
Abstract

Introduction
Head and neck cancer is the sixth most common malignancy worldwide, with an estimated 450 000 deaths annually.1,2 A key prognostic marker is tumour stage at diagnosis, 3 making early detection essential to better patient outcomes.
Patients are usually diagnosed when the primary tumour or metastatic cervical lymphadenopathy becomes clinically evident. 3 However, given the large volume of imaging studies performed for non-specific symptoms relatively early in the disease process, we believe that some head and neck tumours may be identifiable earlier. Unfortunately, these are not always identified. Understanding where diagnostic errors most commonly arise could help radiologists improve detection.
Materials and Methods
Ethics approval was obtained for a retrospective review of a regional head and neck cancer database over a 5-year period from May 2009 to April 2014. For all patients with a subsequent cancer diagnosis during that period, all prior computed tomography (CT) and magnetic resonance (MR) imaging studies were reviewed to determine if the diagnosis could have been made at an earlier time.
Total Perceptual and Interpretative Errors by Tumour Location and Imaging Modality.
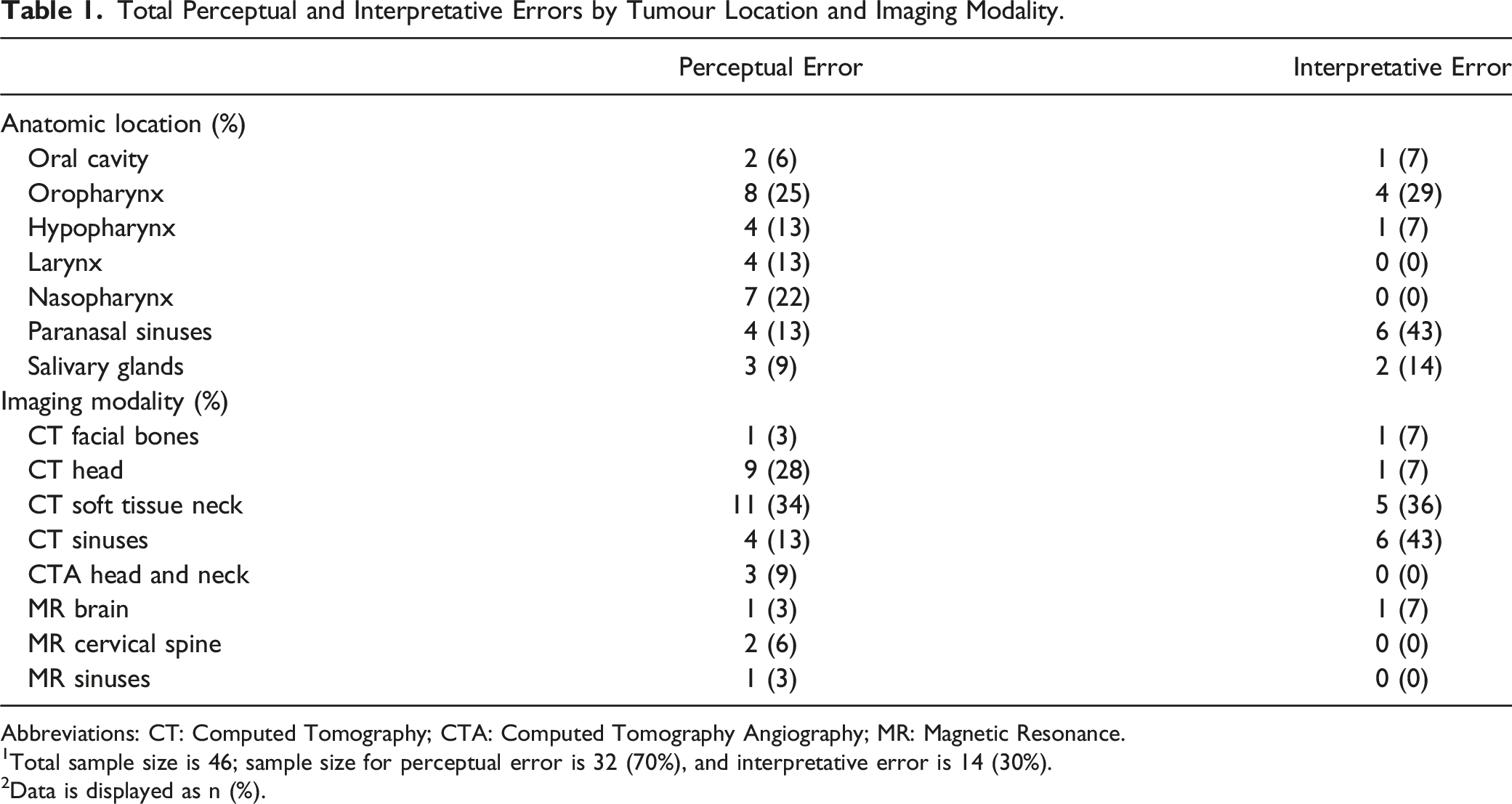
Abbreviations: CT: Computed Tomography; CTA: Computed Tomography Angiography; MR: Magnetic Resonance.
