
Abstract
Purpose
Pre-treatment diagnostic magnetic resonance imaging (MRI) is used in prostate cancer detection and staging; however, little is known about its potential for radiotherapy treatment decision, or its prognostic value. We investigated the findings on pre-treatment MRI and its potential influence on treatment decisions, and its ability to predict biochemical recurrence in patients treated with radiotherapy.
Methods
Files of patients treated by radiotherapy from 2014 to 2022 were searched for if they had had an MRI within 12 months before radiotherapy. Prostate Imaging Reporting & Data System (PI-RADS) score, index lesion diameter and the presence of organ confined disease or extra-prostatic extension were correlated with their Cancer of the Prostate Risk Assessment (CAPRA) score. Distribution of radiological and clinical features between groups were estimated using a chi-squared test.
Results
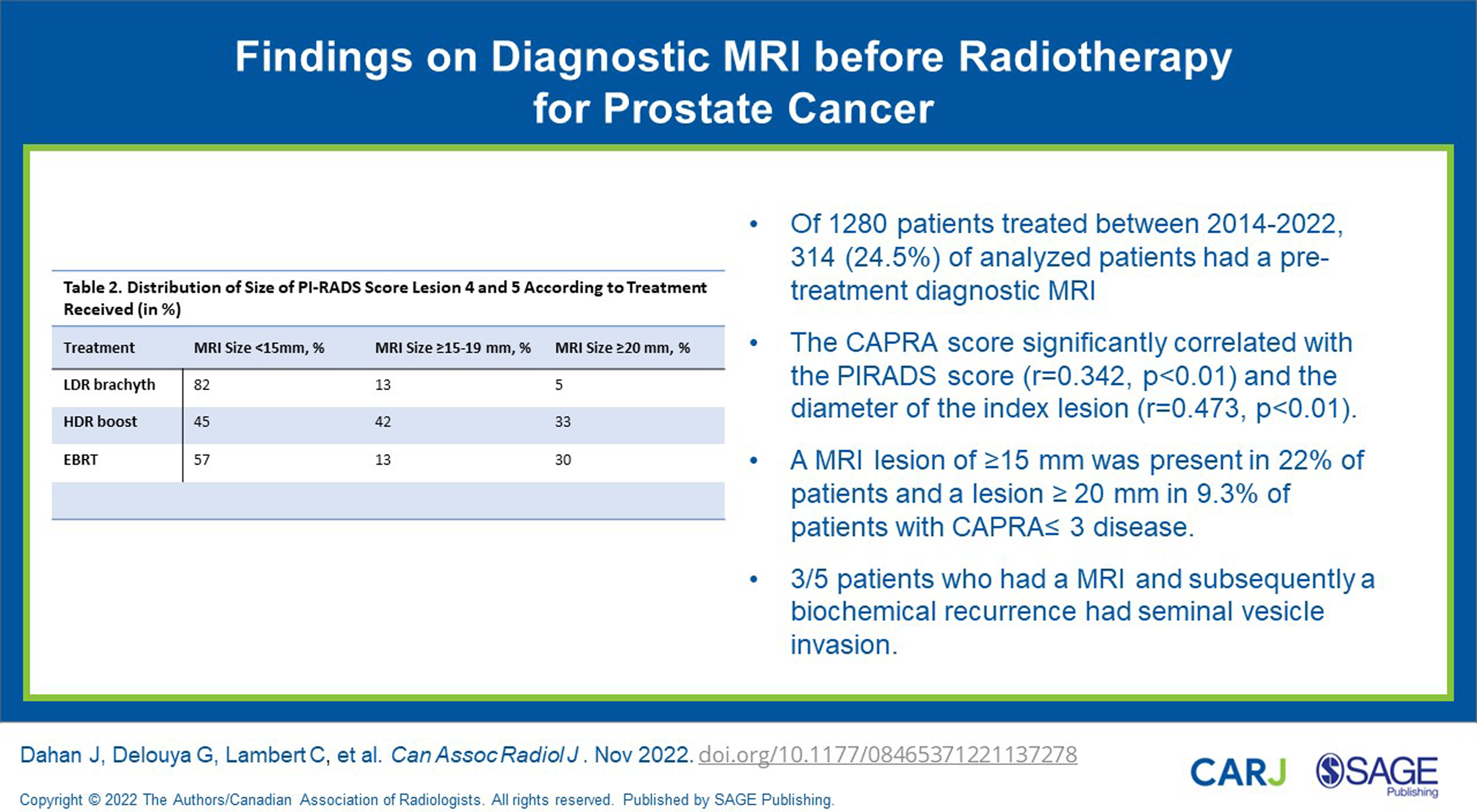
Out of 1280 patients, 314 (24.5%) had an MRI. The distribution depended on the treatment received: 22.5% who received low-dose rate (LDR) brachytherapy as monotherapy, 24.0% treated with high-dose rate (HDR) boost and 32.0% treated with external-beam radiotherapy (EBRT) (P = .017). The CAPRA score significantly correlated with the PI-RADS score (r = .342, P < .01) and the diameter of the index lesion (r = .473, P < .01). A clinically significant number of 22% patients with CAPRA ≤ 3 disease presented with lesions ≥15 mm and were less likely to be treated with LDR monotherapy (P < .01). 39 patients had a recurrence, only 5 had an MRI: 4 had a lesion of ≥20 mm and 3 a seminal vesicle invasion.
Conclusion
More than twenty percent of patients with CAPRA ≤3 presented on MRI a ≥15 mm lesion. An MRI could potentially affect treatment choice, and although exploratory our results suggest an important prognostic potential.
Introduction
Prostate cancer is the leading solid cancer in men in Canada. 1 Multiple studies have shown that magnetic resonance imaging (MRI) has a high sensitivity but low specificity for prostate cancer diagnosis, 2 helping to identify areas at risk of clinically significant cancer. 3 With the recent improvements in MRI, it has been suggested that the use of multiparametric MRIs (mpMRI) should be expanded to cancer detection and monitoring in active surveillance.4,5 Little is known about the influence of MRI in treatment decision and prognosis in radiotherapy for prostate cancer. 6
