
Abstract
During the COVID-19 pandemic, breast imaging must be performed using safe practices. Balancing the need to avoid delays in the diagnosis of breast cancer while avoiding infection requires careful attention to personal protective equipment and physical distancing and vigilance to maintain these practices. The Canadian Society of Breast Imaging/Canadian Association of Radiologists guideline for breast imaging during COVID-19 is provided based on priority according to risk of breast cancer and impact of delaying treatment. A review of the best practices is presented that allow breast imaging during COVID-19 to maximize protection of patients, technologists, residents, fellows, and radiologists and minimize spread of the infection. The collateral damage of delaying diagnosis of breast cancer due to COVID-19 should be avoided when possible.
COVID-19 outbreak has emerged as the single most important health crisis defining this century. As of April 30, 2020, it has infected 3 246 103 individuals, caused 229 239 deaths, and affected 211 countries worldwide. In Canada, 53 236 people are confirmed to have been infected, with 3184 deaths 1 : the first case confirmed on January 25, 2020, 2 and the first death on March 9, 2020. The World Health Organization (WHO) on March 11, 2020, declared the novel coronavirus (COVID-19) outbreak a global pandemic. 3 COVID-19 illness is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 4 Symptoms include cough, difficulty breathing or shortness of breath, fever, chills, repeated shaking with chills, sore throat, new loss of taste or smell, muscle pain, headache. 5 About 20% of patients also report diarrhea. 6 Doctors have noted erythematous skin lesions on the toes (“Covid Toes”) and sometimes fingers of children. 7 The predominant method of transmission of the virus SARS-CoV-2 is droplet or direct/indirect contact transmission. When an infected person expels virus-laden droplets and someone else inhales them, the virus SARS-CoV-2 enters the nose and throat. Other mechanisms of infection include contact with an infected surface, where a person can get COVID-19 by touching a surface or object that has the virus on it and then touches their own mouth, nose, or eyes. 8 The virus may survive for up to 48 hours on steel and 72 hours on plastic surfaces. 9
Health Care Workers
Human-to-human transmission occurs, and health care workers have been shown to be highly vulnerable to contacting and dying from COVID-19 infection. The first medical doctor to succumb to the disease was the Chinese ophthalmologist Dr Li Wenliang from Wuhan, China, who contacted the illness after treating his patient, a storekeeper from the Huanan Seafood Market. It is likely that this patient’s high viral load exacerbated the severity of Li’s infection, and he died at age 33 years of COVID-19 on February 7, 2020. 10
People are often infectious 2 to 3 days before they exhibit symptoms. 11 This differs from SARS where infectiveness increased 7 to 10 days after symptom onset. 12 It is found that the proportion of presymptomatic transmission ranged from 46% to 55% 11,13 Spread from asymptomatic carriers is estimated at 25%. 14 Given that asymptomatic individuals may spread 50% of infections, screening for symptoms alone does not provide protection for all people.
By simply speaking, someone can transmit the virus. 15 Thus, mitigating the possibility of acquiring or spreading the infection by unsuspecting patients to exposed health care workers (HCWs) is of paramount importance. While there may be continued transmission of infection for up to 21 days by patients who are symptomatic, 11 this may be reduced by careful screening of patients for any symptoms before they undergo an imaging examination.
A case report from Singapore described the exposure of 41 HCWs who wore various forms of personal protective equipment (PPE) to care for an undiagnosed COVID-19 patient. 16 In this report, 35 (85%) of 41 of the HCW wore a surgical mask during several significant aerosol-generating procedures, including intubation, and the remainder wore N95 masks. None of the HCW developed symptoms of the infection and none were found to be infected on serial testing for coronavirus.
Breast imaging requires very close contact with patients. There is no option of physical distancing when performing a mammogram or breast ultrasound, where the patient’s face may be as close as 20 to 30 cm to the face of the radiologist or sonographer/technologist performing the study. Similarly, during ultrasound, stereotactic, and magnetic resonance imaging (MRI)-guided breast procedures, including biopsies, drainages, and clip placements, an interventional breast imaging radiologist may be within 30 cm of their patient’s face.
