
Abstract
Introduction
Magnetic resonance imaging (MRI) is increasingly used as a primary modality for imaging sacroiliitis in patients with inflammatory spondyloarthropathy due to its high sensitivity for evaluating inflammatory and chronic structural changes in the sacroiliac joint (SIJ). 1 MRI of the SIJs can confirm the diagnosis of sacroiliitis when there is clinical suspicion and can be used to follow known sacroiliitis, including treatment response. 2
The typical progression of imaging findings of sacroiliitis begins with active inflammation (manifested by bone marrow edema [BME]), followed by a mixed stage of structural changes (subchondral sclerosis, erosions, joint space narrowing, and ankylosis) simultaneously present with active inflammation, and finally structural changes without active inflammation in later stages of disease. 3 Although nonspecific, periarticular fatty infiltration is also suggestive of chronic sacroiliitis. 3
At our large academic rheumatology tertiary referral center, we have observed that patients with chronic sacroiliitis may have linear low signal in the subchondral bone parallel to the subchondral plate on MRI. We hypothesize that potential etiologies of this sign include the joining of scarred bases of clustered/adjacent chronic erosions vs sclerosis reactive to subjacent inflammation, in either case producing a low signal subchondral band. The appearance is not unlike a fracture line and is currently not described in the literature to the best of our knowledge. We propose that this line be called the “parallel line sign” (PLS). We define it as a vertically oriented line of low signal on both T1-weighted and fluid-sensitive sequences, at least 1 cm long, parallel to and within 2 cm of the SIJ.
The purpose of this study is to demonstrate the existence of the PLS on MRI examinations and determine its prevalence, characteristics, and associations.
Methods
Study Participants
Approval from the Institutional Review Board was obtained and in keeping with the policies for a retrospective review, informed consent was not required. We estimated the prevalence of the PLS at 10% of subjects having chronic sacroiliitis. In order to achieve statistical significance, a desired sample size of at least n = 159 for this descriptive study of a dichotomous variable was determined using an online calculator.4,5
A total of 200 consecutive subjects were included following a retrospective search of the imaging database (Agfa Healthcare, Belgium) for all relevant MRI examinations at our tertiary rheumatology referral center between January 1, 2018 and December 30, 2019. Searches were filtered by modality (MR and MRI), referring department (rheumatology) and procedure name (MR SI joint and MR SI joints). Subjects were excluded if they had MRI examinations that were referred by physicians other than rheumatologists
Electronic medical records (PowerChart, Cerner Corporation Inc, USA) were reviewed to obtain demographic information (age and sex) and clinical history (HLA-B27 status and clinical diagnosis, including ankylosing spondylitis, psoriatic arthritis, reactive arthritis, enteropathic arthritis, juvenile idiopathic arthritis, osteoarthritis, rheumatoid arthritis, and uncertain).