The Prostate Imaging Reporting and Data System (PI-RADS) score is the most used scoring system to assess clinically significant cancers and standardize imaging acquisition.7 However, prognosis is usually established with clinical and pathological features and not with the MRI. 8 Therefore, literature is still scarce on the added value of an mpMRI for treatment choice and its prognostic value. Indeed, only a few studies have suggested how MRI findings can improve risk stratification when associated with clinical and pathological scores and very few have used a diagnostic MRI in prostate cancer radiotherapy. 9
The aim of our study was to investigate the potential clinical importance of a diagnostic MRI in prostate cancer radiation therapy, its potential role in treatment decisions, and its prognostic significance.
Methods and Material
This is a retrospective study of a prospectively maintained database at our hospital. Institutional Review Board (IRB) approval was obtained for this study (Number 22.011). No signed informed consent was necessary for this study.
Outcomes of Interest
Initially, the main point of interest was to analyse the prognostic significance of an MRI to predict for biochemical recurrence after radiotherapy. Because of the limited follow-up time and the few recurrences, we decided to analyse the prevalence of known factors of aggressiveness on MRI. As such we analysed index lesion diameter, extracapsular extension, or seminal vesicle invasion and its distribution among different treatments and according to known clinical factors of prostate cancer aggressiveness and its potential to influence treatment decision.
Inclusion Criteria
All patients treated between January 2014 and June 2022 with either low-dose rate (LDR) brachytherapy as monotherapy, by External Beam Radiotherapy (EBRT) with or without a combination with high-dose rate (HDR) brachytherapy have been selected for this study. All patients’ files were searched for having had a diagnostic MRI either at our tertiary hospital or in a different facility. A total of 1347 patient files have been reviewed, 388 among them having received a diagnostic MRI.