It has been estimated that the risk of becoming infected by the novel coronavirus depends on the physical proximity to the patient. The Occupational Information Network developed under the sponsorship of the US Department of Labor/Employment and Training Administration calculated occupational risk scores from 0 to 100 based on 3 risk factors: physical proximity, exposure to disease and infections, and daily contact with others. Among the highest professions at risk are dental hygienists at 99, dentists 92, family physicians 90, nurses 86, radiology technologists 84, and sonographers 80. 17 Two mammography technologists died of COVID-19 in March, the first medical personnel in the state of Georgia to die of the disease. 18 Nosocomial infections may be an important mechanism of infection. One infected worker with a mild symptom of a runny nose may potentially infect many patients contacted during a shift. For this reason, the recommendations are to widely test all HCWs, even with mild symptoms. 19
The mortality rate of COVID-19 is estimated at 3% to 4% and increases with age (>60 years) and chronic medical conditions. 20 Patients with cancer are more susceptible to infections. This is because of their systemic immunosuppressive state caused by the malignancy and anticancer treatments, such as chemotherapy or surgery. This is no different with COVID-19. A report of 105 hospitalized patients with cancer and 233 hospitalized patients without cancer, all infected by the SARS-CoV-2 virus, were collected from 14 hospitals in Hubei province in China. 21 Compared with COVID-19 patients without cancer, patients with cancer had higher observed death rates (odds ratio [OR]: 2·88, 95% CI: 1.20-689], P =·02), higher rates of intensive care unit admission (OR: 2.38, 95% CI: 1.23-4.61, P =·01), higher rates of having at least one severe or critical symptom (OR: 2.60, 95% CI: 1.53-4.41, P <·01), and higher chances of needing invasive mechanical ventilation (OR: 4·75, 95% CI: 160-14.41, P = .01). Although the reported death rate of 2% to 3% was in the general population, patients with cancer and COVID-19 not only had a nearly 3-fold increase in the death rate than that of COVID-19 patients without cancer but also tended to have a much higher severity of their illness. Furthermore, patients with cancer also had a 10-fold higher incidence of nosocomial SARS-COV-2 infections than patients without cancer. 22 It is therefore critical to take careful precautions with patients with cancer and avoid unnecessary contact with all immunosuppressed patients and elderly patients.
Personal Protective Equipment
Personal protective equipment, which includes surgical mask, eye protection, gloves, gown, and meticulous hand hygiene, is likely effective in protecting HCW from COVID-19. 23 Professional and homemade face masks have been shown to reduce exposure to respiratory infections among the general population. 24 Although there is some protection afforded from others by wearing even a tea towel mask, the impact is much higher if the infected person wears the mask, reducing the number of droplets leaked into the surroundings at the end of a 3-hour period with no physical activity. 24
Physical Distancing Measures
Avoiding others by physical distancing, keeping a distance between you and others, is the best method to avoid being exposed to the coronavirus and to slow its spread of infection locally and globally. 8 It is especially important in people who are at a higher risk of the infection. This includes pregnant women, immunosuppressed patients receiving breast cancer treatment, older age individuals, and someone with comorbidities. This should be considered when scheduling vulnerable staff and when imaging patients. 25
There should be a benefit to increasing the spatial separation between desks and workstations as well as individuals (eg, employees, patients) from each other, ideally a 2-m separation should be maintained, unless there is a physical barrier (eg, cubicle, Plexiglas window). 23,26
Teams Approach
Public health authorities mandate that anyone who had close contact with a patient with confirmed COVID-19 while not wearing PPE self-isolate at home for 14 days. 27 This has the potential to effectively close down a small imaging department or section and places an incredible strain on the ability to have enough clinicians available to provide health care. 28 Breast imaging team restructuring during a pandemic optimizes patient care and ensures the well-being and vitality of the workforce while ensuring the entire workforce is not compromised.
Resuming With Screening and Lower Priority Breast Imaging
A key metric for the success of physical distancing is whether critical care facilities are exceeded. Because 50% of infections may be presymptomatic or are asymptomatic, limiting imaging to asymptomatic patients will not reduce the spread of infection. It has been suggested that intermittent distancing will be required into 2022 unless critical care capacity is increased substantially or a treatment or vaccine becomes available. 29
This means that crowded waiting rooms of patients and rapid screening using shared mammography units among technologists will likely have to change. A return to the previous efficient way of performing breast imaging will likely not be possible in the foreseeable future. We will have to adapt to this new reality. Table 1 demonstrates scenarios of safe return to breast imaging. This may include spreading breast screening examinations over longer times during the day into evening hours, staggering scheduled visits to avoid crowding, only using one machine per technologist, and providing more time to clean equipment adequately in between patients. Encouraging all patients to wear face masks while staff continue to wear PPE will likely be important to maintain a lower risk of infection, as has been advocated in many Asian countries. 30 Patients should be asked to bring their own mask to preserve PPE. But if they arrive without a mask, one should be provided for them.
