
Abstract
Background
A growing body of evidence supports the benefits of family engagement in patient care in intensive care units (ICUs). The English version of the FAMily Engagement (FAME) tool has been validated to measure ICU family engagement. This study aimed to validate the French-Canadian version of FAME.
Methods
Participant-level data from two prospective observational validation studies of the FAME tool, involving family members of patients from eight Canadian ICUs between May 2022 and July 2024, were included. Family members completed FAME in English or French-Canadian. Following discharge, family members completed questionnaires measuring care satisfaction and mental health (anxiety and depression). Reliability was assessed by internal consistency, and convergent and predictive validity by correlation between FAME and related outcome measures. A comparison of French and English scores was also conducted.
Results
A total of 104 family members completed the French-Canadian FAME questionnaire (age 57.0 ± 15.2 years; 62% women; 8% non-White; 53% spouse/partner). This version demonstrated internal consistency (Cronbach's alpha = 0.84) and convergent and predictive validity. FAME was associated with care satisfaction, but not anxiety or depression scores. There were no significant differences in overall FAME, care satisfaction, or anxiety and depression scores between the French and English cohorts (p > 0.05).
Conclusion
The French-Canadian version of the FAME tool demonstrated reliability and convergent and predictive validity in French-Canadian speakers, supporting the inclusion of French-speaking family members in future studies utilizing the FAME tool to measure family involvement in ICU patient care.
This study includes data from Measuring Family Engagement in Care (The FAME Study), ClinicalTrials.gov (NCT05659485): https://clinicaltrials.gov/study/NCT05659485
Keywords
Background & Purpose
Family members are increasingly recognized as essential partners in the delivery of patient care in the intensive care unit (ICU) (Marra et al., 2017). Family members can provide emotional and physical support to their loved one, participate as surrogate decision-makers, and even engage directly in care (e.g., delirium detection and reorientation, mobility exercises, feeding) (Olding et al., 2016). Engaging families in ICU patient care has been shown to enhance patient- and family-centered outcomes in randomized controlled trials (Duong et al., 2024; Wang et al., 2023).
Family engagement in patient care has been reported to decrease the duration of mechanical ventilation and reintubation rates, as well as reduce patient anxiety, delirium and post-traumatic stress symptoms, while improving care satisfaction and post-ICU quality of life (Duong et al., 2024). Family members have similarly been found to benefit from family engagement interventions with decreased anxiety, depression, stress, grief, and post-traumatic stress symptoms
The FAMily Engagement (FAME) tool was developed and validated to measure family engagement in ICU patient care (Goldfarb et al., 2022; Kifell et al., 2025). Before its development, there was no standardized instrument available to evaluate family member engagement in patient care. The FAME tool is currently used as a primary outcome measure to quantify changes in family engagement behaviours in clinical trials involving family members of ICU patients (Abdallah et al., 2025).
The FAME tool validation study was conducted in a primarily English-speaking population. There is a need for patient-reported outcome measures (PROMs) that are specifically tailored to diverse populations. Culturally and linguistically adapted tools are essential to capture accurate data, particularly in the context of self-reported health-related questionnaires, where items may be subject to variability in interpretation. Health practices and quality of life determinants may vary significantly across cultures. Cross-culturally adapted measures are particularly important in large, multicenter, and international trials (Guillemin et al., 1993). Developing culturally and linguistically appropriate versions of a tool helps prevent the underrepresentation of marginalized populations, minimizes attrition or missing responses caused by unclear or culturally incongruent items, and enhances the tool's applicability, promoting diversity in the participant population (Slade et al., 2021).
To expand the reach of future studies on family engagement strategies, the FAME tool was translated into French-Canadian and adapted for Francophone family members. The primary objective of this study was to validate the French-Canadian version of the FAME tool within this population. The secondary objective was to compare family engagement, satisfaction and mental health (anxiety and depression) scores between French- and English-speaking family members.
