
Abstract
Background and Purpose
Nurse practitioners (NPs) make treatment decisions impacting older people with neurocognitive disorders (NCDs), like mild cognitive impairment and dementia. Research has shown that when this patient population has cancer, they face barriers accessing care, have higher mortality rates and limited involvement in decision-making. Despite their critical role, few NPs have been included in studies exploring treatment decision-making affecting this population. To improve experiences for older people and their families, this study explored NPs’ decision-making experiences when individuals were living with an NCD and cancer.
Methods
This qualitative study was informed by interpretive description, a practice-oriented approach. Data collection methods included semi-structured interviews and reflective journaling. Data analysis was iterative with identification and revision of themes that have accompanying illustrations. The research team drew on relevant nursing and practice knowledge to identify meaningful implications for NP practice.
Results
Five themes were identified which included the observation that participants’ decision-making was shaped by NPs’ knowledge and assumptions. NP participants experienced uncertainty and ethical challenges while needing to creatively navigate health systems. Drawing on nursing knowledge, NPs sought to actively involve older people and their family in decision making.
Conclusion
NPs experience complex treatment decision-making when older people are living with an NCD and cancer, requiring navigation of multiple factors and challenges. The results showed shared decision-making processes are applied, suggesting that NPs take up relational treatment decision-making practices. However, there is a need for institutional change, further education, and research about NPs experiences in community settings.
Background & Purpose
The growing prevalence of both cancer and neurocognitive disorders (NCDs), such as mild cognitive impairment (MCI) and dementia (Alzheimer's Association, 2022; Canadian Cancer Society, 2023), presents significant challenges for advanced practice nurses, like nurse practitioners (NPs) caring for this population of older people. The increasing incidence of cancer is associated with advancing age, with approximately 60% of new cancer diagnoses and 70% of cancer-related deaths occurring in people over 65 years (Canadian Cancer Society, 2023). Similarly, NCDs, such as MCI or dementia, affect nearly 10% of individuals over 65 years and more than 30% of those over 85 years 85 years (Alzheimer's Association, 2024). It is estimated in the United Kingdom that 1 in 13 people are living with comorbid conditions of cancer and dementia (Collinson et al., 2022), however, there is no clear understanding of how many people are living with cancer and MCI (McWilliams, Farrell, Grande et al., 2018; Tonelli et al., 2017).
As a minor NCD, MCI is often diagnosed when a person has cognitive decline that exceeds expected age-related changes but does not significantly impair their activities of daily living (Davis et al., 2017). Major NCDs, including Alzheimer's disease, vascular and other forms of dementia, are characterized by one or more of the following symptoms: memory loss, attention difficulties, problem solving, and behaviour changes (Alzheimer's Association, 2022). Symptoms may initially fluctuate, but over time they become persistent as the patient transitions to more advanced stages of dementia. This is also known as the MCI-dementia continuum (Alzheimer's Association, 2022; Darby & Dickerson, 2017).
Cancer is a broad classification encompassing more than 100 disorders characterized by the abnormal growth and spread of cells, “ranging from those that are rapidly changing and lethal to indolent lesions with delayed potential to progress to death” (Tran et al., 2020, p. 1052). The four most common cancers, include, lung, colorectal, prostate, and breast, which account for 50% of all cancer diagnoses in Canada (Public Health Agency of Canada, 2018). The Canadian Cancer Society (2023) special report acknowledged people over 65 years living with cognition disorders are more likely to receive a later diagnosis of cancer, receive fewer treatments, and have worse health outcomes when compared to older people with no cognitive impairment. When changes in cognition and cancer intersect for older people, healthcare professionals (HCPs), face unique challenges in treatment decision-making (Ashley et al., 2023).
Studies focused on how NPs make treatment decisions show they rely on intuitive and analytic approaches Chen et al., 2016; Levy-Malmberg et al., 2024. Intuitive decision-making reflects unconscious processes shaped by NPs’ tacit knowledge and past experiences (Gasaway, 2024). NPs draw on their knowledge and intuition through pattern recognition and familiarity with similar cases to make rapid decisions in dynamic clinical situations (Levy-Malmberg et al., 2024). Analytic decision-making is rooted in empirical and deductive reasoning, offering a deliberate and systematic way for identifying the problem, exploring options, evaluating possible outcomes, and selecting the most desirable solutions based on probabilities (Weirich et al., 2020). This structured approach helps NPs to weigh evidence in relation to patient risks and benefits, while logically assessing alternatives before reaching a conclusion (Thomas et al., 2021). NPs undertake these complex processes in their practice, creating a need to enhance our understanding of their experiences of treatment decision-making. The ultimate purpose of the study is to improve patient experiences when living with these comorbid conditions.
Extant Literature
We conducted a systematic review of qualitative research about HCPs' experiences and perceptions with treatment decision-making affecting older people with memory loss and comorbidities (Shapkin et al., 2025). Most participants in the review were licensed HCPs inclusive of medical doctors and nurses (n = 360 participants), with only one study identifying that NPs worked in primary care (Green et al., 2019). Four of 14 studies reviewed focused on older people with an NCD and cancer (Ashley et al., 2021; Courtier et al., 2016; Griffiths et al., 2020; McWilliams et al., 2018), with the remainder reporting on older people living with diverse comorbid conditions (Baker et al., 2019; Blair et al., 2020; Gilmore-Bykovskyi & Bowers, 2013; Green et al., 2019; Helton et al., 2006; Jefferis et al., 2014; Kaasalainen et al., 2007; Levine et al., 2020; Lichtner et al., 2016; Scott et al., 2018). The synthesis of evidence showed HCPs’ treatment decision-making was shaped by their experiences of uncertainty and assumptions they held toward older individuals living with memory loss. When making treatment decisions affecting older people with memory loss and other comorbid conditions, HCPs experienced communication challenges and identified contextual factors unique to the older person, their family, and the healthcare organization as contributing factors. Additionally, HCPs identified processes, such as learning more about the older person, risk management and sharing responsibility with others to protect and support older individuals with memory loss when treatment decision-making was needed (Shapkin et al., 2025).