Exclusion Criteria
Out of the 388 patients having received an MRI, 315 were deemed eligible because they had complete information on prostate volume, Prostate Imaging Reporting and Data System (PI-RADS) score and its localization regarding the capsule. Their MRI was also done not more than 12 months prior to treatment initiation.
MRI
For the purpose of this study, we used the reports of the MRIs done in each centre. No revisions of the MRIs were done. We didn’t record whether patients had a 1.5 T or 3 T MRI performed. In case of multiple MRIs present, the findings of the closest one to the treatment date has been selected. Grading of the MRI: prostate volume and PI-RADS score were recorded. The index lesion was defined as the lesion with the highest PI-RADS score and if several had the same PI-RADS score, the one with the largest diameter was chosen. In very rare cases when there was a lesion erroneously described as PI-RADS 4 but showing extracapsular extension (ECE), this lesion was chosen as the index lesion even in the presence of a larger PI-RADS 5 lesion but without ECE. It was noted if the lesion was in contact with the prostate capsule or if there was clear extension beyond the capsule. Contact with the capsule was, for the purpose of this study, classified as non-organ confined (OC) because of the risk that there might be a microscopic ECE. Such a microscopic ECE would change the clinical stage and the treatment offered.
The length of the extent of the contact was not measured. In the absence of clear mention of a capsular contact or any modification of it, the lesion was assumed to be organ confined. Any contact with the capsule without extension beyond was recorded as ‘capsule contact’; furthermore, presenting clear suspicion of ECE or invasion of the seminal vesicles (SVI) was recorded.
CAPRA Score
