
Abstract
Background
Dialysis as treatment for kidney failure can result in significant physical and psychosocial symptom burden. Kidney supportive care (KSC), encompassing advance care planning (ACP), is an approach to care involving early identification and treatment of symptoms that improves the quality of life of people receiving dialysis. However, ACP is underused and often initiated late in the illness. The delay or lack of engagement in KSC by nephrology nurses until near the end of life may result in people receiving care that is discordant with their values, wishes, and preferences.
Purpose
The purpose of our study was to construct a substantive theory about the process of engagement in KSC by nurses in Canadian dialysis settings.
Methods
Using Charmaz's constructivist grounded theory method, 23 registered nurses working in hemodialysis and peritoneal dialysis were recruited to participate in two intensive interviews. Concurrent data collection and analysis were undertaken, with constant comparative analysis of codes until the attainment of theoretical saturation, as well as memo-writing and researcher reflexivity, to aid the emergence of categories and concepts.
Findings
In the substantive theory “Breaking Through the Glass Ceiling of Engagement—Having That Conversation,” three stages of engagement (Transactional, Intentional, Actional) are identified that describe nurses’ practice patterns of engagement in communication about goals of care with patients. This engagement is modulated by a boundary of professionalism and familiarity with patients, amid multi-dimensional contextual barriers.
Conclusion
Nephrology nurses have a vital role in discussions about goals of care and require training to enhance their communication skills.
Background and Purpose
Chronic kidney disease (CKD) is a global public health concern for its significant morbidity and mortality affecting over 10 percent of the world's population (Davison et al., 2015; GBD Chronic Kidney Disease Collaboration, 2020; Hill et al., 2016). Kidney failure is a serious complication of CKD, and at the end of 2022, it affected over 48,000 Canadian adults; specifically, over 29,800 individuals were receiving dialysis, and over 18,000 individuals were living with a functioning kidney transplant (Canadian Institute for Health Information, 2023). The mortality and symptom burdens in the dialysis population are comparable to those seen in individuals with advanced cancer (Moss, 2017; Naylor et al., 2019). Patients receiving dialysis could significantly benefit from kidney supportive care (KSC; Moss, 2017). KSC denotes the application of palliative care (PC) principles, such as symptom relief and expert communication through advance care planning (ACP) in which patients’ values and preferences for current and future care are elicited and prioritized, within existing kidney care services (Davison, 2021; Ducharlet et al., 2021; Gelfand et al., 2020). Nephrology nurses working in dialysis, however, do not routinely engage in meaningful conversations about ACP with patients and their families (Bachynski et al., 2024). Such under-utilization of supportive care in this population can lead to delayed or lack of PC services and unnecessary suffering (Davison, 2002; Ontario Palliative Care Network, 2019). Many individuals spend their final moments in acute care settings where the care provided often contradicts their desires for comfort-focused, home-based PC (Davison, 2010; Davison et al., 2015; Wachterman et al., 2017; Wong et al., 2012). Factors contributing to this misalignment include inadequate supportive or PC training of nurses and a general reluctance to initiate discussions about end-of-life (EOL) care (O’Halloran et al., 2018). The engagement of nephrology nurses in providing supportive care emerges as an area needing urgent exploration through a constructivist grounded theory approach to identify and address these impediments. In our study with Canadian nephrology nurses working in dialysis settings, we aimed to develop a theory explicating the process and factors shaping the nurses’ engagement in KSC using Charmaz's (2014) constructivist grounded theory method 1 (GTM). This theoretical interpretation provides a window of understanding into nephrology nurses’ experiences and practice patterns while normalizing these important conversations about patients’ goals of care (GOC) for a meaningful life and death.
Methods and Procedures
Constructivist Grounded Theory Method (GTM)
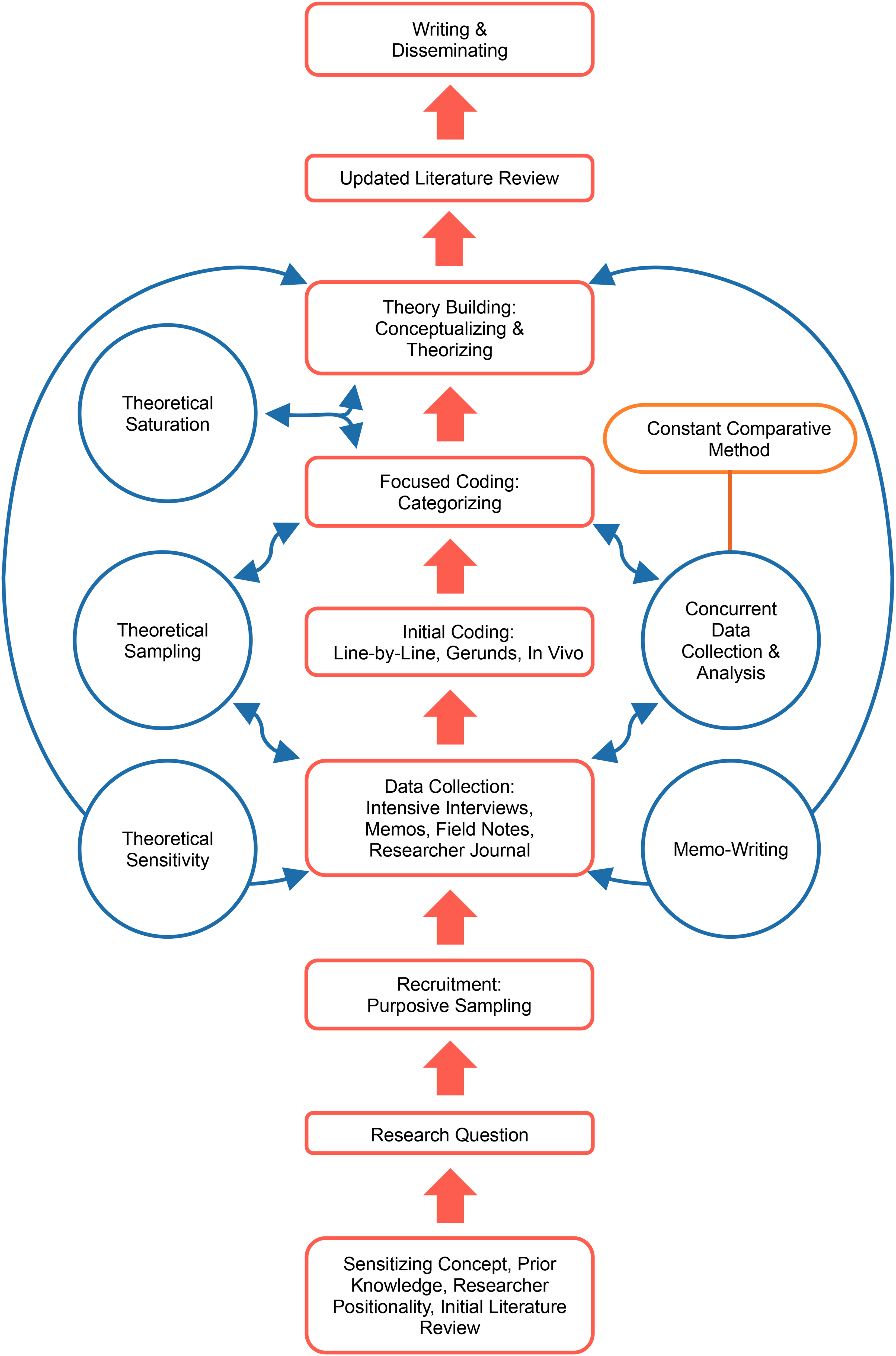
This qualitative study was designed according to Charmaz's (2014) constructivist GTM as depicted in Figure 1. The researcher uses an iterative, inductive, comparative, and reflexive approach to co-constructing—with their participants—a theory or interpretive understanding of a delimited problem within a specific substantive area (Charmaz, 2014). Theory is generated from constant comparison during concurrent data collection and analysis throughout the research inquiry (Chun Tie et al., 2019). The researcher uses coding, theoretical sampling, and theoretical abstraction to reveal hidden assumptions and provide new insights about and clarify fundamental processes (Charmaz, 2014). The resulting grounded theory is thus dependent on the researcher's view and is an interpretive portrayal of the participants’ realities (Charmaz, 2014).
