) and aggregated for analysis. Differences in outcome variable reporting pre- and post-implementation of the standardized template, calculated as an overall percentage of variable reportage, were tested using Z-tests (standard score). Analysis was based on the null hypothesis of no difference between pre- and post-implementation responses. Compliance post-template implementation, measured as “yes, the template was utilized” or “no, the template was not utilized,” was calculated as an overall percentage for each institution. A P value less than .05 was considered statistically significant.
Results
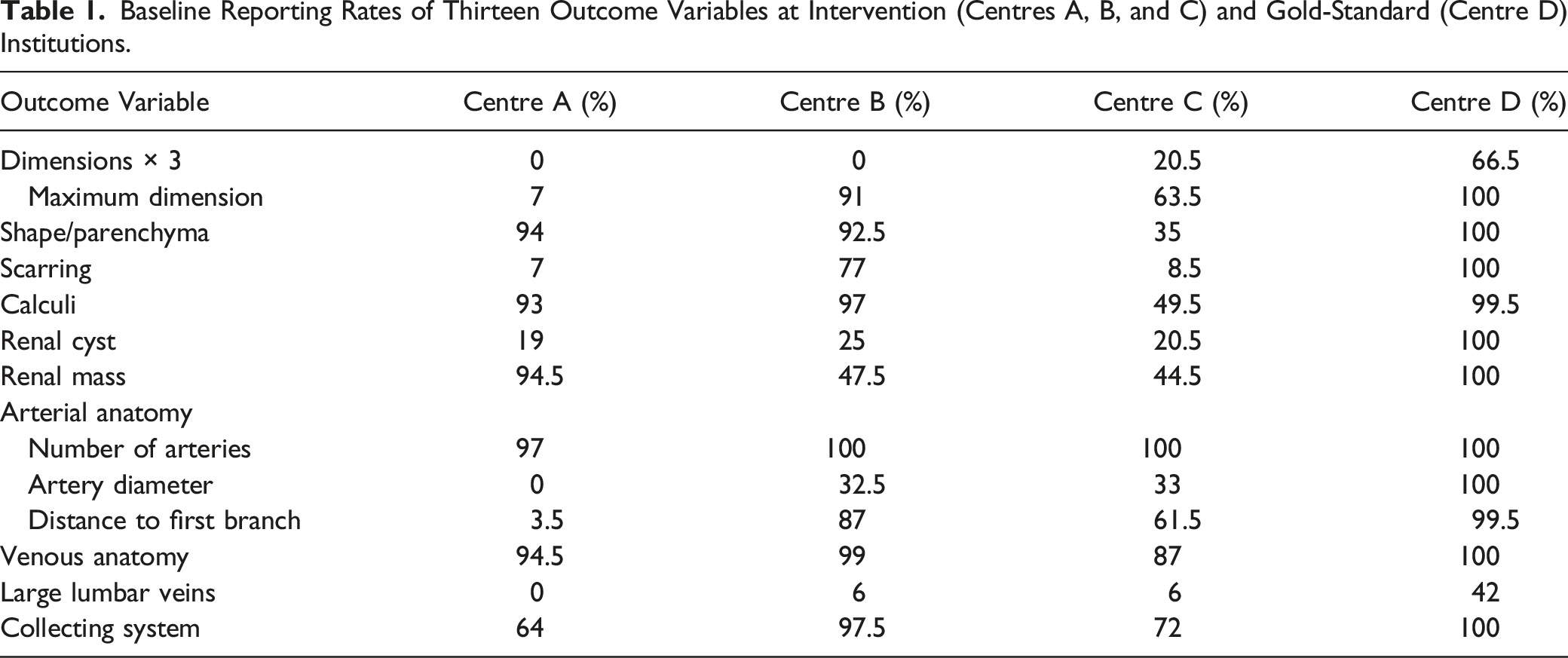
Baseline Reporting Rates of Thirteen Outcome Variables at Intervention (Centres A, B, and C) and Gold-Standard (Centre D) Institutions.
