
Abstract
Background:
Intravenous [IV] esmolol, an alternative to IV metoprolol for coronary computed tomography angiography [CCTA], has shorter half-life that decreases the risk of prolonged hypotension. The primary aim was to prospectively compare IV esmolol alone to IV metoprolol alone for effectiveness in achieving heart rate [HR] of 60 beats per minute[bpm] during CCTA. The secondary aim was to compare hemodynamic response, image quality, radiation dose and cost.
Materials and Methods:
Institutional Review Board approved prospective randomized study of 28 CCTA patients medicated in a 1:1 blinded match with IV esmolol or IV metoprolol to achieve HR of 60 bpm. Serial hemodynamic response was measured at 6 specified times. Two cardiac radiologists independently scored the image quality.
Results:
Both IV esmolol and IV metoprolol achieved the target HR. IV esmolol resulted in significantly less profound and shorter duration of reduction in systolic blood pressure [BP] than IV metoprolol with a difference of -10, -14 and -9 mm Hg compared to -20, -26 and -25 mmHg at 2, 15 & 30 min respectively. No significant difference in HR at image acquisition, exposure window, radiation dose and image quality. Although IV esmolol was expensive, the overall cost of care was comparable to IV metoprolol due to shortened post CCTA observation period consequent to faster restoration of hemodynamic status.
Conclusion:
Comparison of IV esmolol and IV metoprolol demonstrate that both are effective in achieving the target HR but significantly faster recovery of HR and BP in patients who receive IV esmolol was found.
Introduction
Coronary computed tomography angiography [CCTA] is established for non-invasive evaluation of coronary arteries in the appropriate clinical setting. 1 Many centres utilize metoprolol as the drug of choice for heart rate [HR] control during CCTA.2,3 Intravenous [IV] metoprolol shortens the preparation time for CCTA, is effective and safe, even at high doses. 4 CCTA is being increasingly used in diverse patient populations who are at risk of sustained bradycardia and hypotension such as elderly, debilitated patients and patients who have impaired cardiac output due to reduced ventricular function. Hence the long plasma half-life of 3-7 hours 5 for IV metoprolol is of concern. IV esmolol is an attractive alternative to IV metoprolol due to a rapid onset of action of 1-4 minutes and a very short half-life of 4-9 minutes 6 and has been shown to be effective and safe during CCTA. 7 However, there has been no direct head to head comparison of these two drugs. The primary aim of this study was to prospectively compare the efficacy of IV esmolol alone to IV metoprolol alone in achieving a target HR of 60 bpm during CCTA. The secondary aims were to compare the HR and blood pressure [BP] response, image quality, patient radiation dose and overall cost of IV esmolol to IV metoprolol.
Materials and Methods
Patient Selection
The study was approved by the Institutional Research and Ethics Board and performed in the Department of Medical Imaging (BLINDED) from January 2017 to June 2017.Written informed consent was obtained from each patient by a study coordinator. Patients clinically referred for CCTA of native coronary arteries were prospectively randomized using a random number generator, to equal cohorts to either of the limb. The randomisation list was known only to a research assistant who was not involved in any other part of the study. Patients were blinded to which beta blocker was administered. The staff supervising the CCTA examination was aware of which drug was administered, but was not involved in any other aspect of the study. Patients were included if they were aged ≥ 18 years, had a HR >60 bpm, had sinus rhythm and normal renal function. Patients were excluded if they were already taking an oral beta blocker or had contraindications to beta blockers, 8 had a baseline HR <60 bpm, systolic BP < 100 mmHg, or uncontrolled atrial fibrillation. Each patient completed the six item Spielberger State-Trait Anxiety Inventory (STAI) self-evaluation questionnaire prior to the procedure. 9 This was done to compare both patient cohorts for anxiety levels prior to CCTA. In brief, the STAI has six questions; three questions address high anxiety levels and 3 questions assess low anxiety levels. Each question is scored from 1- 4 where a score of 1 represents strong disagreement and a score of 4 represents strong agreement with a given high or low anxiety level statement.
Heart Rate Control
All patients received standard instructions and preparation for CCTA. Once the patient was on the CT table, an 18-gauge IV cannula was placed in a right antecubital vein and three precordial leads were attached and adjusted to maximize the ECG signal. The baseline blood pressure (BP #1) and heart rate (HR#1) were automatically taken and recorded. Patients with HR ≤ 60 bpm were excluded from the study. Patients who were randomized to receive IV metoprolol, received a slow IV bolus of 5 mg over 2 minutes, with a repeat dose of 5 mg every 4 minutes until the target HR of 60 bpm was achieved or until a maximum of 40 mg had been given. Patients randomized to receive IV esmolol were given a slow IV bolus of 100 mg and repeat aliquots of 100 mg over 2 minutes, every 2 minutes until the HR of 60 bpm was reached or a maximum dose of 400 mg had been given. A self-inflating cuff on the left upper arm automatically monitored the systemic blood pressure and HR every 60 s during IV beta blocker administration, to ensure that the systolic BP was maintained >100 mmHg. Following this, 0.3 mg of sublingual nitroglycerine was given for coronary vasodilation. Subsequently BP #2, HR #2, were recorded after the administration of beta blocker and BP #3 and HR #3 were recorded during image acquisition. Following the CCTA, the patient was observed by a nurse for 30 minutes, or until hemodynamic status was restored, and vital signs were monitored. The HR (# 4, 5, 6) and BP (# 4, 5, 6) were taken and recorded at 2 minutes, 15 minutes and 30 minutes respectively following CCTA. The patient was discharged as soon as they felt well and in the absence of systemic hypotension. The cost of the IV beta blocker and the overall cost of care were calculated for each group. The algorithm of patient selection and HR control is summarized in Figure 1.
Algorithm of patient selection, beta blocker administration and monitoring of HR & BP for CT Coronary Angiogram.