Research Design and Protocol.
Sample and Setting
Study participants comprised nurses working in adult in-centre hemodialysis, and home peritoneal dialysis (PD) and hemodialysis (HD). In-centre hemodialysis is delivered in hospital-based outpatient or community-based satellite HD units where nurses provide direct on-site patient care and supervision (Agar et al., 2007). Home dialysis is self-administered by patients at home, with nurses providing remote care by telephone or follow-up care during periodic clinic visits. Purposive and snowball sampling were used initially to recruit 23 nephrology nurses working in in-centre hemodialysis for the study; later, by theoretical sampling, we sought and collected pertinent data from different nurses working in home dialysis based on the preliminary categories emerging from the initial interview data (Charmaz, 2014). At their request, participants are identified as P01, P02, et cetera, and their aggregated characteristics are in Table 1.
Aggregated Characteristics of the Participants.
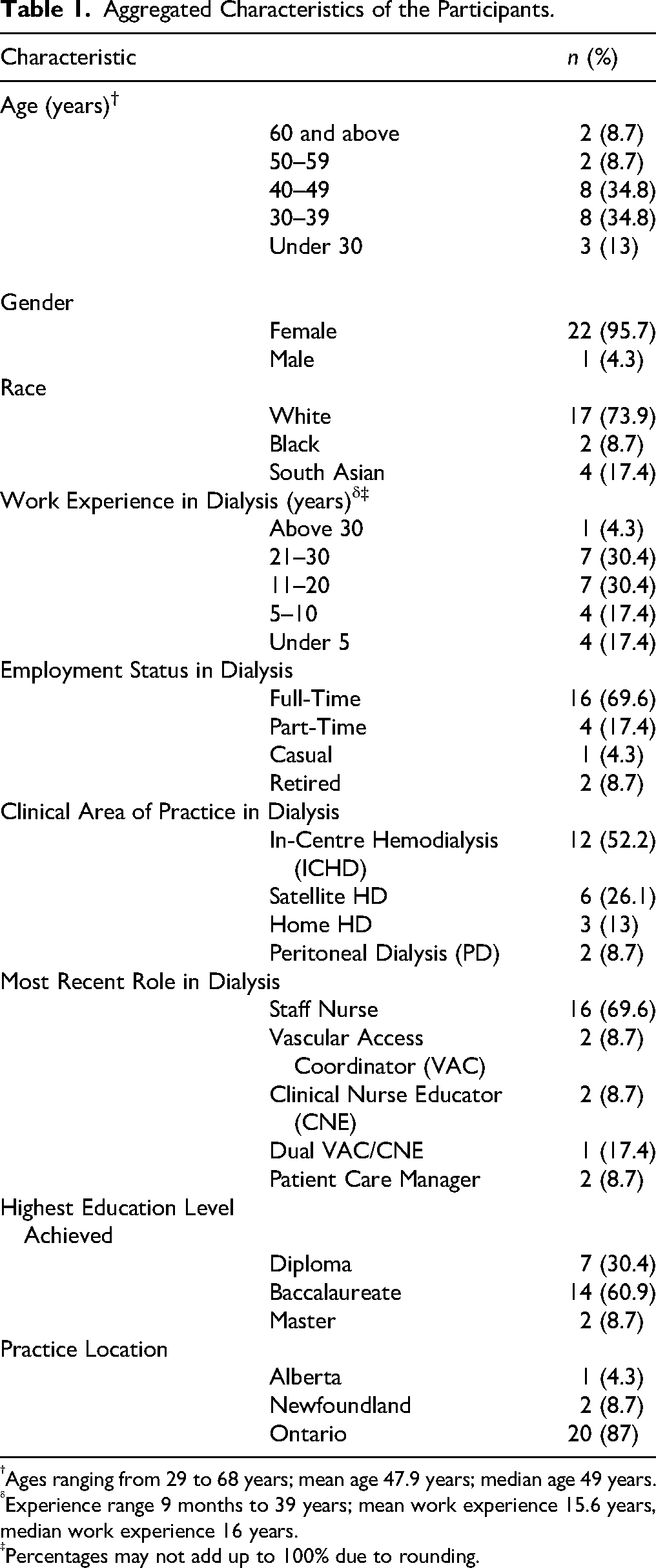
Ages ranging from 29 to 68 years; mean age 47.9 years; median age 49 years.
Experience range 9 months to 39 years; mean work experience 15.6 years, median work experience 16 years.
Percentages may not add up to 100% due to rounding.
Participants were primarily female (95.7%), White (73.9%), and working full-time (69.6%) as staff nurses (69.6%) in outpatient HD settings (in-centre hemodialysis 52.2%, satellite 26.1%) in Ontario, Canada (87%). Participants’ ages ranged from 29 to 68 (mean and median ages 47.9 and 49 years, respectively). Their professional work experience in dialysis ranged from nine months to 39 years (mean and median work experience 15.6 and 16 years, respectively). Most held baccalaureate degrees (60.9%).
Ethical Considerations
Ethics approval was obtained through the Health Sciences & Affiliated Teaching Hospitals Research Ethics Board at Queen's University (TRAQ # 6035254). Informed consent was obtained from participants prior to the first interview and was repeated prior to their second interview. All collected data were stored on an encrypted hard drive on the university's servers and anonymized during data collection and for publications.
