
Abstract
Purpose
To determine if CT can improve the diagnostic confidence for the detection of sacroiliac joint (SIJ) erosions in patients with equivocal MRI findings.
Methods
A retrospective analysis of adult patients who had an SIJ MRI and a subsequent SIJ CT within 12 months was conducted. Using a 5-point Likert scale, two reviewers evaluated the de-identified MRI and CT images in randomized order and in separate sessions to answer the question: “Does the patient have SIJ erosions?”. A Fisher’s exact test was used to analyze the difference in diagnostic confidence, and intraclass correlation coefficient (ICC) was used to determine interrater reliability.
Results
54 patients were included in the analysis (average age, 43.9 years). The average time interval between initial SIJ MRI and subsequent CT was 14.4 weeks (range, 5.6–50.3 weeks). CT resulted in significantly more cases with definitive diagnostic confidence than cases with probable or equivocal confidence compared to MRI (P < .001). Amongst cases with equivocal findings on MRI, 73.2% of cases had definitive diagnoses on CT. There was moderate interrater agreement for MRI, with an ICC of .490 [95% CI, .258–.669], and excellent agreement for CT, with an ICC of .832 [95% CI, .728–.899].
Conclusion
Overall, CT led to significantly increased diagnostic confidence and higher interrater reliability for the detection of SIJ erosions compared to MRI. Judicious use of CT may be useful in detecting SIJ erosions in patients with equivocal MRI findings.
Introduction
Seronegative spondyloarthritis (SpA) is a clinical entity that encompasses a group of chronic progressive inflammatory joint diseases in the absence of rheumatoid factor. 1 SpA includes ankylosing spondylitis, reactive arthritis, psoriatic arthritis and arthritis associated with inflammatory bowel disease. 1
In the 1990s, the European Spondyloarthropathy Study Group (ESSG) proposed classification criteria for SpA. 2 The ESSG split the disease into two subsets—(1) axial SpA (axSpA), dominated by low back pain, and (2) peripheral SpA, dominated by inflammation of the peripheral joints and/or entheses. 2 Sacroiliac joint (SIJ) and spinal inflammation prevails in the early stages of axSpA, with both inflammatory and secondary structural changes prevalent during the later stages. 3 About 20–30% of patients with axSpA develop structural changes in the SIJ within the first two years of the disease, with vertebral fusion occurring at later time points in most patients.4,5 As such, it has been suggested that patients should be treated during the “window of opportunity”—by treating inflammatory lesions prior to the development of irreversible structural changes—for better recovery of mobility and improved patient outcomes. 3 Since axSpA is a significant cause of debilitating change throughout the axial skeleton and often cause long-term disability requiring chronic immunosuppressants, early recognition is important. 3
In 2009, Assessment of SpondyloArthritis international Society (ASAS) developed classification criteria for axSpA.6,7 The ASAS reported that in patients with three or more months of back pain and age of onset less than 45 years old, sacroiliitis confirmed on imaging (i.e., MRI or radiographs) with one or more SpA feature(s), or HLA-B27 positive patients with two or more SpA features, have sensitivity and specificity of axSpA of 82.9% and 84.4%, respectively. SpA features included inflammatory back pain, arthritis, enthethisitis, uveitis, inflammatory bowel disease, family history or elevated CRP.6,7 In 2019, the ASAS MRI working group published an updated set of standardized definitions for MRI lesions of the SIJ in patients presenting with axSpA. 8 A newly defined term included in this 2019 ASAS update is “erosion,” the most frequently detected structural lesion and a well-known feature of axSpA. 8 ASAS reported that erosions were detected almost as reliably as subchondral inflammation, and that even a small erosion with a focus of inflammation in the erosion cavity may be highly specific for SpA. 8 As such, a confident diagnosis of SIJ erosions would increase the diagnostic confidence that subcortical edema is in fact inflammatory. This has implications when applying the ASAS classification criteria for axSpA.