Conditions to Permit Safe Return to Work in Breast Imaging.
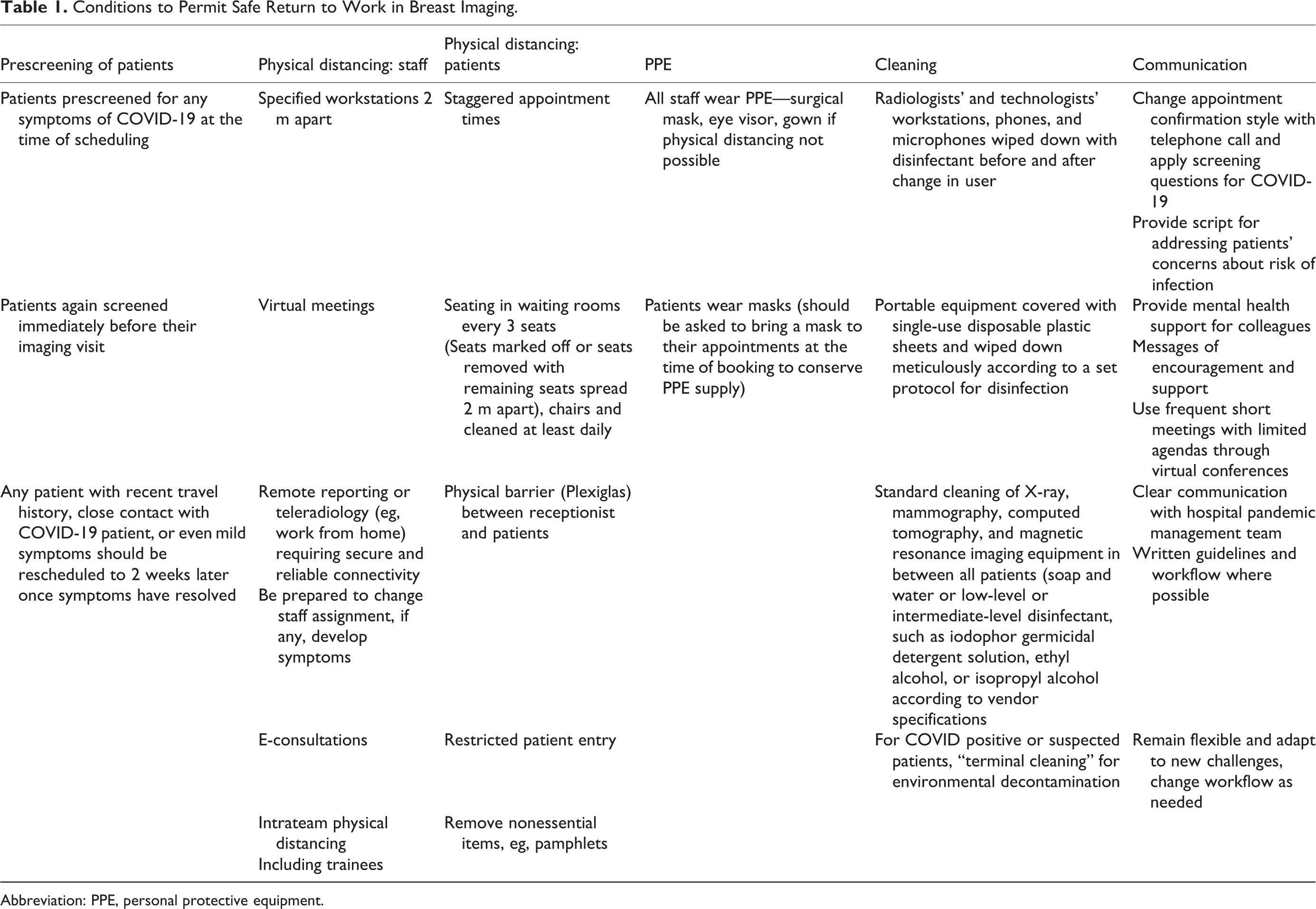
Abbreviation: PPE, personal protective equipment.
Patients should be prescreened for any symptoms of COVID-19 at the time of scheduling and again immediately before their imaging visit. Any patient with even mild symptoms should be rescheduled to 2 weeks later, once symptoms have resolved. Touchless forehead thermometers might be considered before admitting patients to the department. Imaging should proceed only after patients have cleared this screening process. Waiting rooms should be arranged to ensure physical distancing is maintained, removing some chairs, spacing the remaining chairs at least 2 m apart.