Data Collection Tools
An intensive semi-structured interview was the primary method of data collection used to generate data (Charmaz, 2014). Using open-ended questions, the interview guide was divided into domains of inquiry such as the nurses’ collective and individual practice patterns, and the influences shaping their knowledge about and attitudes toward KSC (Guest et al., 2006; Schulz, 2012). Twenty-two participants were interviewed twice to allow for follow-up on emerging ideas from the initial interviews (Charmaz, 2014), and one participant declined the second interview. Interviews were primarily conducted on the virtual platform Zoom© using audio and visual features. The first author manually transcribed each interview as assisted by the speech-to-text program, Otter.ai©, manually revised the transcribed text for accuracy, and then uploaded it to NVivo© (QSR International), a qualitative software analysis program. After pilot testing the interview guide with the first two participants, the first and last authors refined and revised the interview questions to explore emerging concepts in depth such as the differing nurse-patient relationships in dialysis nursing practice. Research journaling and memo-writing also served as secondary data collection tools. Research journaling facilitated reflexivity, wherein the first author reflected on how their assumptions and subjectivities as a nephrology nurse practitioner impacted the research process (Birks & Mills, 2015; Polit & Beck, 2017; Roulston & Shelton, 2015). Analytic memos—recording the path of theory construction—were written successively in increasing abstraction by the first author throughout the research inquiry (Charmaz, 2014). Table 2 is the trustworthiness strategies for this study. Our study is situated within a social constructivist paradigm, which emphasizes the co-construction of knowledge through researcher-participant interactions and the influence of context on meaning-making (Creswell & Poth, 2025).
Trustworthiness Strategies for This Study (Based on Charmaz, 2006, 2014).
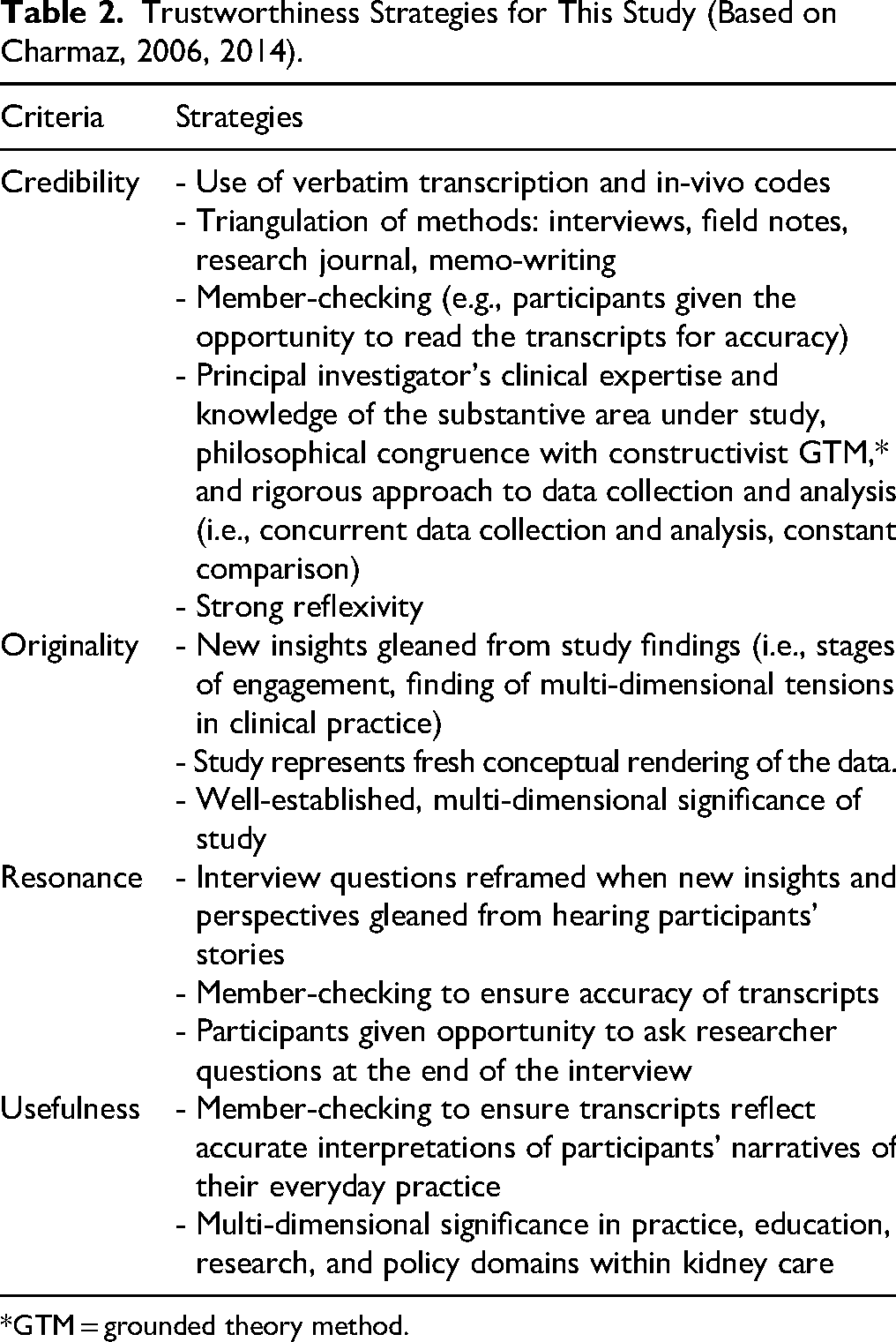
*GTM = grounded theory method.
Data Analysis
Data analysis of the transcribed interviews was conducted by the first author and confirmed by the last author. Data collection and analysis were conducted concurrently to facilitate constant comparison of the data—as captured in analytic memos—beginning with coding the first interview. In GTM, coding represents the critical link between data collection and the explanatory theory that emerges from the data; it reflects what the researcher sees in the data. Through coding, the researcher builds on the analysis from the ground up by remaining very close to and exploring all theoretical possibilities stemming from the data (Charmaz, 2014, 2015; Tarozzi, 2020). An ascending hierarchical approach was undertaken in the process of theoretical abstraction and elaboration in the study as outlined in Table 3—that is, moving from codes at the lowest level through to categories and then to concepts (Bryant, 2017; Bryant & Charmaz, 2007). The concepts or stages of the theory depict the process of engagement in KSC by the participants.