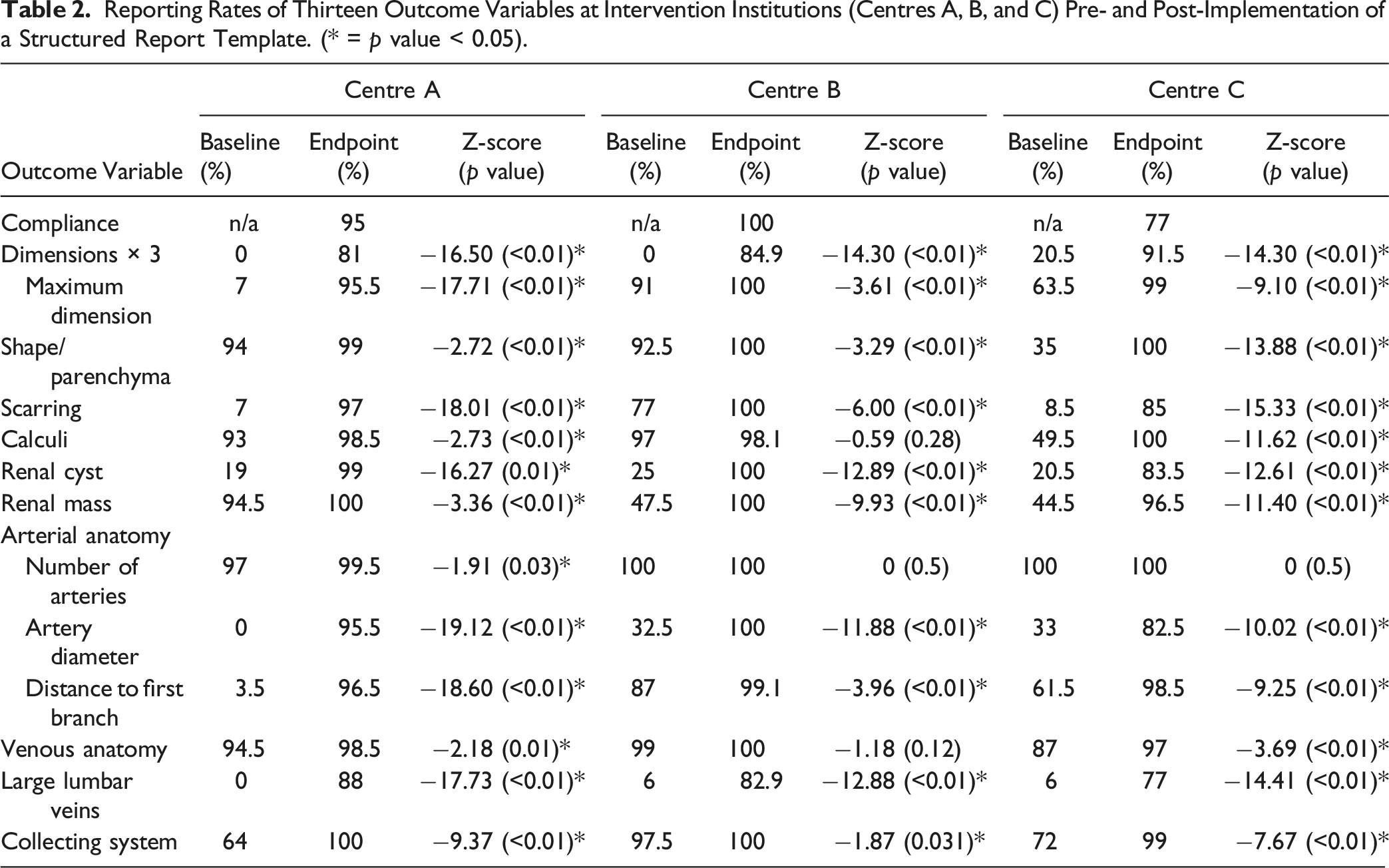
Reporting Rates of Thirteen Outcome Variables at Intervention Institutions (Centres A, B, and C) Pre- and Post-Implementation of a Structured Report Template. (* = p value < 0.05).
Compliance of radiologists’ utilizing their institution’s standardized reporting template was also evaluated and, overall, was excellent amongst all interventional centres. Compliance at Centre A was 95%, Centre B was 100%, and Centre C was 77%. The gold-standard institution, Centre D, demonstrated a compliance of 100%. Long-term compliance of standardized template reporting was also shown to be excellent at the intervention centre with the highest overall volume of renal donor CT scans. A total of 79 CT scans were performed in the 12-month period following the first year of template implementation, with 78 reports utilizing the standardized template (compliance = 98.7%). The only instance where the template was not used was in an unexpected finding of a solitary kidney with an intra-renal mass. As such, a standard abdominal/pelvis template was used given the patient’s ineligibility for renal transplant donation.
The ancillary institution (Centre E), though with fewer cases, demonstrated an equivalent trend to the other intervention institutions (Centres A, B, and C) with overall poor reliability of outcome reporting at baseline. Pre-template implementation, only 8% (1/13) and 38% (5/13) of variables were reported at 90% and 50% reliability, respectively. While limited by a lack of patients’ imaging studies to evaluate post-template implementation (14 reports evaluating 28 kidneys), 13 out of the 13 variables were reported at a rate of 100%, with 100% compliance in utilization of a standardized template.
Discussion
Preoperative assessment of potential living renal donors can be extensive, requiring a multi-disciplinary approach for which radiologists play a crucial role through multiphasic CT imaging evaluation. The results of this study confirm that radiologists who employed a narrative-style free-text report consistently omitted important variables urologists require for surgical planning. The application of a standardized template resulted in a statistically significant improvement in the number of key outcome variables reported. Furthermore, all institutions involved demonstrated excellent compliance in the utilization of a standardized report template.