Healthy patients may be afraid or reluctant to come in for their imaging appointments in the current model, and breast cancer screening participation may likely be reduced. Therefore, it would be important to analyze and consider different types of breast cancer screening approach with mobile mammography units or more screening at smaller clinics. This may facilitate the implementation of telemammography at centralized reading centers to meet high quality standards. 31 After SARS, patients who recovered were observed to have post-traumatic stress disorder. 32 This will likely require promotion of breast awareness and the need to reinforce the importance of screening for breast cancer while reassuring our patients that adequate steps are being taken to reduce the risk of SARS-CoV-2 transmission during their imaging visit.
Financial Impact on Breast Imaging
The financial impact on clinics and hospitals performing breast imaging is not to be underestimated. 33 Because imaging is paid in a great number of models on a fee-for-service basis, this will likely mean that the already high overhead costs of smaller centers and clinics may not be adequately covered by remuneration of patient services when costs of PPE and cleaning supplies with reduced patient volume loads are considered. This may jeopardize the ability of centers to provide breast imaging and result in reduced screening for breast cancer with subsequent higher rates of late-stage breast cancers diagnosed. Every effort should be made to support these smaller centers and clinics to continue to provide high quality breast imaging, even with the exploration of novel screening models cited above. Given that breast cancer results in 25% of all cancers diagnosed in women, this could account for a significant health care burden impact if not addressed.
Canadian Society of Breast Imaging/Canadian Association of Radiologists Recommendations:
Universal precautions should be taken to protect HCWs from infection or disease spread during breast imaging procedures, particularly mammography, breast ultrasound, breast MRI, and breast intervention procedures, such as biopsy, during the pandemic outbreak of COVID-19 in Canada. The close proximity of both the patients’ and HCW’ faces during these imaging procedures raises concern for droplet contamination in addition to blood spatter contamination, which may occur during image-guided interventions (eg, breast biopsy) and spread by saliva through talking during imaging. These precautions extend to all patients, not just those with clinical symptoms or proven COVID-19, as undocumented infections facilitate the rapid dissemination of novel coronavirus. 34 The following protective measures are recommended:
Personal protective equipment
a. Staff should be encouraged to follow Health Canada and WHO guidelines for appropriate use of PPE. 35 Given the novelty of the disease, the increasing incidence, and new information on potential transmission from asymptomatic patients, 34 we adapted those guidelines in the context of breast imaging (Figure 1).
b. It is important to optimize the use of PPE. While it is recognized that there may be a PPE shortage, staff safety must not be compromised.
c. If PPE is not available or potential shortage for higher risk procedures is anticipated, recommend not performing the procedure until available.
d. All patients (regardless of symptoms) should wear level 1 (low fluid resistance) surgical masks (not N95), preferably donned upon arrival to the waiting room or center. This allows protection for others from respiratory droplets and saliva, which are known to be the chief mechanisms of infectivity for COVID-19. 35 -37
e. All staff working closely and having physical contact with breast imaging patients should wear at minimum level 1 surgical masks, gowns, and disposable gloves and should strongly consider visor or goggle protection. 35 -39 The use of sterile gloves is mandatory for physicians (radiologists) performing interventional procedures with any kind of patients. Masks may be worn for several hours and are useful unless touched or wet.
f. Where isolation gowns are not readily available, consider using patient gowns over clothing or scrubs.
g. N95 masks (high fluid resistance) are only required for aerosolizing procedures in confirmed or suspected COVID-19 patients. Besides procedures in patients with continuous positive airway pressure, bilevel positive airway pressure, high-flow nasal oxygenotherapy, and patients with a tracheostomy, there is no evaluation of any diagnostic test or intervention procedure in breast imaging to demonstrate that they are at risk for aerosol generation. Refer to Canadian Association of Radiologists (CAR)/Canadian Society of Interventional Radiology and CAR/Canadian Society of Thoracic Radiology guidelines for further details. 40,41
h. Given the potential for limited availability of PPE and recognizing that selective use of high priority breast imaging will be performed, the safety of staff is paramount. A minimum of 2 surgical masks is required for each technologist, sonographer, and radiologist per day. The use of a face shield for radiologists and technologists that can be cleansed and reused is strongly encouraged and considered essential for all breast interventional procedures. All attempts should be made to minimize the number of staff present for procedures to preserve PPE.
Close adherence to physical distancing with regular handwashing and cleaning surfaces is required in between each patient contact.