Outline of Codes, Categories, and Concepts for the Transactional, Intentional, and Actional Stages of Nephrology Nurse Engagement
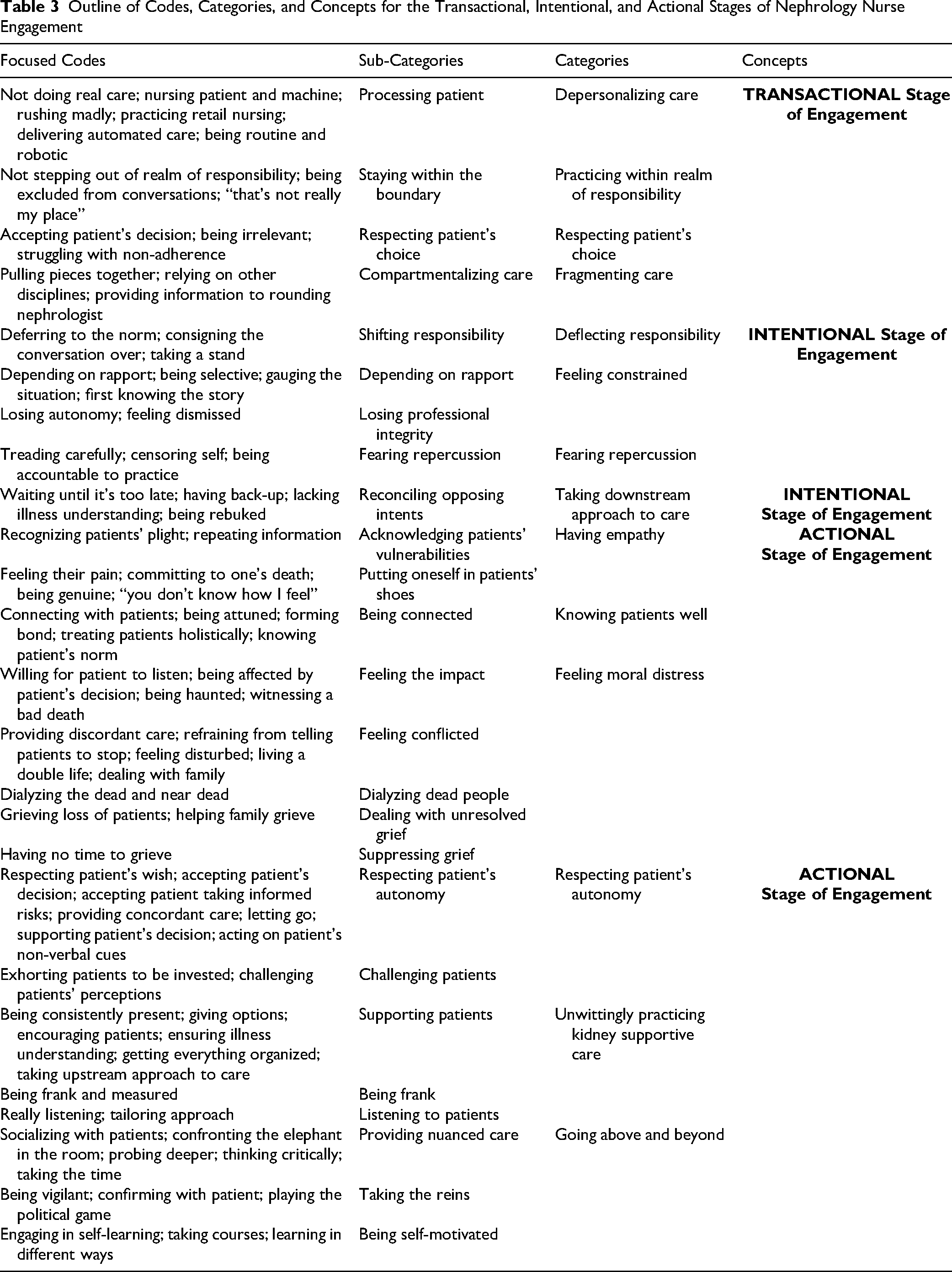
Constructivist grounded theorists use initial, focused, and theoretical coding phases to denote increasingly progressive levels of theoretical abstraction (Birks & Mills, 2015; Charmaz, 2014; Chun Tie et al., 2019). Initial coding, the first step in data analysis, involved detailed line-by-line reading of transcripts, followed by naming meaningful segments of data (for example, sentences or paragraphs) with short labels defining what was happening in the data using action-oriented gerunds to prevent early conceptual leaps (Charmaz, 2014; Chun Tie et al., 2019; Tarozzi, 2020). This was followed by focused coding in which the most significant or frequent codes were clustered together and re-coded into nascent conceptual and abstract categories, thus advancing the theoretical direction of the analysis (Bryant, 2017; Charmaz, 2014; Hadley, 2017). Theoretical coding is a sophisticated level of coding that helps to conceptualize the relationships between the substantive codes and define the relationships between categories in the focused coding phase (Charmaz, 2014). In this study, no attempt was made to use theoretical coding to integrate focused codes, which would have forced a theoretical framework on the analysis and interpretation of the data (Charmaz, 2014; Glaser & Holton, 2023). The data determined the direction of the analysis (Charmaz, 2014).
Findings
The substantive grounded theory on the process of engagement in KSC by nephrology nurses in Canada is called “Breaking Through the Glass Ceiling—Having That Conversation.” This theory comprises three fundamental elements: boundary, contextual factors, and the stages of engagement. Each of these elements and the ensuing products of analysis—codes, categories, core concept, and substantive grounded theory—are firmly grounded in the data comprising the experiences of nephrology nurses in KSC (Charmaz, 2014).
Figure 2 is the conceptualization of the theory. It begins with the implicit boundary between the participants’ professionalism and familiarity with patients receiving dialysis between the first stage (Transactional) and the two higher stages (Intentional and Actional). Through this boundary, the participants negotiated between closeness or familiarity with, and maintaining professional distance from patients. Awareness of this relational entity within the nurse–patient relationship privileges nephrology nurses to either retreat from or catapult toward such engagement. Additionally, KSC engagement is impeded or facilitated by a constellation of structural (knowledge gap), cultural (biomedical focus in dialysis), inter-relational (conversational discomfort), and systemic (lack of conceptual clarity of kidney supportive or palliative care) contextual factors. We write in detail about these contextual factors in a separate published paper (Bachynski et al., 2023). Finally, the stages of engagement denote differing commitments to engaging in conversations about GOC for life and death. These stages are inherently modulated by the negotiated boundary and contextual factors. For some nephrology nurses, their work paradigm evolves to a way of being wherein engagement in KSC is normalized into the everydayness of clinical practice, thus breaking through the glass ceiling of engagement in KSC. In the following model, we present the categories and concepts as outlined in Table 3 depicting the stages of engagement from which the grounded theory was constructed.