Accurate and reliable description of the outcome variables explored in this study is critical to determining whether a candidate is a suitable donor, as numerous contraindications exist to renal transplant donation.3,14,15 Known relative contraindications include: obesity (>30–40 kg/m), hypertension, diabetes mellitus, and active chronic infections (e.g., TB, parasites, Hep B/C). Known absolute contraindications include: bilateral renal calculi, renal artery stenosis, bilateral angiomyolipomas, active malignancy, systemic disease (e.g., fibromuscular dysplasia), severe cardiopulmonary disease, and glomerular pathology. Imaging can be the first investigation to identify a variety of contraindications listed above, which would exclude a patient from donation.
The results of this study are concordant with the findings of numerous publications that have investigated whether structured templates provide superior evaluation of imaging studies. Flusberg et al. compared free-text with a structured LI-RADS (liver imaging reporting and data system) template reporting for evaluating hepatocellular carcinoma (HCC). 16 The authors found that structured reports significantly improved communication of all major HCC features and resulted in consistent reporting of the final LI-RADS category. Nörenberg et al. investigated the effect of structured reporting for primary rectal cancer and demonstrated that most key features (9/12 variables) were included in significantly more structured reports than free-text reports. 17 Additionally, the authors revealed that surgeons felt that information extraction was easy in 96% of structured reports, compared to 14% of free-text reports. The benefits of structured reporting have also been demonstrated in a wide range of other disease processes, including pancreatic cancer, 18 prostate cancer, 19 multiple sclerosis, 20 and inherited neuromuscular disorders. 21
Traditional radiology reports, generated through a narrative, non-structured approach, remains the standard practice despite numerous studies revealing that this style of reporting may hinder patients’ receiving optimal care.22-24 A prosaic approach to reporting may leave clinicians wanting clarity, with a study by Bosmans et al. discovering that half of clinicians believe that if a normal feature was not mentioned in a report that the radiologist may not have explicitly examined it. 24 This may result in the clinician either having to spend time re-consulting the radiologist to determine the answer or trying to evaluate the imaging study themselves, which has been shown to result in suboptimal diagnostic accuracy compared to a radiologist’s analysis.25-27
There exist many benefits to structured template reporting, with information being presented in a consistent format and allowing crucial data to be easily extracted.28,29 Using a checklist provides radiologists with a systematic approach to evaluating imaging studies and alleviates the need to remember every key disease feature or crucial surgical planning variable, which can be exceptionally valuable to trainees and junior staff physicians. Many studies surveying clinicians have shown that the majority of referring clinicians and radiologists have a strong preference for structured reporting.23,24,30 Additionally, numerous radiologic societies have begun promoting this style of reporting.31,32 The Radiological Society of North America (RSNA) has, for example, generated an online library of freely accessible reporting templates for a variety of sub-specialties. 33
Though the implementation of standardized templates can be challenging and labor intensive, the results of this study confirm that radiologists at multiple institutions can utilize a standardized template at an excellent rate of compliance and omit significantly fewer critical variables. The creation of an imaging report template should be performed in collaboration with urologists at a renal transplant centre to ensure that radiologists summarize all pertinent findings needed for the preoperative assessment of living renal donors.
One of the limitations of the present study was that the final outcomes of patients undergoing renal transplant, or of the living donors, were not evaluated. Specifically, we did not determine if using information provided by standardized templates led to a reduction in transplant-related complications. However, this would be very challenging to do as there are many variables that can contribute to adverse patient outcomes and, overall, acute complications related to renal donations are low. 34 Another limitation of this study was that the total time required for the radiologist’s interpretation of the findings, pre- and post-template implementation, was not explored due to the retrospective nature of data analysis.
Radiology reports provide accessible, reliable, and indispensable information for our fellow clinicians. However, the variability in reporting styles can confuse readers and inadvertently omit pertinent findings leading to diagnostic dilemmas. This study reveals that the introduction of standardized templates promotes completeness of reports and superior evaluation of potential renal transplant donors, across multiple institutions and a diverse set of radiologists. Through structured reporting, radiologists can reliably provide our surgical colleagues with needed preoperative anatomy and incidental findings, which will help determine suitable transplant donors and reduce potential complications associated with organ retrieval.
Supplemental Material
Supplemental Material - Standardized Reporting on the Preoperative CT Assessment of Potential Living Renal Transplant Donors: Can We Create a Universal Report Standard to Meet the Needs of Transplant Urologists?
Supplemental Material for Standardized Reporting on the Preoperative CT Assessment of Potential Living Renal Transplant Donors: Can We Create a Universal Report Standard to Meet the Needs of Transplant Urologists? by Hadas Benhabib, Priscila Sacilotto Crivellaro, Heba Osman, Senthujan Gunaseelan, Andrew Chung, Jason Y. Lee, Errol Colak, Vincent Leung, Joseph O'Sullivan, Cynthia Walsh, and Ania Kielar in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.