
Abstract
Myocarditis is defined as a non-ischemic inflammatory disease of the myocardium. It remains a challenge to diagnose given non-specific symptoms and lack of specific blood biomarkers. Cardiac imaging plays an important role in the evaluation of myocarditis with unique strengths and limitations of different imaging modalities, including cardiac magnetic resonance imaging, echocardiography, cardiac computed tomography, and positron emission tomography. The purpose of this review is to discuss the strengths and limitations of various cardiac imaging techniques in the evaluation of myocarditis, review imaging findings in specific causes of myocarditis including COVID-19 and after vaccination, evaluate the role of imaging in differentiating myocarditis from potential mimics and differential considerations, identify current gaps in knowledge, and propose future directions.
Introduction
Myocarditis is a disease characterized by inflammation of the myocardial tissue, with various infectious and non-infectious triggers. It remains a challenge to diagnose given non-specific symptoms and lack of specific blood biomarkers. The clinical presentation can be acute, subacute, or chronic with non-specific features ranging from chest pain, fatigue, shortness of breath, and palpitations to acute decompensated heart failure, cardiogenic shock, and rarely sudden cardiac death. 1 The incidence is challenging to determine given lack of a definitive reference standard. Most patients recover within a few weeks, although a small proportion will have long-term sequelae including persistent myocardial inflammation or progression to a dilated cardiomyopathy phenotype. 2 Cardiac imaging plays an important role in the evaluation of myocarditis, including diagnosis and risk stratification, with unique strengths and limitations of various modalities. The purpose of this review is to discuss the strengths and limitations of various cardiac imaging techniques in the evaluation of myocarditis, review imaging findings in specific causes of myocarditis including COVID-19 and after vaccination, evaluate the role of imaging in differentiating myocarditis from potential mimics and differential considerations, identify current gaps in knowledge, and propose future directions.
Definition and Histopathologic Classification
Myocarditis is defined as a non-ischemic inflammatory disease of the myocardium, characterized by the presence of both inflammation and myocyte damage. 3 Endomyocardial biopsy remains the reference standard for diagnosis, providing information that allows for characterization of the pattern of inflammation and identification of the phase (chronicity) of the disease.4,5 Histologic subtypes of myocarditis are classified according to the type of inflammatory cell infiltrate and include lymphocytic, granulomatous (lymphohistiocytic), eosinophilic, and neutrophilic myocarditis. 6
Lymphocytic myocarditis is characterized by a T lymphocyte-predominant inflammatory infiltrate occupying the myocardial interstitium and injuring cardiomyocytes (Figure 1). The inflammatory infiltrate is usually patchy but may be diffuse in severe cases. Granulomatous myocarditis includes both giant cell myocarditis and myocarditis with well-formed granulomas. In giant cell myocarditis, the inflammation is typically diffuse and myocyte necrosis is significant. Conversely, myocarditis with well-formed granulomas typically demonstrates patchy inflammation and fibrosis with non-necrotizing granulomas. The most common underlying cause of myocarditis with well-formed granulomas in North America is cardiac sarcoidosis, although it can also be seen with mycobacterial or fungal infections. Eosinophilic myocarditis can present with two separate histologic patterns. The majority of cases are characterized by a mild, patchy, interstitial eosinophilic infiltrate without accompanying cardiomyocyte injury. The second pattern, acute necrotizing eosinophilic myocarditis, is characterized by a dense eosinophilic infiltrate with a minor component of mononuclear cells, associated with prominent cardiomyocyte necrosis. Neutrophilic myocarditis is an uncommon pattern mostly occurring in the setting of disseminated bacteremia and sepsis, or as a complication of bacterial endocarditis.
4
Endomyocardial biopsy and cardiac MRI in a 29-year-old woman with acute myocarditis. (A) Endomyocardial biopsy demonstrates several dense aggregates of mononuclear cells (blue) with associated myocyte injury. Hematoxylin and eosin staining. Image digitally captured, Leica DM2500 microscope, 5x objective, OMAX A35180U3 camera, Toupview software. Image edited for brightness and contrast. Scale bar indicates 100 μm. (B) Basal short-axis LGE cardiac MRI image demonstrates subepicardial LGE at the inferolateral wall and mid-wall LGE at the anterior septum (red arrows). MRI: magnetic resonance imaging; LGE: late gadolinium enhanced.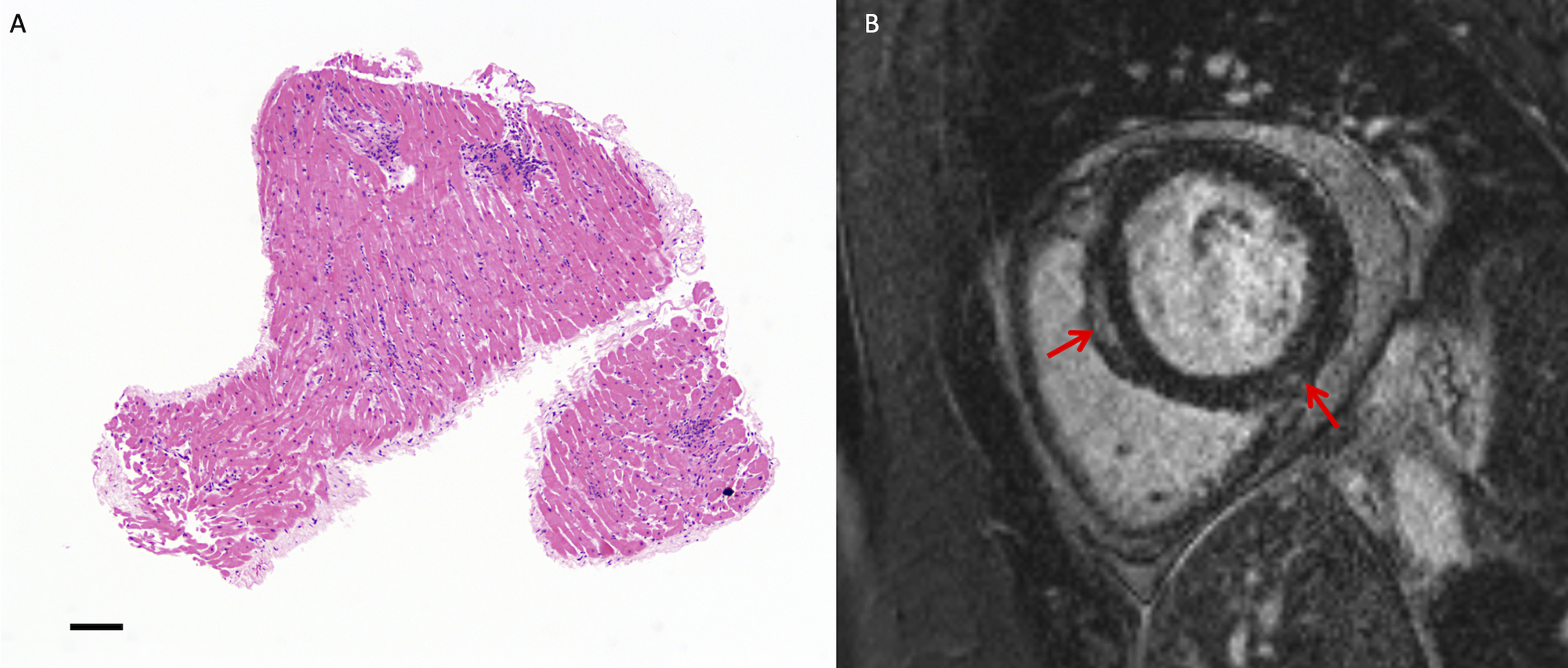
Myocarditis Phases
Patients with myocarditis can present in the acute, subacute, or chronic phase. The acute phase consists of myocardial edema and inflammation centered on and injuring cardiomyocytes. Triggers include various infectious agents (most frequently viruses, but bacteria, fungi, and parasites have also been described), systemic autoimmune diseases (including systemic lupus erythematosus), toxic agents, hypersensitivity reactions to medications, vaccinations (including COVID-19 and small-pox vaccines), and medications (including immune-checkpoint inhibitors). 1 However, despite thorough investigation, many cases remain idiopathic with no identifiable cause. 6
In the subacute phase, as the myocardial tissue begins to heal, interstitial edema and mixed inflammation are typically present. Granulation tissue composed of proliferating fibroblasts and neo-vessels develops and initiates the deposition of immature collagen at sites of prior myocyte dropout. In the subsequent weeks, this collagen matures into well-formed, irregular, haphazardly distributed scars containing entrapped viable cardiomyocytes (healed myocarditis). Uncommonly, chronic active myocarditis can occur, in which active inflammation coexists with healing and healed areas. 4
Clinical Presentation
Most patients with acute myocarditis present with acute chest pain and typically have elevated troponin levels. 7 However, troponin is not specific for myocarditis and is also elevated in the setting of acute myocardial infarction, stress-induced cardiomyopathy, and other causes of myocardial damage. Electrocardiography (ECG) findings in myocarditis are frequently non-specific and can be normal unless there is concomitant pericarditis.