In addition to their MRIs, patients’ Cancer of the Prostate Risk Assessment (CAPRA) score based on both clinical and histological parameters such as age at diagnosis, PSA, Gleason score, clinical stage and percent of biopsy cores involved with cancer were calculated. The CAPRA is a score ranging from 0 to 10 and has been validated across multiple treatment approaches to predict the likelihood of metastasis, cancer-specific mortality and overall mortality. 10
Statistical Analysis
Chi-squared test was used to compare distributions between groups. Log-rank test was used with the Kaplan–Meier method to calculate the impact of the PI-RADS score and other MRI features on biochemical (PSA) recurrence. Pearson correlation coefficient was used for correlation of the PI-RADS score, the index lesion diameter and clinical factors. Statistical analysis was performed using SPSS 27.0 for Windows (IBM SPSS, Chicago, IL, USA).
Results
Patient Characteristics.
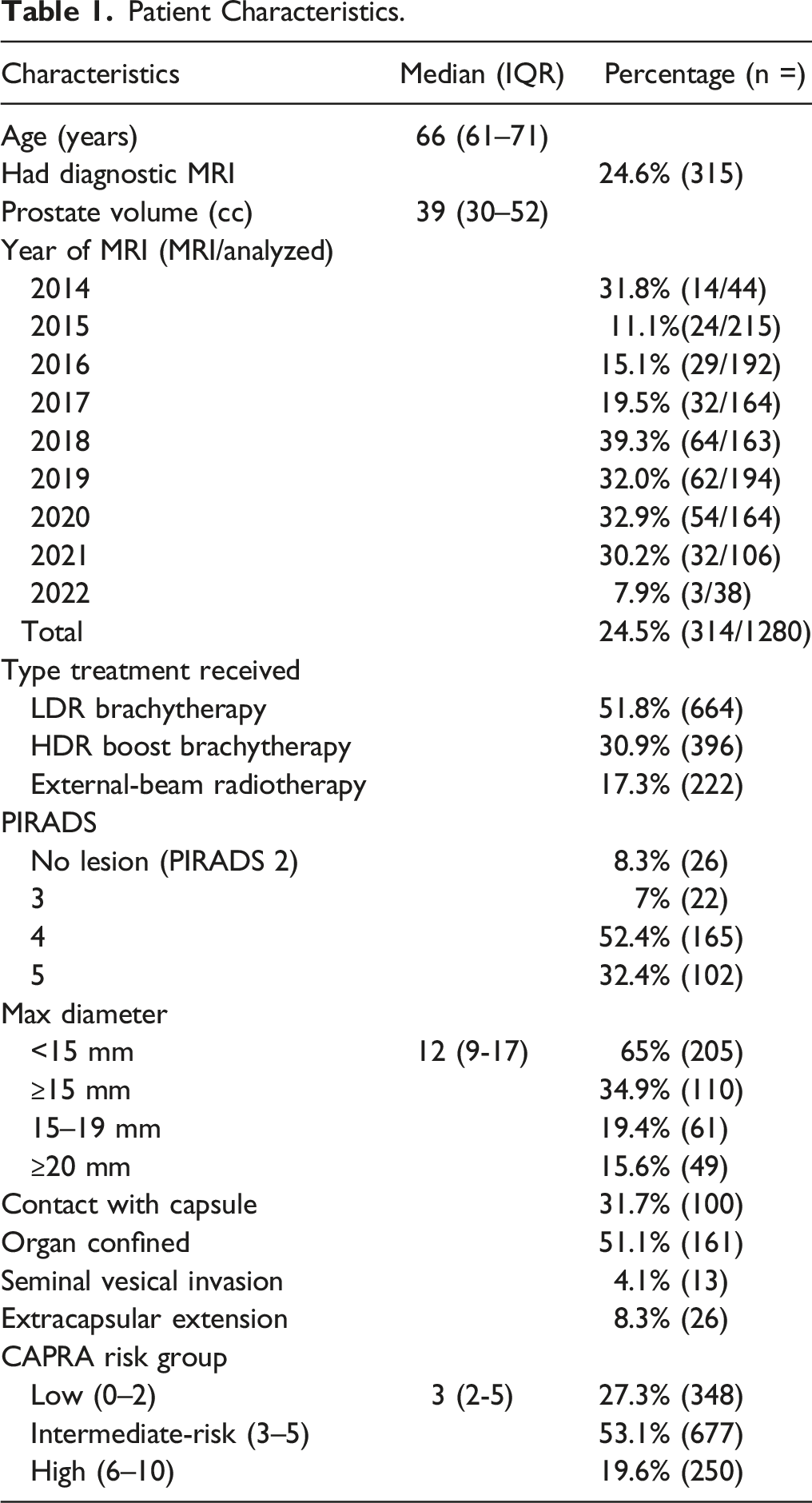
The median maximum diameter of the index lesion was 12 mm (interquartile range, (IQR) 9-17 mm). 102 (32.4%) had a PI-RADS 5 lesion and 165 (52.4%) a PI-RADS 4. A PI-RADS 3 lesion without the presence of a PI-RADS 4 or 5 was seen in 26 (8.3%). Organ confined disease was seen in 161 (51.1%) patients.
The CAPRA score was linearly correlated both with the PI-RADS score (r = .342, P < .01) and the diameter of the index lesion (r = .473, P < .01). The PSA as a continuous variable was correlated with the maximal diameter (r = .418, P < .01) and PI-RADS score (r = .245, P < .01) and the Gleason score with maximal diameter (r = .343, P < .01 diameter and the PI-RADS score (r = .293, P < .01).
Distribution of Size of PI-RADS Score Lesion 4 and 5 According to Treatment Received (in %).

*Chi square test.
Distribution of Relationship With Prostate Capsule According to Treatment Received (in %).