Methods and Procedures
Study Design
We conducted an analysis of participant-level data from two prospective cohort studies involving family members in the ICU setting. The first study, the FAME pilot validation study, was a single-center prospective observational cohort study conducted in a cardiovascular ICU from May to August 2022 (Hallot et al., 2023). The second study, the FAME multicenter validation study, was a prospective observational cohort study conducted across eight Canadian ICUs from January 2023 to July 2024 (Kifell et al., 2025). Institutional ethics approval was obtained for each study at each participating center. This study is reported according to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) reporting guideline for patient-reported outcome measures (Gagnier et al., 2021).
Development of the English Version of the FAME Tool
The development of the FAME questionnaire in English has previously been described (Goldfarb et al., 2022). The process followed an iterative and collaborative approach, guided by an interdisciplinary team with expertise in person-centered ICU care and questionnaire design, and included input from patient and family partners. Questionnaire items were generated by integrating the family engagement domains proposed by Olding et al. with the key principles of family-centered care outlined by the Institute for Patient and Family-Centered Care. The FAME tool consists of 12 items, each assessed using a 5-point Likert scale. On this scale, a score of 1 indicates strong agreement, while a score of 5 indicates strong disagreement. Raw item scores are then converted to a scaled score ranging from 0 to 100, with a raw score of 1 (strong agreement) corresponding to a score of 100, and a raw score of 5 (strong disagreement), to a score of 0. Higher scores indicate greater engagement in patient care. FAME scores are determined by averaging individual item scores. The tool assesses several engagement domains by self-report, including perception of engagement, family presence, communication and education, decision-making, contribution to care, and family needs (Goldfarb et al., 2022).
Development of the French Version of the FAME Tool
Following the initial development of the English version of the tool, a forward-backward translation approach was used to adapt the FAME questionnaire into French. This process was led by a clinical skills nurse with a high level of proficiency in French (Beaton et al., 2000). The French translation was then evaluated for cultural relevance and appropriateness by French-Canadian patient and family partners. Subsequently, the French-Canadian version of FAME was pilot-tested with French-speaking patients, families, and ICU healthcare professionals, including physicians, nurses, and allied health staff, who confirmed its clinical sensibility, face validity, and high content validity (Goldfarb et al., 2022).
Eligibility Criteria
Both studies adhered to the same eligibility criteria. Family members were eligible if they were at least 18 years of age, able to communicate in French or English, and identified as a family member of a patient who had been in the ICU for a minimum of 24h. Family was defined as any individual whom the patient wished to be involved in their care, regardless of biological relationships (Brown et al., 2015). To ensure data consistency, only one family member per patient could participate in the study.
Participant Recruitment
Research personnel approached family members in person for recruitment for both studies. In the single-center pilot validation study, research personnel approached consecutive family members of cardiovascular ICU patients as part of a quality improvement project. In the multicenter FAME study, research personnel consulted with the nurse in charge or another member of the treating care team to review patient lists and identify patients with eligible family members to recruit for the study. A bedside nurse or another member of the care team then sought consent from family members to allow research personnel to approach them. Once consent was granted, members of the research team approached family members to provide a detailed description of the study. All interested and eligible family members provided written informed consent before participating in the study.
Data Collection
At enrollment, participants completed the FAME questionnaire in either English or French, according to their preferred language. Questionnaires were administered either on paper or electronically via REDCap, a secure web-based platform for data collection. Demographic data, including participant age, gender, relationship to the patient, racial/ethnic background, and highest level of education, were collected. Within one month of hospital discharge, participants were invited to complete a follow-up questionnaire, comprising two instruments: the Family Satisfaction in the Intensive Care Unit (FS-ICU) survey and the Hospital Anxiety and Depression Scale (HADS). If the follow-up questionnaire was not completed after two email reminders, research personnel contacted participants via phone or text message. Follow-up was complete if the participant had at least one overall or domain score for FS-ICU or HADS.
Outcome Measures
The FS-ICU questionnaire is a validated and widely used tool to assess family members’ satisfaction with care in the ICU setting (Heyland et al., 2002, 2001; Wall et al., 2007). It comprises 24 items and is scored on a scale from 0 to 100, with higher scores reflecting greater satisfaction. The tool assesses two domains: satisfaction with care (the average of questions 1 through 14), and satisfaction with decision-making (the average of questions 15 through 24). The questionnaire also assesses critical elements of patient- and family-centered care, such as communication, information sharing, decision-making, and family needs. The FS-ICU questionnaire is available in French-Canadian (FS-ICU, 2021).