Management and Outcomes
Treatment of myocarditis primarily includes guideline-based strategies to treat the sequela of heart failure or arrhythmias. Angiotensin converting enzyme inhibitors (ACEi) and beta blocker therapy may have additional benefits specific to patients with heart failure secondary to myocarditis, such as reducing myonecrosis and improving clinical outcomes. 8 NSAIDs have not been shown to be effective for isolated myocarditis.9,10 On the other hand, there is evidence to support the role of NSAIDs in patients with pericarditis and myopericarditis. 11 Hemodynamic instability in patients with myocarditis with heart failure may require mechanical circulatory support. Targeted therapies directed at a specific cause of myocarditis may be indicated, such as immunosuppressive therapy for diseases such as giant cell myocarditis, sarcoidosis, lymphocytic myocarditis, non-infectious eosinophilic myocarditis, and other autoimmune disorders.
The prognosis of myocarditis is variable and depends on several factors including the severity of the initial clinical presentation, presence of left ventricular dysfunction, and the underlying etiology. The disease course is frequently self-limited with spontaneous resolution of symptoms and no long-term sequela. Complicated myocarditis is associated with a worse prognosis and is defined as the presence of one or more of the following: left ventricular ejection fraction <50%, sustained ventricular arrhythmias, advanced heart block, heart failure, or low cardiac output syndrome/cardiogenic shock.12,13 An infrequent long-term sequelae of myocarditis is the development of a dilated cardiomyopathy phenotype, which has a poor prognosis with 5-year mortality estimated at 25%. 13
Clinical Diagnostic Guidelines
Although histopathology remains the reference standard for diagnosis of myocarditis, endomyocardial biopsy is infrequently performed due to the invasive nature of the procedure with associated risks. It is typically only performed where the diagnosis is elusive on non-invasive testing and the results of biopsy are expected to change management. Untargeted endomyocardial biopsy at the right ventricular side of the interventricular septum also has relatively low sensitivity for myocarditis due to the often patchy nature of the disease. Therefore, several different clinical diagnostic guidelines have been proposed for non-invasive diagnosis of myocarditis which typically rely on a combination of clinical presentation criteria and diagnostic test results including cardiac imaging.
For example, the European Society of Cardiology diagnostic criteria for clinically suspected myocarditis indicate that fulfilment of at least one clinical presentation and at least one diagnostic criteria is considered evidence of clinically suspected myocarditis in the absence of angiographically detectable coronary artery disease (coronary stenosis ≥50%), and known pre-existing cardiovascular disease or extra-cardiac causes that could explain the clinical presentation. 2 Diagnostic criteria include (1) functional and structural abnormalities on cardiac imaging (such as left ventricular regional wall motion or global systolic or diastolic function abnormality on echocardiography or cardiac magnetic resonance imaging (MRI)) or (2) edema and/or late gadolinium enhancement (LGE) in a classical myocarditis pattern on cardiac MRI. Diagnostic criteria proposed by the Centers for Disease Control and Prevention (CDC) categorize patients as confirmed or probable acute myocarditis, based on a combination of presence of new or worsening clinical symptoms and diagnostic testing criteria such as cardiac MRI findings consistent with myocarditis. 14 Finally, the Brighton Collaborative has proposed case definitions for myocarditis and pericarditis following immunization with three levels of certainty (ranging from definitive, probable and possible) based on abnormal biomarkers (troponin) and cardiac imaging findings. 15 Thus, cardiac imaging plays an important role in the non-invasive assessment and diagnosis of suspected myocarditis.
Cardiac Magnetic Resonance Imaging
Cardiac MRI is considered the non-invasive reference standard for diagnosis of myocarditis, with a class I recommendation, level of evidence C in the 2012 European Society of Cardiology heart failure guidelines. 16 The 2017 Canadian Cardiovascular Society heart failure guidelines recommend that all patients with suspected myocarditis have cardiac MRI in the absence of contraindications (strong recommendation, high quality evidence). 17 Finally, the 2021 AHA/ACC chest pain guidelines indicate that cardiac MRI with LGE is useful in patients with acute chest pain and suspected myocarditis if there is diagnostic uncertainty (class I recommendation, level of evidence B) and is effective to distinguish myopericarditis from other causes of acute chest pain in patients with myocardial injury and non-obstructive coronary arteries (class I recommendation, level of evidence B). 18
Cardiac Magnetic Resonance Imaging Typical Findings
Typical cardiac MRI findings in acute myocarditis include focal myocardial edema with corresponding LGE, often in a sub-epicardial pattern involving the basal to mid inferolateral and inferior segments
1
(Figure 2). A linear mid-wall pattern of LGE at the interventricular septum is less common but is associated with worse prognosis.