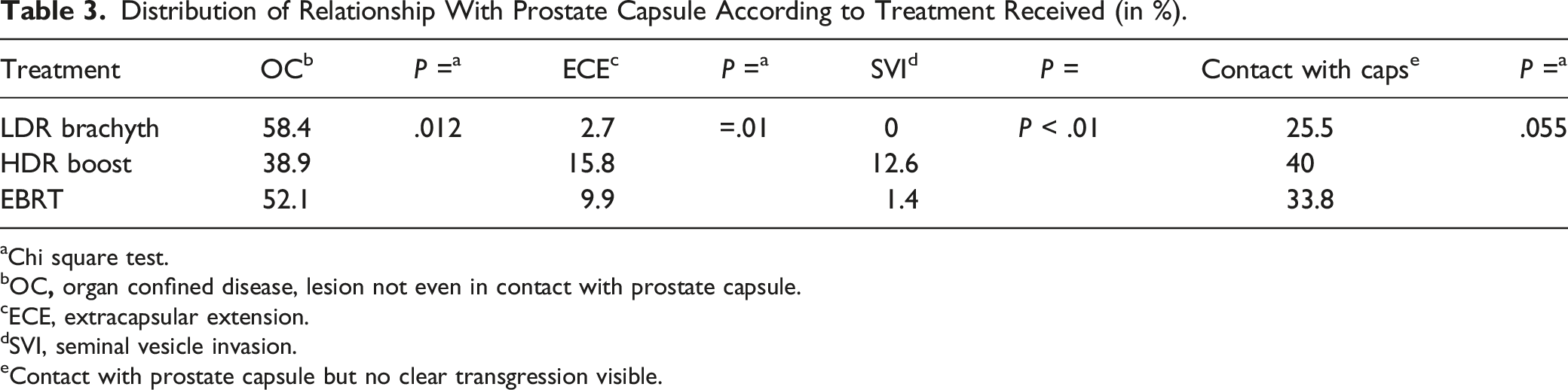
aChi square test.
bOC
cECE, extracapsular extension.
dSVI, seminal vesicle invasion.
eContact with prostate capsule but no clear transgression visible.
Distribution of Aggressive MRI Features According to CAPRA Score (in %).

aChi square test.
Distribution of Relationship With Prostate Capsule on MRI According to CAPRA Score (in %).
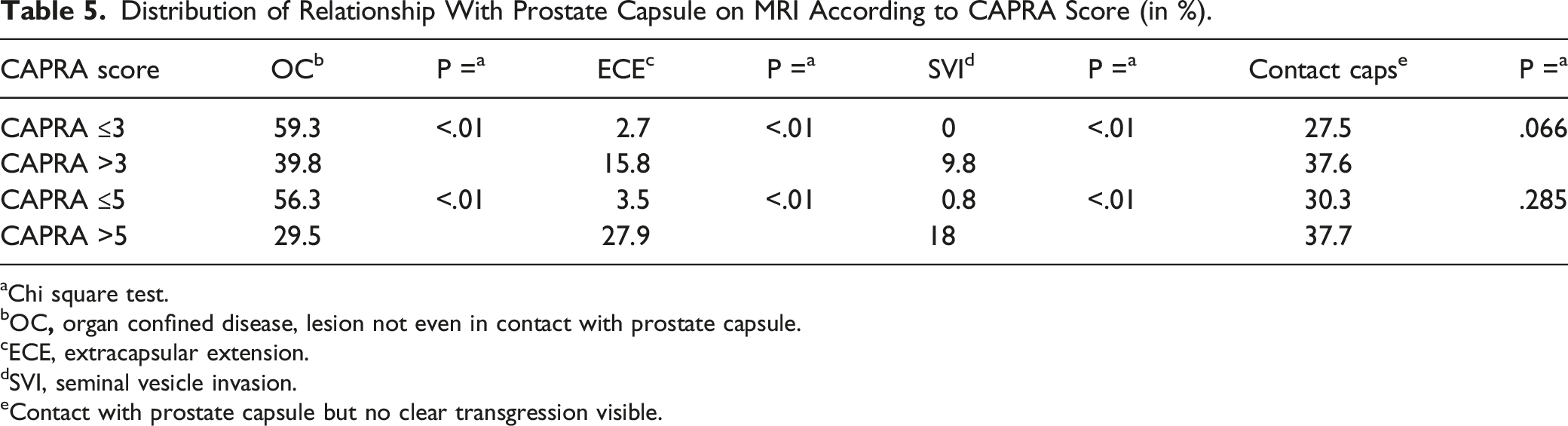
aChi square test.
bOC
cECE, extracapsular extension.
dSVI, seminal vesicle invasion.
eContact with prostate capsule but no clear transgression visible.