MRI Examinations
Each subject underwent an unenhanced MRI examination of the SIJs with all 200 examinations performed using one of two 1.5 T Siemens Aera MR scanners. Combined spine and body matrix coils were used in all cases. Field of view was 280 mm. All studies included TSE T1-weighted (TR/TE 581/10, two averages, matrix: 448 x 336, turbofactor 4, 84 echotrains/slice) and inversion recovery (TR/TE/TI, 4000/38/160, one average, matrix: 256 × 256, turbo factor 8, 56 echotrains/slice, flip angle 150°) sequences. Slice thickness was 4 mm with no gap, for both sequences. All subjects had these sequences in the oblique coronal plane, parallel to the sacrum. Approximately 30% of subjects had the same sequences repeated in the oblique axial plane, perpendicular to the sacrum.
MRI Review
Variable abstraction.
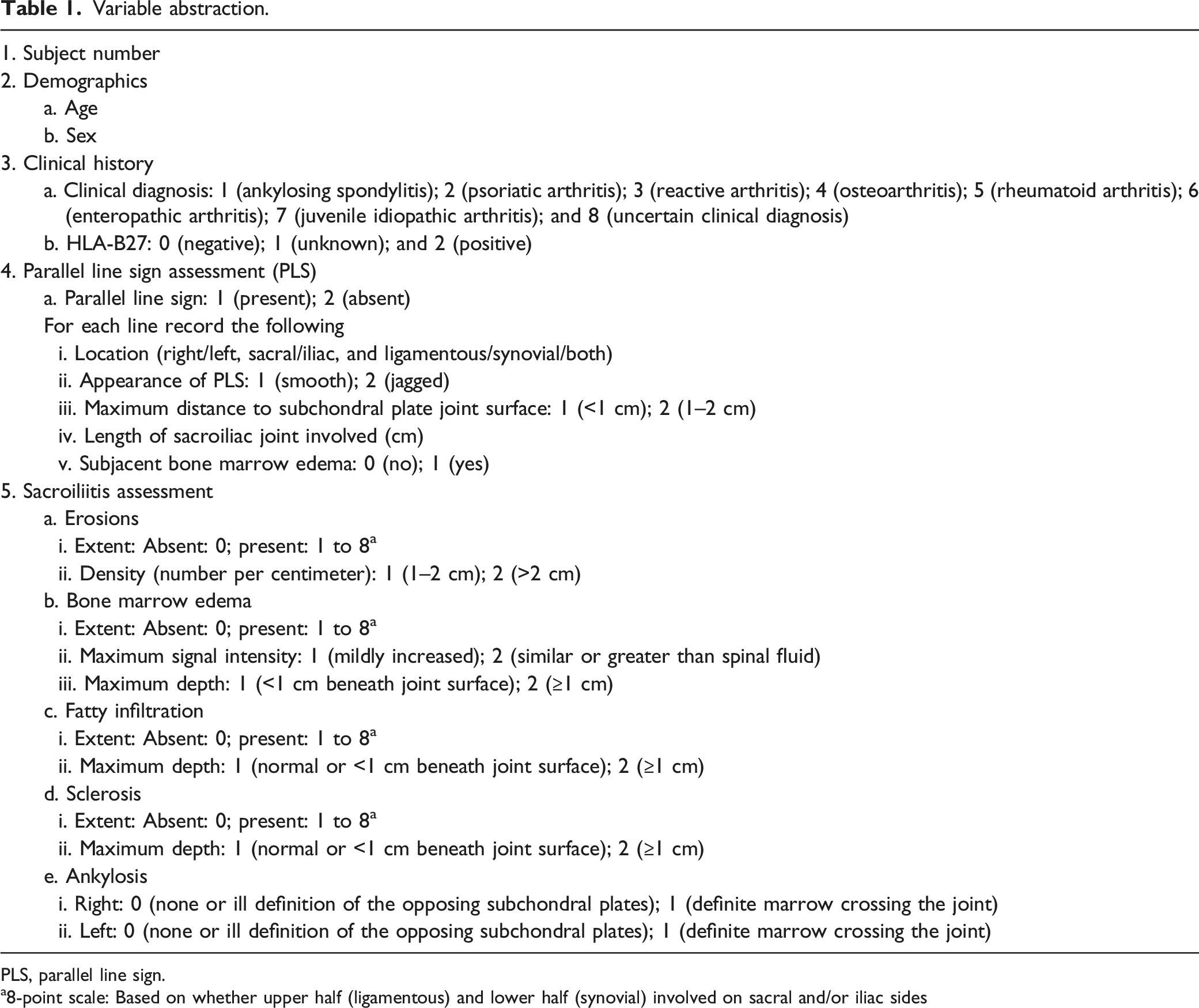
PLS, parallel line sign.
a8-point scale: Based on whether upper half (ligamentous) and lower half (synovial) involved on sacral and/or iliac sides
For evaluation of sacroiliitis, imaging features of acute inflammation (BME) and chronic changes (erosions, fatty infiltration, sclerosis, and ankylosis) were analyzed using the definitions developed by the Canada-Denmark Working Group3,6–9 (T.L.M. and S.R.). To quantify the extent of SIJ involvement by BME, erosions, fatty infiltration, and sclerosis, an 8-point scale was used based on the number of quadrants of each SIJ involved (i.e., 8 separate quadrants per subject including the ligamentous and synovial halves of the sacral and iliac sides of both right and left SIJs). If erosions were present, the density of erosions was recorded as either 1–2 erosions per centimeter or more than 2 erosions per centimeter. If BME was present, its maximal signal intensity (either less than that of spinal fluid vs similar or greater than spinal fluid) and maximum depth of involvement (within or beyond 1 cm beneath the joint surface) were recorded. Similarly, if periarticular fatty infiltration and sclerosis were present, the maximum depth of involvement was recorded (within or beyond 1 cm beneath the joint surface). Ankylosis was defined as complete joint space loss with definite bone marrow fat crossing the SIJ. When more than one quadrant of the SIJs was involved by a feature of sacroiliitis, the quadrant with the numerically largest instance of the feature was recorded for that case.
Statistical Analysis
Descriptive statistics were recorded as percentages and means with standard deviations. Statistical comparisons were made with the chi-squared test for categorical variables and the independent samples t test for continuous variables using SPSS (version 25.0, 2017, IBM, Armonk, NY). Statistical significance was defined as P < .05.
Results
Prevalence and Demographic Associations of the Parallel Line Sign ( Table 2 )
Baseline characteristics of the study population.