Image Acquisition
All CCTA studies were performed on a wide volume multidetector computed tomography [MDCT] scanner (Aquilion ONE, Canon Medical Systems, Ottawa, Japan) using 280-320 x 0.5 mm detectors and a standard procedure for x-ray dose adaptation to individual patient body habitus to ensure diagnostic image quality. 10 All scans were acquired using prospective ECG gated image acquisition with x-ray exposure window being automatically optimized to the patient’s HR using pre-determined manufacturer settings. 50-70 ml of iodinated, non-ionic water-soluble contrast medium (Iopromide 370 mg iodine/mL) was power injected at 4.5-5.0 mL/s, determined by patient bodyweight, followed by a 20 ml saline push. Image acquisition was triggered using a contrast threshold technique in the descending aorta initiated by a luminal contrast threshold of +130 HU at 120 kV, ensuring acquisition at peak arterial opacification.
Image Analysis
Two radiologists with 3 and 7 years of reading CCTA were blinded to the type of beta blocker administered, and independently scored the image quality of the CCTA. Image quality was analysed using an 18 segment model,11,12 0.5/0.3 mm trans-axial images, multiplanar reconstructions and curved planar reformatted images. The image quality of each segment was evaluated using a 4 point scale 13 where 4 = excellent (excellent attenuation of vessel lumen and clear vessel definition with barely perceived image noise), 3 = good (good attenuation of vessel lumen and well- maintained vessel wall definition with minimal image noise), 2 = fair (some limitation in vessel wall definition and contrast resolution with moderate image noise that would affect diagnosis) and 1= poor (impaired image quality with severe image noise). Prior to image analysis, both radiologists participated in a calibration session during which they evaluated a separate series of 10 CCTA examinations that had been independently selected to demonstrate image quality scores from 1-4. Excellent intra observer and interobserver agreement was observed in these assessments. These CCTA studies did not form part of the trial. The number of analysable segments in any particular CCTA was multiplied with a maximum image quality score of 4, to obtain the maximum possible CCTA score for that study. Missing segments or segments smaller than 1.5 mm diameter were excluded from image analysis. Total score for each CCTA was calculated by adding the individual segment quality scores. Diagnostic score for each CCTA is obtained on dividing total score obtained by the maximum possible score for that CCTA (for example, in a CCTA with 17 analysable segments, maximum possible CCTA score is 68. If the total score obtained is 62, then diagnostic score is 62 / 68 = 0.91). Hence the maximum diagnostic score for any CCTA was 1. The mean image quality score per coronary artery segment for each patient was calculated from the separate radiology reads. The nomenclature of the segments was defined by consensus between both radiologists in cases with congenitally abnormal coronary arteries.
Radiation Dose
The x-ray tube exposure parameters (kVp, mAs) were determined by patient body habitus, the x-ray exposure window varied with the patient’s heart rate and the scan length varied with the z-axis length of the heart. Together these parameters determined the dose length product [DLP] in mGy.cm, that was recorded from the CT console. The effective dose was calculated as the product of the DLP and an organ weighting factor of 0.014.14,15
Cost
Although the cost of the IV esmolol was higher than that of IV metoprolol, the cost of nursing supervision in the recovery room following CCTA were less for IV esmolol with a mean cost of $51.15 (30.6) in Canadian dollars [CAD] compared to the mean cost of IV metoprolol CAD $56.79 (20.6) due to faster restoration of hemodynamic status. Therefore, the overall cost of care was comparable for both medications.
Statistical Analysis
The sample size was calculated at 90% power. All continuous variables were assessed for normal distribution and presented as mean ±standard deviation and categorical variables represented as median (interquartile range [IQR]). The difference of the mean between the groups was calculated using the independent T- test. Chi square and Fischer’s exact test were used to determine the significance of the relationship between categorical variables. Cohen’s kappa was calculated to assess the interobserver agreement. A p value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 16.0 for Windows (SPSS, Chicago, IL).
Results
Baseline Characteristics
A total of 28 patients (15 men, 53%), with 14 patients in each arm, were included in the study. The median (IQR) age of the cohort was 53.5 years (16 years). There was no significant difference in age, gender or ethnicity between the two groups as shown in Table 1. There was no statistically significant difference in the pre procedure low anxiety score between the two groups. The high anxiety score was higher in the metoprolol group than in the esmolol group, but this was not statistically significant. The mean (standard deviation [SD]) dose of IV esmolol and IV metoprolol used in this study was 217.86 mg (132.44 mg) and 26.79 mg (15.01 mg) respectively.
Comparison of Demographic Characteristics, Radiation Dose, Image Quality, Cost of Beta Blocker Between the IV Esmolol and IV Metoprolol Cohorts.
