
Abstract
Background
Up to 33% of newly graduated nurses leave the profession within the first two years. This high turnover rate can burden care teams, negatively impacting the quality of care provided. To alleviate this problem, transition programs are offered to new nurses; however, they vary considerably in type and duration. Despite this heterogeneity, many researchers conclude that transition programs have a positive overall effect on new nurses’ competencies, self-confidence, satisfaction, stress, and retention, especially when they are longer than six months and have an explicit framework and structure, such as residency programs.
Purpose
To conduct a pre-implementation analysis of a residency program in the Canadian context.
Methods
Using a case study methodology, two sequential steps were performed to model the already implemented transition program and its components that needed to be upgraded to a residency program. Data were collected through 1) document analysis (n = 1,601) with selected interviews of stakeholders (n = 5) and 2) a survey with new graduate nurses (n = 29) and preceptors (n = 11).
Results
A preliminary logic model of the program was developed, depicting the structure of the proposed activities in terms of organizational orientation, unit integration, autonomous practice, and additional support measures. The operationalization of some program components was variable and sometimes missing, thereby affecting its quality.
Conclusion
This study showed how transition programs already implemented in clinical settings can be enhanced into residency programs by conducting a pre-implementation analysis. This can positively impact the transition of newly graduated nurses, including their retention.
Keywords
Background
In 2024, Health Canada published the Nursing Retention Toolkit, recognizing the negative impacts nurse turnover exerts on the healthcare system. Although the turnover rate varies across countries, studies have shown that the turnover rates for newly graduated nurses (NGNs) are higher than that of other nurses and remains high (approximately 18%–43%) (Bae, 2022). Several reasons can influence an NGN's decision to quit, but negative emotions due to a lack of support from colleagues, increasing complexity of care, or difficulty in balancing personal and professional life are cited often (ten Hoeve et al., 2020). This high turnover rate means there is a constant need to orient new nurses on the unit, which can burden care teams, has a negative impact on the quality of care (Aiken et al., 2012; Bae, 2022) and incurs costs for healthcare organizations (Bae, 2022; Hayes et al., 2012).
Literature Review
Studies on NGN turnover echo other studies on their transition into practice. Gardiner and Sheen (2016) stated that NGNs experience immense stress due in part to their workload, many express a lack of support, and some are victims of violence or intimidation from colleagues under the pretext that they need to build a “shell.” The experience of Canadian NGNs is no exception (Charette et al., 2019a; Duchscher, 2008, 2009; Duchscher & Myrick, 2008). Duchscher (2008) developed a model describing three stages which NGNs go through during their first year of practice and identified the intense negative emotions experienced in the first months of practice that lead to a transition shock (Duchscher, 2009). Duchscher mentioned the difficult conditions at the start of the professional career of NGNs, notably a heavy workload without the necessary support: “Within several weeks of being hired, these novices were afforded full patient loads equal to those of their senior nursing counterparts, but without reasonable access to expert counsel or practice support” (Duchscher, 2008, p. 444). Gardiner and Sheen (2016, p. 9) stated that the workload required of NGNs is often “heavy and unmanageable,” and Charette et al. (2019b) mentioned that NGNs have the necessary competences to ensure safe practice, but that it proves difficult to deploy them when faced with a high workload, which some feel is not suited to their level. Charette et al. (2019a, 2019b) concluded that NGNs need a period of stability and predictability of at least 4–6 months in the same care unit to enable them to fully integrate their professional roles and thus deploy their competences completely.
These studies demonstrate the importance of implementing strategies or measures to ensure adequate support for NGNs. Most hospitals offer transition-to-practice programs to help NGNs adapt to their new working environments, enabling them to further develop their competencies and self-confidence. These programs vary considerably in type and duration, from short programs of a few weeks to those lasting more than 12 months (Edwards et al., 2015; Kenny et al., 2021). Despite this heterogeneity, programs usually include a preceptorship period during which NGNs are gradually immersed in care units under the supervision of a nurse preceptor who needs to adapt to the new recruit's autonomy and progression (Charette et al., 2020). The abovementioned studies (Charette et al., 2019a, 2019b; Duchscher, 2008, 2009) have shown that short-term preceptorship programs do not offer optimal support to NGNs and are insufficient.
The Institute of Medicine (2011) recommended the systematic implementation of long structured transition-to-practice programs for nurses, such as nursing residency programs, without guidance on the structure or minimal requirements for doing so. In an integrative literature review, Chant and Westendorf (2019) identified key components for the sustainability of residency programs, such as the organizational support and dedicated resources, a conceptual framework, didactic component with clinical immersion and a structured evaluation tool. The Canadian Association of Schools of Nursing (2024) also highlights that the purpose of these programs is to support transition and the development of competencies through learning experiences.
The recommendation by the Institute of Medicine was based on the positive outcomes of long structured transition-to-practice programs, as attested by numerous systematic reviews (Edwards et al., 2015; Irwin et al., 2018; Ke et al., 2017; Kenny et al., 2021; Missen et al., 2014; Rush et al., 2019; Tyndall et al., 2018; Van Camp & Chappy, 2017). Researchers have concluded that a structured residency program lasting 6–12 months offers maximum support to NGNs during their transition, increases self-confidence, enhances competence development and deployment, increases job satisfaction and socialization, and decreases perceived stress.
Consequently, studies have shown that residency programs improve NGNs retention rates (Kenny et al., 2021; Van Camp & Chappy, 2017), although this measure was not always explicit, as personnel databank data were used to measure the retention rate. Turnover dropped from a ten-year average of 27% before the implementation of the residency program to 7.1% (Ulrich et al., 2010). Other studies showed an increase of 11%–41% in retention, although the sample sizes were sometimes small (Van Camp & Chappy, 2017). This decrease in turnover is associated with substantial savings for organizations, ranging from $543,131 (USD) to $823,620 (USD) annually (Rush et al., 2013), in direct and indirect costs. Similar savings could be possible in Canada as the cost of turnover is similar in Canada and the United States (Duffield et al., 2014). It is also important to note that turnover has a non-economic impact on work-group processes, nurse staffing ratios, mental health, job satisfaction, and many patient outcomes (Bae, 2022). Therefore, residency programs have the potential to significantly affect many outcomes.
Some nursing residency programs have already been implemented in Canada, but are reserved for critical care units, such as emergency and intensive care (Bérubé et al., 2008; Bérubé et al., 2012). However, less than 15% of NGNs practice in these units (Marleau, 2021), as most (73%) start their practice in acute care (e.g., medical-surgical units). The Canadian Association of Schools of Nursing (CASN, 2024) recently proposed a six-month competency-based residency program to which health organizations can apply, but the results of this program are not yet known.