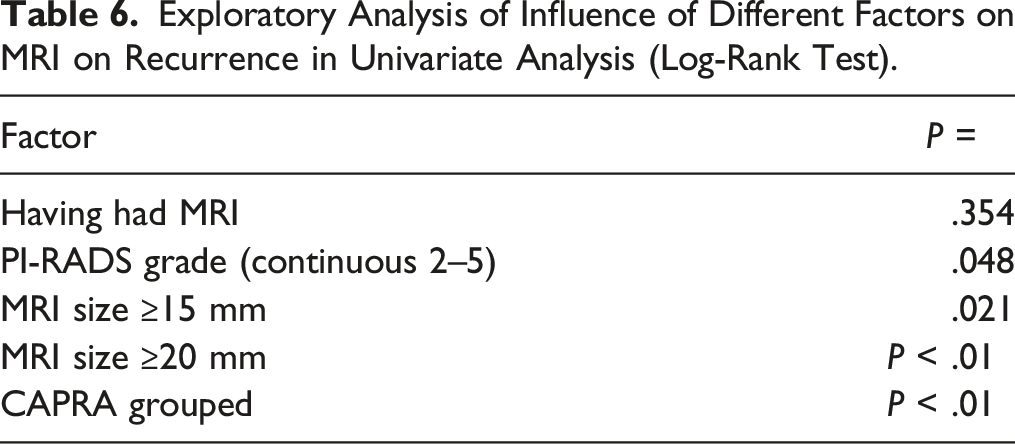
Exploratory Analysis of Influence of Different Factors on MRI on Recurrence in Univariate Analysis (Log-Rank Test).
Discussion
We found that nearly a quarter of patients treated with radiotherapy had an MRI before treatment. The frequency of these MRIs increased in the last years. About 20% of patients with either low-risk or lower tier intermediate risk cancers (CAPRA ≤3) presented with a lesion of ≥15 mm and therefore had a dominant intra-prostatic lesion (DIL) that could benefit from an intraprostatic boost. A lesion of >15 mm has been associated with a higher risk of ECE 11 and a higher risk of biochemical (PSA) failure. 12 Such a lesion was even more frequent at 27% in patients with a Capra ≤5 (lower to unfavourable intermediate risk cancers).
MRIs were done for various reasons, mostly to guide a diagnostic biopsy or to decide whether patients needed active treatment or could benefit from active surveillance. This certainly introduced a selection bias into our cohort. Nevertheless, we believe that the clinical impact of our findings is that a diagnostic MRI before treatment could guide treatment decision. Patients with larger lesions could benefit from intraprostatic dose-escalation either through EBRT 13 or by a brachytherapy boost. It has been shown that pre-treatment PI-RADS 4-5 DILs are at an increased risk for intraprostatic recurrence on biopsy after SBRT. 14 It is possible that the diagnostic MRI changed our treatment decisions. Lesion size is a predictor of ECE and correlates with Gleason score ≥7. 15 We believe that the fact that 31% of patients with a CAPRA score of 3, which is the institutional limit for a LDR brachytherapy, had a lesion measuring ≥15 mm but only 18% of patients treated with LDR brachytherapy had a lesion that was ≥15 mm points towards a bias in choosing patients with more favourable MRI for LDR brachytherapy. Another potential bias in treatment decisions might be that patients with a larger index volumes lesion (≥15 mm or 20 mm) or who presented lesions closer to the capsule were treated less often with LDR but more frequently with HDR boost or EBRT monotherapy.