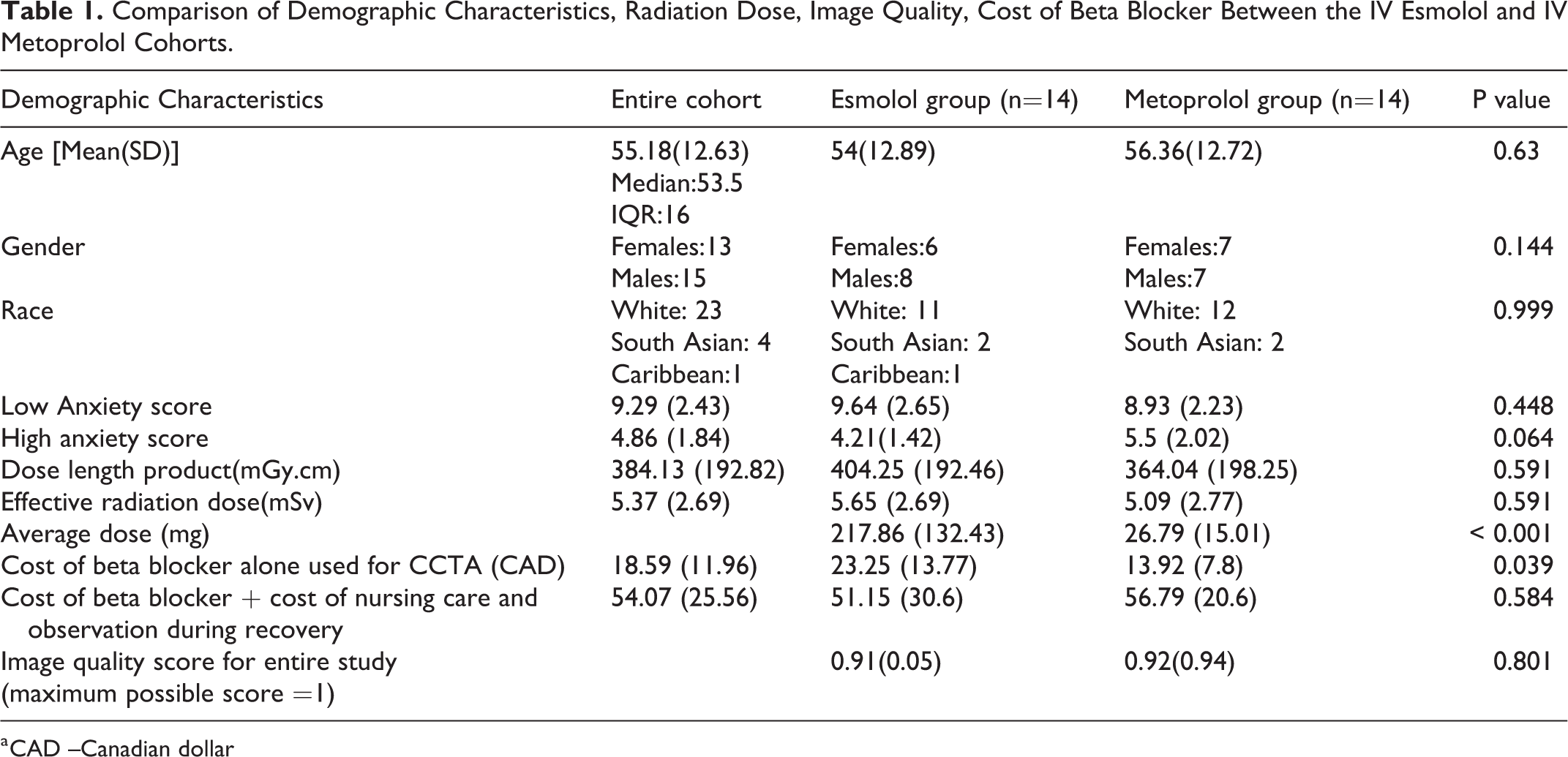
a CAD –Canadian dollar
Hemodynamic Parameters
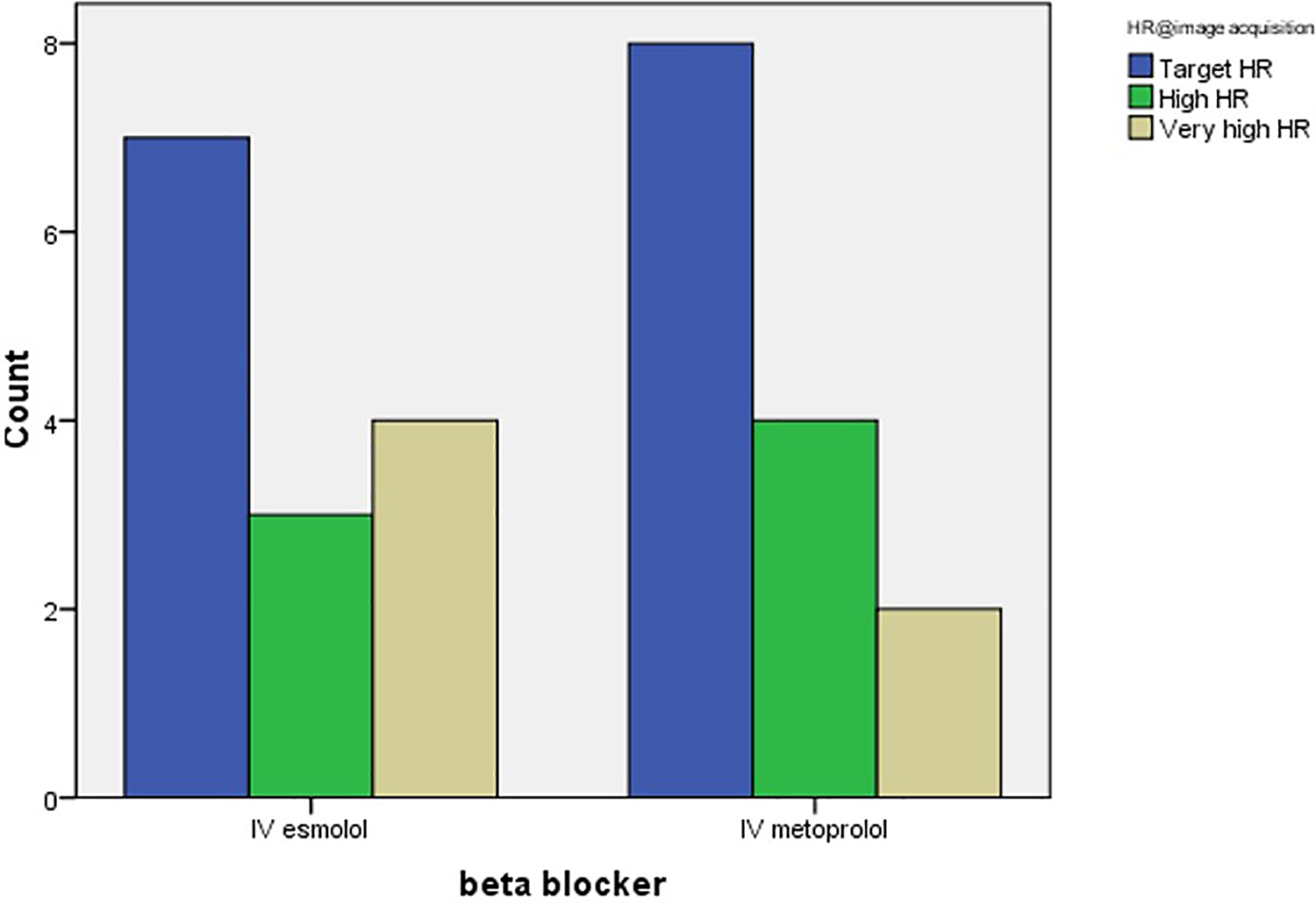
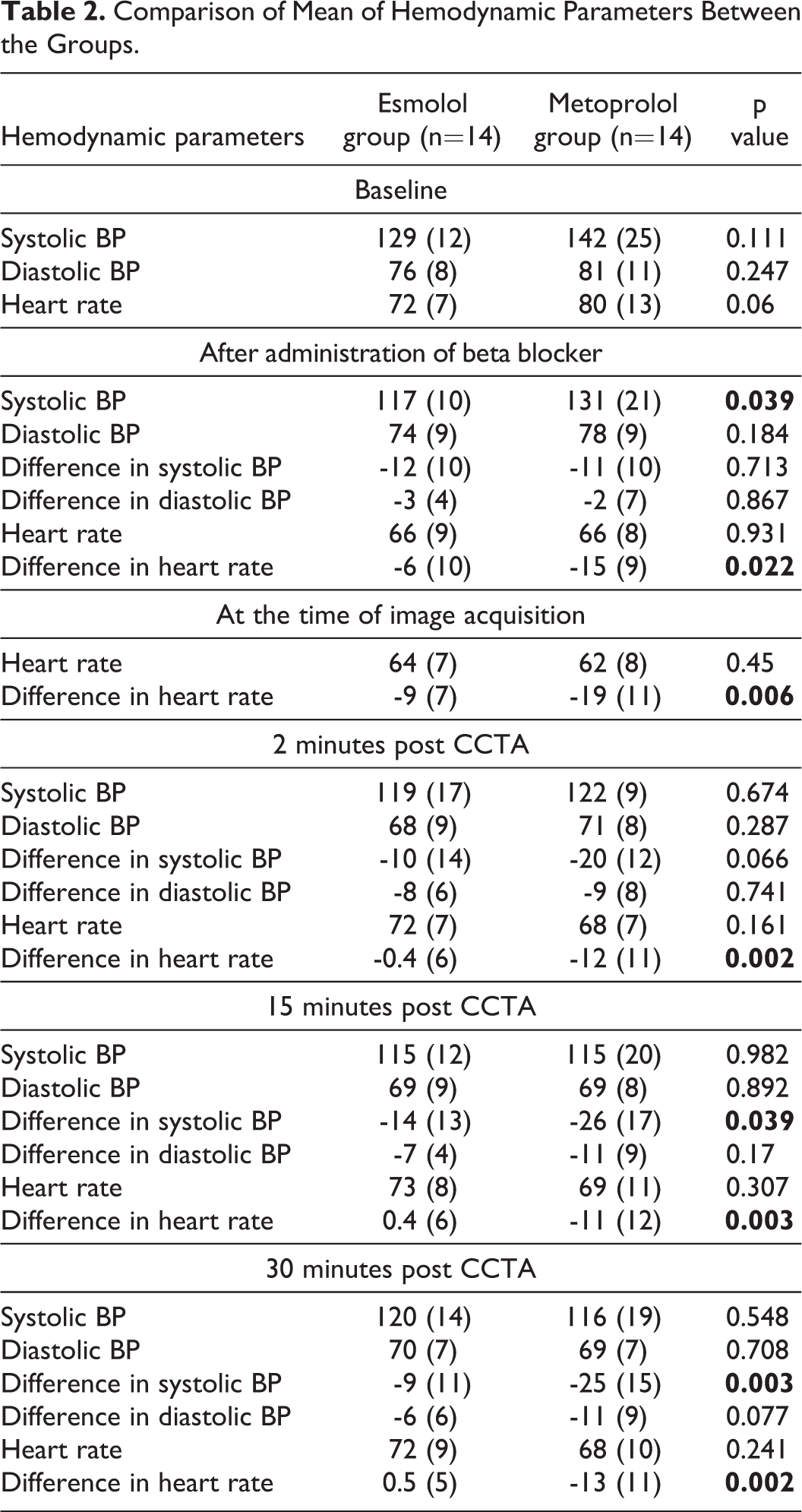
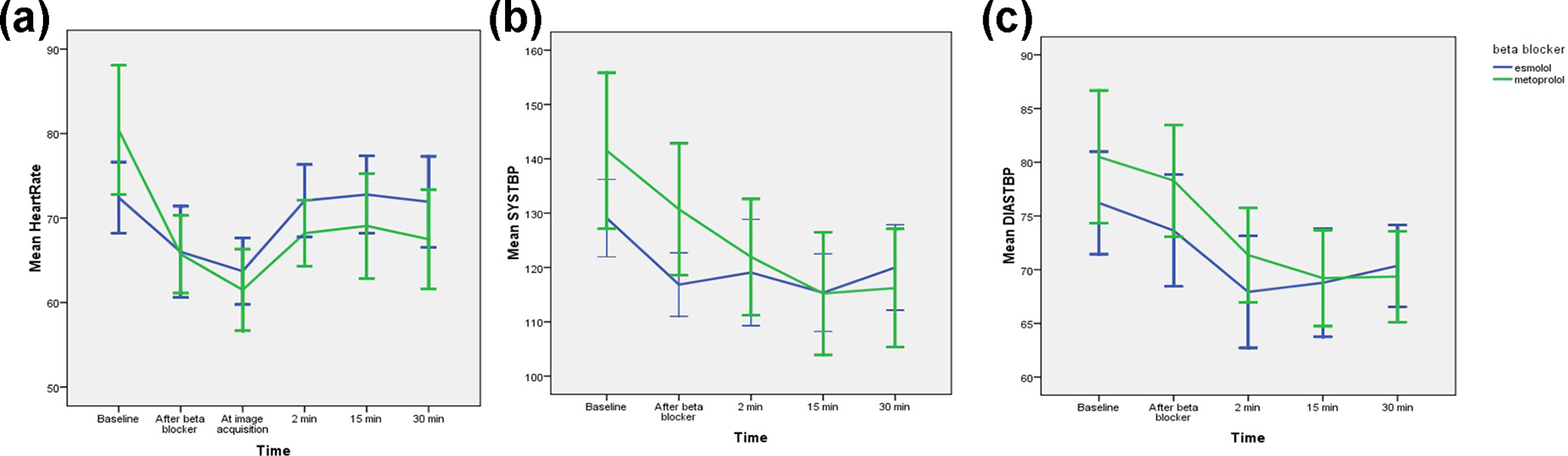
A comparison of the hemodynamic response in the IV esmolol group and IV metoprolol cohort is presented in Table 2. Although the IV metoprolol patients had higher BP and HR at baseline, the response to IV beta blockade was comparable with 15 subjects (54%) achieving a target HR of 60 bpm at the time of image acquisition; 7 patients (50%) received IV esmolol and 8 patients (57%) received IV metoprolol. There was no significant