19
Other patterns of myocardial injury can occur, including more extensive LGE and global edema in the setting of fulminant myocarditis. Other findings include regional or global left ventricular dysfunction and pericardial enhancement if there is concomitant pericarditis (typically involving the pericardium adjacent to the involved myocardium). Cardiac MRI at 1.5T in a 32-year-old woman with viral myocarditis. (A) Mid-ventricular short-axis LGE cardiac MRI image demonstrates extensive subepicardial and mid-wall LGE most prominent at the interventricular septum (red arrow). (B) Mid-ventricular short-axis T2-weighted image demonstrates corresponding high T2 in keeping with edema (blue arrow). (C) Mid-ventricular short-axis T2-map and (D) native T1 maps demonstrate high T2 (55–60 ms) and T1 (1105–1120 ms) values corresponding to areas of LGE. MRI: magnetic resonance imaging; LGE: late gadolinium enhanced.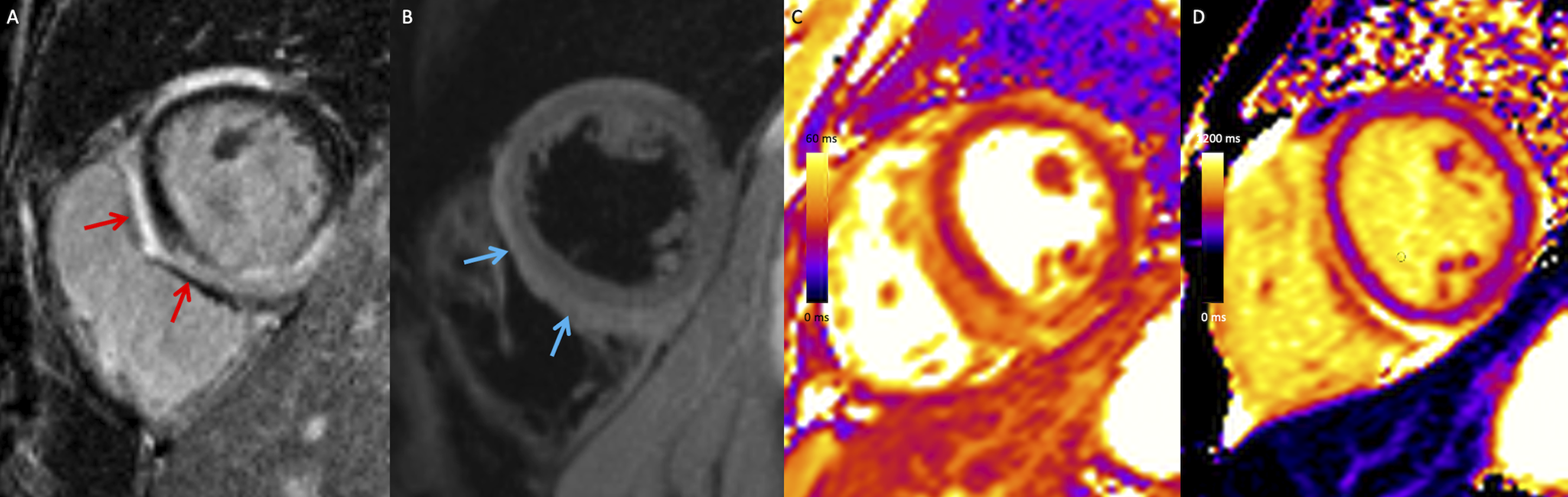
Cardiac MRI findings change depending on the phase of disease and timing of imaging. Myocardial edema is a characteristic early feature of acute myocarditis which typically improves over days to weeks and may not be detected if cardiac MRI is performed weeks to months after symptom onset. Magnetic resonance imaging should be performed as soon as possible in patients with suspected myocarditis, as the diagnostic sensitivity is highest within 2 to 4 weeks of symptom onset. 20
In addition to establishing a diagnosis of myocarditis, cardiac MRI is also useful to distinguish acute myopericarditis from other cardiomyopathies and myocardial infarction. However, cardiac MRI cannot reliably distinguish between different triggers of myocarditis or specific immune cell types.
Cardiac Magnetic Resonance Imaging Diagnostic Criteria
Expert consensus diagnostic criteria for acute myocarditis on cardiac MRI were initially proposed in 2009, frequently referred to as the Lake Louise Criteria (LLC). 21 Presence of at least two out of three of the following criteria were considered positive for acute myocarditis: high T2-weighted myocardial signal, abnormal early gadolinium enhancement (EGE), and non-ischemic pattern LGE. 21 Subsequently, T1 and T2 parametric mapping techniques have become more widely available with increased diagnostic sensitivity for myocarditis compared to the initial LLC.22-24 Therefore, the LLC were revised in 2018 to incorporate parametric mapping findings. 25 In the revised LLC criteria, fulfilment of at least one criterion in each of the following two categories is considered strong evidence of acute myocardial inflammation in patients with high clinical pre-test probability: a T1-based marker of myocardial damage and a T2-based marker of myocardial edema. 25 T1-based criteria include any of the following: LGE in a non-ischemic pattern or regional or global increase of myocardial native T1 or extra-cellular volume (ECV). T2-based criteria include any of the following: regional or global high T2-signal intensity or increase of myocardial T2 relaxation times. Systolic left ventricular dysfunction (either regional or global) and findings of pericardial inflammation (pericardial enhancement, high T1 or T2 mapping values, or the presence of a pericardial effusion) are considered supportive criteria. A comparative analysis demonstrated that the revised LLC have higher diagnostic sensitivity for acute myocarditis compared to the initial LLC criteria (88% vs 73%, P = .03). 26
T1 and T2 parametric mapping techniques allow for quantitative evaluation of the myocardium and are typically evaluated together as they provide complementary information. High T2 is specific for edema (often in the context of inflammation) while T1 is increased in the setting of fibrosis, edema, and infiltration. ECV can be calculated from pre- and post-contrast T1 maps with input of hematocrit and reflects an estimate of the proportion of the myocardial extra-cellular space. ECV is increased in the setting of fibrosis, infiltration (including amyloidosis) and extra-cellular edema. Of note, parametric mapping values are dependent on the technique and scanner (including field strength and sequence) and ideally should be evaluated in the context of a local reference range. 27
Although not included in current diagnostic guidelines, cardiac MRI can also be used to evaluate myocardial strain using techniques such as feature tracking. Myocardial inflammation can result in abnormal myocardial deformation, torsion and dyssynchrony which can be detected by strain analysis, even in patients with preserved ejection fraction
28
(Figure 3). Cardiac MRI strain parameters have high diagnostic sensitivity for myocarditis
29
and are associated with adverse outcomes, with incremental prognostic value beyond left ventricular ejection fraction (LVEF) and LGE.