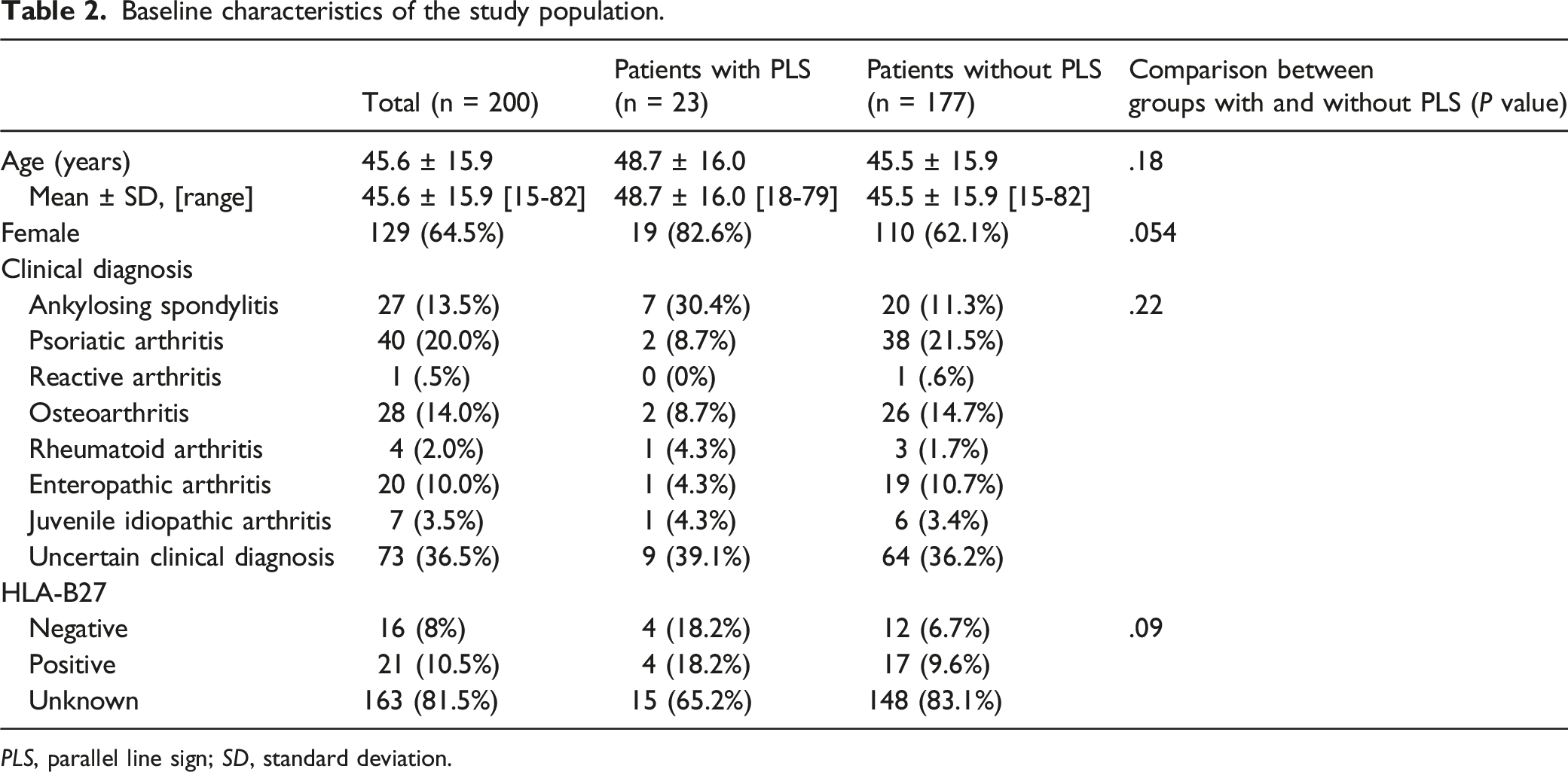
PLS, parallel line sign; SD, standard deviation.
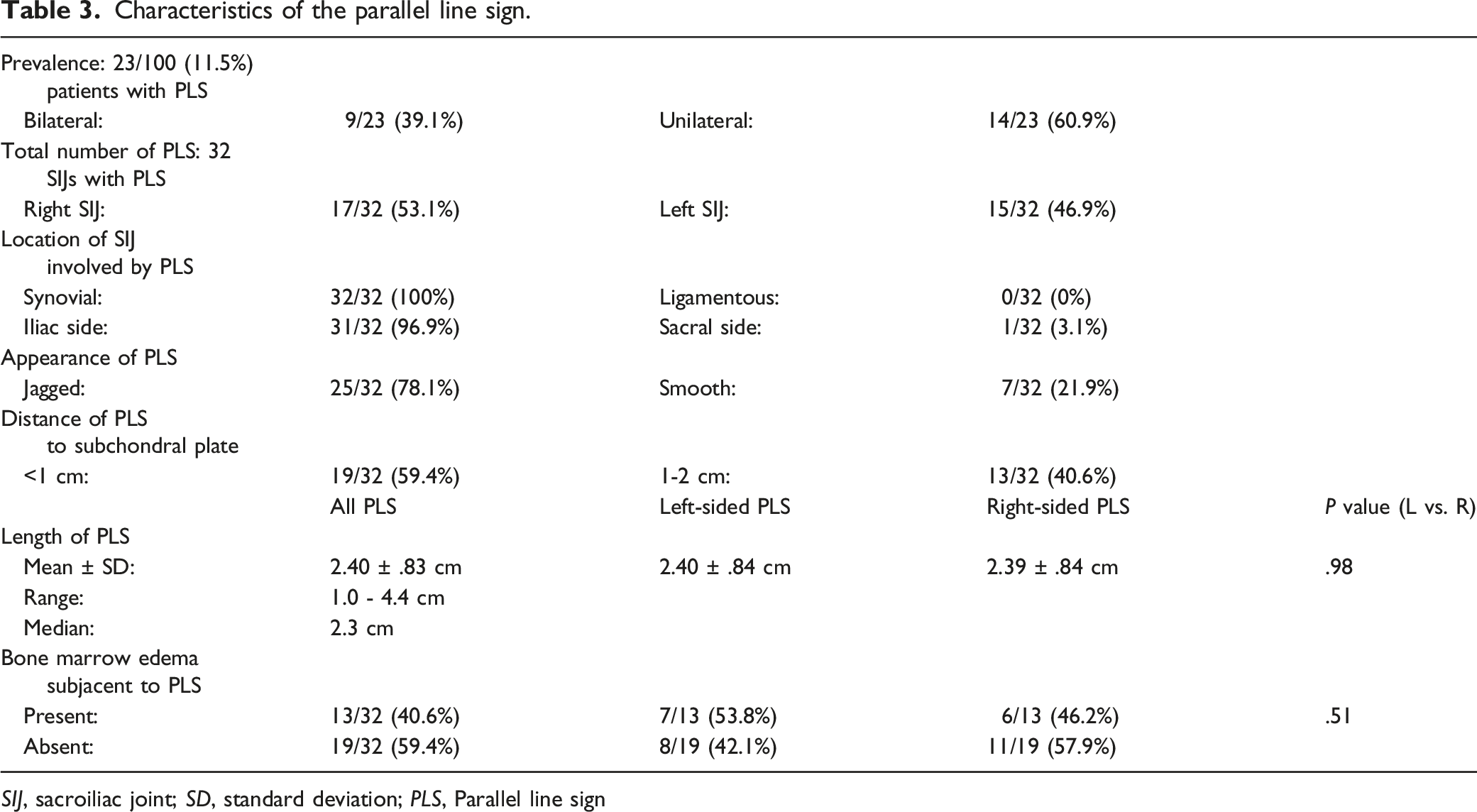
Characteristics of the Parallel Line Sign ( Table 3 )
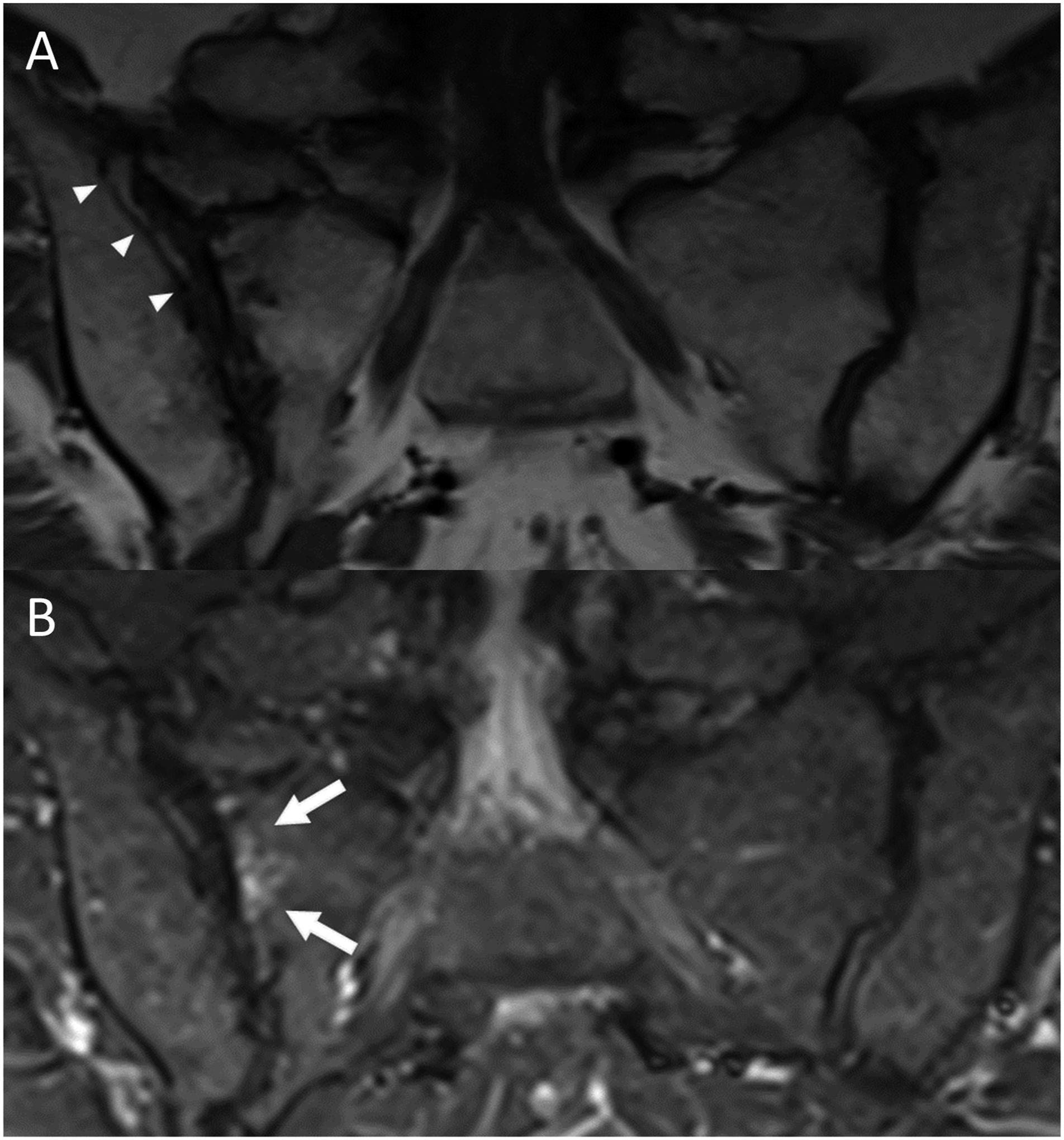
Every PLS involved the synovial (rather than ligamentous) portion of the SIJ. All but one PLS involved the iliac (rather than sacral) side of the SIJ. Over three quarters of the lines appeared jagged (Figure 1), while the remainder had a smooth appearance (Figure 2). The mean length of the PLS was 2.4 ± .8 cm (range 1.0–4.4 cm and median 2.3 cm), with no significant difference in length between left- and right-sided lines. Regarding distance of the PLS to the