Home/offsite review by radiologist
a. Although not ideal, home review by radiologists should be considered where there is a shortage of manpower in breast imaging; however, 5-megapixel screens should be used for primary interpretation. Anyone interpreting mammography from home should be accredited by the CAR Mammography Accreditation Program (MAP) and already in good standing with their home workstations. 31 If not MAP accredited, radiologists should follow specifications as outlined by https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Dig-Mamo.pdf and provincial diagnostic accreditation programs. 42 This means that a physicist must calibrate monitors once per year.
b. During manpower shortages, consider redeploying some office 5-megapixel screens to radiologists in quarantine or isolation. Diagnostic patients should not be released until the radiologist has fully reviewed the case and has completed the evaluation in discussion with the mammography technologists and ultrasound technologists/sonographers. Video clips should be used liberally when performing remote breast ultrasound.
Low-priority breast imaging should be postponed until distancing recommendations have been lifted or COVID precautions have been adopted as per Local Health Authorities. In particular, suggest postponing requests for 4 weeks for evaluation of:
a. Breast screening, as already outlined in the CAR/Canadian Society of Breast Imaging guideline. 43
b. Annual surveillance in breast cancer survivor.
c. Any breast pain as the only symptom, especially cyclical and bilateral.
d. Low suspicion screening recalls (eg, small groups of calcifications, small circumscribed lesions, single-view asymmetries) after review of the breast imaging by a radiologist.
e. Biopsies of low-suspicion Breast Imaging, Reporting & Data System (BI-RADS) 4A lesions (recommend these be reviewed by one or more radiologists to determine if biopsy can, indeed, be delayed).
f. Low-suspicion diagnostic evaluation of elderly patients to avoid infection in the most vulnerable population.
g. Short interval follow-up (BI-RADS 3).
h. Young patients (eg, <25 years old) with low suspicion lesions, likely fibroadenomata.
i. Males with tender retroareolar breast masses, likely gynecomastia.
j. Women at any age to evaluate integrity of breast implants.
k. Proven cysts for drainage.
This may require training of booking staff to reject these types of requests and scripted discussion with referrers. Radiologists will be required to assist in triage at times. Occasionally, this will provide an opportunity for the radiologist to communicate directly with the referrers to discuss the requirement for delaying these examinations.