The HADS questionnaire is a validated and widely used questionnaire designed to assess symptoms of anxiety and depression (Bjelland et al., 2002; Zigmond & Snaith, 1983). It is composed of 14 items, with 7 items assessing anxiety and 7 items assessing depression. All items are scored on a scale from 0 to 3, with higher scores reflecting increased severity of anxiety or depression symptoms. A score of 8 or higher on either subscale (HADS-Anxiety or HADS-Depression) indicates the presence of borderline abnormal anxiety or depression symptoms, with a maximum possible score of 21 for each subscale (Zigmond & Snaith, 1983). HADS has been translated and culturally adapted for French-speaking Canadian populations (Roberge et al., 2013).
Data Analysis
Continuous data are reported as mean ± standard deviation, with between-group differences assessed using either an independent samples t-test or a one-way analysis of variance, as appropriate. Categorical data, presented as frequencies and percentages, were analyzed using the chi-squared test or Fisher's exact test, as appropriate. The reliability of the FAME tool was assessed through internal consistency testing using Cronbach's alpha for the overall 12-item scale. Although the FAME tool encompasses multiple domains of family engagement, the total score was conceptualized as representing a unified construct of overall family engagement in this study. Cronbach's alpha was interpreted as acceptable if the alpha was greater than 0.70 (Cortina, 1993; Streiner & Norman, 1995). Convergent validity was assessed using Pearson's correlation to evaluate the relationship between the FAME score, its relevant domains, and corresponding engagement elements of the FS-ICU score. The Pearson's correlation was interpreted as high (±0.50- ± 1.0), moderate (±0.30- ± 0.49), low (<±0.29) or none (0) (Cohen, 1988). Predictive validity was assessed through a multivariable linear regression model to examine the association between family engagement, measured by the overall FAME score, and family satisfaction with care, measured by the overall FS-ICU score. The model was adjusted for participant characteristics, including age, relationship to the patient, gender, racial/ethnic background, and highest level of education. Pearson's correlation was used to assess the relationship between FAME scores and HADS anxiety and depression scores. Missing outcome data was accounted for according to the framework for handling missing data in observational studies (Lee et al., 2021). Differences between the French and English cohorts were assessed using independent samples t-tests comparing overall, domain and subscale scores of FAME, FS-ICU, and HADS. A sensitivity analysis was conducted to assess the FAME score when excluding participants missing demographic variables, such as age, gender, relationship, racial/ethnic background, and level of education. Between-group comparisons of demographic data were conducted to assess differences between participants who completed the follow-up questionnaires and those who did not. Statistical tests were performed using the SPSS 29.0 software (IBM, Armonk, NY). P-values were two-sided with values ≤ 0.05 indicating statistical significance.