Although the reliability of detecting erosions on MRI may be substantial and comparable to bone marrow edema despite the significant heterogeneity of their appearance, smaller erosions were not as reliably detected on MRI.8,9 It has been proposed that CT be used in cases with equivocal SIJ findings on MRI as CT can directly visualize structural changes, such as erosions, with a higher sensitivity. 7 Currently, there is paucity of evidence in the literature in regard to the value of subsequent CT in patients evaluated for SIJ erosions with equivocal MRI findings. Previous studies have compared pelvic plain radiographs, abdominal CT, and SIJ MRI with SIJ CT for the diagnoses of structural sacroiliitis.10,11 This is the first study to assess the difference in diagnostic confidence of dedicated SIJ MRI and SIJ CT for the detection of SIJ erosions.
The objective of this study was to determine if CT can improve the diagnostic confidence for the detection of SIJ erosions in patients with equivocal MRI findings.
Materials and Methods
This retrospective HIPAA-compliant study was approved by the Institutional Review Board; the requirement for informed consent was waived.
Patients
A retrospective analysis of patients was conducted at a tertiary care center. Consecutive patients over the age of 18 who had a dedicated SIJ MRI and a subsequent SIJ CT within 12 months were included. 12 Patients who did not have imaging for dedicated assessment of the SIJ were excluded.
A search for images pertaining to the procedure code “CT Sacrum/SI Joints” acquired between January 1, 2018 and December 31, 2019 was conducted using the institution’s Picture Archiving and Communication System (PACS). Using the procedure code, 87 search results were obtained. After a retrospective review of the results for a preceding SIJ MRI within the previous 12 months, 37 patients were excluded. Reasons for lack of preceding dedicated MRI were (1) no prior MRI as SIJ CT was performed for a concern unrelated to sacroiliitis, for example: neoplasm, trauma, fracture, and non-inflammatory pain (14 cases); (2) preceding MRI performed non-dedicated or incomplete imaging of the SIJ (2 cases); (3) patient contraindications to MRI due to metallic foreign body or claustrophobia (6 cases); and (4) referring physician ordered SIJ CT without MRI for unknown reasons (11 cases). A total of 54 patients who had a dedicated SIJ MRI and subsequent dedicated SIJ CT for evaluation of possible sacroiliitis were included in the final analysis.
MRI Protocol
SIJ MRI examinations were performed with either a 3-T system (Gyroscan; Philips Medical Systems, Best, the Netherlands) or a 1.5-T system (LX Horizon EchoSpeed; GE Healthcare, Milwaukee, Wis).
The imaging protocol for the 3-T MR scanner included coronal T1-weighted (COR-T1) and coronal T2-weighted fat-saturated sequences with spectral attenuated inversion recovery (COR-T2-FS-SPAIR) of the SIJ. For both COR-T1 and COR-T2-FS-SPAIR sequences of the SIJ, slice thickness was 3 mm, and spacing was .3 mm. For the COR-T1 sequence, repetition time (TR) was 573 ms, echo time (TE) was 10 ms, number of excitations (NEX) was 2, and field of view (FOV) was 20 mm by 18.4 mm. For the COR-T2-FS-SPAIR sequence, TR was 3406 ms, TE was 70 ms, NEX was 3, and FOV was 20 mm by 18.2 mm.
The imaging protocol for the 1.5-T scanner included COR-T1 and coronal STIR (COR-STIR) sequences of the SIJ. For both COR-T1 and COR-STIR sequences of the SIJ, slice thickness was 4 mm, spacing was .5 mm, NEX was 3, and FOV was 20 mm by 20 mm. For the COR-T1 sequence, TR was 617 ms, and TE was minimum full. For the COR-STIR sequence, TR was 4850 ms, and TE was 80 ms.