As most organizations offer minimal transition programs, the first step in implementing a residency program is to proceed with a pre-implementation analysis to describe the current transition program and compare it with existing guidelines regarding the structure of nursing residency programs (Brook et al., 2019; van Rooyen et al., 2018). Programs can be illustrated using a logic model (Adams & Neville, 2020; Porteous, 2013) that shows different aspects of the program, such as the target population, objectives, inputs (resources), activities (program components), outputs (product of activities), and outcomes (intended effect). Once the program is modeled, an analysis of operational fidelity can be undertaken, which is a comparison between how the program or activities were designed and what actually happened (Sidani & Braden, 2021). The need for this study arose from a partnership with a healthcare organization who wanted to upgrade their transition program offered to NGNs, to increase retention.
Nursing Education System in Quebec, Canada
In Quebec, Canada, there are two routes to the nursing profession. After graduating high school, students can either complete a three-year nursing program from a general and technical college (called CEGEP) or a two-year pre-university health science program from a CEGEP and then be admitted to university, where they can complete a three-year Bachelor of Science in Nursing (BScN) program. Upon graduation from either program, graduates are eligible to take a professional licensure examination by the nursing board (Ordre des infirmières et infirmiers du Québec) to obtain their practice license. The exam is held only twice a year (September and March) and the NGNs can practice with a title of “candidate to the profession” before getting licensed. This title allows nurses to perform almost all activities permitted by law, with a few exceptions. In this study, NGNs were referred to as nurses within their first year of graduation, with no differentiation between pre-and post-licensure. Nurses holding a CEGEP diploma have an integrated track to pursue a BScN, which is only two years.
Purpose
This study aimed to conduct a pre-implementation analysis of a residency program in the Canadian context. Specifically, the aims were to 1) construct a logic model of the program already implemented to support the transition of NGNs and 2) assess the operational fidelity of the implemented program. To address these aims, the following three research questions were asked:
What measures that facilitate the transition of NGNs have been implemented at the partner organization and how are they structured? What are the inputs and outputs of these measures? Are the measures delivered or offered to all NGNs as intended?
Methods and Procedures
This study was guided by Sidani and Braden's (2021) framework for implementing and evaluating complex interventions. When examining processes, two main stages are identified: pre-implementation and implementation. Collaboration with the study environment is considered central and essential for both stages. While the pre-implementation phase consists of preparing the environment and involving the stakeholders, the implementation phase involves implementing the changes in practice (Sidani & Braden, 2021). In this study, the pre-implementation phase was carried out in two sequential phases, which are explained in detail in the following subsections. This manuscript follows the COREQ reporting guidelines (Tong et al., 2007).
Study Design
A case study design was chosen (Stake, 1995, 2000), as it enables the researcher to study a phenomenon in depth and examine its components, interrelationships, and context to draw a holistic picture of the phenomenon under study (Patton, 2015; Polit & Beck, 2017). The strength of this methodology lies in the in-depth study of the case, which requires extensive data collection (Polit & Beck, 2017). This methodology is particularly useful when the researcher is interested in a program and its complexity (Stake, 2000).
In Phase 1, data were collected about the current program supporting the transition of NGNs at a partner organization to create a preliminary logic model of the program. This was done through document analysis, followed by a descriptive qualitative component. This phase was essential for understanding the links between the inputs (resources) and activities implemented to support NGNs from the perspective of stakeholders. Once sufficient information was gathered to acquire an overview of the program and create the logic model, Phase 2 was implemented to assess the operational fidelity of the activities through a descriptive survey completed by NGNs and nurse preceptors involved in the program.
Setting, Sample and Recruitment
The setting was a Quebec healthcare organization known as an integrated university health and social services center, which comprises all public establishments in a region, such as hospitals, primary care clinics, rehabilitation centers, and long-term care facilities. From the onset of the project, discussions were held with the organization's office of the Director of Nursing to secure the collaboration of key informants essential to this type of project (Sidani & Braden, 2021). To achieve an in-depth understanding of the case, researchers must select key informants with in-depth knowledge of the phenomenon under study (Stake, 2000). Six key informants were selected and invited to participate; only one refused.
In Phase 1, key informants were selected through purposive sampling using a critical case-sampling strategy (Polit & Beck, 2017). Key informants were selected based on their positions within the organization and their knowledge of the current program. They held positions as clinical nurse specialists (CNS) or similar positions within coordination, overseeing clinical support measures and competency development of nurses. Potential participants were contacted via e-mail by the principal investigator, who stressed the confidentiality of their participation in the project and invited them to participate in the study.
For the second phase, a population sample comprising all eligible NGNs and nurse preceptors was recruited. To be eligible, NGNs had to be graduates and newly employed in the organization for less than one year (no restrictions on units), and preceptors should have supervised at least one NGN in the previous year. The target population included approximately 400 participants (200 NGNs and 200 preceptors). All eligible participants were sent a letter containing two QR codes: one leading to a short 3 min video explaining the project, and the other leading to the survey platform.
Data Collection
Data collection began with a document analysis, performed in the spring and summer of 2022. The collaboration of the Director of Nursing was essential to gain access to all relevant documents describing the current program or any activities implemented to support the transition of NGNs, including the organization's internal policies. Next, semi-structured interviews were conducted in the fall of 2022 by the principal investigator to clarify the data collected and gain a deeper understanding of the context in which the activities were implemented or occurred (physical, social, and political), as well as their structure. Key stakeholders were questioned about their roles and knowledge of the activities identified in the documentation analysis, as well as activities that would not have been uncovered through the analysis. The interview guide was developed by the principal investigator based on the document analysis and revised by the research team. Interviews were conducted virtually by the first author using Microsoft Teams, at times agreed upon by each participant and recorded for transcription purposes. NVivo's online transcription service was used to this end, and the transcripts were verified by a research assistant who removed all names or identifying features in the transcripts to ensure confidentiality.
A descriptive survey was conducted for Phase 2, which was developed collaboratively by the research team based on the data collected during the first phase. It was launched in March 2024 using the online platform LimeSurvey and was divided into four sections. The first section contained information about the study, and participants had to confirm that they understood that they had consented to participate by filling out the survey and submitting it. The second section included demographics with eight questions related to age, gender, identification with a visible minority or LGBTQ + community, and education level and experience. Section 3 was to be completed by the NGNs only and included 49 questions (39 quantitative and ten open-ended) about their experiences and the different activities in which they participated as NGNs, aimed at supporting their transition. Finally, the last section was to be completed by preceptors regarding their experience supervising an NGN. This section comprised 23 questions (12 quantitative and 11 open-ended). No question was mandatory.