High-priority breast imaging
a. This should not be considered emergency imaging. Imaging should be delayed if a patient is affected by COVID-19, has symptoms of COVID-19, has returned from recent travel and is within the 14-day isolation period, or has a family member or close contact affected by COVID-19 illness. If any of these situations applies, the breast imaging appointment should be delayed by 14 days or as directed by local public health authorities.
b. The exceptions that may require more urgent imaging include:
Breast abscess, hematoma or infected seroma for drainage.
Clinical suspicion of inflammatory or locally advanced breast cancer.
Suspicion of breast cancer in a pregnant woman to determine management.
Any case discussed at multidisciplinary conference that is determined to be critical for management decisions. 44
c. High-priority breast imaging applies to any of the following symptoms:
New palpable lump or breast thickening that is clinically concerning.
New bloody or watery (not milky, yellow, or green) nipple discharge.
New axillary mass or lump or new-onset lymphedema.
New skin dimpling or tethering or “peau d’orange.”
New nipple inversion.
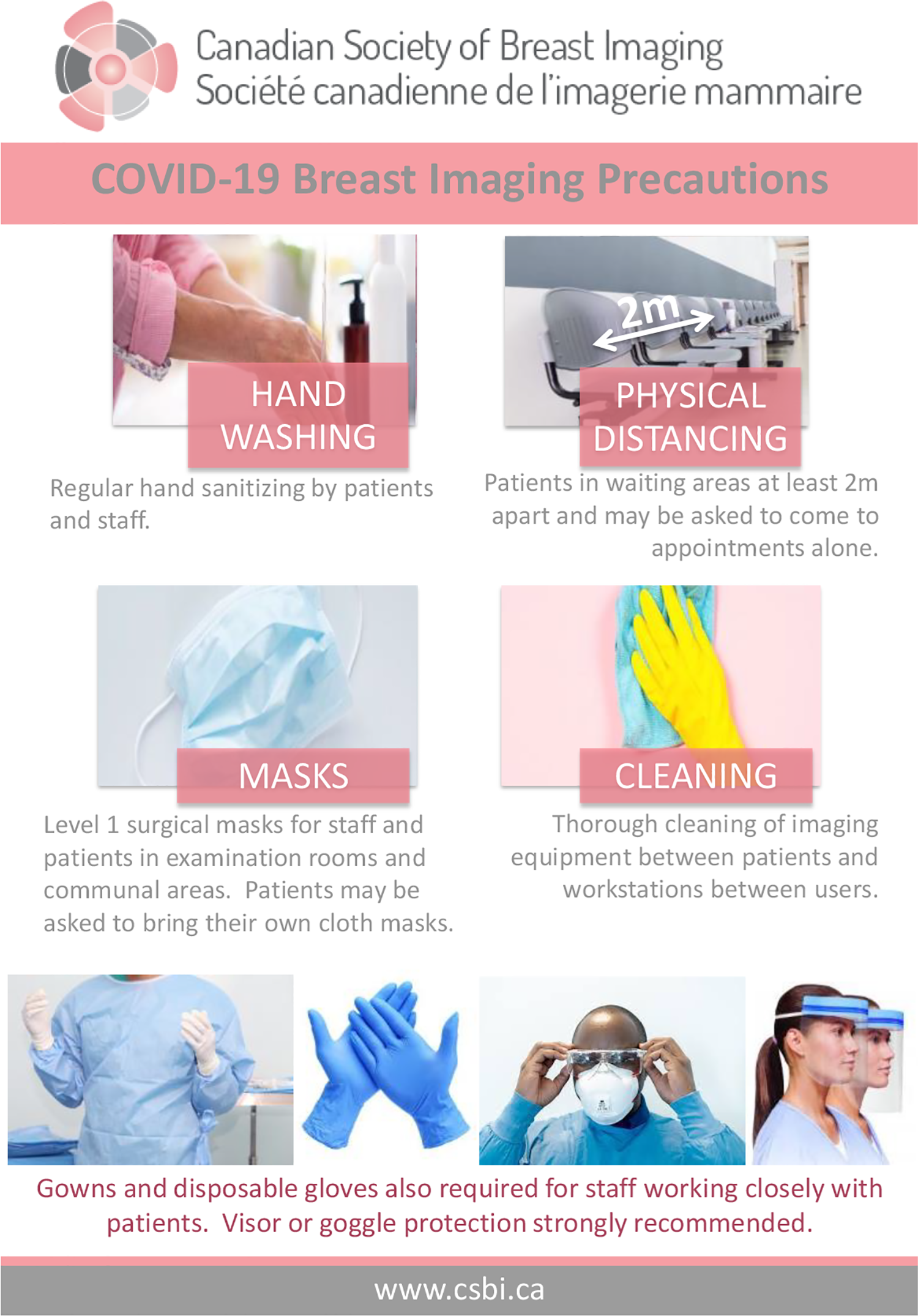
CSBI - COVID-19 breast imaging precautions.
During the pandemic, patients may present with a new palpable lump after being seen by virtual online visit with their referring provider, and the diagnostic visit may be their first clinical examination by the radiologist. A full diagnostic breast imaging workup, including axillary nodes assessment, should be performed as it may expedite the diagnosis and treatment of their breast cancer rather than wait for a physician examination with their health care provider.
During the acute phase of the pandemic, because of delays in breast surgery and increased use of neoadjuvant chemotherapy, additional radiopaque tissue markers may be required for biopsied breast cancers and metastatic axillary nodes. 44 Although these metallic markers lead to additional financial costs, alternative cheaper solutions are available. 45
In re-establishing breast imaging, it may be helpful to consider the order of priority according to the risk of breast cancer, while recognizing that delays in imaging increase the risk and that the lowest risk represent the majority of the population at risk for breast cancer (Tables 2 and 3).