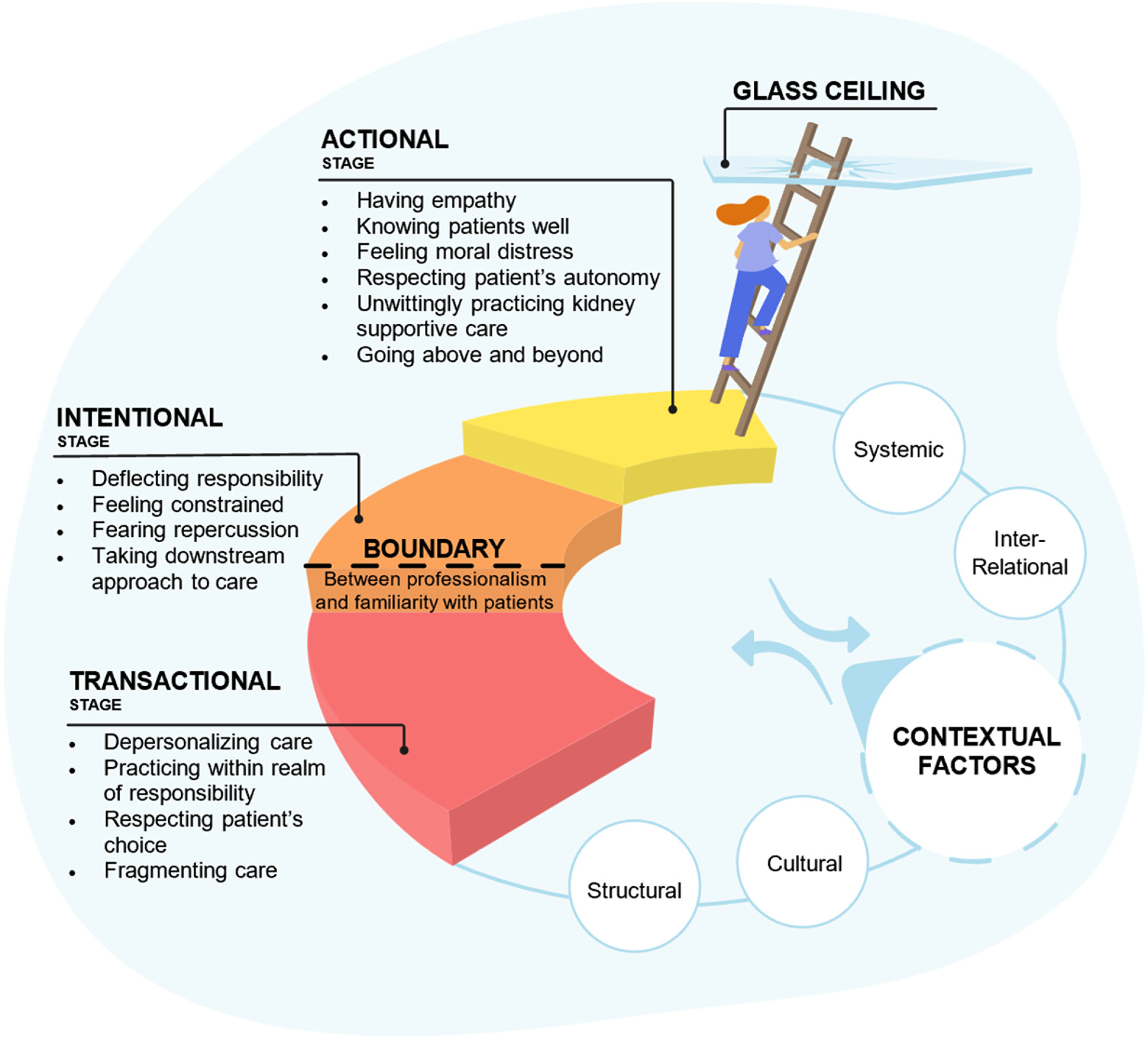
Conceptualization of the Theory.
Stages of the Substantive Grounded Theory: “Breaking Through the Glass Ceiling—Having That Conversation”
Transactional Stage
In the Transactional Stage, nurses concentrate on meeting the biomedical needs of patients within their professional boundaries, which could sometimes lead to neglecting other nuanced aspects of care. As a result, the care becomes routine—a straightforward transaction—emphasizing the distinction between the nurses’ professional responsibilities and their personal understanding of the patients. Engagement in KSC is not characteristic of this stage. This stage is comprised of four core categories: depersonalizing care, practicing within the realm of responsibility, respecting patient's choice, and fragmenting care.
Depersonalizing Care
This core category denotes the depersonalization in the delivery of care in a task-oriented clinical environment, where machinery takes precedence over the humaneness of those receiving dialysis. The participants described dialysis as a “hands-off kind of treatment” (P11), with patients being “processed” like retail items (P16) in a “kind of conveyor belt” system (P06). This “Amazon© [online business] nursing” setting (P16) often leads to a diminished connection with patients, as nurses are not “doing real care” in the same way giving a bed bath is considered the quintessential nursing act (P11). This leads to a depersonalized care approach that lacks meaningful, humanistic conversations about patients’ care goals during their critical kidney care journey.
Practicing Within the Realm of Responsibility
In this core category, there is a clearly demarcated boundary preventing nephrology nurses from participating in discussions about GOC or EOL issues. Nurse participants detailed how they do not extend beyond this boundary of professionalism and function. P06 steadfastly practices within her “realm of responsibility and qualification” unless she is compelled to assist patients. Nurse participation in the dialogue about GOC with patients is encumbered because such discussion is typically conducted by the nephrologist, nurse practitioner, or social worker. The perceived scope of one's role or practice within this context confines nephrology nurses to practice within their circumscribed professional boundaries.
Respecting Patient's Choice
This core category denotes the primacy of patients making their choices and subsequently their decisions around treatment or EOL issues, curtailing the nurses’ involvement. The participants respect and unconditionally accept these choices and decisions, thus delimiting the nurses’ contribution to such dialogue. P08 stated the nurse's role in EOL discussions involves “just giving information and the patient gets to make the decision. You’re not encouraging one way or the other.” Similarly, P06 noted patients may not “want to continue [dialysis] and again, that's their choice.” These statements have the effect of absolving the nurse of any responsibility, yet they negate the nurses’ genuine desire to contribute to any discussion.
Fragmenting Care
This core category involves a mix of care strategies and the distinct separation of healthcare services, driven by task delegation to specific disciplines and specialists. This approach requires nurses to integrate different care aspects into a unified plan, addressing the fragmented healthcare process. P22 expressed “the nephrologists didn’t want us calling them … sometimes we would reach out to the family doctors for help.” Her plight highlighted the challenge of consolidating care and gaps due to limited communication with specialists. P23 emphasized the value of multidisciplinary collaboration as vital for nurses dealing with issues beyond their expertise. P23 shared, “So, if there's any topic that I am not comfortable with, or I’m not familiar with, I reach out to the expert in that area to … provide support to that patient.” Notably, within this piecemeal approach, the holistic perspective can sometimes be concealed to the detriment of patients and their families, especially in critical areas like EOL care.
These experiences highlight a transactional approach to patient interactions, underscoring the fragmentation in today's healthcare. Such segmented approach often compromises the quality and continuity of care. This category makes clear the vital role nurses have in merging the complexities of multidisciplinary and specialized healthcare, ensuring cohesive and comprehensive patient care.
Intentional Stage
The Intentional Stage is marked by nurses recognizing the importance of discussing care goals but being unable to act on it due to contextual factors, such as time constraints, that heavily impact participants’ willingness to engage in KSC. These factors have a strong influence in preventing participants from progressing beyond mere endorsement of KSC. They have the desire (intention) but fail to implement it (as in the third stage of engagement—Actional). This stage comprises four core categories: deflecting responsibility, feeling constrained, fearing repercussion, and taking downstream approach to care.
Deflecting Responsibility
The participants reported a common practice of shifting the responsibility of engaging in GOC conversations to the physician or, at times, to the social workers and nurse practitioners. P13 described delegating this task to the nephrologist: “I said, I’ve noticed that patient has really declined … I asked him to come and assess the patient. He had a conversation if he felt the treatment was still going well, where his goals were.” P15 depicted nursing practice in which the conversation is consigned to a pamphlet: “Nurses just don’t … wanna talk about – they’ll ask but that's it. They don’t explore it any further than here's a pamphlet, some information for you to read about advance directives.”
This apparent routine deflection of responsibility in key GOC conversations suggests an implicit compartmentalization of roles and responsibilities, often leaving nurses on the margins of these conversations.
Feeling Constrained
This core category reflects being held back from initiating crucial dialogues about GOC and EOL concerns with patients. The rapport and relational comfort between nurses and patients were critical, with many nurses hesitant to initiate discussions about KSC without having an established rapport with patients or a level of comfort to initiate these difficult conversations. P10 expressed comfort in addressing sensitive conversations only with those with whom she has a “regular connection.” This need for a foundational familiarity modulates the nature and depth of the conversations, swinging them between professional detachment and personalized engagement.