1Total sample size is 46; sample size for perceptual error is 32 (70%), and interpretative error is 14 (30%).
2Data is displayed as n (%).
Results
1196 patients were diagnosed with head and neck cancer over 5 years. In 46 cases (4%; 95% CI, 3%–6%), there was an earlier CT or MR imaging study on which the cancer was clearly evident (in retrospect) but was missed (32 cases, 70%) or misinterpreted (14 cases, 30%) at the time (Table 1).
The provided histories correctly indicated a concern for malignancy (but were ignored or dismissed by the radiologist) in 17 of 46 cases (37%). Potentially misleading histories suggesting infection or inflammation were present in 13 of 46 cases (28%).
The median delay to diagnosis was 153 days.
Discussion
We found that there was an opportunity to make a diagnosis of head and neck cancer on an earlier CT or MR imaging study in 4% of cases. Most (70%) errors were misses, which aligns with prior general radiology studies that have attributed 60–80% to perceptual errors.4,5 Unfortunately, perceptual errors plague both experienced and novice readers and can be due to a variety of factors such as high-work volumes, reader fatigue, and work-place distractions.4,5 General awareness of commonly missed cancer locations may help influence radiologists to perform a secondary review of possible blind spots. For example, on plain CT heads, many of the missed tumours were in the nasopharynx or salivary glands, which are in the peripheral field of view and are likely not scrutinized to the same degree as the brain parenchyma (Figure 1). 35-year-old male with a provided history of “subacute cranial nerve V deficits with associated right-sided facial muscle wasting.” The non-enhanced CT head study was interpreted as “no acute intracranial pathology.” A) Axial image below the skull base demonstrates asymmetric muscle atrophy (yellow triangle), as well as a soft tissue mass in the nasopharyngeal and prevertebral soft tissues (star). B) Axial image at the level of the skull base shows extension of the soft tissue lesion through the sphenopalatine foramen into the pterygopalatine fossa, and through the skull base at the foramen lacerum (arrowheads). C) Axial image at the level of the orbits demonstrates gross extension of tumour into the right orbital apex (arrow) and right middle cranial fossa (yellow circle).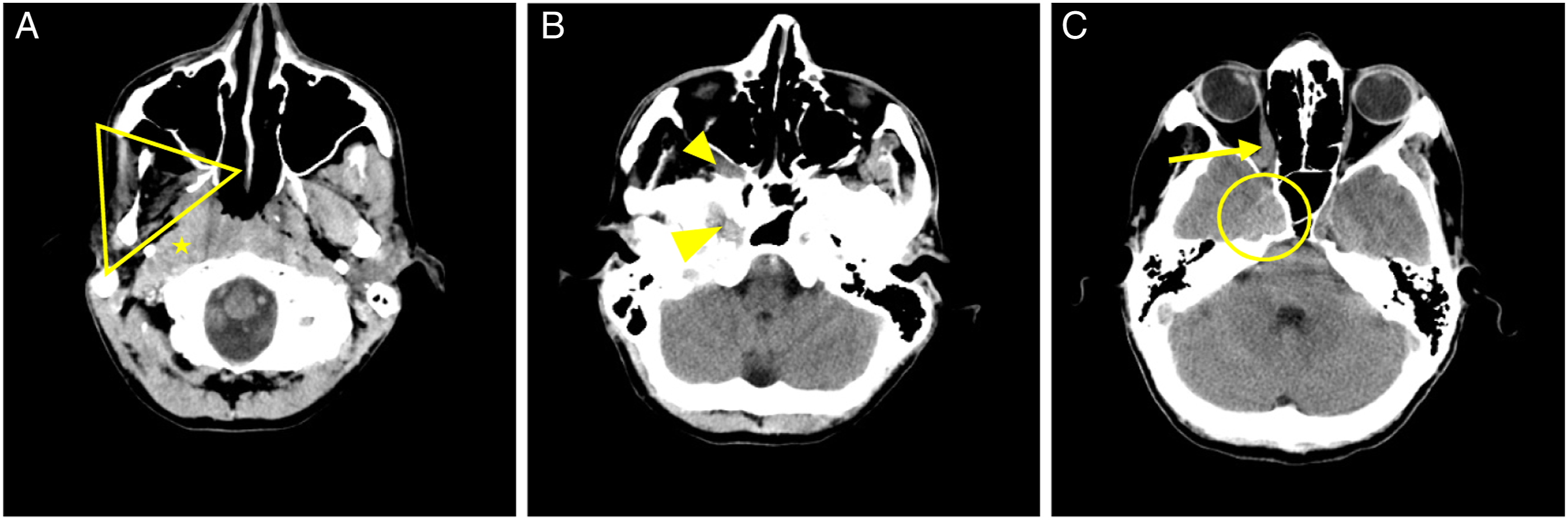
Interpretative errors are affected by various cognitive biases such as the framing bias acquired from clinical history.