The survey was pretested by two graduate students who were aware of the organization's current practices. Three questions were added to Section 3 (NGNs) and one was modified for a total of 49 questions (42 quantitative and 10 open-ended). The pre-test also permitted the completion of the survey, which was estimated to take 20 min for NGNs and less than 5 min for preceptors. The survey was conducted anonymously.
Data Analysis
The analysis of each activity supporting the transition of NGNs began with documentation collected using directed content analysis (Hsieh & Shannon, 2005). Data were extracted by research assistants (AR, JB, EQ) using a standardized spreadsheet, enabling the first stage of data reduction and capturing information about the activity, its implementation and resources, structure, outcomes, facilitators and barriers, and relations with other activities or components of the transition program. Regular meetings between the principal researcher and research assistants ensured consistency in data extraction and helped identify areas for further exploration during interviews with key informants. The interview analysis was performed independently by a research assistant and the principal investigator, and followed the same data reduction and coding steps to understand the structure of each activity in the program and their operationalization, which in turn was condensed into categories. Data triangulation (Denzin & Lincoln, 2018) was performed for each activity, using data from document analysis and interviews. Data analysis and categories were discussed among the research team.
Quantitative data from the survey were exported for analysis using Microsoft Excel. Descriptive statistics were presented as mean and standard deviation (SD), or frequency, as appropriate. Qualitative data from the open-ended questions were analyzed using directed content analysis.
Ethical Considerations
This study was approved by the partner organization research ethics committee for two different projects (Phase 1: #2022-4456; Phase 2: #2024-5247). Participants who participated in the interviews provided written informed consent. Survey completion was deemed as an implicit consent form. Participation was voluntary and confidential, and the only anticipated risk was the time required for data collection. Participants received no remuneration for taking part in this study, but the participants in the survey could win one of the eight $25 gift cards.
Reflexivity
This study was a part of the research program of the principal investigator, who was a researcher at the partner organization but had never worked as a nurse there, which gave him an external perspective. The principal investigator was a nurse with many years of hospital experience, which enabled him to understand the participants’ words and contexts easily. He has been studying transition programs for several years, through literature reviews and other research studies. To enhance reliability and credibility, regular meetings with members of the research team were conducted throughout data collection and analysis. The preliminary results were presented to the organizational partner for feedback on data accuracy and presentation.
Results
Data collection and analysis were conducted in French, but results (categories and verbatims) were translated for the publication of this paper. The results are presented as an integration of Phases 1 and 2. First, the participants characteristics are presented, followed by the preliminary logic model of the residency program and then the four categories of activities in the program.
In Phase 1, 1,601 documents were analyzed, ranging from organizational official policies to training session materials (e.g., PowerPoint presentations). Five semi-structured interviews were conducted with key stakeholders holding various positions (
Phase 2 survey participants’ characteristics are presented below.
Survey Participants’ Characteristics
Forty participants completed the survey (29 NGNs and 11 preceptors) out of a population of approximately 300 (150 NGNs and 150 preceptors). The NGNs were mostly women (n = 27; 93.1%) with an average age of 24.3 years (SD = 4.7). Their initial education was mostly from a CEGEP (n = 20; 69%), with most pursuing a BScN (n = 16; 80%). Only one participant (3.4%) identified as part of a visible minority or the LGBTQ + community. The preceptors were also mostly women (n = 9; 81.8%) with an average age of 39.4 years (SD = 10.4). Their initial education was mostly from a CEGEP (n = 9; 81.8%), with most having already completed their BScN (n = 7; 77.8%). While all participants work at the same organization, specific place of work or unit was not collected (Table 1).
Logic Model of the Program
Based on documentation and interviews, a preliminary logic model of the residency program was developed (Figure 1). It clarified the context of the program, which was a challenging transition and transition shock experienced by NGNs. The intended users were NGNs and other employes who provided clinical support, such as preceptors. It was important to include them as they needed to be trained and cognizant of the program. The ultimate objective of the program was to ensure the optimal integration of NGNs. Two explicit outcomes of the program were identified: 1) competency development at three and six months, and 2) retention using human resources records. Other outcomes were discussed by participants, but were rather implicit and not measured, such as an increase in satisfaction or a decrease in stress.