CT Protocol
SIJ CT examinations were conducted using either the GE LightSpeed VCT 64 imager (GE Healthcare, Milwaukee, WI, USA) or the GE LightSpeed Xtra Pro 16 imager (GE Healthcare, Milwaukee, WI, USA) in helical acquisition. The acquisition parameters for the LightSpeed VCT imager were as follows: scan coverage, L5 pedicle to greater sciatic notch; energy, 120 keV for 10–400 mA; rotation time, .8 seconds; detector coverage, 40 mm; slice thickness, .625 mm; reconstruction interval, .625 mm; pitch, .541:1; and table speed, 20.62 mm/s. The acquisition parameters for the LightSpeed Xtra imager were as follows: scan coverage, L5 pedicle to greater sciatic notch; energy, 120 keV for 10–500 mA; rotation time, .8 seconds; detector coverage, 10 mm; slice thickness, .625 mm; reconstruction interval, .625 mm; pitch, .932:1; and table speed, 20.62 mm/s. Data reconstruction windows were as follows: reconstruction 1, .625 mm by .625 mm, bone+ algorithm and direct multi planar reformat; reconstruction 2, 1.25 mm by 1.25 mm, bone+ algorithm; and reconstruction 3, 1.25 mm by 1.25 mm, standard algorithm. Coronal SIJ cutlines were aligned parallel to the body of the sacrum on the sagittal viewport. Sagittal SIJ cutlines were aligned to include both SI joints and cover entire sacrum. Both planes were reviewed to assess for SIJ erosions.
Outcome Measures
The primary outcome of this study was the difference in diagnostic confidence in detecting or excluding SIJ erosions on MRI compared to CT. SIJ erosions on MRI were defined as “a defect in subchondral bone associated with full-thickness loss of the dark appearance of the subchondral cortex at its expected location, with loss of signal on a T1W non-fat-suppressed sequence compared with the normal bright appearance of adjacent bone marrow.”8,9 SIJ erosions on CT were defined as a lesion that met the following criteria: (1) interrupts the sacral or iliac cortical bone on at least two consecutive slices, or visible on at least two planes; (2) measures at least 2 mm in size; (3) has a neck as wide as the remainder of the lesion (i.e. not a narrow neck); and (4) demonstrates clearly demarcated low attenuation in the subcortical area.11,13
Secondary outcomes were (1) interrater agreement of reviewers of SIJ MRI and CT, (2) analysis of patients with differing diagnostic confidence ratings between SIJ MRI and CT, and (3) analysis of patients with differing findings of the absence or presence of SIJ erosions between MRI and CT.
Image Analysis and Data Collection
All patient identifying parameters and demographics were anonymized and each patient’s imaging was allocated a unique study number (range 0–1000) allocated by a unique random number generator. First, dedicated SIJ MRI images were assessed and scored independently by two readers (staff radiologists specialized in musculoskeletal imaging with 5 and 7 years of experience) blinded to clinical information and other components of the MRI examination. Images were read independently and in random order on three monitor workstations using GE Centricity software with standardized viewing conditions. Following a 1-month interval, dedicated SIJ CT images were read independently and in random order, in identical viewing conditions.
Global Assessment
At each sitting, the readers were asked to make a global assessment based on CT and MRI definitions of “erosions” to answer the following question: “Does the patient have SIJ erosions?”. 8 A scoring system using a 5-point Likert scale was devised to assess the reader’s level of certainty: 1 = strongly disagree (definitive absence of erosions); 2 = disagree (probable absence of erosions); 3 = equivocal (uncertain); 4 = agree (probable presence of erosions); and 5 = strongly agree (definitive presence of erosions).
Statistical Analyses
A total of 54 patients were included in this study. As each patient’s imaging was scored in duplicate by two independent staff radiologists, a total of 108 scores were included in the final statistical analyses.
A score of 1 and 5 on the Likert scale was categorized and interpreted as the reviewer indicating the “definitive” absence or presence of SIJ erosions. A score of 2 and 4 was categorized and interpreted as the reviewer indicating the “probable” absence or presence of SIJ erosions. A score of 3 was interpreted as the reviewer indicating “equivocal” findings. A Fisher’s exact test was used to compare diagnostic confidence of detecting or excluding SIJ erosions on between MRI and CT. A P-value less than .05 was used to determine significance of findings.
Intraclass correlation coefficient (ICC) was used to determine interrater reliability of MRI and CT interpretations. Agreement was characterized as follows: ICC of .81–.99 as excellent agreement, ICC of .61–.80 as substantial agreement, ICC of .41–.60 as moderate agreement, ICC of .21–.40 as fair agreement, and ICC value of .20 or less as slight agreement.
A score of 1 and 2 on the Likert scale was interpreted as the reviewer detecting the “absence” of SIJ erosions. A score of 4 and 5 was interpreted as the reviewer detecting the “presence” of SIJ erosions. A score of 3 was interpreted as the reviewer indicating “equivocal” findings.