difference in the mean (SD) HR between the groups, at the time of image acquisition; esmolol: 64 (7); metoprolol: 62 (8) (p =0.45) [Figure 2]. Both IV esmolol and IV metoprolol resulted in a similar reduction in systolic BP of 11-12 mmHg prior to CCTA. IV esmolol resulted in a significant (p < 0.05) and quicker restoration of baseline systolic BP than IV metoprolol with a difference (baseline - time point) of -10, -14 and -9 mmHg compared to -20, -26 and -25 mmHg at 2, 15 and 30 min respectively. There was also quicker restoration of baseline heart rate in the IV esmolol group compared to the IV metoprolol group with a difference (baseline – time point) of -0.4, -0.5 and -0.5 bpm compared to -12, -11 and -13 bpm respectively at 2, 15 and 30 mins respectively. At 2 minutes, 12 (84%) patients in the IV esmolol group had restoration of the baseline HR compared to 4 (28%) patients in the IV metoprolol group, and at 30 minutes, 13 (93%) patients in the IV esmolol group had restoration of baseline HR compared to 5 (36%) patients in the IV metoprolol group. No adverse event occurred in either group.
Comparison of Mean of Hemodynamic Parameters Between the Groups.
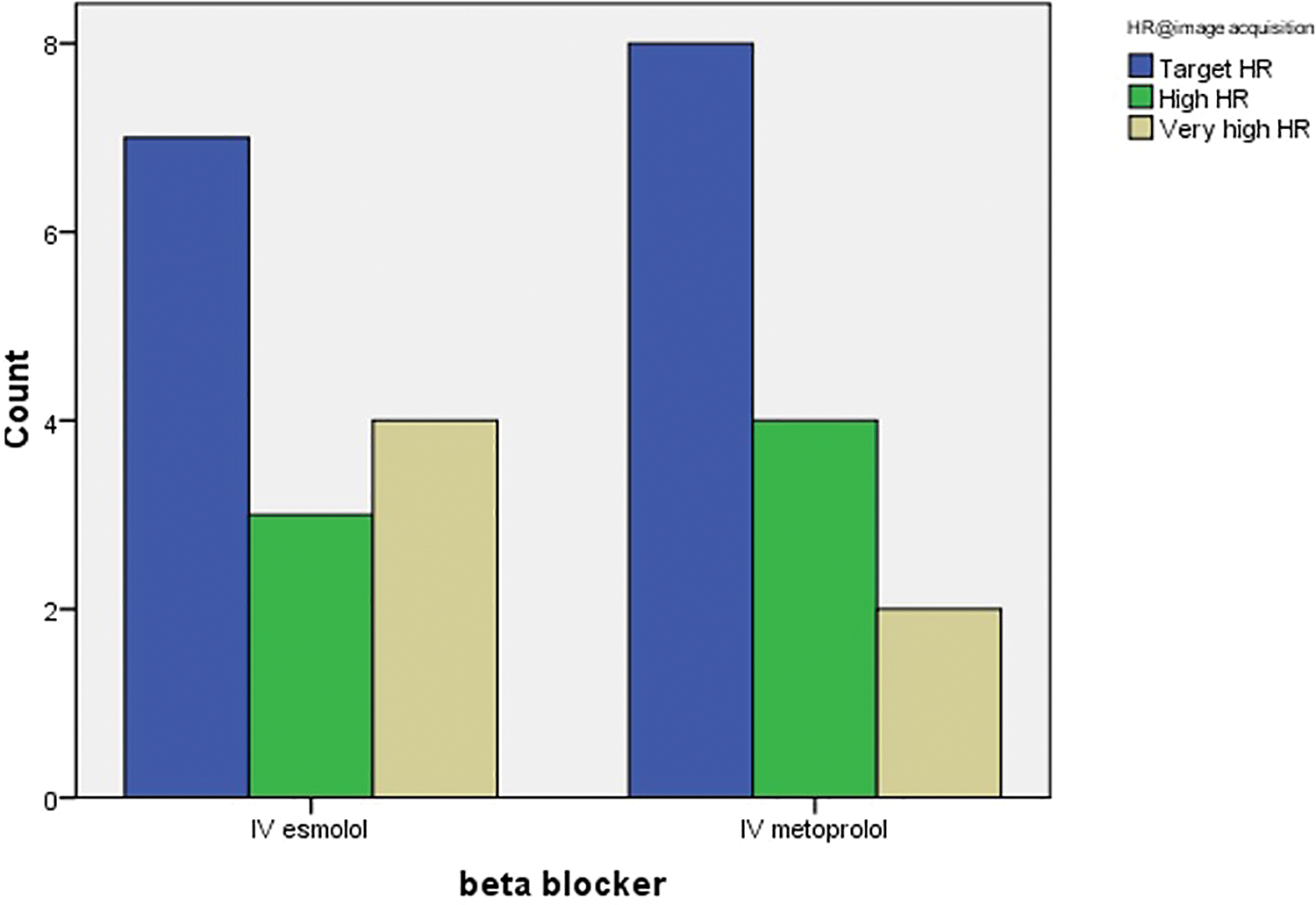
Heart rate at image acquisition of CCTA in two groups.