A key finding from our systematic review identified that NPs have not been studied similarly in the context of decision-making as other HCPs, and consequently there was limited evidence about how they conduct treatment decision-making affecting this population. NPs play a key role in the optimization of treatments, as they provide diagnoses, offer treatment recommendations, and regularly tailor treatments to suit older people (De Leede-Brunsveld et al., 2023; Green et al., 2019). Physicians and NPs often consider and apply treatment decision-making processes that involve the collection and evaluation of information resulting in a decision to prevent, cure, ameliorate, support, or slow progression of cancer and associated health concerns (De Leede-Brunsveld et al., 2023). Treatment decision-making is a part of shared decision-making processes that embrace these purposes and involve the older person and their family as active participants. Person- and family-centred decision-making is essential in treatment planning for older people living with an NCD (Plantinga et al., 2024).
Research Questions
Given the expected increase in the number of people to be affected by these concurrent health conditions and recognizing that NPs are significantly understudied, we sought to explore this phenomenon. The following questions guided this study:
What are the experiences and perceptions of NPs when making treatment decisions affecting older people living with an NCD and cancer? What strategies do NPs describe and use when engaged in treatment decisions affecting older people with an NCD and cancer?
Methods and Procedures
Study Design
Our study was informed by an interpretive descriptive approach that is philosophically grounded in constructivist and naturalist paradigms (Thorne, 2014). A distinguishing feature of interpretive description is the generation of knowledge that yields practical, clinically focused recommendations (Thorne, 2014). When analyzing and interpreting the information gathered, we considered the data within the participant context, while acknowledging the mutual construction of meaning (Guba & Lincoln, 2005). This was in keeping with the interpretive descriptive approach, which recognizes researchers’ disciplinary knowledge fundamentally influences the methods, analysis, and interpretation of data (Thorne, 2016). The findings from this study also align with Tong et al. (2007) “Consolidated Criteria for Reporting Qualitative Research.”
Sampling and Recruitment
At the time of data collection, in 2022 there were 7,399 NPs registered in Canada (Canadian Institute of Health Information, 2024); however, the number practising in oncology or working with older people living with cancer was unknown. For this study, we sought eligible NP participants who were English-speaking and had experience caring for older people living with an NCD and cancer. There was no minimum standard defining the years of work experience or the type of experience NPs needed to meet these criteria. NPs living in Canada of any age or gender who were employed full-time, part-time, or were working on an as-needed basis were considered eligible for the study. Using this inclusion criteria, we purposively recruited through the Canadian Association of Oncology Nurses (CANO), as we believed that there would be a pool of NPs interested in participating in this study. Recruitment flyers and emails were distributed by the CANO organization across Canada to all members who identified that they were nurse practitioners. In addition, some members distributed flyers to colleagues who they felt maybe interested in participating in the study. Recruitment for the study was open for six months and interested NPs were able to contact the first author during this time. Acknowledging NPs would have diverse experiences and that the pool of possible participants was small, the number of needed participants in our sample was not set a priori. Rather participants were recruited until we were able to gather meaningful clinical descriptions of the phenomenon (Thorne, 2016).
Data Collection
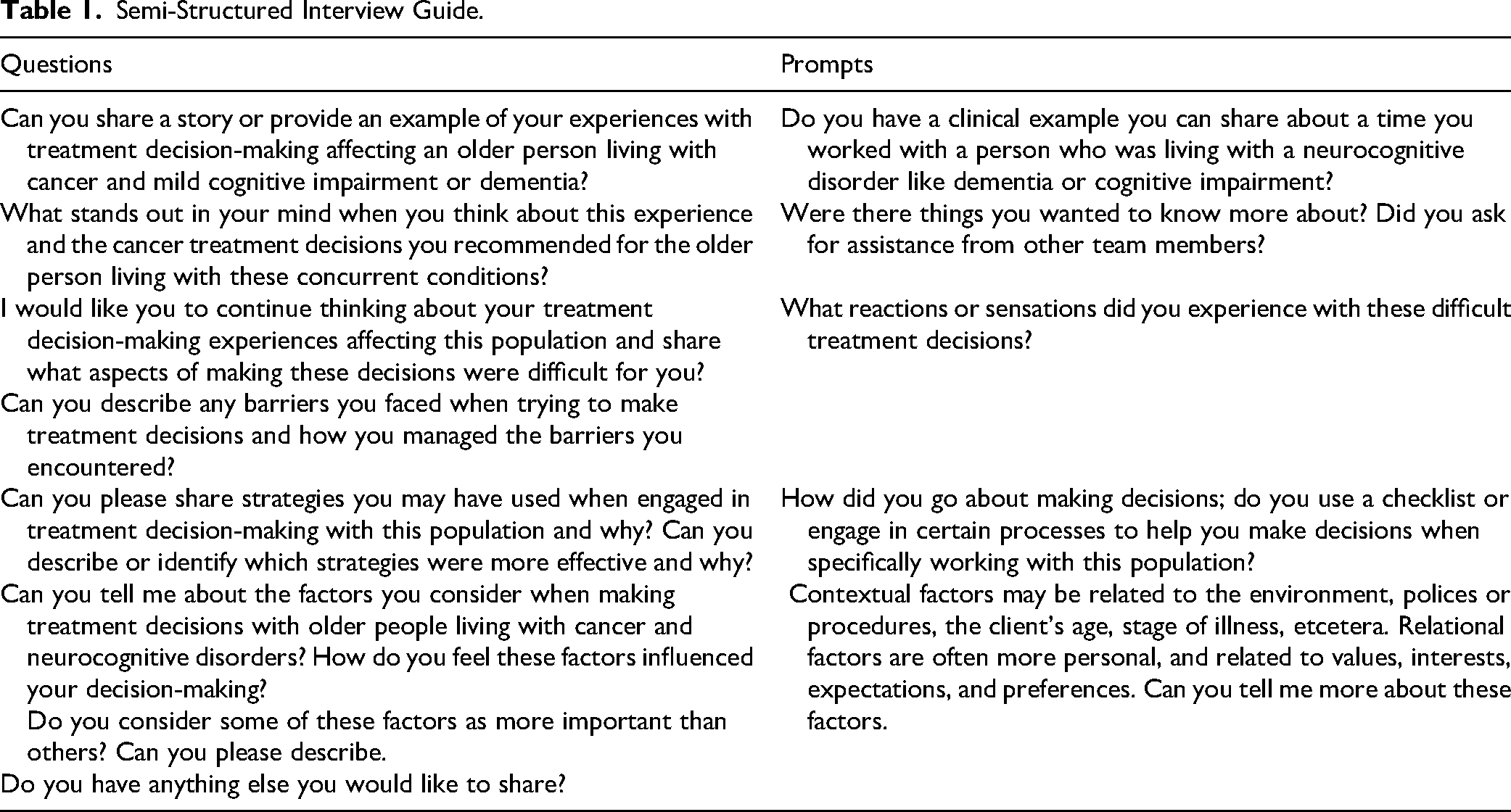
In this qualitative study, we employed semi-structured interviews and thematic analysis. Prior to the interview, the participants completed an electronic consent and demographic questionnaire. The interviewer and first author (KS) confirmed with the participants that they understood the consent and provided an opportunity for questions before the interview began. A semi-structured interview guide was created by the first author, critiqued and revised based on feedback from members of the research team and a practicing NP familiar with the study. See Table 1 for the guide. Following completion of the consent, individual interviews were conducted via a secure institutional Zoom (a virtual conferencing platform) by KS during the months of November and December 2022. The electronic methods for consent and data collection were approved through the Human Research Ethics Board to accommodate coronavirus disease (COVID) pandemic restrictions that were in place. The participant interviews lasted approximately 1 h, ranging from 42 to 67 min. All participants were aware that the study was part of the interviewer's doctoral research and that she was an NP with disciplinary knowledge of gerontology and cancer care.