30
Cardiac MRI in a 23-year-old man with acute myocarditis following COVID-19 vaccination. (A) Basal short-axis LGE cardiac MRI image demonstrates mid-wall LGE at the inferior and inferolateral wall (red arrow). (B) Feature-tracking strain analysis on 2-chamber cine SSFP MRI image. Regional circumferential strain was impaired at the basal inferior (−6%) and inferolateral (−7%) segments. MRI: magnetic resonance imaging; LGE: late gadolinium enhanced.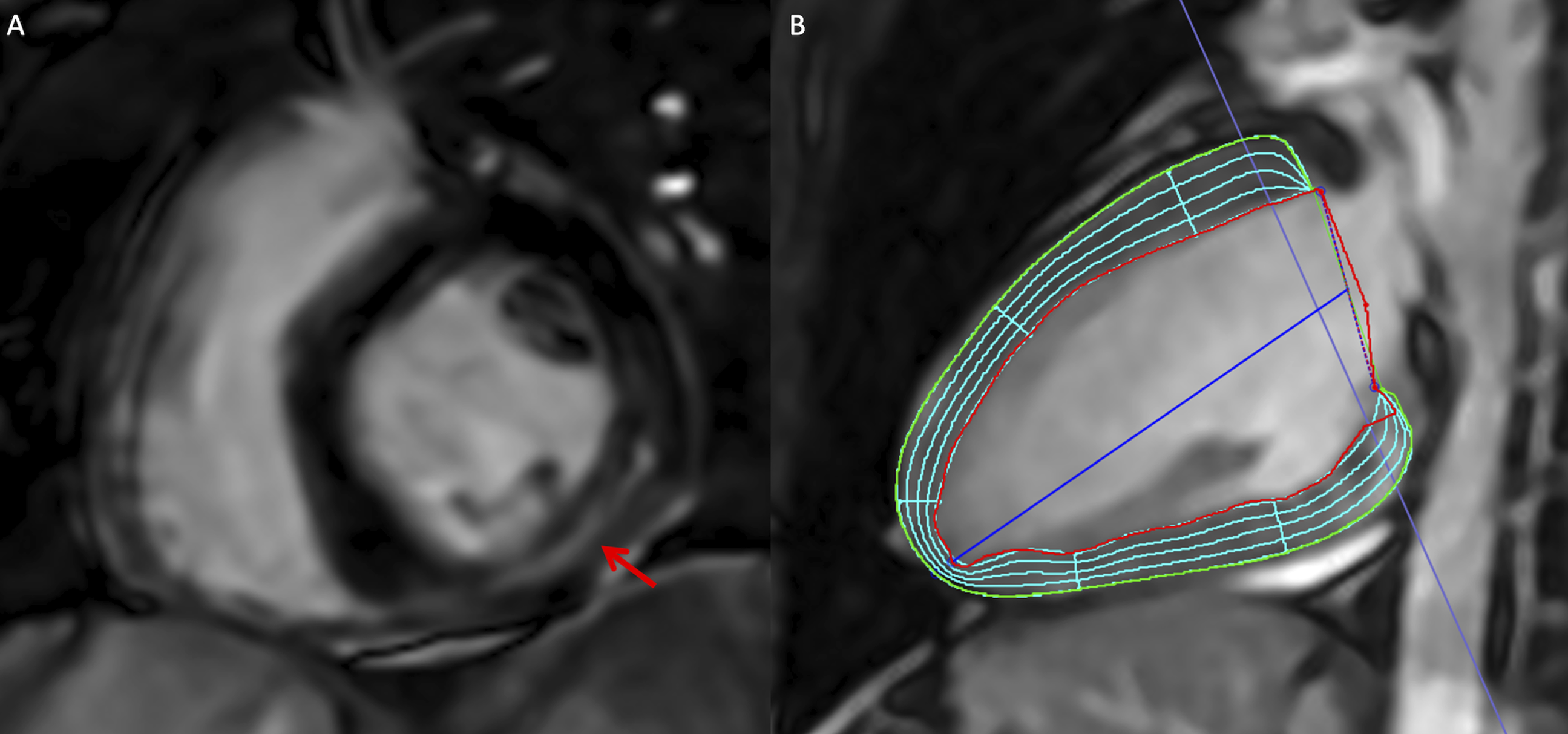
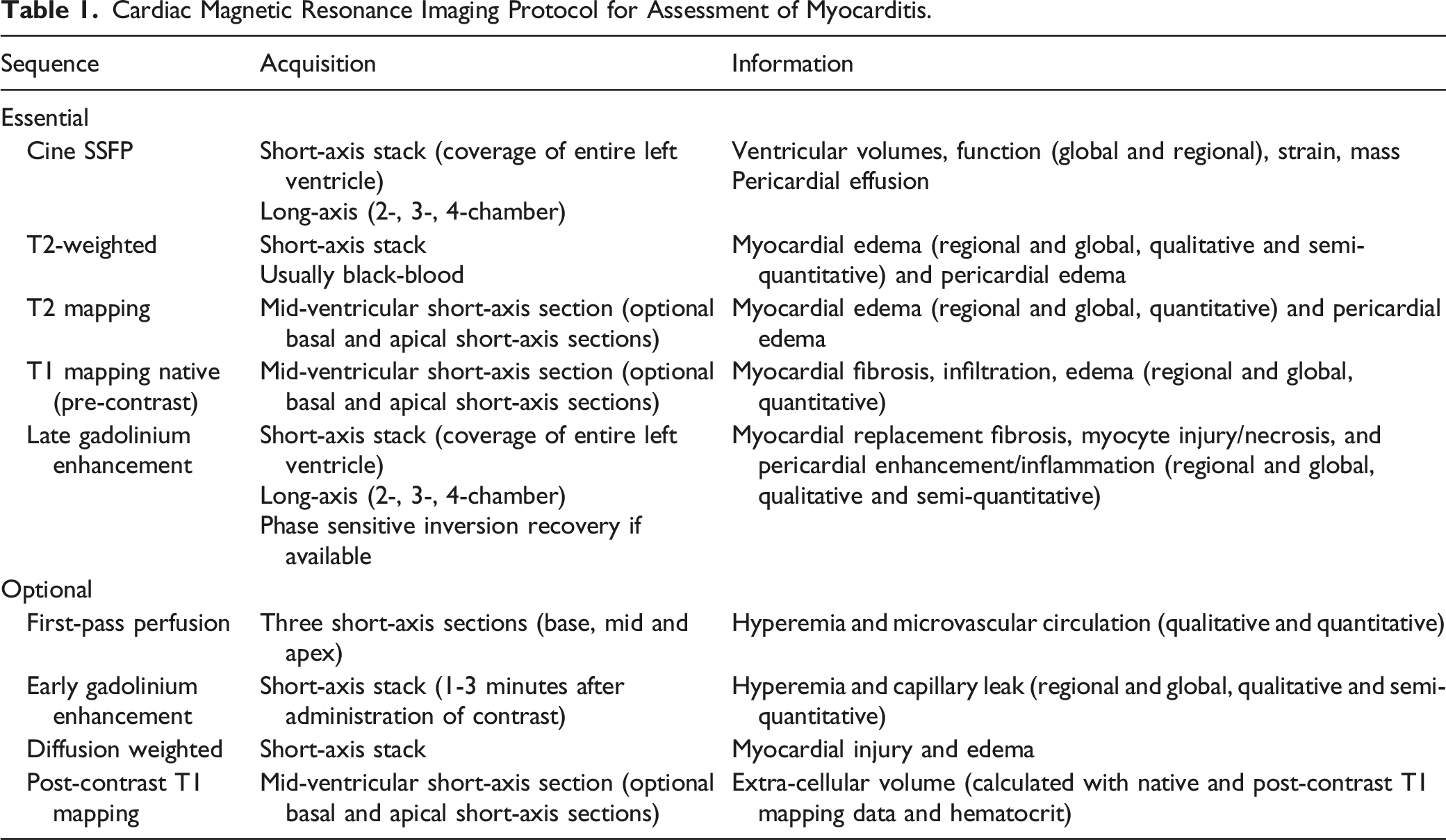
Cardiac Magnetic Resonance Imaging Protocol for Assessment of Myocarditis.