Data were statistically analyzed using Statistical Package for the Social Sciences (SPSS Version 23.0. Armonk, NY. IBM Corp, 2015).
Results
Patient Characteristics
Patient demographic characteristics (n = 54).

Abbreviations: SIJ, sacroiliac joint.
Difference in Diagnostic Confidence Between MRI and CT
Difference in Diagnostic Confidence Between MRI and CT.
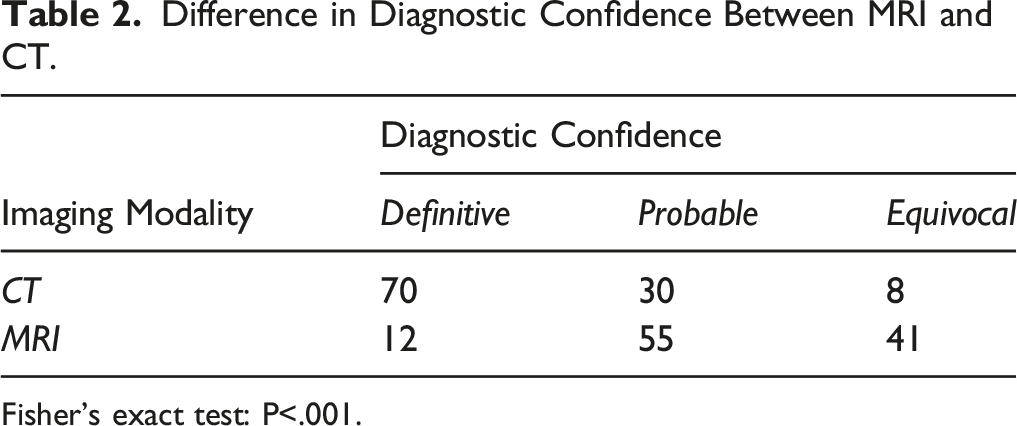
Fisher’s exact test: P<.001.
Interrater Agreement of MRI and CT
There was moderate interrater agreement for MRI, with an ICC of .490 [95% CI, .258–.669], and excellent agreement for CT, with an ICC of .832 [95% CI, .728–.899].
Cases with Differing Diagnostic Confidence Between MRI and CT
Evaluation with MRI resulted in 11.1% of cases with definitive diagnoses (n = 12), 50.9% with probable diagnoses (n = 55), and 38.0% with equivocal diagnoses (n = 41). Evaluation with CT resulted in 64.8% of cases with definitive diagnoses (n = 70), 27.8% with probable diagnoses (n = 30), and 7.4% with equivocal diagnoses (n = 8).
Cases with Differing Diagnostic Confidence and Cases with Differing Imaging Findings Between MRI and CT.
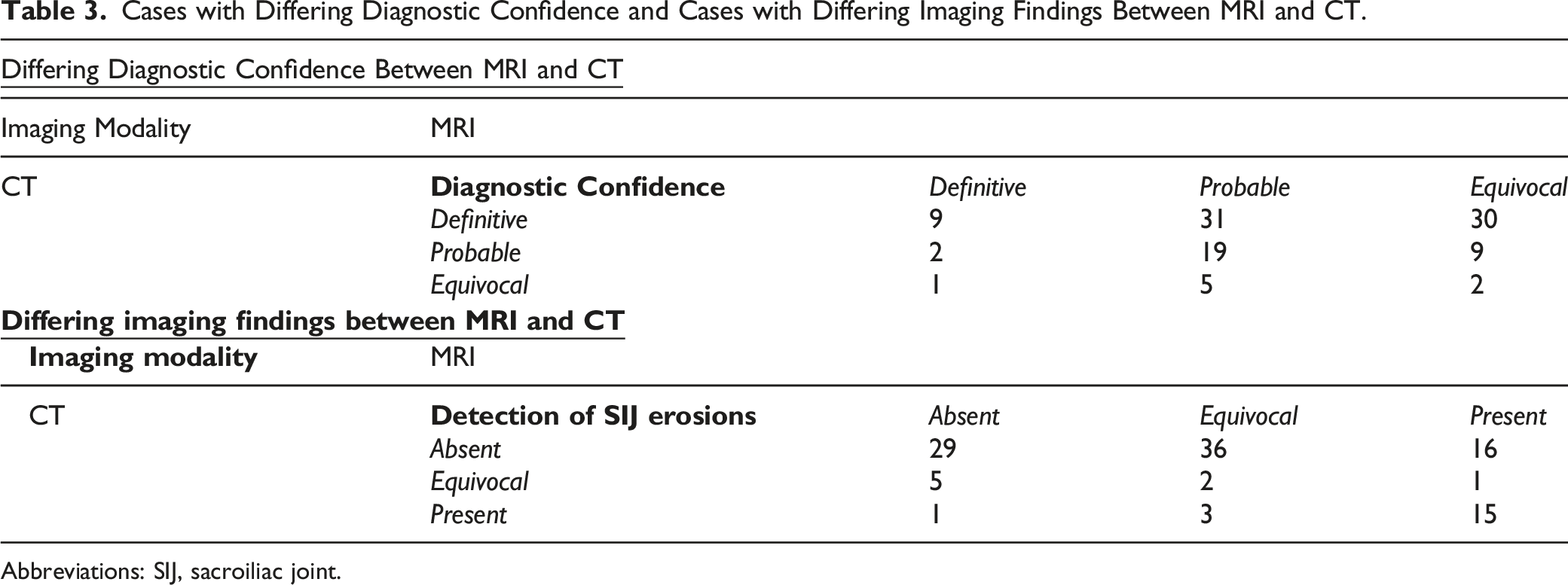
Abbreviations: SIJ, sacroiliac joint.
Cases with Differing Findings Between MRI and CT