Semi-Structured Interview Guide.
Recognizing that not only the first author, but the research team came to this study with expert knowledge in the areas of gerontology (JNL) and oncology (LN), we consciously tried to put aside our professional practice expertise and conduct the interviews and analysis from a place of curiosity (Thorne, 2025). This approach enabled us to have confidence that we would learn from the participants through the experiences that they shared about treatment decision-making affecting older people living with an NCD and cancer.
Following each interview, the interviewer (KS) documented the participant's verbal cues, and reflected on the data, recording initial impressions, and early conceptualizations through journalling. Each interview was transcribed, and the transcripts were checked for accuracy against the recordings. Data collection in this study resulted from multiple data sources including, demographic data, interviews and recording of participant cues, which provided rich information for analysis. This study was carried out in accordance with human research ethics and received approval from the University of Victoria Human Research Ethics Board (No. 22-0239).
Data Analysis
We used Braun and Clarke's (2021) six-step thematic analysis to provide a rigorous systematic and flexible approach for analyzing data gained from exploring participants’ perspectives. After verifying the transcripts accuracy, they were uploaded into the NVivo 12 (QSR International, 2020) software to assist with management of the data. For the first step of data familiarization, the first author repeatedly read, took notes, and conducted reflective memo writing. During the second step, the first author triangulated the multiple data sources to appreciate the varying perspectives that were present. Through this process the meaningful data segments were identified and resulted in the generation of preliminary codes. Then two members of the research team (KS, LN) searched the preliminary codes for themes and grouped the data based on the similarity of meaning and concepts. The fourth and fifth steps occurred iteratively through discussions with members of the research team (KS, KM, LN, JHL), which provided deeper insights and challenged the initial thinking and understanding, supporting the process of defining and naming themes (Braun and Clarke, 2021). The members of the research team continually posed the following questions to stimulate a deeper understanding of the data. What are the data telling us, what is it we want to know from the data and what relationships is the data trying to push us to see (Thorne, 2025)? As Thorne (2025) suggests engaging with the data in this way, facilitates ongoing reflexivity. Despite our efforts to keep these questions at the forefront, we recognized that our rich practice knowledge of gerontology and oncology partially shaped our interpretation of the phenomenon. Through these ongoing and iterative processes of deeply exploring the data, five themes resulted. The final step of writing the report included the first author (KS) regularly meeting with members of the research team (KM, LN, JHL) to ensure methodological coherence, enhanced interpretation, and to generate clinically applicable conclusions.
Rigor
Rigor was established through our demonstration of credibility, trustworthiness and interpretive authority. Credibility and epistemological integrity were achieved through prolonged engagement with the phenomenon in our qualitative systematic review, and engagement with the study participants (Thorne, 2016, 2025). Trustworthiness was conveyed through the collection of meaningful clinical descriptions, triangulation of the data sources, and expert review. A description of our analytic logic in articulating the themes and supporting data for this study further demonstrated interpretive authority (Cuthbert et al., 2017; Thorne, 2016, 2025).
Results
We interviewed six NPs from Western Canada who had more than 10 years of nursing experience (combined RN and NP experience) and assigned them participant codes (P1 through to P6) in the study results to protect their anonymity. Four of the NP participants viewed oncology as their area of expertise, three worked in tertiary care outpatient clinics, and one worked in a community clinic. The remaining two NP participants worked with older people living with a variety of comorbid conditions. One of these two NPs had expert gerontology knowledge and worked in a tertiary care outpatient clinic. The other in a rural community outpatient clinic, caring, in part, for older people living with an NCD and cancer. Table 2 includes demographic data.
Participant Demographic Descriptions.