4
We found this to be a particular problem for CT sinus studies, where a history of chronic sinusitis was provided, and a tumour was misinterpreted as a benign inflammatory polyp in the majority of cases. In these cases, there was clear evidence of osseous destruction or invasion of adjacent structures (Figure 2), which should raise the alarm for more aggressive pathologies. 39-year-old male with a provided history of “chronic maxillary sinusitis.” The non-enhanced CT sinuses study was interpreted as “compatible with a large polyp in the setting of chronic inflammatory disease.” A) Axial bone algorithm image through the superior nasal cavity reveals destruction of the nasal septum (arrowhead). B) Axial soft tissue algorithm image at the same level shows an expansile soft tissue mass centered in the nasal cavity with extension into the right maxillary sinus (white circle). C) Coronal image through this expansile mass demonstrates osseous destruction of the palate (arrow) with extension of the lesion into the oral cavity.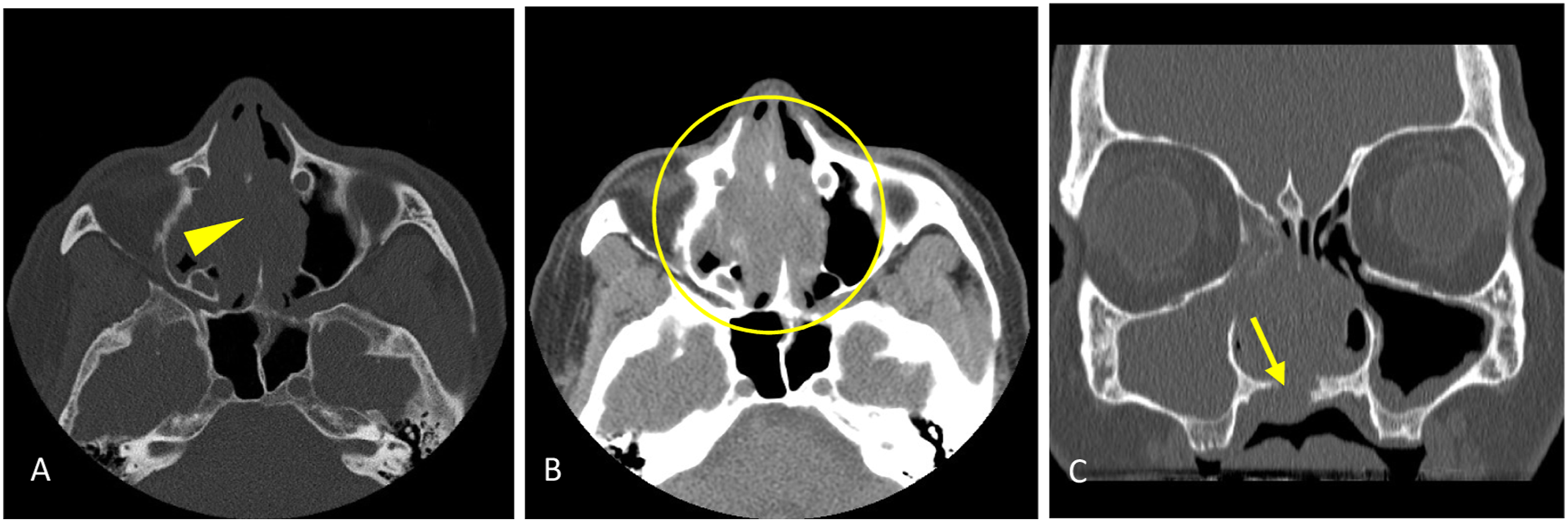
Our study is limited due to its retrospective and descriptive nature. However, we were able to identify some repeated blind spots, the knowledge of which is a good first step toward improving radiological accuracy. Given the median delay to diagnosis of approximately 5 months, there is a good opportunity to make meaningfully earlier diagnoses in these cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.