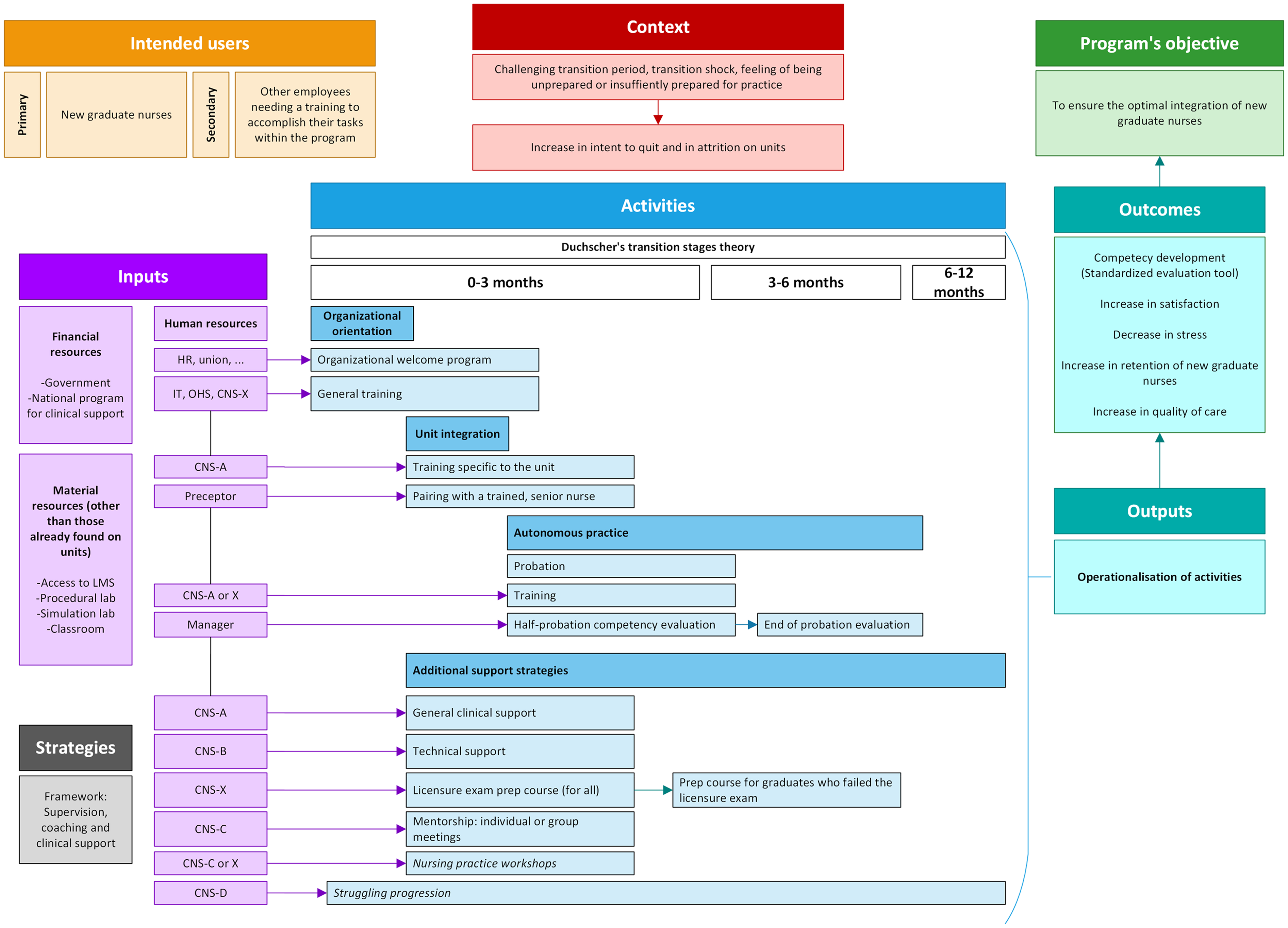
Preliminary logic model of the residency program.
The inputs, which were the resources needed for the program, were divided into financial, material, and human resources. Financing comes from the government, which implements provincial measures within a national framework for clinical support (Ministère de la Santé et des Services Sociaux du Québec, 2008). The framework was non-prescriptive: it outlined broad objectives and steps organizations should take to implement a transition program (determine needs, design the intervention, implement it, and evaluate it). The partner organization went beyond this framework and designed its own framework for supervision, coaching, and clinical support.
Many different people were involved in the program, but most resources were from a coordination that focused on nurses’ competency development. Although some activities (the components of the program) clearly identified the people in charge of or overseeing the activity, others were ambiguous. For example, at the partner organization, the CNS had a specialization that could include mentorship and clinical support. In the clinical model, these specializations were marked as CNS-A to CNS-D. When the resource was ambiguous, it was marked as CNS-X, meaning that many CNS with different specializations could be asked to collaborate during that activity.
The last two elements (and the most central parts) of the logic model were activities and outputs (survey results, Table 2), which are discussed in the next section.
Activities in the Program and Outcomes
The activities implemented in the partner organization to facilitate the transition of NGNs were divided into four categories: organizational orientation, unit integration, probation, and additional support measures. They were based on Duchscher (2008) transition stages theory, with a focus on technical skills and unit routines in the first three months and later, on the development of professional identity. The program lasted for 12 months, although there was explicit mention that the transition period could extend up to two years.
Organizational Orientation
During the first week of hiring, the NGNs participated in an organizational welcoming program and general training. These activities lasted approximately five days, during which the new employe received general information about the job and employer from the human resources department and attended a series of general training sessions intended for all new nurses. Examples of general training include informatics access and systems (such as electronic medical records), principles of safe patient movement, and procedures and protocols applied to all units.
Most participants from the survey took part in the organizational welcoming program (n = 23; 79.4%), whereas some did not participate because they already worked in the organization. All the participants participated in general training activities (n = 29; 100%). Some thought that these activities were not relevant for people already working in the organization, because they already knew what was covered (“[it was] too general, not relevant for most people who are already working here, or those who did an internship here.” Survey ID19 - NGN) and because it was not particularly relevant for the unit they were assigned to (“The orientation is not adapted to some units, for example short-term care in general.” Survey ID39 - NGN). This was corroborated in an interview with a participant. The general training is standardized. Right now, it's a three-day training. […] We are looking into making it relevant so that the training is given to the right employee at the right time. […] For example, the way our general training is designed, it won’t be relevant for an NGN who will work in psychiatry. However, once their integration and probationary period is over, if they float, then they might need this general training. (Interview Participant B)
Unit Integration
After organizational orientation, NGNs were welcomed to the units in which their integration commenced. Unit integration comprised two activities: specific training and preceptorship period. Specific training was unit-dependent; it could be received on the unit or in a classroom-like setting, and the content is necessary for the nurses’ work on that unit. There was confusion about how this training was referred to across the units: some called it “training,” others called it “orientation,” or integration. Recent years have seen a boom in the use of web-based platforms so that training can be delivered online in synchronous or asynchronous modes. Consequently, some training was delivered online, whereas some was provided face-to-face in the classroom, either as didactic sessions or workshops. Finally, approximately one-third of the new nurses did not receive any specific training (n = 11; 37.9%), as it was not mandatory and was unit-dependent.
Preceptorship involves the pairing of an NGN with an experienced nurse who supports them in integrating into the care unit, acquiring shift-specific routines, and continuing to develop their skills. This period corresponds to the time when the new graduate is supernumerary, meaning that they share the preceptor's patient assignment while remaining responsible for the care they provide. The preceptorship period has a fixed length depending on the sector (e.g., critical, acute, or long-term care), but the preceptor can request to extend the preceptorship for a few days if they think the NGN is not yet capable of providing autonomous care to their patients.