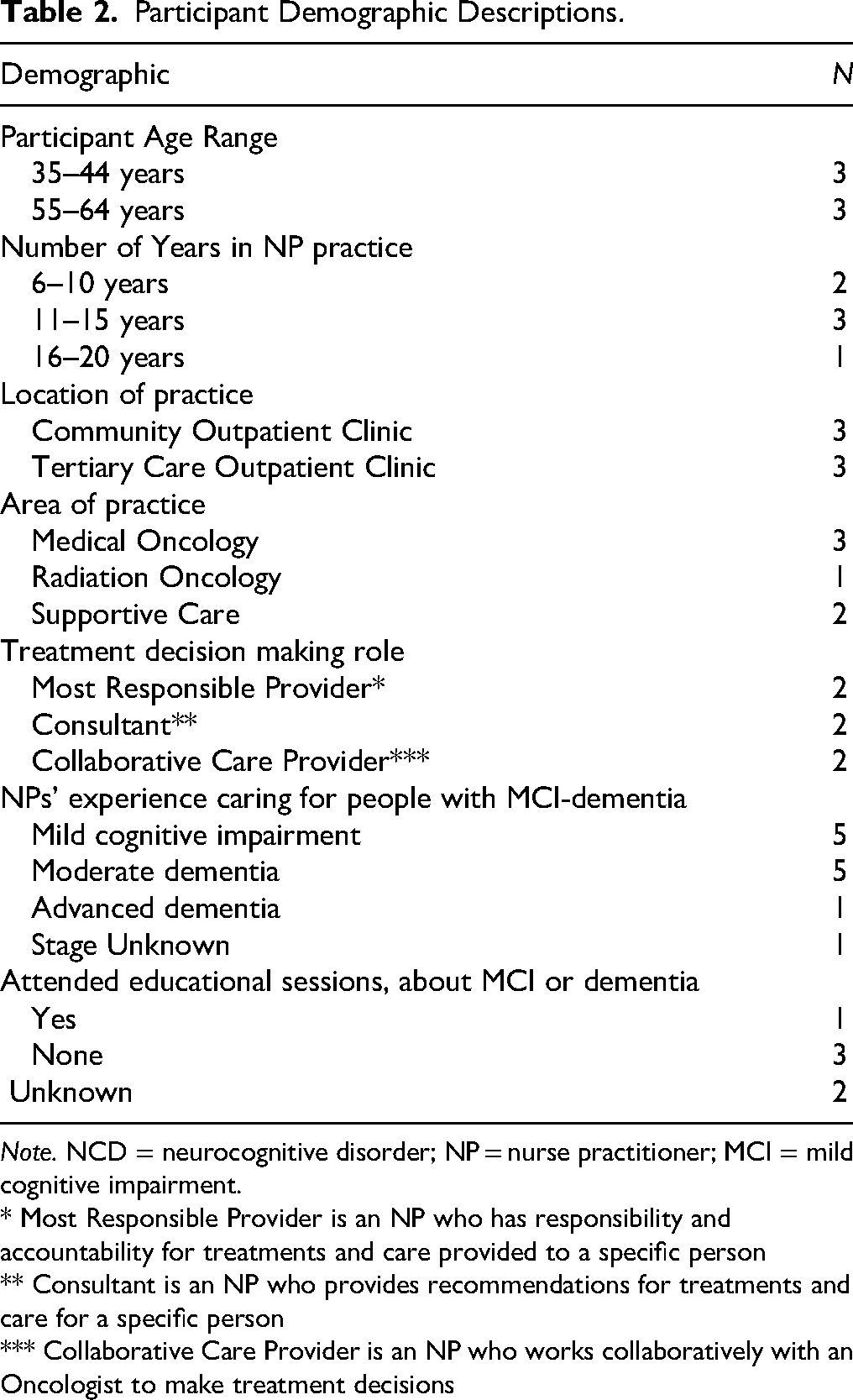
Note. NCD = neurocognitive disorder; NP = nurse practitioner; MCI = mild cognitive impairment.
* Most Responsible Provider is an NP who has responsibility and accountability for treatments and care provided to a specific person
** Consultant is an NP who provides recommendations for treatments and care for a specific person
*** Collaborative Care Provider is an NP who works collaboratively with an Oncologist to make treatment decisions
Five themes resulted from the analysis that reflected the experiences of NPs navigating treatment decision-making when older people were living with an NCD and cancer. Throughout the iterative processes, it became apparent that NP participants were committed to providing high-quality care tailored to their patients’ needs and wishes.
NPs Experience Uncertainty with Treatment Decision Making
NPs experienced uncertainty with treatment decision-making when older people's underlying NCD changed, or their cancer progressed. This often occurred when NPs were caring for an older person with cancer, particularly when they were questioning the patient's cognitive abilities. In these instances, NPs expressed a lack of confidence with the patient's ability to understand treatment plans and changes with prognosis, particularly when NPs did not know if these changes were transient or occurring from the progression of the person's dementia, as illustrated in the following excerpt: His wife, a frail woman with Parkinson's, could not look after him, and he refused to do anything until we finally said he had to go to the Palliative Care Unit, because there was nothing else [we could do for his cancer]. Was he demented? I don’t know, but he had cognitive issues. . . When I started to ask about palliative care, he was very angry. (P5)
NPs drew on their past experiences of working with older patients living with cancer to support their treatment decision making. Deviations from normal treatment routines also led to the feelings of uncertainty, as described in this experience: Typically, with patients who are cognitively intact, they would normally have surgery and then they come into our [NP] clinic for lower grade tumor management. We see them and determine together if they want to proceed with oral antiestrogen therapy. We use a decision tool called PREDICT. . . I input their data, such as, age at diagnosis, tumor, size, tumor grade, lymph nodes status, what type of surgery they had, what type of treatments they’ve had, and it gives a quantifiable number to quote with an impact of 10-year overall survival. It shows if endocrine therapy may be beneficial. But in one case her longevity was limited because of her dementia. She did not have surgery, and I didn’t have any data to input into the [PREDICT] tool [pause, and pace of the speech quickened], so I could not provide her and the guardian with any more information. Now, I was shooting in the dark with this case. (P1)
The NP experienced uncertainty when she shared that she did not have all of the data needed to effectively use the prognostic tool that would provide information about the survival benefits from cancer treatments. When this occurred the NP could not provide the patient and her family with the best recommendations for treating breast cancer, creating uncertainty, which she described as “shooting in the dark” (P1).
Other NP participants shared doubts about not knowing how the person would tolerate treatment, describing that in these cases they used the cancer-specific assessment tools to gain more functional information about the patient to predict future risks of toxicities. One NP shared the following: If we’re worried about them [the person with an NCD and cancer] reporting their symptoms or just their tolerance of the treatments, we use performance tests like the ECOG [Eastern Cooperative Oncology Group] or Karnofsky Performance Scale [KPS]. If their performance status goes below a two . . . if they go too far down the performance status scale, then, basically, we’re putting them at risk of dying, so, in this case it will change their treatment options. (P4)
In these descriptions NPs recognized the person had cognitive changes and relied on objective data from laboratory tests and screening information gained from the KPS or ECOG to assist with decision-making. However, it was evident that this did not eliminate their doubts, nor did it provide complete information about the person's cognitive abilities. NPs did not describe using knowledge gained about the person's functional status as way to also learn about the person's cognition. Overall, NPs experienced uncertainty with treatment decisions in spite of using some assessment and prognostic tools to mitigate concerns.