Results
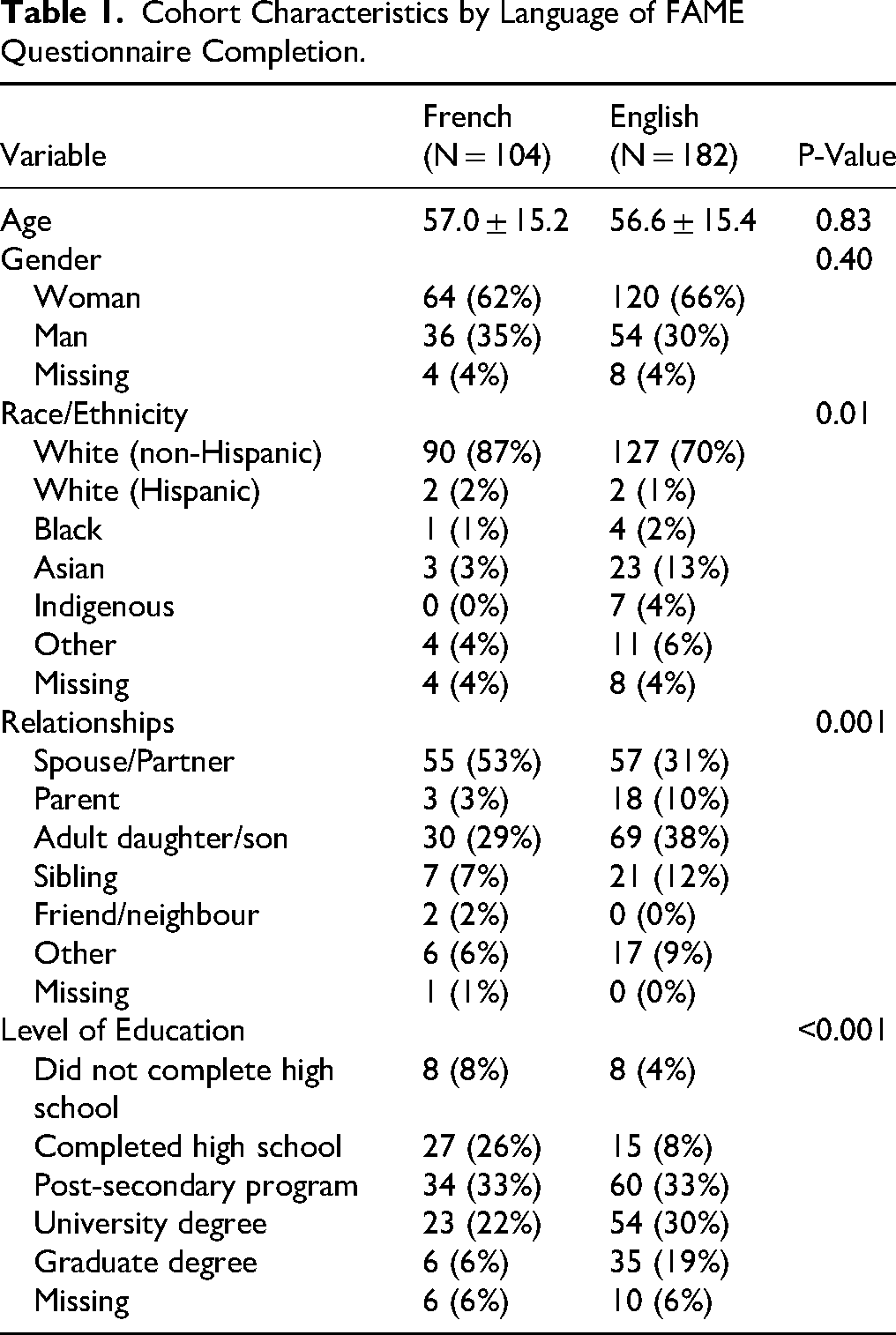
There were 104 participants in the French language cohort (mean age 57.0 ± 15.2; 62% women, 8% non-White; Table 1). The most common relationships with the patient were spouse/partner (53%) and adult daughter/son (29%). Compared to the English language cohort, the French language cohort differed significantly in terms of racial/ethnic background, relationship to the patient, and level of education (all p < 0.05).
Cohort Characteristics by Language of FAME Questionnaire Completion.
The overall mean French FAME score was 79.8
Follow-up data were available for 69 participants, resulting in an attrition rate of 34%. There were no differences in the FS-ICU and HADS scores or subscale scores between the French and English cohorts (p > 0.05). FAME scores were similar between participants who completed the follow-up and those who did not (79.1 ± 14.8 vs. 81.7 ± 15.0, respectively, p = 0.40). There were 28 participants (27%) who met the threshold for anxiety symptoms, 19 participants (18%) for depressive symptoms, and 14 participants (13%) for both anxiety and depressive symptoms.