Knowledge Gaps and Future Directions in Imaging Myocarditis.
Chest Radiography
Although there are no specific features of myocarditis on chest radiography, this imaging modality is often performed in patients presenting with acute chest pain. Chest radiography is considered usually appropriate in the setting of chest pain in patients with low to intermediate probability for acute coronary syndrome according to the ACR Appropriateness Criteria. 34 Chest radiography can be useful in identifying potential sequelae of myocarditis including pulmonary edema in the context of heart failure and presence of a moderate to large pericardial effusion in the context of myopericarditis. 35
Echocardiography
Echocardiography is frequently the initial cardiac imaging modality used in the investigation of suspected myocarditis. Although findings are non-specific, they provide important diagnostic and prognostic information and are useful for excluding other diagnoses such as primary valvular or pericardial disease. Echocardiographic features on 2-dimensional echocardiography include left ventricular dilatation, wall thickening, left or right ventricular systolic dysfunction, diastolic dysfunction, and presence of a pericardial effusion if there is concomitant myopericarditis.2,36 LV systolic dysfunction can be global or regional with wall motion abnormalities typically involving the inferior and inferolateral walls. 12 Wall thickening is usually transient, reflecting edema.36,37 Although uncommon, ventricular thrombi can form adjacent to hypokinetic or akinetic walls, exacerbated by inflammatory involvement of the endocardium. 36 Finally, changes in myocardial texture leading to increased echogenicity have also been described in inflamed myocardial segments. 38
Due to low sensitivity of 2-dimensional echocardiography, a normal exam does not exclude acute myocarditis, particularly in the setting of mild inflammation. As a result, advanced techniques such as speckle-tracking echocardiography are increasingly used. Left ventricular global longitudinal and circumferential strain and strain rates correlate with presence of inflammation on endomyocardial biopsy and LGE on cardiac MRI
39
and are associated with adverse cardiac events.
40
Segmental strain abnormalities are also present in patients with acute myocarditis and normal function, and therefore may be useful to detect subtle findings of myocarditis prior to overt systolic dysfunction
41
(Figure 4). Echocardiography speckle-tracking strain analysis and cardiac MRI in a 20-year-old man with acute myocarditis. (A) Speckle-tracking assessment of segmental and global strain on an apical long-axis echocardiography view with bulls-eye plot of regional longitudinal strain values, which demonstrates impaired strain at the basal inferior and inferolateral wall. (B) Basal short-axis LGE cardiac MRI image demonstrates subepicardial LGE at the inferior and inferolateral wall (red arrow). (D) Basal short-axis T2-weighted image demonstrates corresponding high T2 in keeping with edema (yellow arrow). Left ventricular ejection fraction (global function) was normal. MRI: magnetic resonance imaging; LGE: late gadolinium enhanced.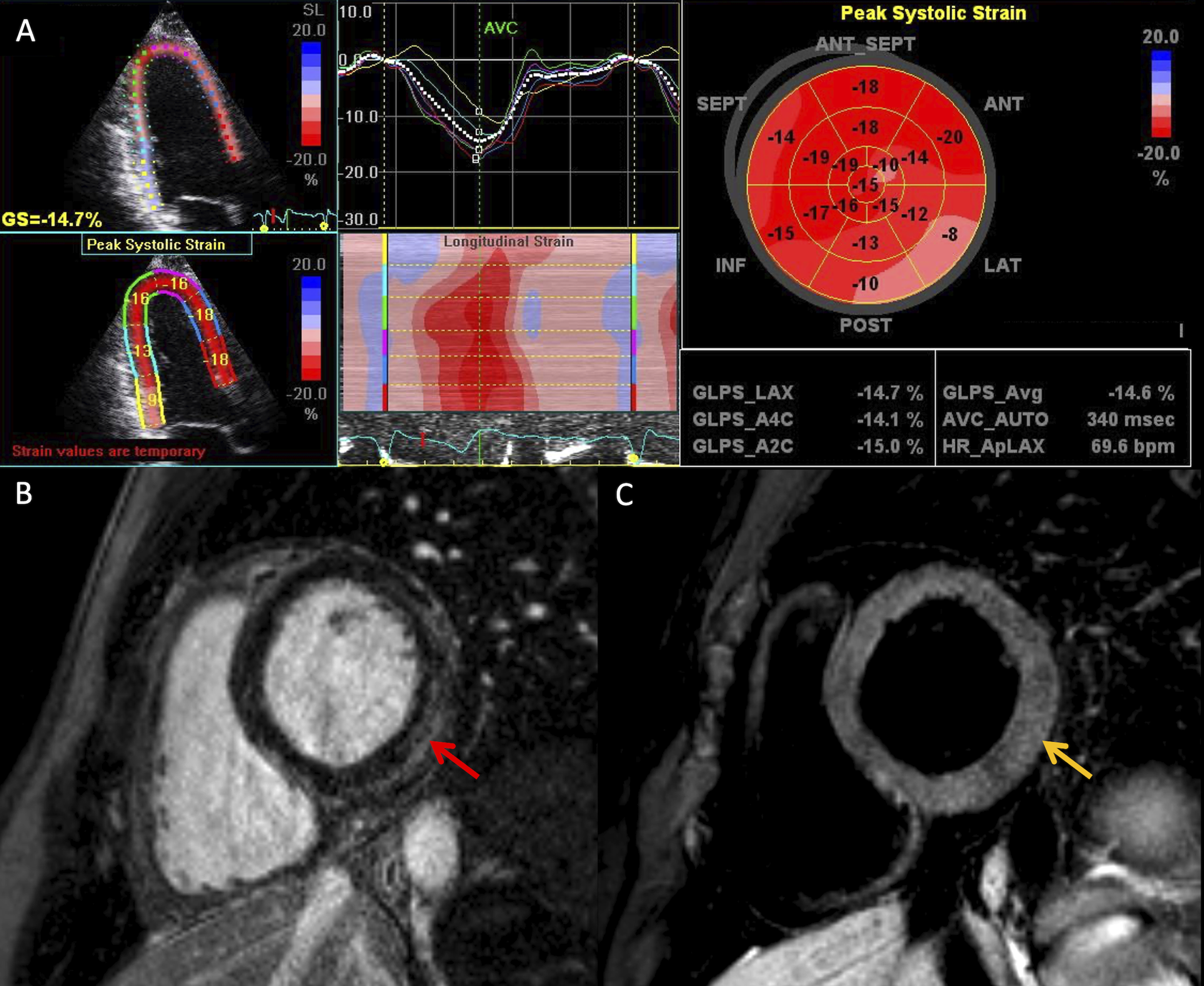
Computed Tomography
Cardiac computed tomography (CT) typically has a limited role in the evaluation of suspected myocarditis, other than to assess for other causes of acute chest pain such as coronary artery disease and acute pericarditis.