NPs’ Knowledge and Assumptions About the Progression of MCI and Dementia Influences Decisions
To navigate the complexities associated with treatment decision making, NPs described how they used their knowledge about cancer, NCDs (MCI and dementia), and what they knew about the person and their family. The participants relied on their past experiences, knowledge, and beliefs to assist with determining a plan that met the person's needs and goals. More experienced NPs described that they anticipated challenges and when they did this, they were able to adapt more easily.
One NP participant described how she had assumed the cancer treatments would negatively affect the person's function or quality of life when living with these comorbid conditions. However, she found this assumption was not always true. This NP participant shared that it was “like nothing had really changed and he wasn’t acutely going to die from the cancer, it was always there in the background, but it didn’t really change what I was trying to do” (P6). In this situation, the progression of the patient's dementia had a greater impact than the cancer treatment, enabling the NP to draw on her expertise in gerontology.
Another NP participant shared that she had some knowledge about the MCI-dementia continuum based on her previous work as an RN. This participant shared that because her patient had a possible diagnosis of dementia, she believed communication would be difficult in the consultation. [In prepping for the visit], I made assumptions that there would be potentially some limitations to her understanding, and then, when I met her, it was very obvious. She drifted [demonstrating an inability to stay focused on the topic] throughout our consult. She wanted to talk about her grandchildren. I could tell she was drifting. (P1)
The participant explained how she managed her assumptions that were reinforced or confirmed when she met the patient: Then I had to make decisions about how to speak to her and make it meaningful while still providing her with practical information. I do not normally need to help people stay focused on the conversation and remind them why they are meeting me. (P1)
Another experienced NP participant described how she challenged assumptions about cancer and aging based on her knowledge of how performance status affects the older person's success with cancer treatments. She explained her use of the Karnofsky Performance Status scale (Karnofsky & Burchenal, 1949), which provided physical performance information, sharing that in her experience “age did not matter” (P4), she valued the person's functional ability. All my patients are old. I would say if anything performance status outweighs everything. . . there is nothing that I’m going to do different for a 62-year-old versus an 85-year-old. If they both walked into my clinic, and they both were functioning, they would both be offered the same treatment. (P4)
NPs navigated treatment decision-making by applying knowledge gained from their past experiences as an RN and from their advanced practice knowledge. They described how they tested their beliefs and assumptions, resulting in the need to alter their plans while caring for the older individual.
NPs Experience Ethical Challenges with Treatment Decisions Making
NPs described experiences when they faced challenges and took specific actions to navigate difficult decisions, while ensuring their actions were ethical. Difficulties seemed to arise when participants described an inner conflict with managing their feelings of personal responsibility that resulted when determining what was in the patient's best interest. They described questioning if treatments were futile: [The cancer treatment has] very manageable side effects, but what was it adding to his life right now? He was not going out anymore. He was stuck in his bedroom all day, and it was stressful for his wife to make sure he takes all of his medications. What was the value? Was it just the peace of mind that you think the cancer is well controlled? (P2)
When NPs recognized the patient was progressing toward end of life, they did not differentiate the causes (dementia or cancer); rather, they focused on the patient's quality of life and the most appropriate decisions for the person and family. At times, when NPs brought forward the need to discuss the cessation of treatments, it was met with challenges from family members wanting to exhaust all lines of treatment first. As shown in the following example, NPs described some families as not wanting to give up, sharing that when this occurred family members were typically unwilling to accept that the patient was no longer responding to the cancer treatments: Cognitive impairment or not, I struggle with people/families who want more treatment when there are no more, or when they no longer qualify, or when they’re struggling with the end-of-life or the end-of-treatment diagnosis. Usually, there's no great way to move forward, medically and ethically speaking. Sometimes I have to say [to the patient/family] that I can’t give you treatment. (P3)
Another NP participant described their experience of ethical conflict with a family when the older person was living with end-stage dementia, particularly when the cancer was treatable. The family continued to provide assisted nutrition despite the knowledge that this action might harm the patient: The family was just [saying], “No, no, no, no, no!” It was months of push back and of me trying to explain to the family [that thedementia was progressing faster than the cancer] and that she [the patient] was going to continue to decline. Eventually she [the patient] had to be admitted into the hospital, and then the palliative care team got involved. In the end, the patient aspirated, developed pneumonia, and died. It was hard [pause]; we controlled the cancer but there were other things that were going to cause her to decline. (P2)
The ethical challenges NPs shared were frequently described as occurring when the person was near end of life or experiencing treatment failure. They described how ethical conflicts developed despite having what they believed was a well-planned course for treatment decision making.
Needing to Navigate Healthcare Organizations Influences NPs’ Decisions
All participants described how they needed to navigate complex healthcare organizations to be able to provide care that was in the best interest of the older persons. NPs mitigated healthcare organizational constraints, particularly when they experienced challenges with providing quality care in the way that they preferred, resulting in work arounds.
NP participants recognized that large healthcare organizations could not be controlled; rather, they described needing to be skillful, and at times creative, to navigate these complex health systems. NPs working in tertiary cancer care clinics faced constraints on their time and often had heavy caseloads. As one participant described, NPs were also expected to follow the rules set by administrators who seemed more concerned about efficiency and productivity than with what was in the best interest of the patient: My clinic runs from 8 a.m. until noon, and I see about 12 patients, the appointments are all 15 min. When a new patient gets booked as a virtual appointment for 15 min, I have my secretary send a note, saying you’ve been booked on Friday for 15 min at 10:15 but you have been moved to a Zoom meeting for Friday afternoon at 2 p.m. for 1 h. It gets put into my calendar as an extra appointment, outside of my clinic. (P4)
The NP described the patient's booking schedule had to be navigated to accommodate the organization's barriers, inferring that if it was managed in this way, she did not have to choose between policies or providing the care that was viewed as essential.