Comparison of heart rate, systolic BP and diastolic BP between the two groups at baseline, after administration of IV beta-blocker, at the time of image acquisition (for HR only), 2 min, 15 min and 30 min after CCTA image acquisition with confidence intervals are demonstrated in Figure 3A-C.
Radiation Dose
The x-ray exposure windows used in these patient cohorts were determined by the manufacturer settings according to the patient HR and included the following ranges: 73-77%, 70-80%, 60-80%, 40-80% and 35-80% phases of the R-R interval. The 70-80% exposure window was used in 57% of the IV esmolol group and in 64% of the IV metoprolol group as demonstrated in Figure 4, with no significant difference between the two groups (p =0.81) . The mean (SD) radiation dose (mGy.cm) and the mean (SD) effective radiation dose (mSv) received by the IV esmolol patients was 404 (192) mGy.cm and 5.7(2.3) mSv; and by the IV metoprolol patients was 364 (198) mGy.cm and 5.1(2.7) mSv respectively, with no significant difference between the two groups (p= 0.59).
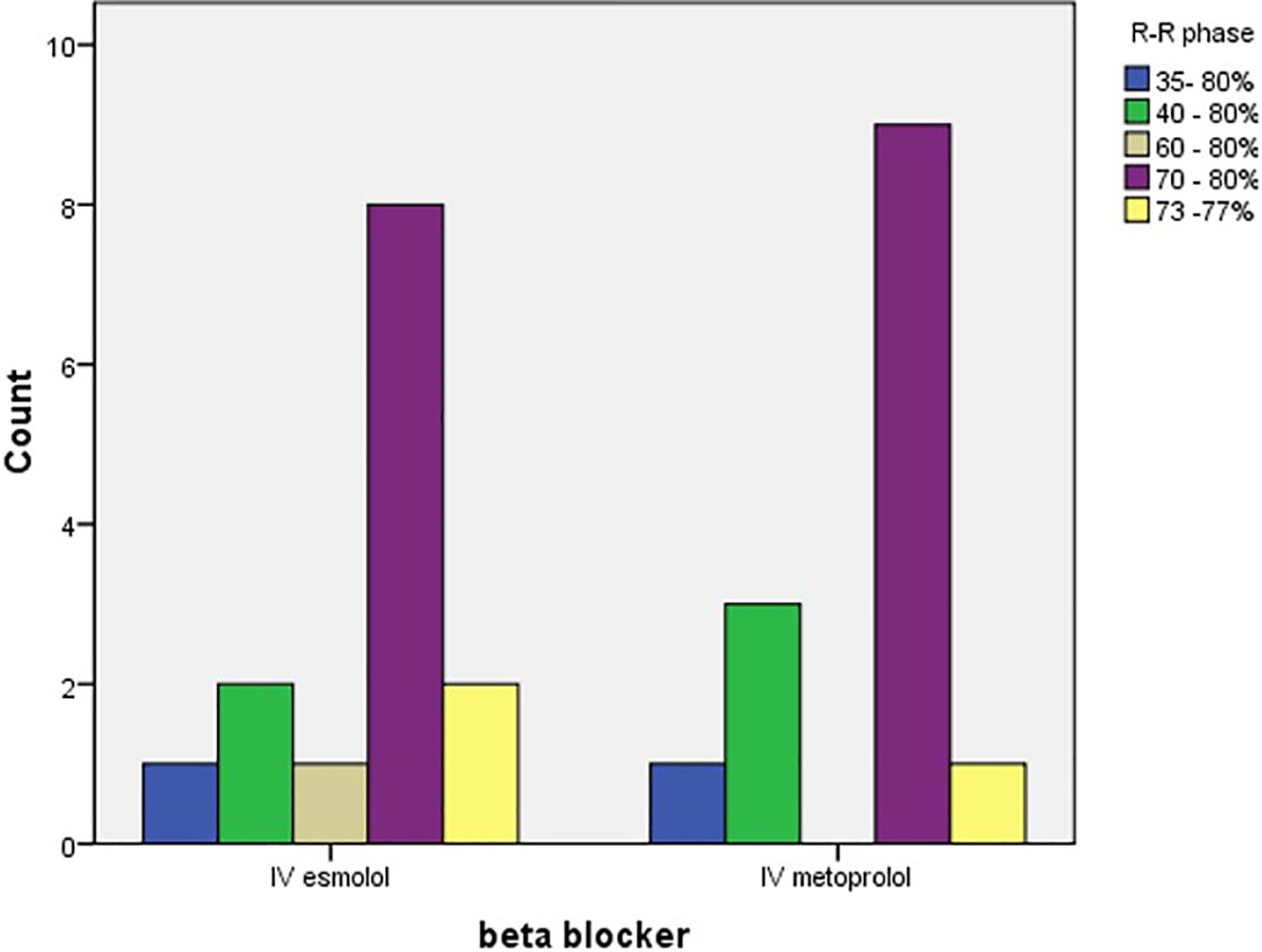
Exposure window used during image acquisition in two groups.