Also, there is a concomitant subtle erosion of professional legitimacy and autonomy. Some participants often find their critical judgments being subjected to bureaucratic approval, diminishing their professional autonomy and undermining their role in patient care. P04 described: “We don't have physicians there all the time … the patients are more unstable and … we're using our nursing skills and judgment to possibly even call an ambulance; [however,] we have to call management now and get permission to do that, where before we had some autonomy.” This lack of autonomy within the healthcare system not only heightens frustration among those participants but also detrimentally affects patient care. Thorne et al. (2016) succinctly describe this situation as an ironic reality wherein those who are consistently involved in care are often the ones whose voices are silenced.
Fearing Repercussion
This core category reflects the intricate balance nephrology nurses must strike between patient advocacy and workplace norms and expectations. Some participants practice self-censorship to carefully navigate professional relationships. They are careful about making their concerns known to avoid conveying the wrong message. This conundrum renders nurses guarded within their interprofessional relationships to preserve their integrity, while simultaneously pushing the limits on behalf of patients’ interests and well-being. P04 wished for a nephrologist's presence in her satellite unit for fear of saying “something that a nephrologist is gonna say [to a patient], well, who had that conversation with you?” These participants described a desire for professional support and validation, which delineates the acknowledged boundaries of their advocacy within the care team. Thus, the fear of reprisal, the need for professional validation and support, and inherent professional accountability weave a complex tapestry, reflecting the multifaceted challenges and constraints faced by nurses in their pursuit of optimal KSC for their patients.
Taking Downstream Approach to Care
This core category is about the importance of initiating key conversations about GOC and EOL matters early in the patient's kidney care journey. The participants criticized the delayed timing of these discussions. P14 noted conversations start only “at that level” when the patient's condition has significantly worsened, limiting restorative care options. As a result, patients are often unprepared for the life-limiting nature of kidney failure. This delayed approach is systemic to which some participants contribute by not engaging in KSC early enough in the patient's kidney care journey. This omission can lead to severe repercussions. P04 recounted a coroner's criticism of the responsible nephrologist for not “paint[ing] a realistic picture” following the death of a patient with diabetes who suffered cardiac arrest two months prior to his death in the dialysis unit: This family thought this man was going to live forever. Did anyone ever have a discussion with this family that [he] has so many issues with his health on top of dialysis? … if the family was psychologically prepared that he may only last a year or two on dialysis … they would have been in a better place. [P04]
Delaying these conversations deprives patients of the chance to express their wishes at a time when it might significantly impact their future care.
Actional Stage
The Actional Stage is characterized by actioning with the intent to engage in conversations with patients about what constitutes the most meaningful care for them in their kidney care journey. Study participants transcend the contextual factors that negatively shape this engagement, thereby breaking through the glass ceiling of engagement as they cross the boundary demarcating professionalism and familiarity with patients. This stage comprises six core categories: having empathy, knowing patients well, feeling moral distress, respecting patient's autonomy, unwittingly practicing kidney supportive care, and going above and beyond.
Having Empathy
This core category connotes the multi-faceted and nuanced attribute of being able to relate to and understand patients’ situatedness and using this insightful knowledge as the motivation to approach patients with the intent to engage in KSC. At this stage, the participants expressed a deep sense of empathetic connection with their patients, actively attempting to put themselves in the patients’ shoes. P19 shared the conflict and pain of witnessing a patient caught in the dichotomy of not wanting to die and not wanting dialysis, highlighting the profound emotion experienced by nurses as part of their daily work. P19 said, “It breaks your heart that the patient spends four hours crying out in the chair. They don’t want to be here. They’re in pain … it is just heart-wrenching.” The unveiling of another's depth of suffering and innermost emotion is a powerful force that connects humans, transcending professional boundaries.
Being genuine and authentic in caring for patients is also revealed as a crucial aspect of empathetic nursing practice. P17 associated genuine care with a symphonic combination of “empathy, beautifully tangled or enveloped with your clinical portion,” implying a harmonious integration of these elements fosters genuine, beneficial, and truly caring interactions. Thus, genuine care is the way nurses connect with patients, leading to a mutual and authentic understanding of them—and which positions nurses for greater engagement in KSC.
Knowing Patients Well
This core category elucidates a transformative journey where nurses transcend the conventional boundary of professionalism to establish deeper, more holistic connections with their patients. Mutual understanding, genuine care, and holistic consideration for the patient's well-being converge, fostering an environment conducive to KSC discussions. The continued presence of nurses and their developed familiarity with patients’ norms and preferences position them as pivotal figures in directing patients toward KSC that is reflective of their values and preferences. As P10 described, “You have the most interaction with patients … over time … you know what is the norm for that patient … what they like … don’t like, what are their preferences.” Further, P19 alluded to mutual familiarity in which “you really are connected with your patients, and it's a community.” This sense of community and mutual connectedness enhance the supportive framework in which patients navigate their healthcare journeys, reinforcing the idea of care as a shared journey rather than isolated interactions.
Feeling Moral Distress
Moral distress refers to “experiences of frustration and failure arising from struggles to fulfill [health professionals’] obligations to patients, families, and the public” (Austin, 2011, p. 28) This core category denotes a state of internal conflict experienced by the participants between providing equitable care and navigating the complex, often conflicting, ethical and moral landscape of EOL care. The participants shared their experiences of enduring the emotional brunt of witnessing patient suffering and demise—difficult dilemmas that could lead to some existential misgivings. Shedding light on the ethical implications of dialyzing patients near the end of life, P17 candidly asked, “When did we start dialyzing dead people?” and P12 noted the potential to “dialyze someone [until] they are basically a corpse in a bed.” Such utterances elucidate the profound moral dilemmas encompassing the decision to prolong life without evaluating quality or respect for patients’ wishes. P19 revealed the inherent challenges and emotional toll involved in discussing potential discontinuation of treatment with patients, voicing the complexity and emotional considerations of such discussions: It's hard to have those conversations with patients and not telling them, like, oh, I think you should stop, but giving them the, you know, you don’t feel great and you’re not enjoying your four hours here. … we just kind of look at them and reassure them, like, it's okay if you don’t want to do this anymore.
P19 is rendered as a spectator at the sideline who strives to enable patient autonomy while communicating the harsh realities of their healthcare situations and the profound implications of potential treatment discontinuation, balancing conveying the factual severity of the disease without imposing the provider's viewpoints.
The collective narratives also expose the suppressed grief within the workplace. The nurses discussed the poignant pain when patients die and the accompanying suppressed grief due to workplace cultures. P19 mentioned, “Most of us have cried over many patients,” illuminating the unaddressed emotional and mental consequences of their profession and highlighting the need for structural support and acknowledgment of grief within the health professions community.