NPs described making very specific decisions to ensure the individual received care that was in their best interest. NPs needed to pause and carefully consider how their treatment decisions affected the older patient's access to care: I do a lot of liaising with the community nurses to get a better idea of what's going on at home, which I don’t always get from the patient. Sometimes, they [community nurses] tell me that they’re [older person] living precariously, and their houses are in disarray. Then we need to consider if the older person should move into a long-term care (LTC) facility. I think that's always hard because LTC has long wait lists and when you’re living with lung cancer, generally you have a limited prognosis. They [patients] are stuck in the gray zone; they’re really not a hospice candidate yet. [Pause] Alternatively, if I stop cancer treatments, then a hospice unit would take the patient. It's like trying to manipulate the system so the patient can get the care that they need to be safe. (P2)
NPs shared strategies they employed to make the health system “work” by creating new ways to see their patients. Seeing the individual in their own environment was considered respectful, in addition to being important to NPs, as the knowledge gained significantly influenced and informed their decisions: She's in a wheelchair, so we had to use transport, but during COVID that was more complex, and the patient found it hard, like physically, it caused her pain, it was a 20-minute bumpy ride, and she felt every bump. . . I wish I had more flexibility [to see her], so I thought about ways to potentially go and see her at her [LTC] facility. But the advice that I received [from the unit manager] was that it was probably not in my best interest to do [a facility visit], as it sets a precedent. I went anyways, to see her at the [LTC] facility. I think she performed better there because she wasn’t exhausted [referring to a functional assessment]. There were a few other patients at that [LTC] facility that I could have seen when I was there. Oh, it was such a missed opportunity to go there and [purposefully] see other patients too! It's such a shame [that the hospital organization stops us from doing this]. (P1)
In this description the NP showed how she did not comply with the suggested actions from the manager, who represented the healthcare organization's interests. Instead, the NP described how she pushed back against the organization's systems, demonstrating her ethical actions to do what she believed was in the best interest of the patient.
NPs relied on other HCPs, such as physicians and nurses, to assist with different aspects of patient care to ensure that the patient received care from the most appropriate professional. At times, when this occurred, NPs were met with resistance by other HCPs questioning who was responsible for providing non-cancer-related care. This led to confusion for the older person and their family. One NP shared, We bump a lot back to family doctors if it is not a cancer-specific problem. Then the family doctor says, “No, this is a cancer issue,” and we say, “No, it is not,” and the families ask, “What are you guys doing?” (P3)
NPs navigated the rules of healthcare organizations by creating ethical workarounds to ensure their patients were eligible to receive supportive care; however, the patient and their family were sometimes caught in the middle. NPs found they had to bend the rules, recognizing new cancer patients and those with an NCD needed more time. They also had to be creative on how and where they would see patients, making efforts to meet them in their home (i.e., in an LTC facility) or via an additional Zoom visit to ensure they had enough time and opportunity to assess the patient. NPs shared how they took up ethical actions demonstrating that they were aware their treatment decisions needed to be carefully determined to navigate the complex healthcare systems. When NPs did this, they believed it ensured patients remained eligible for various healthcare supports.
NPs Foster the Older Person's and Their Family's Participation in Decision-Making Processes
NP participants used common strategies to support shared decision-making with patients and their families in determining the best treatment options. When these strategies were taken up, NPs’ treatment decision-making was inclusive as they navigated decisions together with patients and their family members. One NP shared how she considered the individual and tried to accommodate the best times for the older patient to participate in discussions about cancer treatments: Some people are more reliable if you book them for a morning appointment; some people are more reliable after their afternoon nap. It depends on the dementia, so what you see at one clinic visit might be very different than 3 weeks prior, or 3 weeks in the future. (P1)
NPs also described strategies that included both the patient and their family in discussions: l always kept the patient closest to me [during a meeting], and then all of their family will be in the seats, beside them. I usually started with the daughter and asked how things were going, and how they think things are. Then I asked the son how he thinks things are going and what he notices, because they each spend time with Dad in different ways. Then I asked the wife how she thinks things are going, and by the end we’re having this group discussion, and the patient is part of it. Then after I’ve gathered all of the information, and he's heard them talk on his behalf. I say, “Now it's your turn. I want to hear from you.” (P4)
NPs shared other strategies, such as promoting a safe environment for engagement: “I never rush, sometimes things are discussed repeatedly until all questions are answered [until everyone understands]” (P5). Participants described their awareness of the patient's responsive behaviours, and they used this information during treatment discussions to ensure they were not viewed by the patient as “confrontational” (P6). NPs noted giving the person space or using other techniques to facilitate the older person's participation, such as “distraction or reorientation” (P6), to re-engage the person when needed. Overall, NP participants created opportunities to hold inclusive discussions by creating safe spaces for the person living with an NCD and cancer.
NPs shared it was helpful to have family members who knew the patient, which made it easier to call and confirm how the patient was managing with treatments. One NP described how she interacts with a family member in the following way: I talked to her [the patient's daughter] on the phone separately, just to make sure that we got all the information that [the patient] might not be disclosing. Especially, when we see that he's losing weight, or that he's having a little bit more difficulty with word finding. (P2)
To be able to connect with people in this way, NPs described how they needed to spend time with the patients and their families, getting to know them. NPs developed these relationships because they recognized that family members of people with an NCD and cancer were actively involved and viewed themselves as participants in the shared decision-making processes.
Discussion
The aim of this study was to explore NPs’ treatment decision-making experiences when providing care to older patients with cancer and an NCD (secondary to MCI or dementia). We learned from this study that treatment decision-making affecting this population occurs in complex clinical situations and consists of multiple processes and relationships that are interconnected like a web. We found NPs were continuously navigating the complex web to ensure the best interests of the older person were at the forefront. Understanding it in this way provides a visual representation of how treatment decision-making was experienced by the NP participants. It gives us a deeper understanding of the themes resulting from this study and situates what we learned from each theme in a way that was clinically meaningful. To navigate decision-making NPs relied on their knowledge, past experiences, and beliefs to interpret the diverse and changing conditions to gauge how they should proceed, adapt or pivot treatment decisions. The results of this study are supported by findings from other research reporting that treatment decisions are contextual and consist of multiple complex processes (Ashley et al., 2023; Caba et al., 2021).