Evaluation with MRI demonstrated an absence of SIJ erosions in 32.4% of cases (n=35), presence of erosions in 29.6% of cases (n=32), and equivocal findings in 38.0% of cases (n=41). Evaluation with CT demonstrated an absence of SIJ erosions in 75.0% of cases (n=81), presence of erosions in 17.6% of cases (n=19), and equivocal findings in 7.4% (n=8).
Amongst the 76 cases with absent-to-equivocal findings of SIJ erosions on MRI, CT detected erosions in only 4 (5.3%) cases. Amongst the 32 cases with SIJ erosions detected on MRI, CT confirmed erosions in 15 (46.9%) cases. Furthermore, amongst the 41 cases with equivocal findings on MRI for erosions, CT demonstrated erosions in 3 (7.3%) cases and absence of erosions in 36 (87.8%) cases. (Table 3)
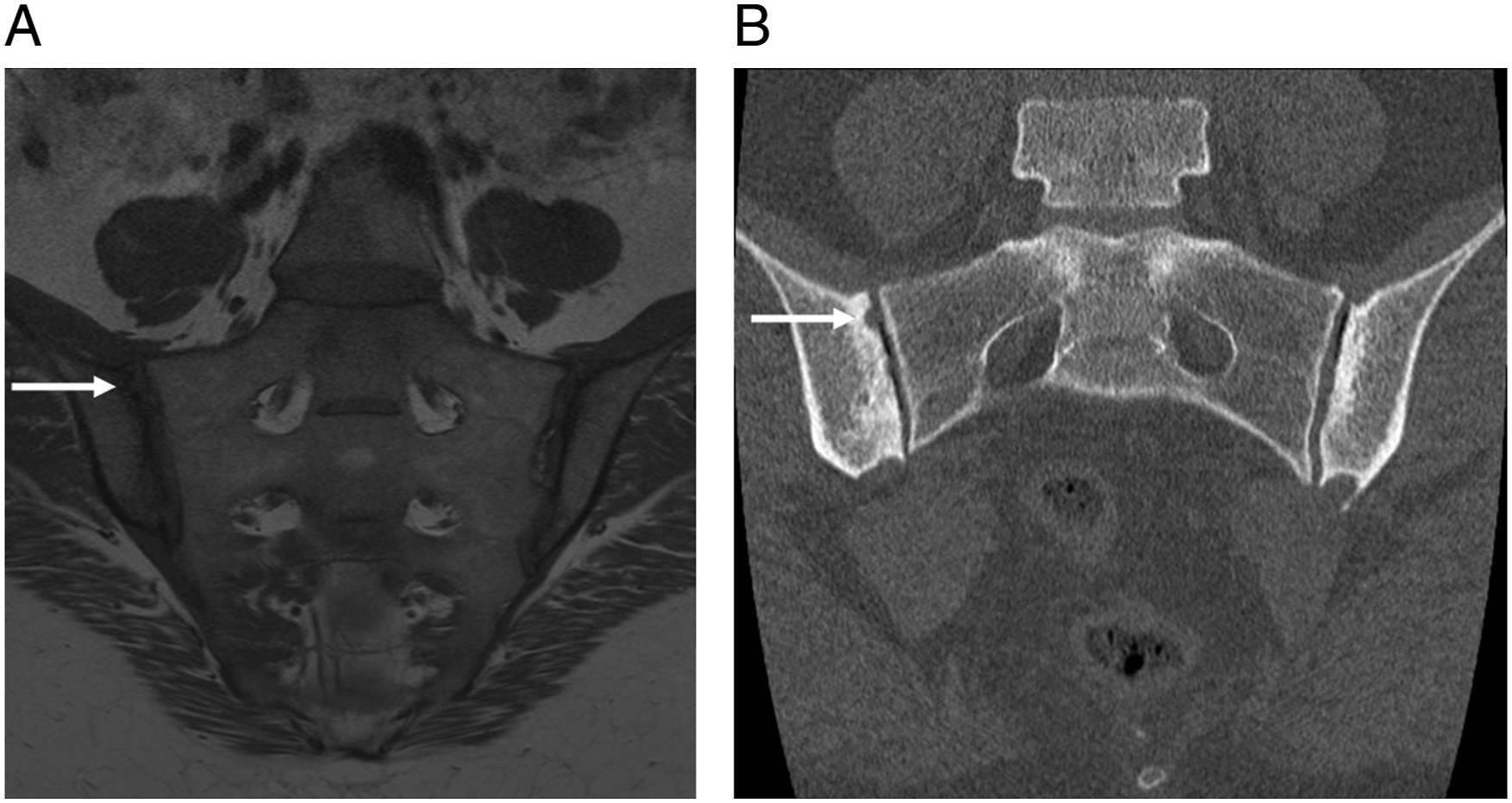
Representative images of patients with differing findings of sacroiliac joint erosions between MRI and CT are presented in Figures 1 and 2. 21-year-old female with dedicated Sacroiliac joint MRI and CT. (A) MRI demonstrates equivocal findings (white arrows). (B) CT demonstrates definitive absence of SIJ erosions. 35-year-old female with dedicated Sacroiliac joint MRI and CT. (A) MRI demonstrates equivocal findings (white arrow). (B) CT demonstrates definitive Sacroiliac joint erosions (white arrow).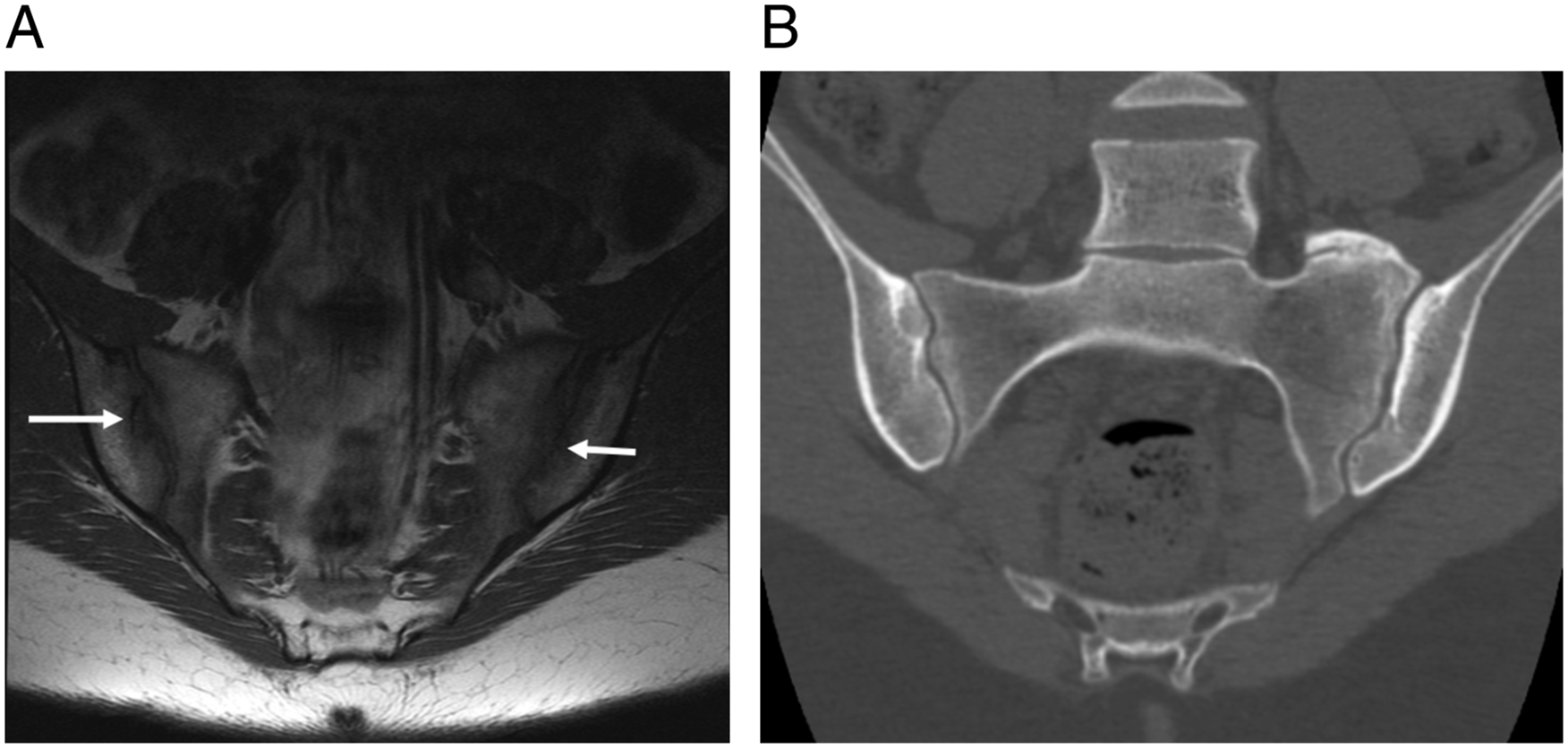