At this partner organization, the duration of the unit integration, including specific training and preceptorship, was generally ten days for most acute care units and could go up to 20 days for critical care units. According to the documentation, the duration of this period was flexible and could be extended based on the needs of NGNs. However, the interview participants mentioned that the length of the period was more often dependent on the unit's resource requirements; therefore, rather than lengthening the period, it was more often shortened. I would say ten days is what's usually recommended. But often, […] it's not possible to give them ten days, depending on the number of nurse preceptors available, depending on the resources that are not sufficient in number to be able to provide these ten days of orientation. […] Unfortunately, and that's my own opinion, we’re putting their development, their learning in second, because the unit efficiency is more important, because we need these professionals, otherwise we can’t function. (Interview Participant E) I would love to give you the guarantee that every NGN gets their ten days. But in reality, and I’ve worked extensively in acute care, they don’t even get their ten days. (Interview Participant B)
In the survey, approximately half of the preceptors agreed that they felt pressure (n = 3; 27.3%) or sometimes felt pressure (n = 2; 18.2%) to end the preceptorship, even if they thought the NGN was not ready to take on their autonomous practice, which is consistent with the previous quote that in some cases, the unit's needs are a priority over the development of NGNs. The preceptors also mentioned that they were not advised sufficiently before being paired with an NGN, with only one preceptor saying that they were advised in advance. This was corroborated by NGNs in open-ended answers in the survey: “There was no official pairing: I was paired with the preceptor who was present on that day” – Survey ID41 - NGN.
NGNs were paired with a preceptor for an average of 10.7 days (Range: 1–20, SD: 6.3); most NGNs (n = 17; 58.6%) found this to be sufficient and did not require more days. By contrast, the preceptors felt that the number of days spent in preceptorship was insufficient (n = 2; 18.2%) or not always enough (n = 8; 72.7%). During the preceptorship period, NGNs were paired with an average of 4.3 preceptors (SD: 2.6), with a maximum of 12 different preceptors in 20 days. Nonetheless, most NGNs were either satisfied or very satisfied with their experiences during unit integration (n = 20; 69%), with very few dissatisfied or very dissatisfied (n = 4; 13.8%). Some commented that it would be better to pair with only one or two preceptors to ensure proper progression and follow-up of their development.
One NGN also felt that some preceptors did not have prior training to exercise their role, especially regarding how to provide feedback. This was corroborated by the survey in which approximately half of the preceptors in the sample did not receive any training (n = 5; 45.5%). Preceptors also did not feel supported in their roles (n = 6; 54.5%) and their patients’ assignments were not reduced (n = 11; 100%).
Autonomous Practice
Once the unit integration and preceptorship came to an end, NGNs began their autonomous practice for a probationary period whose length depended on their degree: NGNs holding a nursing degree from a CEGEP had an 80-day probationary period, whereas those with a BScN had 100 days, which roughly translates to working full-time for 5–6 months. Although most NGNs were satisfied (n = 17; 58.6%) or very satisfied (n = 5; 17.2%) with their probationary period, some expressed harsher words about its difficulty. Some felt that their patient assignments were heavier than when they were paired with the preceptor, and that there was no progression. Others mentioned that they did not feel supported or received feedback: I would have liked some feedback, but since I was on my own after four days, nobody could really evaluate my work. – Survey ID41 – NGN Once the ten days of unit integration are over (I asked for two more), we don’t really have any follow-up. – Survey ID40 - NGN
During this autonomous practice, NGNs’ competencies were evaluated at the midpoint and at the end of their probationary period using a standardized evaluation tool. The evaluation was performed by the unit or hierarchical manager if they were on a floating team. However, many NGNs mentioned that they did not receive this evaluation either at the midpoint (n = 12; 41.4%) or at the end of their probationary period (n = 17; 58.6%), with nine NGNs (31%) stating that they did not receive either: I had absolutely no meetings [with my manager]. I asked the person in charge of my unit and I could sense that it wasn’t a priority and that the person in charge didn’t want to know us as new nurse. – Survey ID27 - NGN
Others mentioned that even if the manager was responsible for the evaluation, they were not the ones observing NGNs, and they received contradictory feedback from different nurses during their probationary period, which was stressful: The evaluation process was adequate, but different nurses have different standards. Sometimes, one tells you are doing good and then another one tells you you are not doing the right thing, yet you are doing the exact same thing. It was very stressful. – Survey ID25 - NGN
During this period, NGNs could be asked to participate in mandatory training sessions, or were encouraged to participate in optional training sessions of their choice. Most NGNs (n = 20, 68.9%) did not participate in any training sessions, either mandatory or optional.
Additional Support Measures
Different measures were implemented to support NGNs, mostly during their autonomous practice periods; however, they could also be available to them during unit integration. As the interview participants mentioned, the different measures that addressed the different needs of NGNs could have the following: I think the support we provide to our recruits is “multimodal”: we have different measures or different focus to give them the support they need, a more comprehensive support. (Interview Participant E) With the nurse shortage, we can’t afford to lose them. This has led to a profound change in the organization, towards a learning organization. […] We try to develop each person's potential, because we believe that everyone has the potential to be who they want. (Interview Participant B) We offer personalized strategies to support them, depending on their integration. If I take, for example, someone who would have more difficulty with organizing and prioritizing, we can offer some coaching on the unit. But we can also organize coaching outside of the unit, like in the simulation lab. We offer it to everyone, when we organize simulation activities, but it can also be individualized. (Interview Participant D)
The additional support measures included:
General clinical support offered by the CNS assigned to the unit, who could help the NGN (or any other nurse) with any question relating to their work in the unit, including protocols and unit specialty. Technical support by a CNS specialized in psychomotor skills who could relieve the NGN from their patients’ assignment if they needed to practice specific skills, and proposed a practice session in a procedural laboratory or simulation center. Support from a mentor (a CNS specializing in mentorship), who could organize individual or group meetings or be reached using Facebook Messenger, based on the NGN's needs. All the NGNs were assigned mentors at the beginning of their employment. The mentor's helped NGNs develop their professional identity and think about their career trajectory. A licensure exam preparation course provided to every NGN who had not yet passed the exam, composed of online modules and an on-site workshop (with an additional workshop for NGNs retaking the exam).
These four measures were accessible to any NGN, but it is important to note that mentorship meetings and licensure exam preparation courses were to be conducted in the NGN's own time (unpaid), whereas the other two measures were conducted at work (paid). From the survey, it appears that most NGNs received general clinical support, but only a few times (n = 16; 55.2%), and approximately one-third said they did not receive any support (n = 10; 34.5%). Most did not receive any technical support (n = 16; 55.2%). Some NGNs expressed that they knew they could get this support but simply did not need it. Most NGNs knew that they had a mentor and communicated with them (n = 20; 69%), but they rarely met (M = 1.5 meetings; SD = 1.4) and only discussed a few times (n = 16; 80%). Almost all NGNs participated in the licensure exam preparation course either by completing both components (n = 11; 37.9%), online modules only (n = 4; 13.8%), or an on-site workshop only (n = 12; 41.4%).