Respecting Patient's Autonomy
In this core category, nurses persevere through their moral distress because the patients will themselves to be kept alive. The nurses strive to navigate their ethical convictions and professional duties, aspiring to support and adhere to patients’ decisions. P21 reveals the struggle to accept a patient's decision to undergo medical assistance in dying (MAID), bringing forth the profound emotional ramifications and ethical considerations characteristic of such circumstances. P21 noted, “We feel like we're failing that person because that's not what we're supposed to be doing. We're supposed to help them live a full life.” Her poignant words highlight the internal conflict experienced by nurses, thrust between their desire to preserve life and their duty to respect and support patients’ EOL choices. Further, the role of challenging the patients is pivotal in sustaining patient autonomy. P05 suggested patients need to be accountable, affirming the symbiotic relationship between patients and nurses. P05 stated, “You have a responsibility, too,” pinpointing the mutual responsibility in sustaining care, thus underscoring the role of nurses in supporting the empowerment of patients to make congruent and informed decisions about their care.
Unwittingly Practicing Kidney Supportive Care
The majority of the participants were not able to define KSC. As such, this core category denotes nurses engaging in KSC without being aware they are practicing the tenets of ACP that are integral to KSC. Possessing an intuitive understanding of the benefits of practicing KSC is evident in this study. The participants described providing support to patients as they navigate the different transition points in the kidney care journey. Being consistently present for patients during “their entire week of treatments … is one of the highest priorities that is sometimes missed, but it's so crucial” [P13] in HD practice. In this manner, P13 has well transcended the boundary of professionalism and familiarity with patients to “almost like you become their family.” Once again, we make note of the symbiotic connectedness when both nurses and patients come away with their professional integrity and well-being intact, respectively. Within this developed connectedness, P05 attested to the importance of having GOC conversations as part of holistic care in stating, “I know what your dialysis prescription is, and I know what your medications look like. So why should I not know what your wishes are for every part of this journey, right?”
Such knowledge has allowed P05 the privilege of helping organize PC for a patient with kidney failure and late-stage cancer (who made the deliberate choice to stop treatment) and witness their (“wonderful”) dying process. Arranging EOL care for this patient according to her specifications illustrates how KSC helps patients graciously live with and die from their disease (Davison et al., 2015).
Going Above and Beyond
As a critical step toward breaking through the glass ceiling of engagement in KSC, this category denotes nurses transcending the boundary of familiarity with patients and the associated barriers delimiting conversations concerning GOC or EOL. The participants advocated for their patients well beyond minimum expectations. The participants in this stage act on their affirmation of advocating for patients. P12 bypassed the nephrologist and instead made a “not so backdoor plea” to the most responsible physician for a PC consultation for a patient deemed in need of such support. In noting she had “all of these conversations under the table … off the record, behind closed doors kind of thing,” P12 underscored the tenacity to stare down hierarchical structures in the healthcare system that puts primacy on process rather than patients’ interests. Rivaling these actions is the dogged determination to probe deep into the patient's existential situatedness and address their core concern, as exemplified by P05's response to an opening in a conversation with a patient who was failing from multiple comorbidities and stated he would be “better off dead.” After much probing, P05 elicited information that his cancer-stricken sister had recently died by MAID, and pointedly asked the patient: “How would you feel if you had to make that decision for yourself, hon? Because, I said, you have a lot of problems right now.” In this regard, P05 attested to being “vested” enough in this patient's care to take that further step to sensitively lead him to confront his mortality amid his suffering. Rather than objectifying the patient as the one in receipt of care, the patient's vulnerabilities are brought into the fore as part of providing holistic and nuanced care. Nurses in this category can assuredly be described as supererogatory in their obstinate pursuit of ensuring conversations about GOC and EOL issues are included in the daily dialysis lexicon and practice.
Glass Ceiling
The glass ceiling is the penultimate barrier preventing nephrology nurses from actualizing KSC involving communication with patients about their GOC, values, and preferences for care within a person-centred approach. Unlike the Transactional and Intentional stages, the Actional stage is significant for nurses straining toward (Santos Salas, 2006) this glass ceiling of accountability and responsibility for their clinical practice wherein primacy is placed on providing holistic care beyond merely attending to routine, taken-for-granted concerns in dialysis. Thus, in this person-centred approach, the patient is front and centre in the crosshairs of care. This level of patient advocacy circumvents roadblocks to quality communication, particularly the felt discomfort with initiating sensitive or difficult conversations with patients. The core concept of breaking through the glass ceiling illustrates breaking through this barrier in which the nurses feel empowered against all constraints, imbuing them with comfort and confidence in broaching and engaging in meaningful GOC conversations with their patients.
Beyond the glass ceiling lies a clinical environment encultured by a change in practice patterns wherein conversations with patients about GOC and EOL matters are ubiquitous and normalized, and are embedded as such. In so doing, nephrology nurses become responsive to the patients’ present and future needs and wishes for care, leading to concordant outcomes. Such inclusion in normative dialysis practice would support similarly empowered patients and their families to envision their futures and realize these wishes on their own terms according to their shifting GOC.
Discussion
The aim of this constructivist GTM study was to construct a substantive theory that would explicate the process of engagement in KSC incorporating ACP conversations by nephrology nurses in Canada. In a related literature review, there was overwhelming evidence of a lack of integration of KSC in nephrology nursing practice as manifested by the lack of engagement in ACP conversation with patients receiving dialysis and their families (Bachynski et al., 2024). In our study, such conversations are not routinely happening at the nurse–patient interface at the bedside. Conversations about what constitutes a meaningful life or death for the patient occur closer to the EOL (Axelsson et al., 2019, 2020; Hutchison et al., 2017; Lazenby et al., 2016). Implicit in this premise is that patients are (potentially) receiving care that is discordant with their values, wishes, and preferences.
Nephrology nurse engagement in KSC in the study has been shown to be significantly shaped by multidimensional contextual factors that permeate practice and affect care at the bedside. We had previously surmised how these factors, if left unaddressed, could contribute to the fragmentation of supportive care in which the responsibility for ACP discussions is consigned to some other practitioner (Bachynski et al., 2023). Such relegation is indeed reflected in the Transactional Stage where there is a clear demarcation between the nurse's ethical and relational, and professional responsibilities. This transference is lessened, to some degree, in the Intentional Stage, in which nurses appreciate the virtues of having ACP discussion but are constrained from actioning their intent due to a constellation of contextual factors, such as the lack of dedicated time to meaningfully conduct or the discomfort with having conversations with patients. It is in the Actional Stage where nurses show themselves capable of surmounting or navigating around these barriers and exercising their supererogatory tendencies to advocate for their patients by broaching and facilitating challenging and difficult conversations like EOL preferences (Axelsson et al., 2019, 2020). Part of the difficulty in engaging in such conversations is patients do not associate kidney failure with mortality the way patients living with cancer do (Naylor et al., 2019; Sellars et al., 2017). The progression of kidney failure is also unpredictable, partially contributing to the difficulty in initiating ACP discussions (Chen & Lin, 2021).
The lack of understanding of KSC underscores the knowledge gap in this regard. Regardless of dialysis work experience, all the participants acknowledged lack of formal inculcation in KSC, with some seeking related knowledge through learning online or being mentored by a colleague. In Frandsen et al.'s (2023) study, nephrology nurses with less than 10 years of work experience were likely to feel less comfortable in having ACP conversations with patients; however, those with over 10 years of experience could draw on their clinical experience and self-reflective capability to mitigate the discomfort with these conversations. This calls to mind Benner's (1982) five levels of proficiency (ranging from novice to expert) in the acquisition of a skill in which experience beyond mere longevity is predicated on exposure to practical solutions. On both accounts by Frandsen et al. (work experience) and Benner (skill acquisition), knowledge per se fell second to comfort with having the conversation as the more critical dimension determining their engagement in KSC (Haras et al., 2015). Neither work experience nor proficiency in communication skills could reliably account for the nurses’ practice patterns because ACP discussions were not routinely happening. This is to say, all nephrology nurses need multidimensional support, so they feel comfortable enough in their knowledge and communication skills about ACP, to normalize these difficult conversations. The participants have expressed interest in having standardized scripts as starting points to having the conversation.