When the NP participants experienced uncertainty, they navigated decision-making by drawing on their extensive knowledge within their area of expertise and combined it with their past RN experiences of caring for people with an NCD. Although NPs possess extensive knowledge in both areas, we found it difficult to determine how they combined their expert NP knowledge with their RN knowledge of NCDs to inform their treatment decisions. For example, NPs shared that they had a fulsome understanding of how a person's functional status was a predictor of future toxicities secondary to cancer treatments; however, they did not appear to apply knowledge about the person's function as a measure of cognitive abilities. Possessing advanced knowledge of both oncology and an NCD and being able to apply it effectively is important when caring for this population.
Scholars and researchers have identified that there is a strong relationship between a patient's performance status (functional abilities) and their cognition. In their retrospective study of older adults with cancer, Papadopoulos et al. (2022) reported dependence (i.e., need for assistance) in one or more activities of daily living was an independent predictor of cognitive impairment. Building on this understanding, Valvani et al. (2024) found a correlation between a person's function and cognition, suggesting as frailty increases there is a high likelihood of progressive cognitive decline. Frailty refers to a state of increased vulnerabilities resulting from decreasing physiologic reserve across multiple organ systems (Valvani et al., 2024), which is a strong predictor of health outcomes and can be used to assist with determining risk for hospitalization (Haase et al., 2022). Therefore, it is important for NPs to continue to draw on their diverse disciplinary knowledge of cancer and NCDs (memory and cognition changes) in the context of oncology care as it has the potential to enhance patients’ experiences and health outcomes.
NPs’ uncertainty with treatment decision-making observed in this study has similarly been reported in the literature (Ellis-Smith et al., 2021; Scott et al., 2023). Uncertainty is considered to arise in complex clinical situations when there is limited or unpredictable information available to HCPs (Ellis-Smith et al., 2021). In our study, as in others, HCPs describe uncertainty when they are unsure of the diagnosis, the recommended treatment, or when they do not fully understand the patient, their problems, or the disease trajectory (Scott et al., 2023). From a treatment perspective, uncertainty may arise because older people living with cancer are significantly underrepresented in clinical trials, and those who are included tend to be selected based on having few comorbid conditions and high level of physical fitness (Cook et al., 2024). Given this lack of representation in research, there is limited evidence available to inform NPs’ treatment decision making. Until this changes, it is unlikely that decision uncertainty regarding some treatments will resolve quickly, highlighting the need for studies to be conducted with this population.
Recognizing the reality of having limited supportive evidence for treatments, clinical experts and scholars have suggested the use of applicable geriatric focused assessment tools as a method of resolving some uncertainties when working with this population (Du Montier et al., 2020; Goldberg et al., 2018; Nightingale et al., 2021). Partially adhering to these recommendations, NPs in this study used oncological assessment tools, such as the ECOG test (Oken et al., 1982), KPS scale (Karnofsky & Burchenal, 1949; see also Schag et al., 1984), and other prognostic indicators. However, applying these oncology focused tools did not reduce NPs’ experiences of uncertainty. An alternative to using these tools is the use of a comprehensive geriatric assessment (CGA), which offers a multidisciplinary approach to identifying patient vulnerabilities for toxicity and potential complications (Hamaker et al., 2022). While the evidence supporting the effectiveness of a CGA is robust, it has unfortunately been poorly adopted across Canada due limited funding and a shortage of qualified practitioners (Cook et al., 2023). There is clearly a gap in accessing and using geriatric focused assessments that could be integrated by NPs and nurses into their everyday clinic practice. However, healthcare administrators and policymakers also need to do their part by supporting this strategy through policy development and integration of tools into electronic medical records.
The complexity of treatment decision-making affecting older people with cancer and an NCD has, at times, led to strained relationships between NPs and family members. This was mostly experienced when patients transitioned from curative or supportive care to end of life care. End of life applies to a person living with progressive and terminal conditions whose survival is less than months to live Hui et al. (2014). NPs described experiences resulting in ethical conflicts arising from a differing understanding between the NP and family members about the need for certain treatments or the way care should be delivered in the late stages of a person's life. The situations were emotionally charged, and some NPs believed that in some situations the best interests of the patient were not at the forefront of family members’ decision making. In this context, the ethics of care theoretical framework may help interpret the conflicts NPs face as their patients transition to end-of-life care (De Panfilis et al., 2019; Noddings, 2013). This approach emphasizes relationships, context, and compassion, while recognizing vulnerability (De Panfilis et al., 2019). It provides NPs with a moral framework to navigate interconnected relationships while nurturing communication and trust with families (Bianchi & Ghirotto, 2022).
NPs also identify ethical conflicts when they experience the inability to offer high-quality care. NPs describe how they recognize the healthcare system rules but feel they need to navigate the constraints and create workarounds to meet the older person in a way that is respectful and more convenient. Workarounds in healthcare are common, particularly when nurses’ sense of responsibility and experiences are linked to acts of conscience (Bianchi & Ghirotto, 2022), as described in our study.
Workarounds in clinical practice also result when HCPs need to ration their time due to organizational constraints (Bianchi & Ghirotto, 2022). Healthcare organizations create barriers for patients and families by limiting access to NPs and other HCPs through the rigid structures that tightly allocate their time (Ashley et al., 2021). This knowledge is in keeping with the experiences NPs shared in this study, findings from our systematic review of the evidence, and other literature that similarly recognized the challenges of time constraints hinder personalized care and adequate family support (Ashley et al., 2023; Caba et al., 2021). Gaining this understanding not only highlights the need for structural changes within healthcare organizations to allow HCPs more time and flexibility to spend with their patients but also reveals the deeper moral commitment NPs hold as they navigate treatment decision making.