18
Global and regional wall motion abnormalities can be evaluated on prospectively triggered cardiac CT with coverage of the entire cardiac cycle. More recent developments include late iodine enhancement (LIE) and CT assessment of ECV which have potential to improve the diagnostic performance of cardiac CT for myocarditis (Figure 5). Extra-cellular volume assessed by CT correlates strongly with ECV assessed by MRI and is useful in identifying diseased myocardium in cardiomyopathies.42,43 Late iodine enhancement has high sensitivity and specificity for acute myocarditis compared to MRI as the reference standard.
44
Late iodine enhancement in a 65-year-old woman with acute myocarditis. (A) Short-axis late iodine enhanced image (8-minutes post contrast injection) demonstrates enhancement at basal inferolateral segment (subepicardial to mid-wall, red arrow. (B) Corresponding color overlay demonstrates enhancement with higher attenuation in the basal inferolateral wall. (C) Basal short-axis LGE cardiac magnetic resonance imaging image demonstrates corresponding LGE (yellow arrow). LGE: late gadolinium enhanced.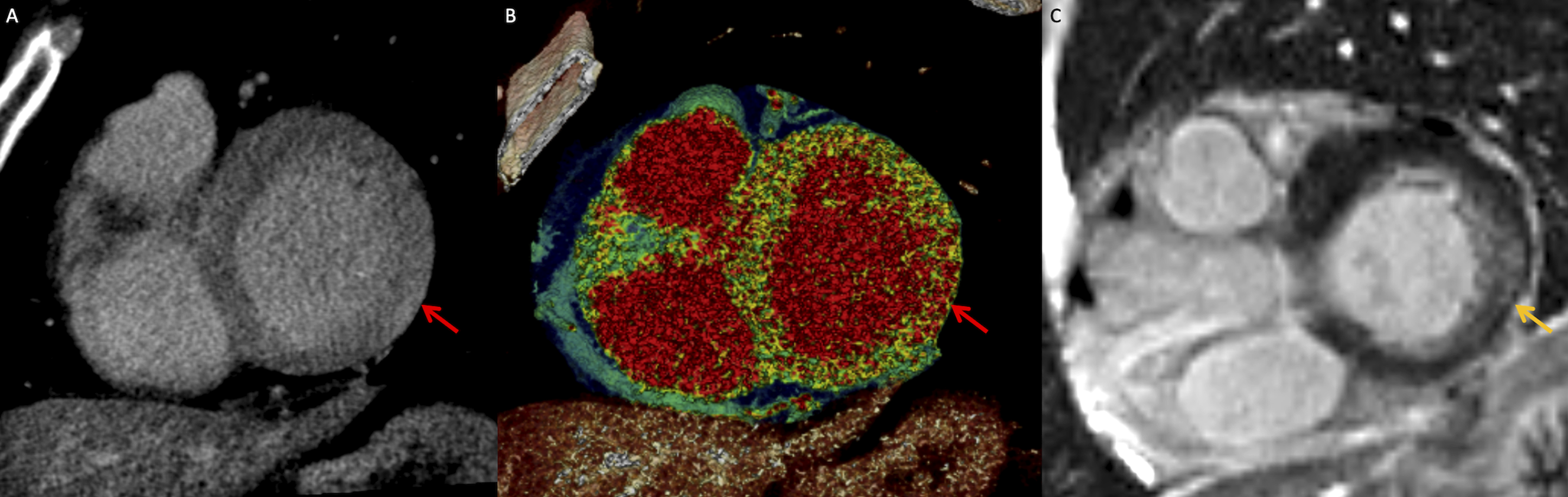
Positron Emission Tomography
18F-fluorodeoxyglucose (FDG) is a glucose analogue commonly used to image metabolically active processes such as malignancy and inflammation using positron emission tomography (PET). Although cardiac-gated FDG-PET is most frequently used in the setting of cardiac sarcoidosis,
45
FDG-uptake is also identified in acute myocarditis, reflecting metabolically active inflammatory cells (Figure 6). The myocardium is normally glucose avid and therefore a diet preparation protocol is required to suppress physiologic myocardial activity that could mask inflammation. Typical preparation protocols include a high-fat and low-carbohydrate diet for 12–24 hours followed by a complete fast other than water for the 6–12-hour period prior to FDG-injection. FDG-PET is often performed with CT for attenuation correction and interpreted in conjunction with nuclear perfusion imaging. However, the more recent availability of combined PET/MRI scanners allows for co-registration and combined analysis of PET and cardiac MRI which provide complementary information.46-48 In a recent study, focal FDG-uptake was identified in a small proportion of patients recently recovered from COVID-19 and was associated with cardiac MRI abnormalities.
49
Future directions include evaluation of novel PET radiotracers and targets including the C-X-C motif chemokine receptor 4 (CXCR4) which mediates the migration and recruitment of immune cells to sites of inflammation.
50
FDG-PET and cardiac magnetic resonance imaging in a 52-year-old woman with lupus myocarditis. (A) Axial FDG-PET image demonstrates focal FDG-uptake at the basal inferolateral wall in keeping with inflammation (blue arrow). (B) Basal short-axis LGE cardiac MRI image demonstrates corresponding mid-wall LGE (red arrow). (C) Fused PET and LGE image demonstrates focal FDG-uptake and LGE in the same myocardial segment (yellow arrow). LGE: late gadolinium enhanced; FDG: fluorodeoxyglucose; PET: positron emission tomography.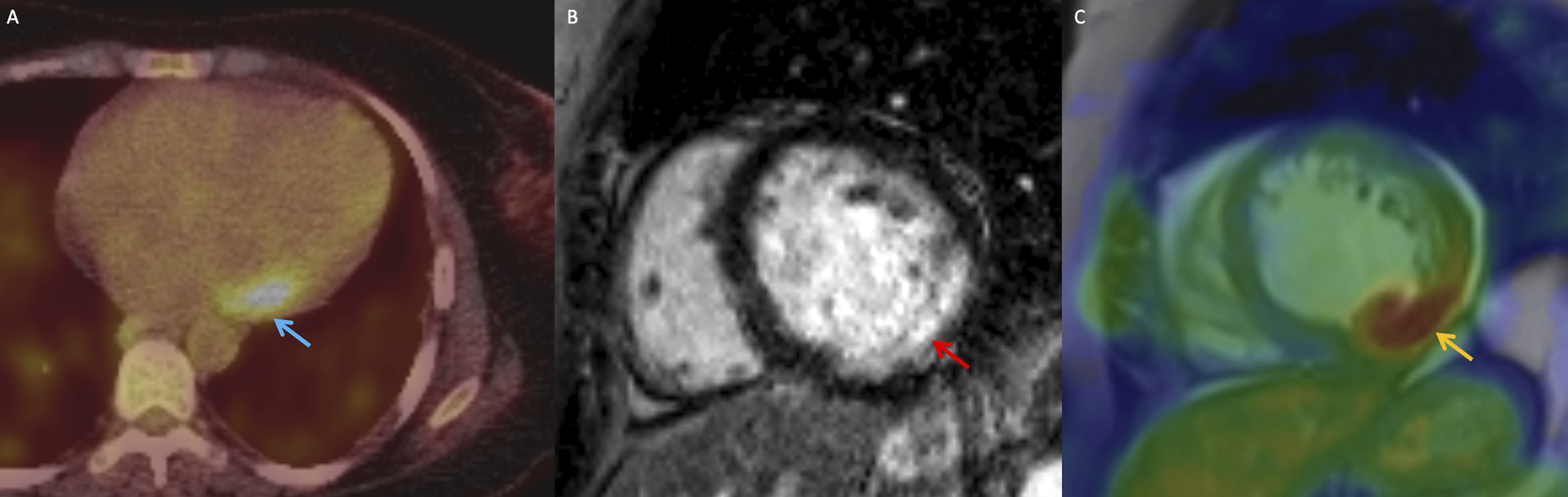
Cardiac imaging modalities offer unique strengths and limitations in the evaluation of myocarditis. Specific cardiac imaging targets in myocarditis are summarized in Figure 7, including edema (T2-weighted imaging or T2 parametric mapping on MRI), inflammation (FDG-uptake on PET), hyperemia (EGE or perfusion imaging), necrosis, fibrosis, and scar (LGE, native T1 mapping, ECV, LIE, or abnormal perfusion), and regional or global ventricular dysfunction (on echocardiography, CT, or MRI). Cardiac imaging techniques for assessment of myocarditis. MRI: magnetic resonance imaging; LGE: late gadolinium enhancement; ECV: extracellular volume fraction; SSFP: steady state free precession; CT: computed tomography; FDG: fluorodeoxyglucose; PET: positron emission tomography. Created with BioRender.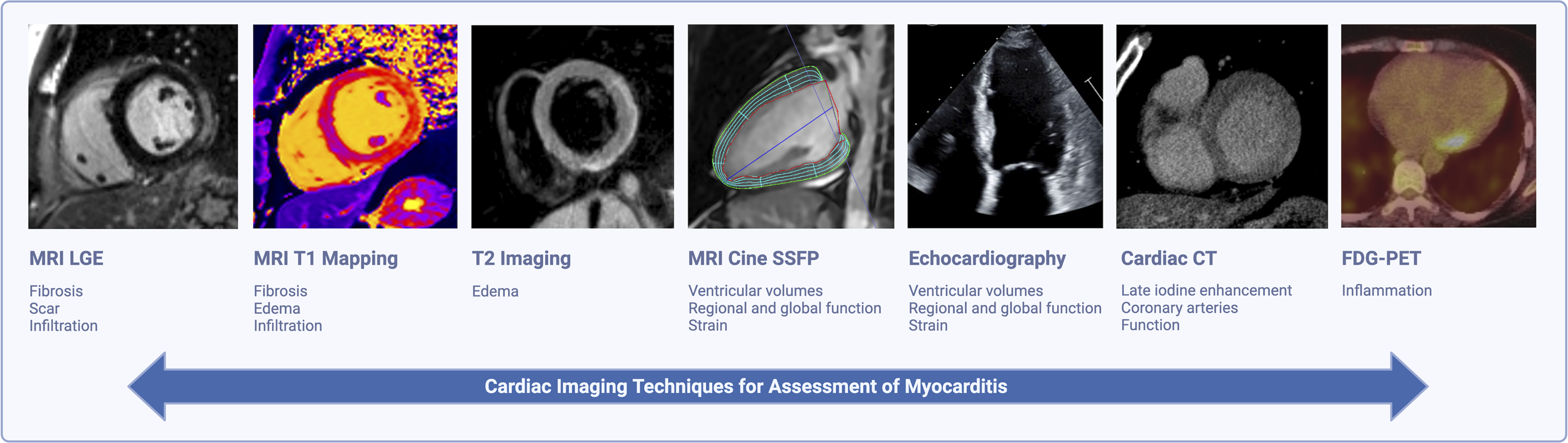
Prognostic Significance of Imaging Findings