Two additional measures were proposed for NGNs who struggled with integration. The first was a practice improvement workshop specifically designed to target a difficulty faced by NGNs. Managers were contacted to try to identify topics of interest, and NGNs could register at the workshop if they believed it to be beneficial to them. None of the survey respondents remembered participating in the practice improvement workshop. The second measure was more comprehensive and was actually a set of measures. Once an NGN was identified as having significant difficulties, they were individually supported by a CNS that specializes in integration. The CNS could review the NGN's development path to identify which measures or activities should be added or modified to ensure their successful integration. For example, it could be decided to ask another preceptor to supervise the NGN, change their unit assignment, add days to the preceptorship period, and so on. Overall, most NGNs were either very satisfied (n = 2; 6.9%) or satisfied (n = 18; 62.1%) with the different support measures offered by the partner organization.
Discussion
This study conducted a pre-implementation analysis of a residency program by constructing a preliminary logic model of the program that had already been implemented and assessing its operational fidelity. The results show that although many activities were implemented to support the transition of NGNs, their output was uncertain, their operationalization was not standardized, and no clear communication was made available to NGNs about all activities and measures implemented or how they could benefit from them. To discuss the findings, a comparative analysis of each activity was conducted in light of the literature, and more specifically, considering Chant and Westendorf (2019) framework of key components ensuring the sustainability of residency programs, namely : 1) strong foundation, 2) structured program, and 3) evaluation process. The results of the present study showed that the current program could be upgraded to a residency program if recommendations are implemented, which was performed in the subsequent phase.
Strong Foundation
The first theme from Chant and Westendorf (2019) framework is the foundation on which the program is built: organizational support, committed leadership, dedicated resources, and providing a healthy work environment. The findings of our study showed that when leadership was committed, there was a disconnect between higher decisions and day-to-day operations. As evidenced by the results, when there was a shortage of nurses in a specific shift, priority shifted from the NGN's personal development to the unit's needs. This made some NGNs feel like they were not respected as individuals; rather, they were simply a number within the organization. This echoes the study by Tuckett et al. (2015), in which nurses felt they were a “commodity” to managers. This study showed that nurse managers play an important role in nurses feeling supported, including NGNs. Our results showed a disconnect between committed leadership from higher management and how it translated to nurses; the missing link might be to ensure that unit managers have the latitude to help their teams.
According to Chant and Westendorf (2019) is the identification of a person or resource overseeing a program, which is essential for its sustainability. This resource not only coordinates but also facilitates teamwork to ensure program success. In a centralized healthcare organization, such as the one in this study, it is impossible for a single resource to have this responsibility, which is why a specific direction of nurses’ competency development was involved. While working as a team has benefits, it also presents the challenge of gathering a comprehensive overview of the transition program and all the activities implemented.
Structured Program
The second theme is the structure of the program, which comprises the framework on which it is built, defined outcomes, trained preceptors and mentors, didactic components, clinical immersion, and the duration of the program (Chant & Westendorf, 2019). In this study, the program was based on Duchscher's model of transition stages (Duchscher, 2008). This model established which support measures or activities are more relevant to NGNs depending on their stage. The program duration was 12 months, which was consistent with recommendations for having support measures for at least nine months (Rush et al., 2019). However, the results of this study showed that after the first few weeks, once the preceptorship period was over, most NGNs did not receive much support. They barely had contact with their mentors, and most did not reach the CNS for additional support. This may mean that they received support from their peers, as other studies have shown that nurses value their colleagues’ insight for their continuing professional development (King et al., 2021; Mlambo et al., 2021); however, other studies also shown that NGNs cannot receive the support they need from peers (Tuckett et al., 2015). This raises the question of whether NGNs received enough feedback during this period to properly identify their development, learning needs, and progress. It is not only a matter of receiving sufficient feedback, but also quality feedback.
Another key element related to the structure of the program is the need for dedicated preceptors, mentors, and their training to successfully play their roles. This study showed that although training was available and supposed to be mandatory, half of the preceptors were not trained, and they were often not told in advance that they would train someone. This finding is worrisome as other studies have pointed out that training preceptors is crucial if we want them to play their roles (Chan et al., 2019; McNeil & Jakubisin Konicki, 2021). The results also indicate that the preceptors in this study did not feel supported in their roles. This shows that learner progress was not really at the heart of the decision when pairing an NGN with a preceptor, and was sometimes more a question of meeting targets or fulfilling obligations. This did not align with recent literature that shows that preceptors need to be trained and supported, and that they need ongoing education opportunities (Smith et al., 2022).
On average, NGNs were paired with more than four preceptors, even though the pairing was supposed to be fixed or one-on-one. This is the most commonly found model in nursing (Ke et al., 2017). The literature is inconsistent regarding the stability required for the preceptorship period. There are benefits to being paired with different preceptors, as NGN have different styles and ways of working. However, studies have also shown that NGNs require stability, especially in the first few weeks and months of practice, to develop optimally (Charette et al., 2019a, 2019b). Stability does not mean NGNs should always be paired with one preceptor; rather that the pairing should be well thought out to match the needs of the NGN to the best preceptor, and that it should not simply be a matter of “who is available that day,” which was the case for some NGNs in this study. Acknowledging that the availability of preceptors is limited, collaborative models have emerged, such as co-precepting and team preceptorship, in which two or three preceptors work in teams to train two to three preceptees (Cooper Brathwaite & Lemonde, 2011; Ulrich et al., 2010). These models show benefits for both preceptors and preceptees; however, more studies are needed to compare this style with one-on-one preceptor models.
Participants’ characteristics.