Multidimensional tensions resulting from perceived differences in segments of practice that impact nurses’ approach to care have been identified in this study, with great attention paid to the differences in dialysis modalities. Similar to Wilkinson et al.'s (2016) findings, repeated contact with patients receiving PD allowed for greater nurse–patient relationship; however, in our study, this purported greater connectedness did not necessarily translate to greater frequency of ACP discussions. Unlike Wilkinson et al., our study yielded novel and more nuanced explanations in this regard. There is a perception that, although the template for ACP conversations may be similar in HD and PD, the answers may differ. More specifically, the concept of death is less imminent in PD than in HD because the latter becomes the default when PD fails. Patients receiving PD have better functional status leading to greater autonomy and self-directed care than their counterparts receiving HD; as such, PD recipients have a greater need for KSC as a result of having more treatment options available (Lu & Chai, 2021). This may lull nephrology nurses working in PD into thinking the need for ACP conversations is not urgent. On the other hand, participants view HD as the terminal choice—once a patient starts on this treatment modality, they do not leave. In this regard, the need to engage in KSC should prompt nurses working in HD to ensure timely KSC, but the lack of routine engagement in ACP discussions does not privilege one modality over the other.
The technical care given in dialysis is perceived as the antithesis to doing “real” nursing care. Such depersonalized care denotes distal nursing in which nurses lose their physical (touching), narrative (knowing the patient), and moral (recognizing the patient as Other) proximities with their patients in the interest of processing bodies (Malone, 2003). Such operational efficiency reflects the highly routinized, task-oriented approach to care—described by Tranter et al. (2009) as “get em on, get em off, and get home” (p. 34)—inherent in the Transactional Stage, where nurses, within their professional limits, focus on patients’ biomedical needs, often sidelining other nuanced aspects of care. There is a recognition of the pitfalls of distal nursing in the Intentional Stage, but it is in the Actional Stage that proximal nursing can be realized as an act of resistance against the commodification of patients as mere bodies (Malone, 2003).
Strengths and Limitations
This constructivist GTM study exploring the engagement of nephrology nurses in KSC, particularly in the conversation about GOC and EOL issues, is the first such study from a qualitative lens that is focused solely on nephrology nurses within the Canadian context. The inductive and iterative nature of the research design, and the meticulous and rigorous means of ensuring trustworthiness add to the significance of the study within the context of potentially contributing to embedding a nursing practice change that would meet the patients’ supportive needs in dialysis. Findings from the study contribute greatly to the current nephrology nursing scholarship on KSC.
A key limitation in our study, due to feasibility reasons, was the exclusion of nurses working in the pre-dialysis care setting, where meaningful GOC conversations should begin, as well as nurses working in inpatient nephrology units where patients receive care for complications related to their multiple comorbidities that might require them to re-evaluate their goals for current and future care. The inclusion of these nurses’ experiences would enhance our holistic interpretation of nephrology nurses’ engagement in KSC. In addition, there was lack of representation from parts of Canada outside of the three participating provinces in the study that would further strengthen the rendering of a broader portrayal of the Canadian experience and account for the regional and jurisdictional differences in practice.
Implications for Practice and Future Research
This study has wide-ranging implications. First, regional and jurisdictional differences in perceptions and practice patterns emerged in the study, underscoring the need for future research to reconcile the commonalities and differences experienced by nephrology nurses within the broader context of the current state of nephrology nursing in Canada. This includes nephrology nurses in the pre-dialysis clinic setting where the kidney care journey earnestly starts, as well as nurses working in inpatient nephrology units where the journey might end for some.
The transition in the level of engagement from detached to supererogatory requires a cultural change of embedding person-centred practice in nephrology nursing that truly privileges the patient-as-person's values, wishes, and preferences to guide clinical and non-clinical actions. The practice of KSC incorporating ACP can be emotionally and ethically challenging; as such, nephrology nurses require multidimensional support to help them navigate the complexities of providing quality KSC and acquiring the level of comfort needed to initiate conversations with patients and their families. This will require modes of practical learning beyond the didactic approach to kidney supportive or palliative approach to care, including tools for conversations such as script templates, and changing the dialysis culture that privileges efficiency over quality of care, thus allowing nurses to emotionally invest themselves in having these vulnerable conversations (Sellars et al., 2017). This should unite the interests of all interested parties in kidney care to promulgate a common understanding of quality integrated KSC at the public policy domain.
Conclusion
KSC, encompassing ACP, is an approach to care that improves the quality of life of people living with kidney disease, particularly those receiving dialysis, through the relief of suffering from the ravages of treatment. The longstanding relationships forged through frequent interface with patients receiving dialysis imbue nurses with the responsibility to engage in ongoing conversation with patients about their values, goals, and preferences for current and future health states. Evidence supports such conversations are not happening in this clinical space. Our substantive grounded theory—“Breaking Through the Glass Ceiling—Having That Conversation”—provides an explication for what is happening in the process of engagement in these conversations by nephrology nurses. This process takes time, requiring due consideration for nephrology nurses to attain a level of comfort with or knowledge about conducting such difficult and challenging conversations. This engagement is heavily modulated by the demarcation between professionalism and familiarity with patients, within inhibitory contextual barriers. Yet, nephrology nurses have the potential to transcend or break through these challenges to ensure these conversations are ubiquitous to the point of invisibility (Merrow, 2016). Nephrology nurses have a pivotal role in guiding patients along the kidney care journey, from the restorative phase to the EOL (Smith & Wise, 2017) by first making explicit the unsayable in the difficult conversations about GOC to ensure concordant care is delivered. This dialogic relational space allows nephrology nurses to reclaim an ethical and virtuous moment while their patients reclaim expertise “in their own experience of illness and what is important for them” (Freidin et al., 2019, p. 408), thus attesting to the symbiotic interconnectedness of nurse and patient.
Footnotes
Acknowledgements
The authors would like to thank the participants for their time and insights into their experiences with kidney supportive care.
Ethical Considerations
The study was approved by the Health Sciences & Affiliated Teaching Hospitals Research Ethics Board at Queen's University (TRAQ # 6035254) on February 7, 2022.
Consent to Participate
Informed consent to participate in the study was obtained from participants prior to the interviews.
Author Contributions
JCB conceived and designed the study.
JCB worked on the analysis and interpretation of findings, with feedback from PCP.
JCB drafted the article, and all authors provided critical feedback and approved the version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and or publication of this article: JCB was supported by the 2021 Canadian Association of Nephrology Nurses and Technologists (CANNT) Research Grant and the 2022 American Nephrology Nurses Association (ANNA) Career Mobility Scholarship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.