subchondral plate, approximately 60% of the lines were within 1 cm, with the remainder between 1 and 2 cm of the subchondral plate. Approximately 40% of instances of the PLS had subjacent BME, with no significant difference in the presence of BME between left- and right-sided lines. 57-year-old HLA-B27 negative and RF negative female with 3 years of progressive lower back and buttock pain, referred by rheumatology for query sacroiliitis. ( 80-year-old female with mechanical back pain, referred by rheumatology for query sacroiliitis. (A) Coronal T1-weighted MR image of the sacroiliac joints demonstrate diffuse bilateral subchondral plate irregularity with multiple erosions, more prominent on the right, reflecting chronic sacroiliitis. There is a smooth iliac-sided parallel line sign on the right (arrowheads). Mild right sacral periarticular fat deposition was also present (not shown). (B) Coronal inversion recovery image demonstrates mild periarticular edema involving the sacral side of the superior right sacroiliac joint suggesting active inflammation (arrows). Characteristics of the parallel line sign. SIJ, sacroiliac joint; SD, standard deviation; PLS, Parallel line sign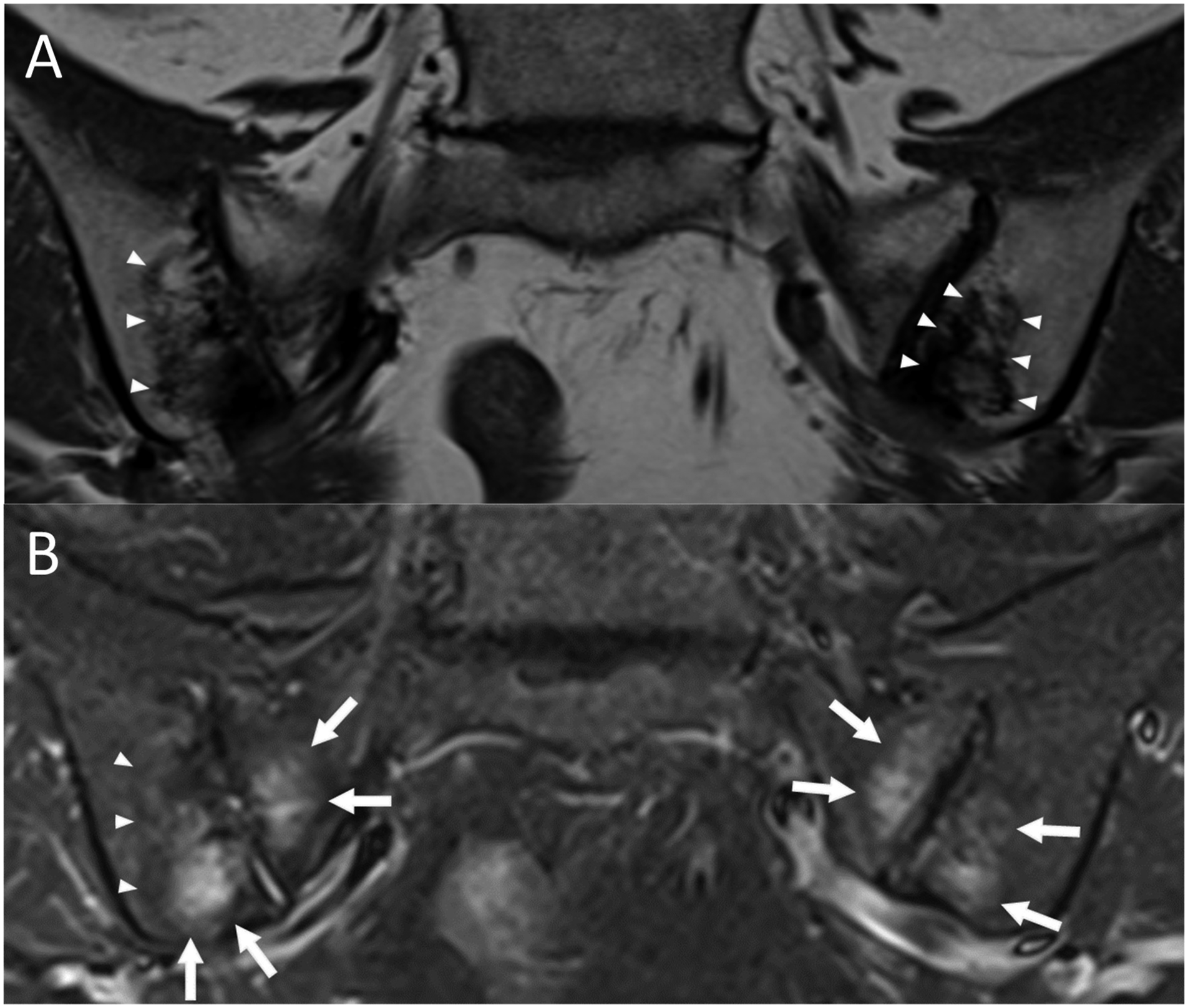
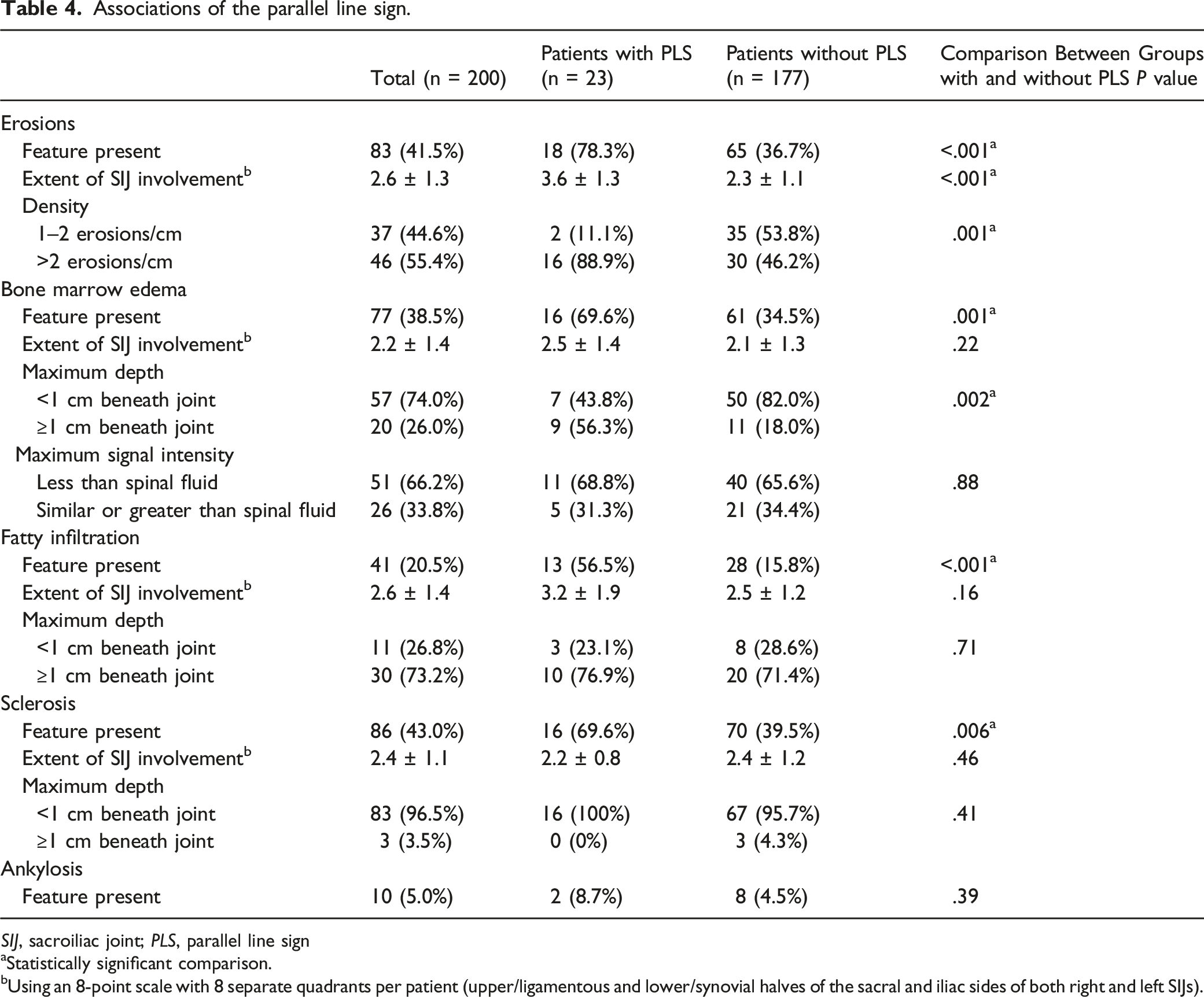
Imaging Associations of the Parallel Line Sign ( Table 4 )
Associations of the parallel line sign.
SIJ, sacroiliac joint; PLS, parallel line sign
aStatistically significant comparison.
bUsing an 8-point scale with 8 separate quadrants per patient (upper/ligamentous and lower/synovial halves of the sacral and iliac sides of both right and left SIJs).
Prevalence of erosions, BME, fatty infiltration, and sclerosis were each significantly greater in those with PLS than those without the sign; however, there was no significant difference in prevalence of ankylosis between the two groups. With respect to erosions, the presence of PLS was associated with greater extent of SIJ involvement by erosions as well as a higher density of erosions per centimeter, compared to those without the PLS.