Cardiac MRI findings, including impaired LVEF and LGE, have prognostic value in myocarditis. The presence and extent of LGE, high ECV, high T1 and high T2 are associated with adverse cardiac events in myocarditis including ventricular arrhythmias and cardiac death.51,52 A mid-wall septal pattern of LGE and increasing LGE extent at follow-up are both predictors of poor prognosis in myocarditis.20,53 Left and right ventricular systolic dysfunction is associated with poor prognosis54-56 with LVEF <40% associated with 4-fold higher risk of death. 51
Follow-Up Imaging
Although LVEF generally improves or remains normal at follow-up, a minority of patients have persistent impaired function at long-term follow-up, with highest prevalence in those presenting with fulminant myocarditis. 57 Therefore, follow-up imaging is important to evaluate functional recovery, particularly in patients with systolic dysfunction at initial presentation. 58 Repeat imaging is often performed approximately 4–6 months after baseline assessment, although there are no established guidelines on the optimal timing of follow-up. Both echocardiography and cardiac MRI can be used to quantify ventricular function, although repeat MRI provides incremental information including more reproducible assessment of ventricular function and volumes, as well as the ability to assess for resolution of edema and the extent of residual LGE.12,59 On follow-up MRI, edema and inflammation typically improve quickly with resolution within a few weeks. 20 Decreased T2 values at follow-up are associated with clinical improvement. 52 The extent of LGE usually decreases over weeks to months, and in some cases LGE may completely resolve. 60 Persistent LGE without edema reflects fibrosis, which is associated with ventricular arrythmias and sudden cardiac death, warranting long-term follow-up. 53
Specific Causes of Myocarditis
Viral Myocarditis
Viral infections are the most common trigger of myocarditis in developed countries, 61 including enteroviruses, adenoviruses, coronaviruses, and Epstein–Barr virus. 62 Up to 80% of patients present with prodromal flu-like or gastrointestinal symptoms in the preceding weeks before symptom onset. 63
COVID-19 Myocarditis
SARS-CoV-2 infection can lead to myocardial injury via multiple mechanisms, including direct viral invasion, oxygen supply-demand imbalance, ischemia, cytokine storm, and immune dysregulation. 64 The clinical presentation of myocarditis in patients with COVID-19 ranges from asymptomatic to fulminant myocarditis with heart failure. Findings on cardiac MRI in patients with COVID-19 myocarditis are similar to other causes of myocarditis, including linear subepicardial and mid-wall LGE, often involving the basal to mid inferolateral and inferior segments. 65
COVID-19 Vaccine-Related Myocarditis
Myocarditis is an infrequent adverse event following administration of messenger RNA (mRNA) based COVID-19 vaccines, with highest risk in adolescent and young adult men. 66 The pattern of myocardial injury in patients with myocarditis after COVID-19 vaccination is similar to other causes of myocarditis, but typically with less severity.67,68 A small case series demonstrated resolution of myocardial edema, normalization of left ventricular function and interval decrease in LGE extent at intermediate term follow-up (median 159 days). 60 However, minimal persistent LGE without corresponding edema has been reported in some patients at follow-up.
Autoimmune Myocarditis
Patients with autoimmune and connective tissue disorders, including systemic lupus erythematous and rheumatoid arthritis, are at increased risk of myocarditis. 69 Up to 46% of patients with rheumatoid arthritis and no known history of cardiovascular disease have nonischemic LGE on MRI and up to 10% have corresponding high T2 in keeping with myocardial edema. 70 Subclinical cardiac inflammation is also common in systemic sclerosis, with a similar pattern and distribution of non-ischemic pattern LGE in 53% of patients. 71 Several vasculitides are associated with myocarditis, most notably eosinophilic granulomatosis with polyangiitis where cardiac involvement is the primary mechanism of disease specific mortality.