Image Quality
113 (22%) coronary segments from a total of 504 potential segments were excluded from the study as they were absent or too small to analyse (<1.5 mm). All of the evaluated coronary segments were of diagnostic image quality. There was no significant difference in the image quality of the coronary segments between the two groups with mean (SD) diagnostic scores for esmolol of 0.912 (0.05) and for metoprolol of 0.919 (0.94) as shown in Table 3. There was moderate to strong inter observer agreement in the image quality scoring between the two radiologists. There was a statistically significant strong inter observer agreement, in the following coronary segments: left main, proximal RCA, the first and second diagonal branches, the second obtuse marginal branch and the ramus intermedius.
Image Quality Score Between the Two Groups and Interobserver Agreement for the Cohort.
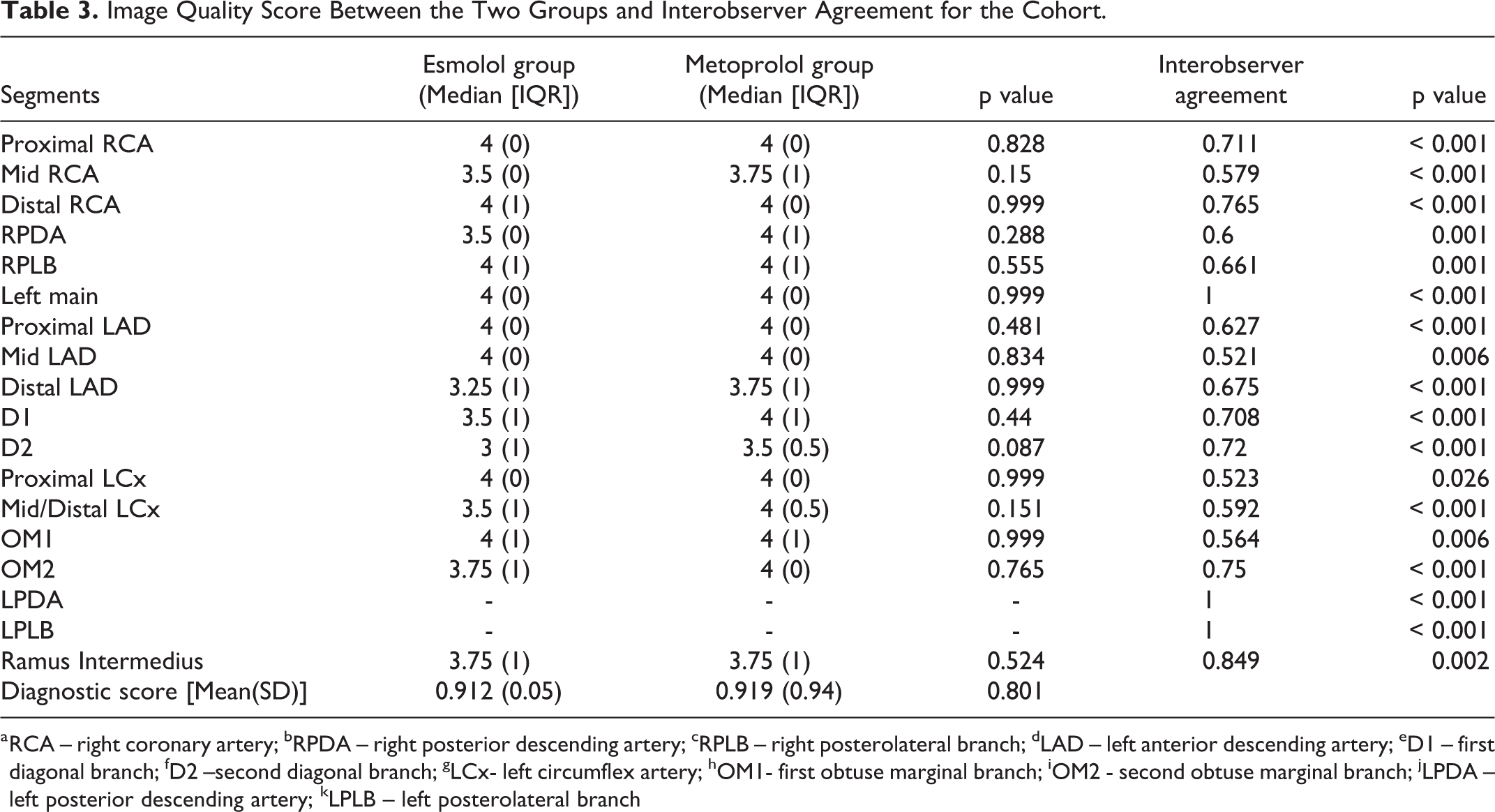
a RCA – right coronary artery; bRPDA – right posterior descending artery; cRPLB – right posterolateral branch; dLAD – left anterior descending artery; eD1 – first diagonal branch; fD2 –second diagonal branch; gLCx- left circumflex artery; hOM1- first obtuse marginal branch; iOM2 - second obtuse marginal branch; jLPDA – left posterior descending artery; kLPLB – left posterolateral branch
Discussion
This is the first prospective randomized control trial to compare the clinical effectiveness and image quality of IV esmolol alone to IV metoprolol alone, without prior administration of oral beta blocker, for CCTA. This study has highlighted that both medications have comparable efficacy in achieving the target heart rate of 60 bpm but that the significantly shorter half-life of IV esmolol results in a faster restoration of heart rate and systolic blood pressure towards baseline values.