Discussion
AxSpA is a chronic progressive inflammatory arthritis affecting the axial skeletal system. It is characterized by inflammatory back pain, excess spinal bone formation, limited spinal range of motion, and a high prevalence of HLA–B27.1,3 Ideally, treatment should be initiated during the “window of opportunity,” referring to the early reversible inflammatory lesions of the axial skeleton prior to patients developing irreversible secondary skeletal changes.3–5 In 2019, the American College of Rheumatology published treatment recommendations for SpA and axSpA. 14 The recommended treatment algorithm suggests conditional continuous treatment with NSAIDs. In patients with failed therapy with NSAIDs, biologic agents such as TNF inhibitors should be initiated.1,14 In situations where TNF inhibitors are unavailable or there is significant peripheral SpA, conventional disease-modifying anti-rheumatic drugs (DMARDs) such as methotrexate and sulfasalazine are recommended.1,14 However, chronic use of biologic agents and DMARDs carry significant morbidity, with increased susceptibility to infections, including opportunistic and reactivation of latent tuberculosis infections, increased risk of lymphoproliferative malignancies, and increased risk of drug-induced lupus erythematosus.15-17
Considering the “window of opportunity” for the treatment of axSpA and the chronic immunosuppressants recommended, accurate and early detection of axSpA is of vital importance. Erosions on imaging are a critical diagnostic finding of axSpA that can vastly impact the final opinion of the radiologist.7-9 Although its contribution to sensitivity and specificity for SpA is unknown, erosions are the most frequent structural lesions seen on imaging. 8 Subchondral marrow edema, sclerosis, and fat deposition are imaging features common to both inflammatory and degenerative/mechanical changes of the axial skeleton. However, the ASAS MRI working group suggests that even a small erosion with a focus of inflammation in the erosion cavity may be specific for SpA. 8
Reliability for detection of erosions has varied widely, possibly due to the complexity of the lesion, challenges distinguishing erosions from other imaging features including subchondral cysts and the application of different lesion definitions.8,9 As such, a literature review was conducted and several experts in the field were consulted to define SIJ erosions on MRI and CT. Using these definitions, the objective of this study was to compare the diagnostic confidence for the detection of SIJ erosions on CT compared to MRI.