NPs express a strong desire to work together with patients and families to achieve the best possible outcomes that align with the patient's values, despite potential ethical conflicts. NPs explain decision-making approaches are strengthened when they apply strategies to enhance information sharing in a way that is meaningful to all parties involved in the processes. Participants describe these actions as deliberate and consistently present, regardless of the patient's stage of dementia. Similar information-sharing strategies have been reported in other studies of older patients with NCDs and cancer (Mattos et al., 2023). However, our results differ in that NPs not only approach information pragmatically but also make deliberate efforts to engage the older person, even when communication is atypical. To encourage effective shared decision making, scholars have called for HCPs to deliberately engage with the patient and/or family members to fully understand their concerns, values, and preferences (Daly et al., 2018; Mattos et al., 2023). The shared decision-making processes reflected by NPs show how they develop rich relationships, suggesting they use a relational approach to enhance treatment decision-making that is guided by the ethic of trust and care (Dove et al., 2017; Noddings, 2013). This differed from our initial understanding of NP decision-making that was described as an intuitive-analytic approach. We found NPs make consistent efforts to involve patients in decision making, yet the impact of this involvement on patients and their families remains unclear. As such, further investigation is needed.
Our discussion presents treatment decision-making affecting this population of older people as a complex embodied practice at the intersection of multiple factors, challenges and processes. It is apparent that NPs in this study sought to effectively navigate these complex relations in particular practice situations. The metaphor of navigating the complex web of treatment decision-making offers insights into NPs’ decision-making processes. This metaphor highlights the dynamic and relational nature of NP work, illustrating how NPs continually adapt and adjust as circumstances evolve (Doane & Varcoe, 2015). In the face of uncertainty and anticipating challenges, NPs draw on their knowledge, past experiences, and personal beliefs to navigate and interpret the multi-faceted factors that influence treatment decisions. Together, with all people involved (the older person, their family and other HCPs) NPs apply strategies to engage in a course of treatment that strives to meet changing goals and needs.
Strengths and Limitations
This study has several strengths and limitations. To our knowledge, it is one of the first focusing on NPs’ experiences of treatment decision-making affecting older people living with an NCD and cancer. This study recognizes NPs are providing complex care to this population of older people in a meaningful way and use a relational decision-making approach, in addition to intuitive-analytic methods. We also confirmed NPs need dedicated time to be able to provide effective and tailored care in creative ways for this population.
A limitation of the study was the small sample size, and the results may only be applicable to NPs working in a Western Canadian context due to a lack of representation of participants from other provinces. Limited participation may have been due to the timing of the study, which was conducted near the end of the COVID restrictions, when HCPs experienced high burnout (Lavoie-Tremblay et al., 2022).
Our sample consisted of NPs working primarily in tertiary outpatient clinics that were part of larger healthcare organizations, with only one NP located in a rural community outpatient clinic. The limited representation of NP community providers and the knowledge that older people with cancer and NCD are cared for in their communities identifies a need for further investigation in this area.
Recommendations
The analysis of data, and interpretation of the themes, resulted in development of the overarching metaphor of NPs' navigating a complex web of unique practice situations and multiple intersecting relationships and processes. Thinking about NP treatment decision-making in this way can offer an alternative way to inform nursing education and practice. The following statements represent how the cumulation of what was learned from this study influences nursing by way of making these recommendations for practice and education: 1) NPs caring for this population should have advanced practice knowledge of cancer and the MCI-dementia continuum, enabling them to make contextual decisions. 2) NPs should acknowledge that uncertainty will be experienced as the course of treatment decision-making may be unpredictable when patients with NCDs and cancer seek treatment. 3) NPs may have differing values and beliefs from the older person and their family, but the ethic of care framework, when integrated into practice, creates the opportunity for relational decision making. 4) NPs should demonstrate a high level of commitment and persistence with navigating healthcare systems to effectively support patients and their families. 5) NPs should work together with older people, their families, and other members of the healthcare team to foster a safe and engaging environment that facilitates shared-relational decision making.
Policy recommendations include a need for flexible scheduling of appointments and the opportunity for more time with the person and their family. When changes to policy occur, it may enable NPs to provide care that meets the needs of the individual (and family). To reduce uncertainty with treatment decision-making, NPs’ need access to appropriate geriatric tools and resources. When health organizations prioritize geriatric focused tools and resources as an essential component of care, patients will more likely receive tailored care.
Recommendations for research include further study be broadened to include older people with cancer and an NCD accessing care from community clinics, and from continuing care facilities (LTC and Assisted Living). Conducting research in these other areas will not only provide a further understanding of NPs’ treatment decision-making but it will recognize that this population of older people are cared for outside of formal cancer care settings. The focus of this study was on NP treatment decision-making however it would be prudent to study how diverse healthcare professionals experience treatment decision-making affecting this population and triangulate their experiences with family members and older people living with these comorbid conditions wherever possible.
Conclusion
This study highlights the complexity of treatment decision-making when older people are living with an NCD and cancer. NPs encountered uncertainty and ethical challenges when typical treatments were not applicable. These challenges were compounded by limited supporting evidence and by healthcare systems that created barriers to care aligned with the patient's best interests. Functional assessments were a key factor influencing treatment decisions, although NPs did not always clearly recognize the relationship between function and cognition. NPs relied on relational decision-making to uphold an ethic of care, creating the opportunity for collaborative processes. The study findings highlight the unique and valuable role NPs play in treatment decision-making for older people living with an NCD and cancer.
Footnotes
Acknowledgements
The authors wish to thank the nurse practitioner participants who generously gave their time to share their experiences and to Dr. Esther Sangster-Gormley for her time with developing the ideas for this research project. This project contributed towards a PhD in a Nursing degree for KS.
Ethics Approval
Ethics approval was gained from the University of Victoria Human Research Ethics Board No. 22-0239.
Consent to Participate
All participants provided informed consent prior to participating in the study.
Consent for Publication
All participants provided informed consent for study results to be published during data collection.
Author Contributions
Kimberly Shapkin (KS): Conceptualization, methodology, investigation, formal analysis, manuscript writing-original draft, review & editing, project administration. Lorelei Newton (LN): Conceptualization, methodology, investigation, formal analysis, manuscript review & editing. Karen MacKinnon (KM): Conceptualization, methodology, investigation, formal analysis manuscript review & editing. Jayna Holroyd-Leduc (JHL): Conceptualization, methodology, investigation, manuscript review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study is available from the corresponding author upon reasonable request.