Immune-Checkpoint-Inhibitor Myocarditis
Myocarditis is an uncommon but potentially fatal complication of immune check-point inhibitor (ICI) therapy. Cardiac MRI findings include high native T1, T2, and ECV. Late gadolinium enhancement is less frequent than in viral myocarditis, and more commonly involves the mid-wall of the basal and mid septum. 72 A retrospective analysis of 79 patients with ICI-myocarditis and mapping data showed that 100% of patients met at least one of the revised LLC on MRI and 48% met both T1 and T2-based criteria. 73
Mimics and Differential Considerations
The clinical presentation of acute myocarditis can mimic other acute cardiac conditions and cardiac imaging often plays an important role in differentiating myocarditis from other diseases. Timely differentiation is important given differences in management and prognosis.
Acute Coronary Syndrome
Acute myocarditis often presents similarly to acute coronary syndrome (ACS), including chest pain in the setting of ECG abnormalities and elevated troponin. Coronary angiography or CT are useful to evaluate the coronary arteries and rule out ACS if suspected. On cardiac MRI, inflammation due to myocardial ischemia is confined to a coronary artery vascular territory in a subendocardial to transmural pattern (depending on the extent of injury) and is characterized by high T2 signal with or without LGE. 74
Stress-Induced Cardiomyopathy
Stress-induced (or Takotsubo) cardiomyopathy is a clinical syndrome characterized by left ventricular systolic dysfunction often triggered by an emotional or physical stressor. Patients typically present with chest pain and elevated cardiac biomarkers. In stress cardiomyopathy, wall motion abnormalities can be detected on echocardiography, MRI, or angiography. The classic pattern is apical ballooning although mid-ventricle and basal patterns have also been described less commonly. Late gadolinium enhancement is infrequent on MRI although there is usually marked edema corresponding to the regional wall motion abnormality.
Pericarditis
Pericarditis refers to inflammation of the pericardium and can occur in isolation or in conjunction with myocarditis (myopericarditis). Patients with pericarditis usually present with acute onset chest pain, although unlike myocarditis, troponin is not elevated unless there is concomitant myocarditis resulting in myocyte injury. Electrocardiography changes are usually present including diffuse ST segment elevation and T wave abnormalities. Pericardial inflammation can be diffuse although in the setting of myopericarditis it is more commonly focal, involving the pericardium adjacent to the inflamed areas of myocardium. Typical MRI findings in pericarditis include presence of a pericardial effusion, pericardial thickening, edema, and enhancement
11
(Figure 8). Cardiac MRI in a 28-year-old man with acute pericarditis. (A) Basal short-axis late gadolinium enhanced cardiac MRI image demonstrates extensive circumferential pericardial enhancement and thickening. (B) Basal short-axis T2-weighted image demonstrates corresponding high T2 in keeping with pericardial edema and inflammation. MRI: magnetic resonance imaging.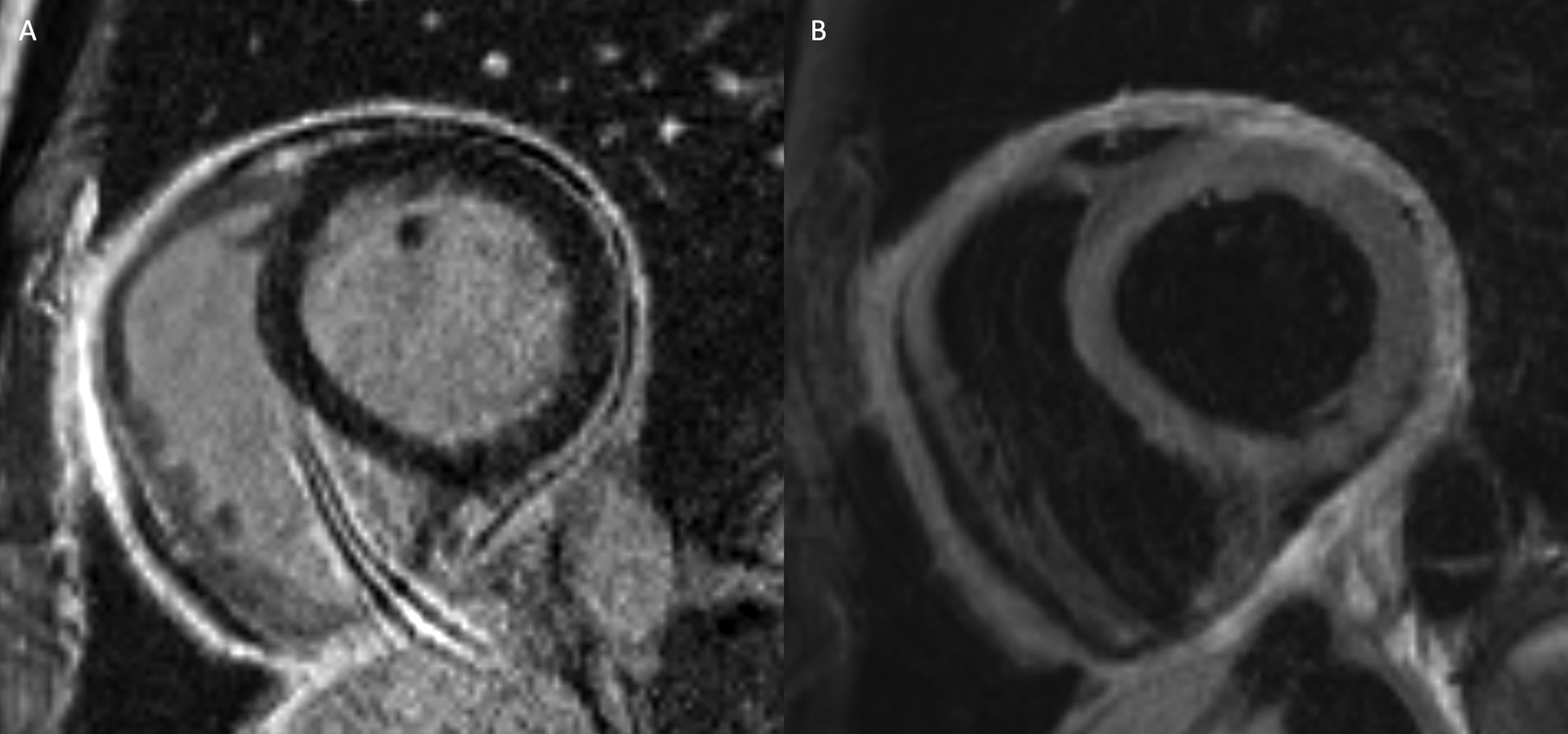
Conclusion
Cardiac imaging plays an important role in the evaluation of myocarditis including establishing a diagnosis, differentiation of acute myocarditis from other disease processes, prognostication and risk stratification, and evaluation for potential long-term sequelae on follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.