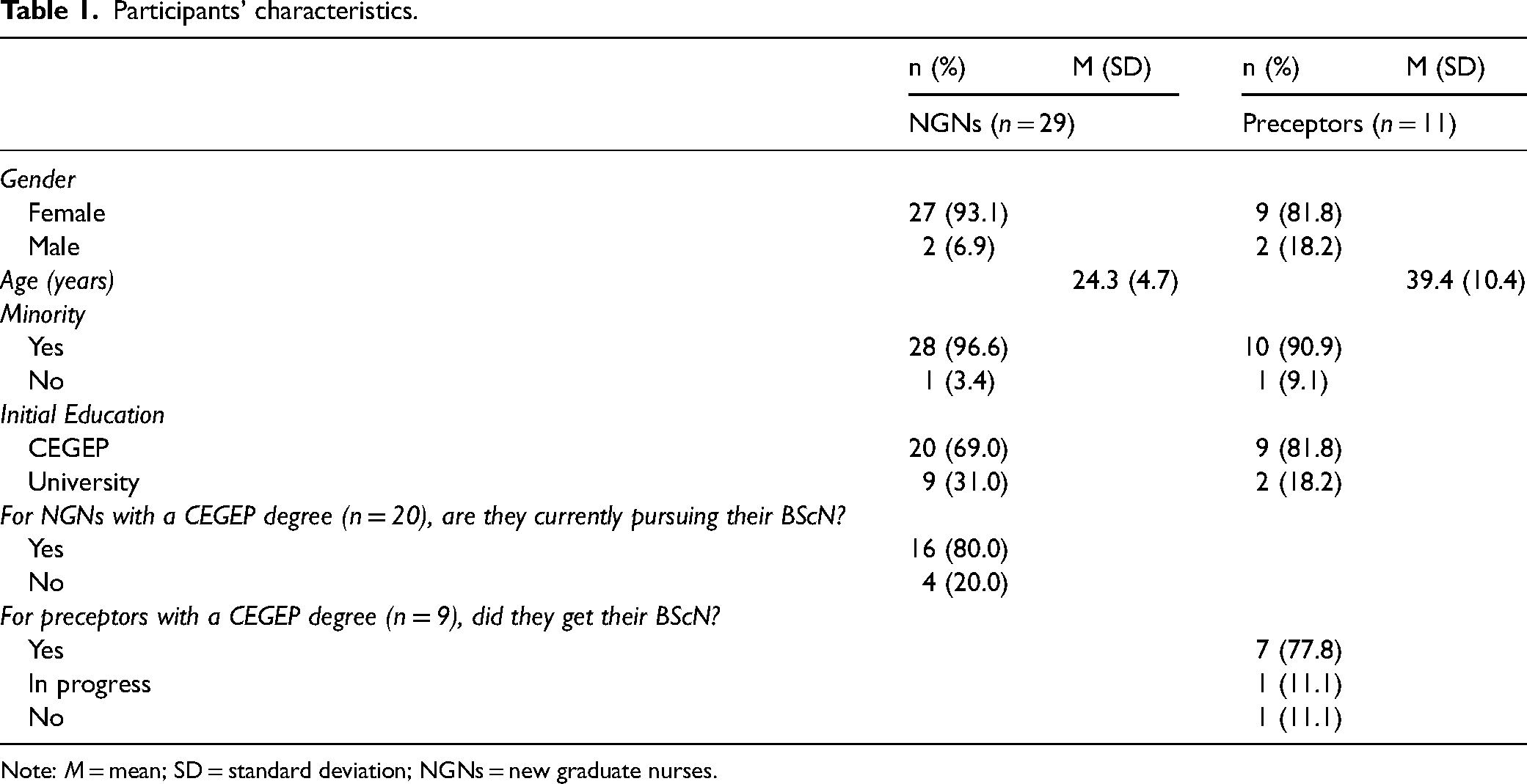
Note: M = mean; SD = standard deviation; NGNs = new graduate nurses.
According to Chant and Westendorf (2019), yet another key component of residency programs is the use of didactic sessions. Again, the literature is inconsistent regarding what is needed to offer optimal support for NGNs, but the integration of theory and practice through classroom activities, case studies, seminars, etc. has enhanced the progression of NGNs. These activities also help with peer socialization. In our study, apart from unit integration at the beginning of the program, more than two-thirds of the NGNs did not participate in any training sessions, either mandatory or optional. This is worrying and may reflect the difficulty nurses face in identifying opportunities for continuing professional development (Mlambo et al., 2021). This refers again to the fact that the NGNs in this study did not meet regularly with their mentors; without regular feedback, they were unable to identify their learning needs and did not reflect on their trajectories or development plans. Some studies have shown that there is no difference in the transition score for NGNs who have all their education at the beginning of integration compared to those who receive their education spread out across a year (Rush et al., 2019), although the relationship between educational components and their contribution to the transition experience of NGNs is limited. Nonetheless, Bakon et al. (2018) found that a plurality of learning methods positively influenced this transition. It also shows that NGNs who are encouraged to join ongoing training and skill development is a positive factor influencing continuing professional development in nurses (Mlambo et al., 2021).
Evaluation Process
The last theme from Chant and Westendorf (2019) framework is the program's evaluation process. Outcomes should be identified using measurable indicators to follow up on the attainment of these outcomes. The main outcome identified in our study was competency development with a rubric specific to the organization; however, as the results show, half of the evaluations were not conducted in the previous year. Thus, this indicator was not a reliable measure of the program's success.
Survey responses.
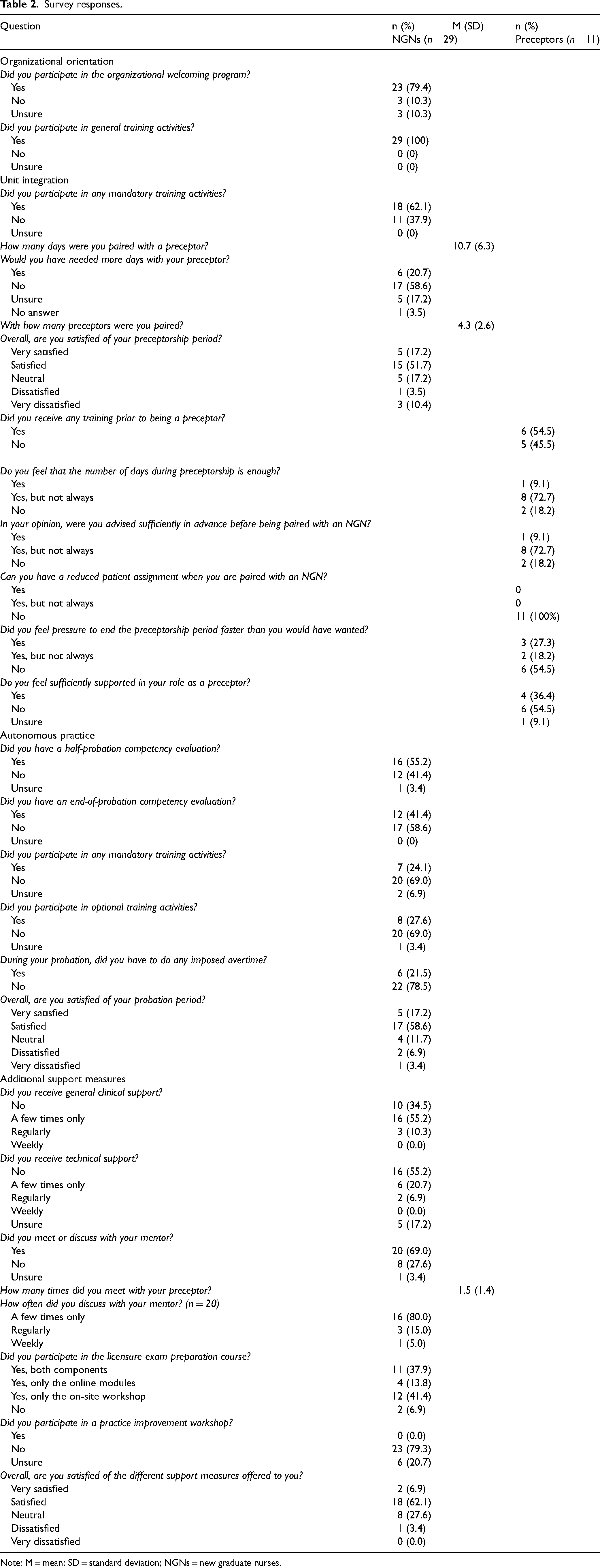
Note: M = mean; SD = standard deviation; NGNs = new graduate nurses.