Risk of Breast Cancer.a
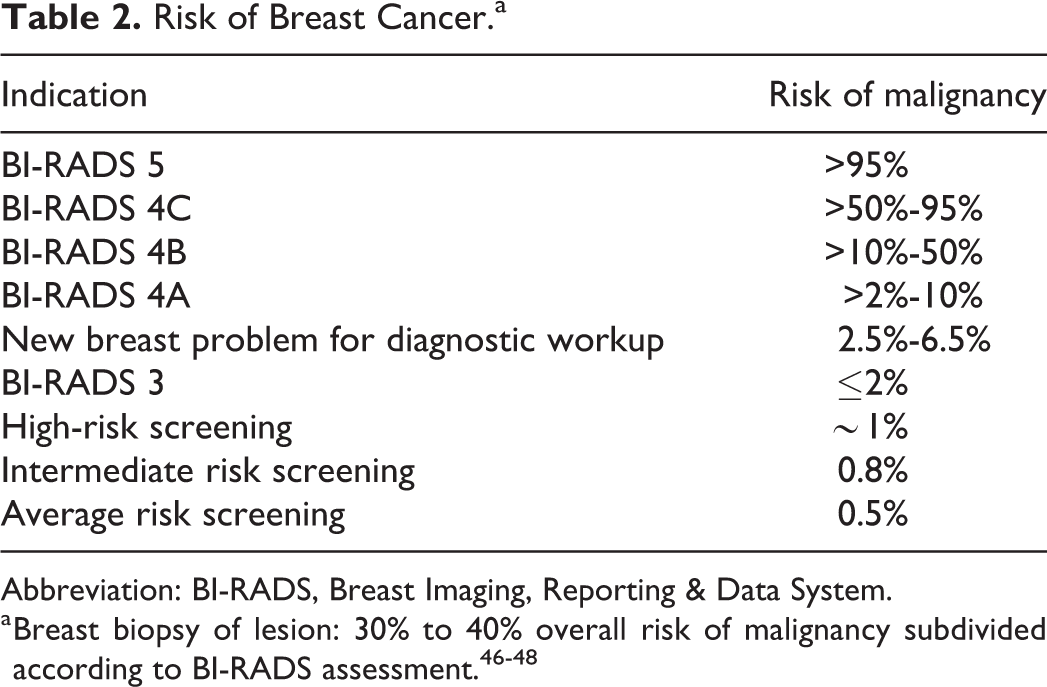
Abbreviation: BI-RADS, Breast Imaging, Reporting & Data System.
Canadian Society of Breast Imaging (CSBI)/Canadian Association of Radiologists Breast Imaging Wait Time Benchmarks.a
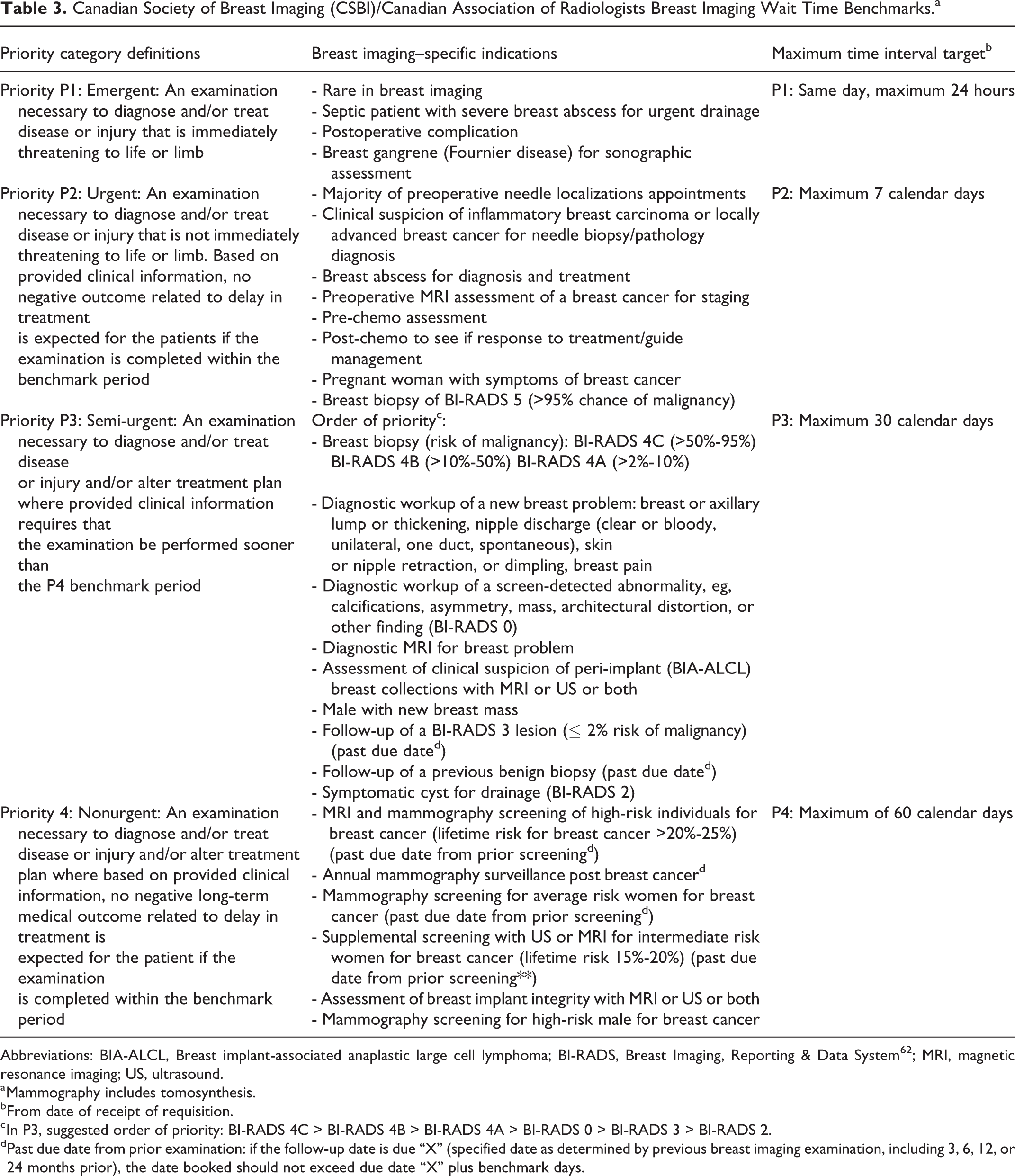
Abbreviations: BIA-ALCL, Breast implant-associated anaplastic large cell lymphoma; BI-RADS, Breast Imaging, Reporting & Data System62; MRI, magnetic resonance imaging; US, ultrasound.