While prevalence of BME, fatty infiltration, and sclerosis was higher in those with PLS compared to those without PLS, the extent of SIJ involvement by any of these features was not significantly different between the two groups. Maximum depth of BME was significantly greater in those with PLS than those without PLS, but there was no significant difference in maximum signal intensity of BME. There was no significant difference in maximum depth of fatty infiltration or maximum depth of sclerosis between those with and without the PLS.
Discussion
This study shows that low signal lines subjacent and parallel to the subchondral plate of the SIJ are an occasional finding in patients referred for MRI of the SIJ by rheumatologists at our center. We propose that these lines be called the parallel line sign (PLS). These lines were only found in the presence of at least one established MR finding of sacroiliitis and were almost exclusively associated with chronic structural manifestations of sacroiliitis. The PLS was associated with a greater prevalence, extent, and density of erosions as well as a higher prevalence of BME, fatty infiltration, and sclerosis. The sign was almost always seen on the iliac side of the SIJ.
Our data suggest the PLS is usually a manifestation of chronic sacroiliitis given its association with established chronic findings of sacroiliitis, in particular erosions, sclerosis, and fatty infiltration. Most instances of the PLS occurred with both acute and chronic manifestations of sacroiliitis, while a third occurred with manifestations of chronic disease alone. Only one subject with bilateral PLS had active inflammation solely without any chronic changes. Of note, the proportion of females and average age of our study participants exceeded the general population in our region (64.5% compared to 51.4% and 45.6 years compared to 40.9 years, respectively 10 ).
One possible mechanism explaining the formation of the PLS is coalescence of scarred subchondral erosions within healing segments of sacroiliitis. Supporting this theory is the correlation with prevalence, extent, and density of erosions. Predominance of iliac-sided involvement fits with predominance of erosions on the iliac side of the joint in sacroiliitis due to thicker articular cartilage on the sacral side of the joint. 11 Also, distance of the PLS to the subchondral plate was found to be similar to the usual depth of subchondral erosions.
Another potential etiology for the PLS is sclerosis reactive to subjacent inflammation. In one case of bilateral PLS, there were no manifestations of sacroiliitis other than BME, leaving no other explanation evident on MRI. The prevalence of BME was significantly higher is subjects with the PLS compared to those without. Subjacent BME was common in the presence of the PLS, seen in 40% of instances. In these cases, the PLS appeared to marginate the BME (Figure 1). On the other hand, there was no correlation between intensity of BME and the presence of a PLS.
Anecdotally, we observed study cases with a mixture of erosions and dark lines shorter than those included in our definition of the PLS, suggesting that a forme fruste of the PLS may exist (Figure 3). We have also anecdotally observed, in patients outside of the study, a multitude of prominent PLSs subjacent to chronic sacroiliitis without ankylosis in one SIJ, with a faint PLS subjacent to a partially ankylosed contralateral SIJ in the same patient, raising the possibility that ankylosis could result in the remodeling of a PLS. If confirmed by further research, the presence of these intermediate forms would support evolution of the PLS from formation to maturity to potential dissolution in some cases. Dissolution could occur as ankylosis rearranges subarticular trabeculation to match rearranged lines of force. Longitudinal MRI studies that follow patients with sacroiliitis over time would be required to confirm this evolution. 65-year-old male with longstanding HLA-B27 positive ankylosing spondylitis presents with chronic pain, currently treated with sulfasalazine and infliximab. Coronal T1-weighted MR image of the sacroiliac joints demonstrates significant structural abnormality of both sacroiliac joints indicating chronic sacroiliitis, including subchondral plate irregularity, periarticular erosions, and periarticular fat deposition (not shown). There is a prominent iliac-sided jagged parallel line sign on the left (arrowheads). On the right, there are shorter discontinuous dark lines parallel to the subchondral plate that may represent a forme fruste of the parallel line sign (arrows). There is no bone marrow edema on the inversion recovery images (not shown) to suggest acute sacroiliitis.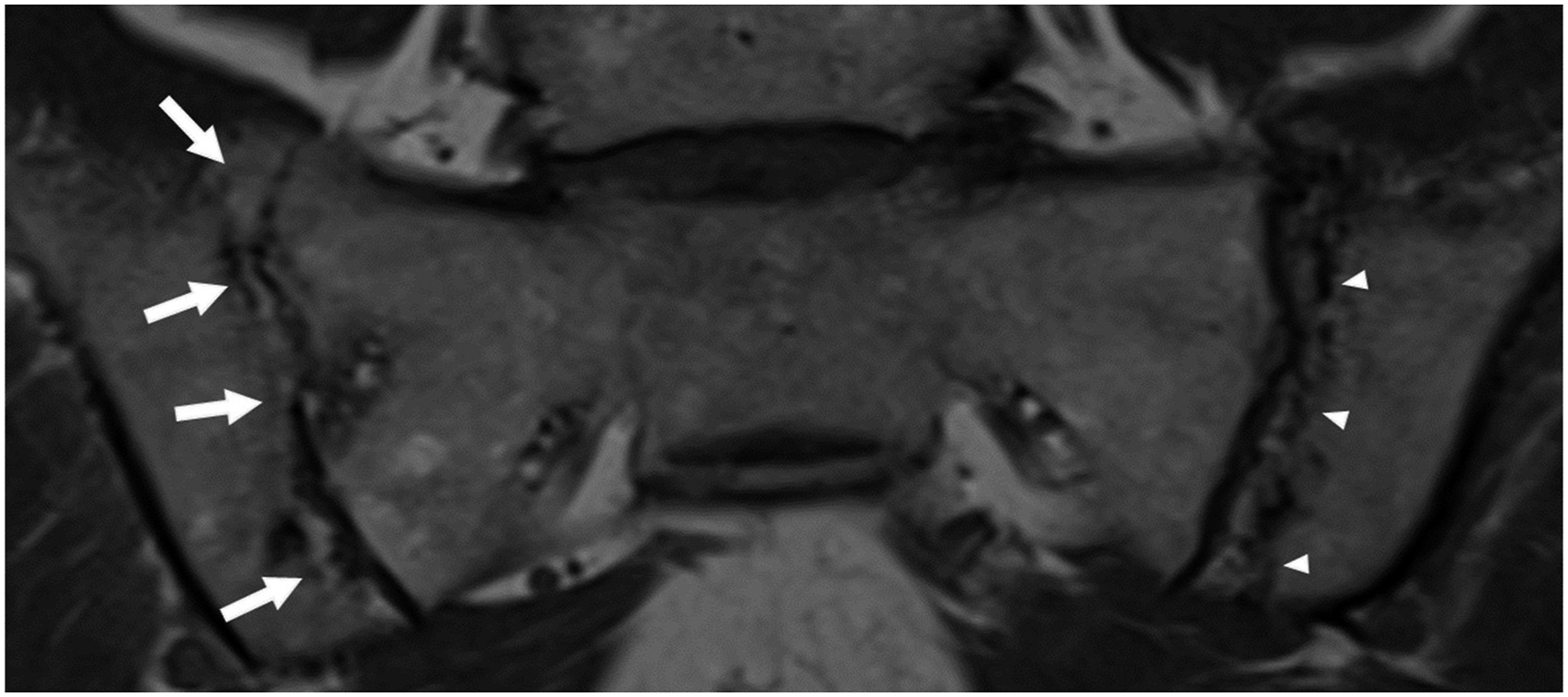