Intersubjective variability in the effectiveness of beta blockers has been previously described 16 and ethnic background has been demonstrated to influence the responsiveness to oral beta blockers predominantly due to variation in liver activation of the inactive oral compound. 17 The IV preparation does not have similar limitations.
There are two previous studies that have demonstrated the safety and efficacy of using IV esmolol in achieving a target heart rate for CCTA.18,7 Degertekin et al [18] performed CCTA in 391 patients using 64 MDCT and IV esmolol with retrospective data acquisition. The target heart rate of 65 bpm was achieved in 52% of the patients using a mean (SD) dose of 158 mg (55 mg) of IV esmolol with a mean effective radiation dose of 5.7 (2.3) mSv. Wang J D [6] performed CCTA in 232 patients using a dual source CT system and IV esmolol. In their study, the target heart rate of 65 bpm was achieved in 85% of the patients using a mean (SD) dose of 57.26 (15.39) mg of IV esmolol with a mean effective radiation dose of 2.28 (0.02) mSv. In both of these studies, the safety of IV esmolol was established in a large cohort of patients, however neither study provided a head-head comparison of IV metoprolol to IV esmolol.
The current study demonstrated a significantly faster restoration of the baseline hemodynamic parameters in the IV esmolol group compared to the IV metoprolol group. The difference between the baseline heart rate and heart rate at 30 mins after CCTA showed a significantly prolonged bradycardia (<60 bpm) in 2 (14%) patients in the IV metoprolol group compared to none in the IV esmolol group with a mean heart rate of 68 bpm in the IV metoprolol group compared to 72 bpm in the IV esmolol group at 30 minutes. There was prolonged hypotension (systolic BP < 100 mmHg) in 3 patients (21%) in the IV metoprolol group compared to none in the IV esmolol group. In a larger cohort study of 1871 patients done to assess the safety of IV metoprolol in CCTA, one patient had an adverse event requiring hospital admission.19,20 Sustained and symptomatic bradycardia has been reported following the administration of IV metoprolol.20,21 For the majority of patients having CCTA, the difference in hemodynamic response between IV esmolol and IV metoprolol is unlikely to be clinically significant; however, for elderly patients and patients with impaired left ventricular function who are at increased risk of falling from the dampened systolic BP and heart rate recovery, IV esmolol may provide a safer alternative to IV metoprolol due to the quicker restoration of baseline hemodynamic parameters.
In the current study, both IV beta blockers were equally effective in achieving the target heart rate at the time of image acquisition. This is contrary to the study by Maurovich-Horvat et al, 21 where 89% of patients receiving IV esmolol achieved the target heart rate of 65 bpm compared to 78% of patients given IV metoprolol. The dose of IV esmolol used was 100-500 mg with a mean (SD) dose of 325.6 (158.4) mg compared to 5- 20 mg of IV metoprolol with a mean dose of 10.7 (6.3) mg. The dose of IV esmolol used was higher compared to the current study (217.86 [132.44] mg) whereas the dose of IV metoprolol was lower compared to the current study (26.79 [15.01] mg).
In the current study, although the heart rate at the time of image acquisition was similar in both groups, the reduction in HR from baseline was more pronounced in the IV metoprolol group compared to the IV esmolol cohort due to a higher pre-study HR in the metoprolol group. This could be related to the higher pre-test anxiety scores in the metoprolol group.
Although the shorter half-life of IV esmolol is favoured for improved patient safety from reduced risks of hypotension and bradycardia following CCTA, the shorter duration of action necessitates that the CCTA scan is performed during the peak action time of IV esmolol and necessitates an efficient clinical operation.
The mean patient radiation dose in the current study was slightly higher than previous studies which were performed using a similar CT platform.22,23 This difference is likely to reflect a difference in the body habitus of the study population and a difference in heart rate at the time of image acquisition. Twenty-one per cent of the current study population had a heart rate above 70 bpm at the time of image acquisition resulting in a wider exposure window; a multi heart beat acquisition was used in 8 patients. Tomizawa et al recorded a similar experience using 320 MDCT to perform cardiac CT in 123 patients with 23 (18.6%) patients requiring multiple heart beat acquisitions due to a heart rate >75 bpm. 24 In the current study, all of the examinations were of diagnostic image quality despite the high heart rate in one fifth of the patient cohort.
There are a few limitations to this study. The trial was performed in a single tertiary centre, hence multi centre trial will be required for further validation of results. The study has a relatively smaller sample size; and a larger patient cohort may produce different results. The sample size might affect the power to detect a statistically significant difference in the acquisition time HR between IV metoprolol and IV esmolol cohorts. We believe that this difference would not be clinically significant as the haemodynamic responses observed during this study are as expected from the known pharmacokinetics of the medications and in line with previous publications.
Conclusion
IV esmolol and IV metoprolol are equally effective in achieving a target heart rate of 60 bpm for CCTA but there is a significantly faster recovery of heart rate and systolic blood pressure in patients who receive IV esmolol. There is no significant difference in the image quality and radiation dose from use of the two medications. The shorter recovery time for restoration of hemodynamic status with IV esmolol is reflected in a reduced cost of nursing care for post procedural observation. Hence, IV esmolol can be used as a safer, cost effective alternative to IV metoprolol while performing CCTA in patients at risk of prolonged bradycardia and hypotension.
Footnotes
Authors’ Note
Leena Robinson Vimala is also affiliated with Department of Radiology, Christian Medical College, Vellore, Tamil Nadu, India.
Acknowledgements
The authors acknowledge the cardiothoracic imaging fellows and technologists in CT Cardiac suite of Toronto General Hospital, for their help and support during the research.
Authors acknowledge the technologists in cardiac CT suite in Toronto General Hospital for their help during the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.