Not only can the MRI characterize aggressiveness, but it has been shown to also be of prognostic significance in addition to clinic-pathological features such as PSA and Gleason score. Higher PI-RADS-scores have been shown to be independently associated with a higher risk of metastasis and lower cancer-specific survival independently of treatment type and other clinical–pathologic features. 16 Another important prognostic information gained from MRI is simply based on whether a lesion is visible or not. Visible lesions have an increased risk of developing metastasis and prostate cancer death by over ten times compared to invisible lesions. 16 Jambor et al. 17 demonstrated that MRI in combination with clinical variables and biopsy had the best predictive value for biochemical recurrence after prostatectomy. The relative volume of the lesion on MRI compared to the overall prostate volume had a better prognostic value that the PI-RADS score and was similar in value to the genetic Decipher score.
In our exploratory analysis, limited by the fact that only 5 patients with a recurrence had a diagnostic MRI, we found that larger index tumour lesion and PI-RADS score have a higher risk of recurrence, especially patients with SVI. In our study, the 5 patients who had diagnostic MRI and later developed a recurrence, 3 patients had SVI.
However, MRI staging is not always accurate. Wibmer et al. 18 found that extracapsular extension on MRI overestimated the true extension at prostatectomy. However, even with this discordance between MRI and the histopathologic specimen, imaging still provided added value to the prognosis. In fact, patients with ECE on MRI, but organ confined disease on the prostatectomy specimen, presented worse oncologic outcomes than patients who had OC both on MRI and on pathology. 18 The size of the lesion on MRI has been shown to have prognostic significance. Parsons and Hutten et al.19,20 found in two studies from the same centre that the cut-off for a lesion on MRI for increased biochemical (PSA) failure was ≥22-23 mm while Kauffmann et al. 12 found that lesions >15 mm were associated with a higher risk of failure.
Previous studies on MRI in prostate cancer radiotherapy have shown the importance of pre-treatment MRI to identify the DIL as it is the most common site of recurrence after prostate radiation. 14 Indeed, Pucar et al. 21 demonstrated that the site of recurrence of their patients who had received radiation therapy was in all cases the site of the primary tumour identified by MRI pre-treatment. Furthermore, it has also been shown by the phase III of the FLAME trial, that local control specifically targeting the DIL with radiation boost can significantly reduce the risk of biochemical (PSA) recurrence. This risk of recurrence has been shown to be higher in PI-RADS 4 or 5 lesions. 14 This demonstrates the relevance of our study, and the impact diagnostic MRI pre-treatment could have on treatment planning and prediction of possible disease progression. The question if an MRI can lead to overtreatment is as important as the question if a pre-biopsy MRI could lead to overtreatment of cancers.22,23
Our study has some limitations. Since we used the files of patients that were treated, it was somehow expected to find more clinically significant lesions than in a population of patients on active surveillance or before a diagnostic biopsy. This explains the high prevalence of larger PI-RADS 4-5 lesions. Also, a relatively low recurrence rate can be noted because of the short follow-up period and the usage of MRI only increasing within the last 5 years. There is undeniably a source of inter-observer variability because of various readers with different experience and lack of standardization or peer-validation of the MRI reports. A review of all MRIs was not possible. Additionally, there is a learning curve over the years analysed and we used MRI reports from different centres, tertiary and not, with a non-uniform sequencing and different MRI machines. Furthermore, the large number of cancers with contact to the capsule could be an underestimation because radiologist didn’t routinely describe whether there is contact with the capsule or not. Furthermore, a few PI-RADS 3 lesion could have shown high-grade cancers been cancerous or weren’t even mentioned in the MRI report. And not all PIARS 4 or 5 lesions correspond to prostate cancer on biopsy. 24 This could have under- or over-estimated the presence of clinically significant lesions.
Conclusion
We showed that more than 20% of patients treated for cancer with relatively low aggressiveness (CAPRA ≤3) presented with unexpectedly large PI-RADS 4 and 5 lesions measuring ≥15 mm. An MRI could potentially affect treatment choice, as larger index volumes and higher PI-RADS scored lesions were less often treated with LDR brachytherapy. Even though exploratory, our results suggest that MRI findings have an important prognostic potential.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JD was supported by an educational grant from the Department of Radiology of Université de Montréal.