The PLS may mimic an insufficiency fracture given its thin linear low signal on both T1-weighted and fluid-sensitive sequences on MRI. However, the location, imaging context, and clinical context are different. The PLS tends to involve the iliac side of the SIJ rather than sacral involvement seen with typical insufficiency fractures. 12 The PLS is associated with imaging findings of sacroiliitis. In our experience, typical insufficiency fractures are rare in those with sacroiliitis. Sacral insufficiency fractures generally occur in elderly females with osteoporosis, 13 whereas we saw the PLS in much younger patients (average age of 48). Knowledge of the PLS as an entity distinct from an insufficiency fracture is potentially helpful to prevent subjecting sacroiliitis patients to the additional trials of fracture investigation and treatment. Additionally, the PLS could potentially be used to help confirm the diagnosis of sacroiliitis in challenging cases, such as those with prominent late changes related to healing such that sacroiliitis may be hard to recognize.
This study is limited by its retrospective nature, lack of a formal control group, lack of reassessment of the MRI findings over time, lack of a validated scoring system, and only a single observer. Those subjects with no imaging findings of sacroiliitis served as an informal control group. There were no cases of PLS in this subset of subjects (i.e., every PLS had at least one established imaging feature of sacroiliitis), which suggests relatively severe or established sacroiliitis may be necessary for this sign to occur. While most of the features of sacroiliitis in this study are based on prior scoring systems, we chose to use an abbreviated scoring system compared to established and validated scoring systems such as the SPARCC.6,7 We expected to see an association between clinical diagnosis and PLS. This was not seen in our study, perhaps due to the large number of subjects where the clinical diagnosis was uncertain, the small numbers of each known clinical diagnosis in our study, and potential variability in the criteria used for clinical diagnosis. We did not anticipate the existence of multiple PLSs, one subjacent to the other, and this was not included in our data collection. We note anecdotally that there were two obvious examples of a double PLS amongst our subjects (Figure 1). Finally, none of the subjects in this study had gross pathologic correlation, which is a limitation that is difficult to avoid because the standard of treatment for sacroiliitis rarely, if ever, involves surgical resection. Although the PLS is statistically associated with erosions and BME, causation is not proven, and this finding could theoretically be related to fracture or another process altogether. Our definition of the PLS needs to be validated with investigation regarding interobserver and intraobserver variability in identifying this sign. Future studies with a larger sample of subjects, use of established consensus definitions of diagnoses, and a control group are required, as are studies that follow the imaging findings of the PLS over time. This study was designed to verify that the PLS is seen with meaningful frequency in a rheumatology practice. Its usefulness in clinical practice has not yet been established.
In conclusion, the parallel line sign is an occasional finding in rheumatology practice, usually associated with chronic sacroiliitis, and particularly associated with erosions. The PLS should be distinguished from subchondral fractures to avoid inappropriate treatment. If validated by further study, its presence may help confirm the presence of chronic sacroiliitis in cases where the imaging findings are otherwise not definitive.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Based on the presentation at the 2021 virtual annual meeting of the American Roentgen Ray Society.
Ethical approval
Ethics approval was granted by our institutional review board for this study.