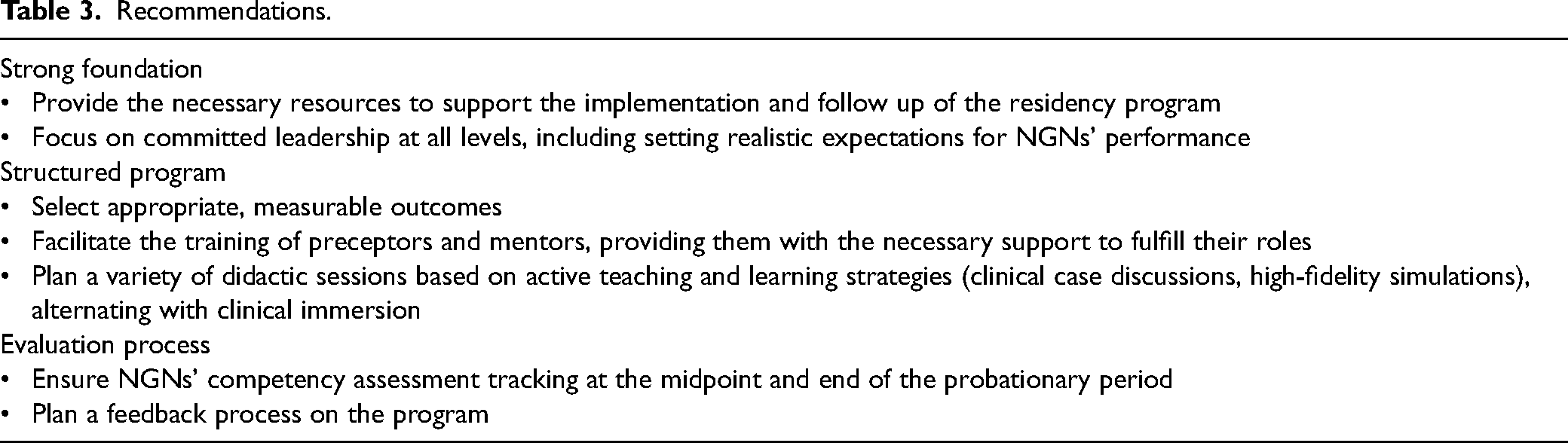
Finally, a pre-implementation analysis was performed as the first step in revising and upgrading the program to a residency program. Several recommendations were identified by comparing the current program with Chant and Westendorf (2019) framework, which also highlighted many activities that had already been implemented (see Table 3). The next step will be to implement the improved residency program as a pilot program in the selected units to assess its feasibility and acceptability.
Recommendations.
Limitations
The main limitation of this study is the difficulty in the transferability of the results, as they are the result of the analysis of a single transition program, and other organizations may have a different program. However, the method used in this study can be replicated to perform similar analyses. The second limitation concerns the availability of key actors and survey respondents in a context recognized as difficult in the healthcare network in the aftermath of the COVID-19 pandemic. The survey was pretested, which ensured face validity. While all NGNs and preceptors were invited to respond to the survey, very few did and their specific place of work was not collected. However, this study is important because the recommendations can support the clinical environment in improving the components of nursing residency programs, which may positively impact the transition of NGNs and increase their retention rates. Additionally, a social desirability bias may be present, especially when studying activities that have already been implemented. Participants who may have been involved in the development or implementation of the activities may not have attempted to embellish this process. To limit this bias, the participants’ confidentiality was ensured. Although member checking was not performed after Phase 1, the results have been presented and discussed with senior leadership of the office of the Director of Nursing.
Conclusion
In this study, we showed how transition programs already implemented in clinical settings can be enhanced into residency programs, which have a positive impact on the transition of NGNs, including their retention. We provided a framework to proceed with a pre-implementation analysis of a transition program, which is necessary to make significant improvements to said program. The findings from this study demonstrated a discrepancy between how a program is developed or thought and how it is operationalized. The results emphasize the need for continuing program evaluations, which is also consistent with Chant and Westendorf (2019) framework for the sustainability of residency programs.
Footnotes
Acknowledgments
Authors’ Contributions
All authors have made substantial contributions to conception and design of the study. MC, AR, JB and EQ made substantial contributions to acquisition of data and analysis. MC, IL and MEC made substantial contributions to analysis and interpretation of data. MC prepared the first draft of the manuscript which was critically revised by all authors. All authors have given their final approval of the published version.
Availability of Data
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by Université de Sherbrooke and from Équipe FUTUR (financed by the FRQ-SC); (Fonds de démarrage professoral).
Ethical Considerations
This study was done in two phases.
The Ethics Review Committee at CIUSSS de l’Estrie-CHUS approved Phase 1 (approval: 2022-4456), which included interviews, on December 7th, 2021. Respondents gave written consent for review and signature before starting interviews. The same Ethics Review Committee approved Phase 2 (approval #2024-5247) on February 7th, 2024. Participants to this anonymous survey had access to an inform consent before answering the survey, but signature was not necessary. Submission of the survey was deemed an implicit consent.
Consent to Participate
Respondents gave written consent for review and signature before starting interviews. Participants to this anonymous survey had access to an inform consent before answering the survey, but signature was not necessary. Submission of the survey was deemed an implicit consent.
Consent for Publication
Informed consent for publication was provided by participants.