a Mammography includes tomosynthesis.
b From date of receipt of requisition.
c In P3, suggested order of priority: BI-RADS 4C > BI-RADS 4B > BI-RADS 4A > BI-RADS 0 > BI-RADS 3 > BI-RADS 2.
d Past due date from prior examination: if the follow-up date is due “X” (specified date as determined by previous breast imaging examination, including 3, 6, 12, or 24 months prior), the date booked should not exceed due date “X” plus benchmark days.
Collateral Damage on Breast Cancer Diagnosis and Treatment
Due to the COVID-19 outbreak, in 6 weeks, a large number of lower priority requisitions have been postponed. Existing delays in imaging due to staffing and equipment shortages already in many places in Canada will be compounded by added delays due to COVID. 49 Consequently, most of these postponed examinations are now in more acute range. Imaging departments will need to review the prioritization with 2 objectives: minimizing the risk of patient and staff contamination and avoiding additional morbidity due to delaying management of potentially dangerous conditions. The use of hospital resources such as PPE and staffing should be weighted in the final decision. Decisions remain the responsibility of local health care delivery systems, including provincial and local health officials, and those clinicians who have direct responsibility for their patients. However, in analyzing the risk and benefit of any medical treatment or service, the clinical situation must be assessed in association with the clinical team to ensure conservation of resources and best patient outcome. 50 In the transition to the “new normal” after the acute phase of the COVID-19 pandemic, institutions will face dual challenges of maintaining operations during stay-at-home safety orders and planning for a future that will not resemble our past “normal.” The economic impact of the pandemic also threatens current and future support for imaging scientists and research activities in cancer imaging and image-guided therapy. 51
The costs of delaying cancer diagnosis are well established with breast cancer. There is a positive correlation between time to diagnosis and tumor size, 52 -54 risk of metastases to lymph nodes, 52,55,56 stage of disease, 57,58 and death. 58,59 A high-quality systematic review of 87 observational studies published between 1907 and 1996 and involving 101 954 patients with breast cancer examined the relationship between the time from onset of symptoms to the start of treatment (all modalities) and clinical outcomes. 57 In 3 separate comparisons, 5-year survival rates were significantly lower (statistically and clinically) for patients with longer delays. Patients with delays of >3 months had 12% lower 5-year survival rates than those with delays <3 months (OR: 1.47, 95% CI: 1.42-1.53); patients with delays of 3 to 6 months had 7% lower 5-year survival than those with delays <3 months (OR: 1.24, 95% CI: 1.17-1.30); and patients with delays <6 months had 12% lower 5-year survival rates than those with delays >6 months (OR: 1.45, 95% CI: 1.40-1.50). 57 Not only having impact on patient survival, the costs of treating more advanced breast cancers are significant, numerous studies showing that costs may be 2 to 5 times higher. 60,61 Delays exceeding 3 months between symptom onset and the start of treatment could be considered excessive. The collateral damage of COVID-19 on cancer treatment is significant; a recent analysis of delays in treatment of cancer by 6 months showed that a delay in 6 months was associated with up to 1% to 20% decrease in survival from breast cancer, worst for triple negative cancers and in women under age 60. 62
Summary
Breast cancer screening using regular imaging methods saves lives by the risk of dying from breast cancer. Until a cure for COVID-19 is established, breast imaging must be performed using safe practices that maximize protection of patients and staff and minimize the spread of coronavirus infection. Balancing the needs of avoiding delays in diagnosis of breast cancer while avoiding infection requires careful attention to PPE and physical distancing and vigilance to maintain these practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.