The French-Canadian version of the FAME tool demonstrated high internal consistency (Cronbach's alpha = 0.84), ranging from 0.80 to 0.85 when individual items were removed. The FAME communication and education domain was moderately correlated with the FS-ICU communication score (r = 0.37; p = 0.002), and the FAME decision-making domain was moderately correlated with the FS-ICU decision-making domain (r = 0.46; p < 0.001). The FAME communication and education domain was moderately correlated with the FS-ICU decision-making domain (r = 0.46; p < 0.001). In the univariable analysis, the FAME score was associated with the FS-ICU score (p = 0.003). In the multivariable analysis, the FAME score (p < 0.001) and the level of education (p = 0.014) were positive predictors of the FS-ICU score, while age (p = 0.050) was a negative predictor of the FS-ICU score. FAME was not correlated to the HADS anxiety (r = -0.076, p = 0.54) or HADS depression (r = -0.03, p = 0.80) subscales. There was no difference in FAME scores for participants who met the threshold for anxiety or depression symptoms compared with those who did not (both p > 0.05).
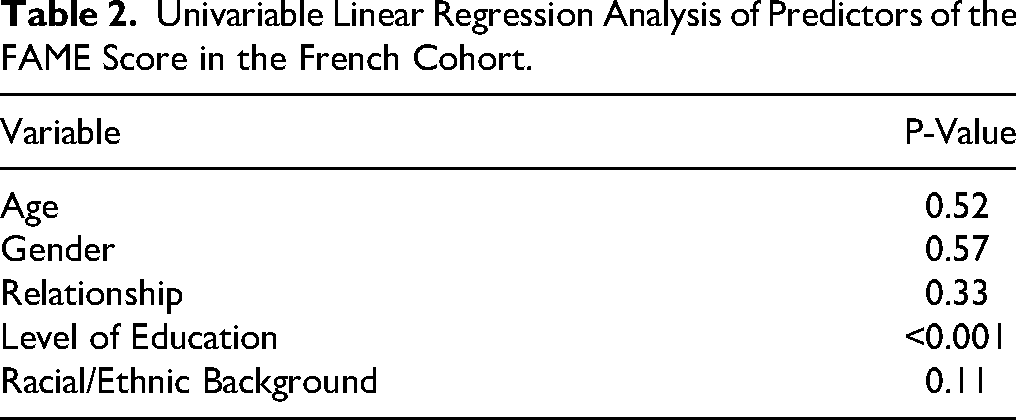
In the univariable analysis, the level of education was a significant predictor of the FAME score, whereas age, gender, relationship to the patient, and race/ethnicity were not (Table 2). A lower level of education was associated with a higher FAME score. Additionally, parents had higher FAME scores than adult daughters/sons (93.8 ± 7.5 vs. 76.9 ± 12.1, p = 0.03).
Univariable Linear Regression Analysis of Predictors of the FAME Score in the French Cohort.
There were no significant differences in FAME scores (p > 0.05) when excluding participants missing demographic data (age, gender, relationship, racial/ethnic background, and level of education). Additionally, between-group comparisons of demographic data revealed no significant differences between participants who completed the follow-up questionnaires and those who did not in the French cohort (p > 0.05).
Discussion
This study aimed to validate the French-Canadian version of the FAME tool. Our findings support the FAME tool as a reliable instrument, demonstrating internal consistency, and predictive and convergent validity. This study establishes the mean and range of FAME scores within the French-Canadian population. The FAME score for the French-Canadian version of the instrument was a predictor of family satisfaction, but not anxiety or depressive symptoms. These results support the use of the French-Canadian version of the FAME instrument for measuring family member involvement in ICU patient care.
Rather than developing a new instrument, the FAME questionnaire was translated into French to measure family engagement within the French-Canadian population. Evidence suggests that developing a PROM in collaboration with representatives of the target population, translating and adapting the original PROM is preferable to creating a new measure, as it preserves the established face and content validity of the original measure (Krogsgaard et al., 2021). However, following translation, it is essential to re-evaluate the psychometric properties of a PROM, as the translation process can alter the meaning and interpretation of individual items (Alpers & Hanssen, 2023). Indeed, many translated PROMs have not undergone formal validation, which may lead to issues with scientific rigour and reliability (Krogsgaard et al., 2021). The present validation of the French-Canadian version of the FAME questionnaire addresses this gap and supports its use for measuring family engagement in the French-Canadian ICU population.