This study found that dedicated SIJ CT resulted in significantly more cases with definitive diagnostic confidence than cases with probable or equivocal confidence compared to dedicated SIJ MRI (P<.001). There was also significantly greater interrater agreement for detecting SIJ erosions on CT compared to MRI. Amongst the cases with equivocal findings on MRI, 73.2% had definitive diagnoses on CT. Amongst the cases with equivocal-to-probable diagnoses on MRI, 63.5% had definitive diagnoses on CT. Therefore, it can be concluded that CT significantly increased confidence in detection of SIJ erosions. Amongst the cases with absent-to-equivocal findings of SIJ erosions on MRI, CT detected the presence of erosions in 5.3% of cases. However, amongst the cases with SIJ erosions present on MRI, CT demonstrated the absence of erosions in 50% of cases. Given that CT demonstrated more cases with absent SIJ erosions compared to MRI with significantly more confidence, these findings suggest that patients without definitive SIJ erosions on MRI have a statistically low probability of erosions.
These findings have important implications in the clinical setting. For example, initiating treatment with biologic agents and DMARDs on a patient with “false-positive” findings of SIJ erosions on imaging is expensive, unnecessary, and not without significant potential complications. Judicious use of CT may be useful for confirmation of SIJ erosions, considering the better spatial resolution afforded by CT over MRI. In particular, dual-energy CT may be a strong alternative for the evaluation of SpA, especially due to its excellent ability in visualizing inflammatory and structural changes. Wu et al. investigated a virtual non-calcium technique with dual-energy CT in the detection and grading of subchondral bone marrow edema in patients with axSpA and found that dual-energy CT had excellent diagnostic performance.18,19 Their findings also challenged the role of MRI as the primary imaging modality for evaluation of SpA.18,19 However, radiation exposure from CT examinations, primarily in young patients, is an eminent argument against the routine recommendation of CT for the SIJs. 7
Studies consistently report increased risk of malignancy associated with CT of the pelvis.20-22 Smith–Bindman found the adjusted lifetime attributable risk of cancer in women who underwent pelvic CT examination to be two cancers per 1000 exposed women. 21 The concern about radiation exposure may limit the routine use of CT to assess SIJ erosions, particularly in studies involving healthy patients. 9 The median dose length product (DLP) for the CTs performed in this study was 702 mGy-cm (range, 81–1834 mGy-cm). The DLP found in this study is consistent to what has been reported in the literature. 23
This study has a few limitations. First, this study involved rheumatology referred patients who had a dedicated SIJ MRI and subsequent SIJ CT, likely due to equivocal MRI findings. The findings of this study may not be transferrable to routine non-specialist referred patients with different pre-test probabilities of SpA. Second, both the MRIs and CTs were evaluated in isolation for the presence or absence of erosions and not the global assessment that is advocated in clinical practice. Third, there is a possibility that patients may have developed SIJ erosion findings in the time interval between initial SIJ MRI and subsequent SIJ CT. However, Giejer et al. found that only 3.0% of patients with symptoms suggestive of inflammatory back pain and multiple SIJ CTs progressed from normal or equivocal to unilateral or bilateral sacroiliitis at a median of 5 years between examinations (range, 1–21 years). 12 The interval between initial SIJ MRI and CT in this study ranged from 5.6 to 50.3 weeks. Finally, the MRI protocol did not employ volumetric MR imaging that may improve the diagnostic confidence of erosions.
In summary, low-dose CT led to significantly increased diagnostic confidence and higher interrater reliability for the detection of SIJ erosions compared to MRI. Targeted use of CT may be useful for the evaluation of SIJ erosions in patients with equivocal MRI findings.
Footnotes
Acknowledgments
The authors would like to thank Dr Kim Madden from the Department of Health Research Methods of McMaster University (Hamilton, ON) for her contribution in the statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect tothe research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship,and/or publication of this article.