Differences observed between the English and French cohorts in demographic characteristics and domain-specific engagement scores may reflect underlying variations in population characteristics, as well as the influence of language and culture on how family members participate in care. The French cohort, which had an overall lower level of education, demonstrated higher scores in the family presence domain. The mechanism underlying this relationship is unclear but may reflect a greater motivation among some family members to be actively involved in the patient's care. Hospitalizations, particularly in the ICU, can be a significant source of stress for family members, as the severity of the patient's condition often imposes substantial emotional strain and decisional responsibility. Family members with lower levels of education may experience reduced confidence in navigating the complexities of their loved one's care, which could heighten their desire to remain physically present. This group may have greater needs for guidance and support from the care team and may benefit from enhanced communication and targeted educational interventions. Supporting evidence from other healthcare settings corroborates this notion: a cross-sectional survey of over one thousand homecare caregivers found that lower levels of education were linked to a heightened desire for direct involvement in their relative's care (Woldring et al., 2024). In contrast, family members with higher levels of education may require less information due to greater health literacy, which may result in a reduced desire for active involvement in patient care. However, the limited number of studies examining the influence of educational level on family member engagement in the ICU underscores the need for further investigation of this finding in future research.
Another notable finding was that the FAME score was higher among parents of ICU patients compared to adult daughters/sons. This observation may be explained by the unique dynamics of the parent-child relationship, where parents often feel a heightened sense of responsibility for their child, even in adulthood, especially when the child is critically ill. To our knowledge, this study is the first to demonstrate that parents of adult children exhibit a higher level of engagement in patient care than other family members. However, the overall number of parents in the sample was low and further studies are warranted to explore the relationship between the nature of familial ties and the level of engagement in patient care within the ICU setting.
Implications and Future Directions
The validation of the French-Canadian version of FAME facilitates the inclusion of French-speaking family members in family engagement research and quality improvement initiatives. However, to ensure broader applicability, the FAME tool must be validated in other languages, settings, and populations. The FAME score should be cross-culturally adapted and validated within various French-speaking cultural groups. Developing multiple linguistically and culturally congruent versions of FAME could enable comparisons of family engagement behaviours and help identify significant cultural differences in family engagement practices. To gain a more nuanced understanding of these differences, qualitative research is warranted to explore the cultural factors influencing families’ motivations to engage in care.
Several family engagement strategies that have been associated with improved family outcomes, such as guided family presence, family meetings and structured communication protocols, are nursing-led or nursing-facilitated, underscoring the central role of nurses in operationalizing family engagement at the bedside (White et al., 2018; Yuan et al., 2023). ICUs can use FAME as a benchmark for performance, helping units to assess baseline engagement levels and monitor the impact of new family-centered initiatives. Beyond unit-level quality improvement, FAME also provides a framework for individualized practice. Nurses may use FAME to screen for family members with lower engagement levels and offer tailored opportunities to meaningfully support their participation in care.
There are several limitations to this study that should be considered. First, the study was conducted in Canadian ICUs, which may impact the interpretation and generalizability of the findings. Additionally, French-speaking participants were from the province of Quebec, and as such, the results may not apply to other French-speaking populations. The cohort also had limited representation of non-White participants, which may limit broader applicability. Future studies targeting family members of ICU patients should employ strategies to include a more diverse participant population. Furthermore, follow-up data were available for only two-thirds of the cohort, highlighting a need for strategies to improve participant retention, particularly among family members of ICU patients who may face unique and significant psychological stress.
Conclusion
The French-Canadian version of the FAME tool demonstrated reliability, as well as convergent and predictive validity. This validation paves the way for the inclusion of French-speaking family members in future interventional studies aiming to improve care delivery through family involvement.
Footnotes
Acknowledgements
With gratitude to Liza H’Ley Pierre and Claudine Robert for their invaluable guidance and support.
Ethical Considerations
Institutional ethics approval was obtained at CIUSSS West-Central Montreal (2022-3191; June 23, 2022).
Consent to Participate
All interested and eligible family members provided written informed consent before participating in the study.
Consent for Publication
Not applicable
Author Contributions
Funding
Dr. Goldfarb is supported by a Clinical Research Award from the Fonds de recherche du Québec Santé [298332].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, MG, upon reasonable request.