
Abstract
Background
The aim of this study is to explore the practice experiences of new graduate nurses (NGNs) in publicly funded acute healthcare settings in the Greater Toronto Area, their perspectives on the determinants of their desire to stay or leave the nursing profession, and to identify action-oriented strategies to promote retention of NGNs.
Design
Qualitative, descriptive
Methods
Fifteen NGNs participated in focus group sessions, where a semi-structured interview guide was created to generate discussion on NGNs’ lived and professional experiences. We utilised the Social Ecological and Intersectionality frameworks to guide data analysis with an emphasis on social identities, power relationships, and the personal, interpersonal, organizational, and structural determinants of nursing retention.
Results
Participants contextualized their major challenges within four professional development phases: 1.) accessible nursing education and practicum placement; 2) preparedness, orientation and mentorship during entry to practice; 3) navigating transition to independent practice and multi-level structural violence; 3.1) retention strategies; and 4) perspectives on professional trajectory for NGNs.
Conclusion
NGNs experience major challenges throughout their nursing education and career. The study findings indicate that further research and systemic reform is essential to support, develop, and retain nursing leaders in the acute care setting. Furthermore, the findings can inform the development of evidence-based nursing curriculum reform.
Keywords
Introduction
The World Health Organization (WHO) reports that globally nurses make up the largest group of healthcare professionals with over 28 million nurses worldwide (Baumann & Crea-Arsenio, 2023). The human resources crisis in nursing has been a well-documented and known reality of the profession and workforce internationally (McClain et al., 2022). According to the International Council of Nurses (ICN), 13 million more nurses will be required to fill the current shortage over the next ten years (Baumann & Crea-Arsenio, 2023). Pre-COVID-19 pandemic forecasting models have predicted a shortage of more than 117,000 nurses in Canada by 2030, but this shortage is likely to increase exponentially due to heightened levels of nurse burnout, fatigue, and desire to leave the profession as a result of the working conditions during the COVID-19 pandemic (Baumann & Crea-Arsenio, 2023; McClain et al., 2022). Moreso, in 2022 reported there were ten practicing nurses per 1,000 people in Canada; comparatively, the United States averaged 12 (Canadian Federation of Nurses Union [CNFU], 2022; Statista, 2023). In the first quarter of 2023, the number of job vacancies for nurses increased by 5,475 positions, or 24%, to 28,335 from 2022 (Statistics Canada, 2023). Clearly the demand for nurses in the current labour market has outweighed the supply, further underscoring the chronic nursing shortage. Many high-income countries, including Canada, have responded to the nursing labour shortage by recruiting internationally educated nurses (IENs). The depletion of local labour shortages of nurses in low-income countries has sparked concerns from the ICN (2024). The ICN is encouraging high-income countries to be more self-reliant in creating an adequate nursing workforce with enough nurses to meet the needs of their respective populations (Baumann & Crea-Arsenio, 2023; ICN, 2024).
Although the healthcare sector is well aware that the chronic global nursing shortage predates the current nursing shortage crisis, this is lesser known in the general labour market (CNFU, 2022). Recognition in the general labour market is critical to increase funding, improve resource allocation, enhance public support for nurses, and to develop sustainable solutions. According to Baumann and Crea-Arsenio (2023), historically, the labour shortages in nursing were cyclical. Previous shortages were responded to through changes in policies to encourage both the integration of new nurses and retention of the existing nursing labour force. However, the current nursing shortage in Canada is the cumulative effects of many unresolved socio-economic-political events, including neoliberal austerity measures and labour restructuring initiatives which resulted in decreased patient care capacity and the potential displacement of thousands of healthcare workers during periods of fiscal restraint in the 1990's (Advisory Committee on Health Human Resources, 2000). Additionally, emergency unpreparedness during the SARS outbreak put nurses at risk of infection (Lam et al., 2020), which was repeated during the COVID-19 pandemic. The grueling working conditions and workforce pressures during the COVID-19 pandemic exacerbated the shortage of nurses (Aukerman et al., 2022; Baumann & Crea-Arsenio, 2023; Urban et al., 2022).
In response to the ICN recommendation of creating an internal adequate nursing workforce, the federal government in Canada has encouraged provinces to increase enrolment in nursing schools (College of Nurses of Ontario, 2022). On a provincial level, the Ontario Ministry of Health has incentivized employers to hire new graduate nurses (NGNs) through programs such as the New Graduate Guarantee (NGG) that recruit nurses immediately upon graduation (Ontario Health, 2024). However, due to the critical nursing labour shortage, several provinces in Canada have had to resort to actively recruiting nurses from the international labour market (Baumann & Crea-Arsenio, 2023). Despite this decision and action, job vacancies have not reduced in 2023 and only one-third (34%) of nurses indicated they were planning to stay at their current job for less than three years in 2021 (Statistics Canada, 2023).
While there is evidence to suggest that the COVID-19 pandemic may have galvanized many high school students to consider enrolment in nursing programs across the global community (Edmonson et al., 2022), student recruitment alone cannot address the nursing shortage. NGNs entering the nursing labour market accounted for only 8% of the increase in 2022 and 40% were IENs (Baumann & Crea-Arsenio, 2023). A critical question requiring urgent answers is – why are nurses leaving the profession in such high numbers? In Ontario, one third of registered nurses (RNs) who provide direct care to patients are 50 years of age or older and on the brink of choosing early retirement (Registered Nurses’ Association of Ontario, 2021). The Survey on Health Care Workers’ Experience During the Pandemic conducted from September to November 2021 highlighted the top three reasons nurses left their jobs. These included stress or burnout (55%), concerns about mental health and well-being (48%), and lack of job satisfaction (40%) (Statistics Canada, 2023). While considerable efforts and resources have been directed towards nursing recruitment, fewer efforts and resources have been directed to the retention of nurses (CNFU, 2022). Moreover, the cost of recruitment, orienting and professionally developing a newly hired nurse is twice the salary of a departing nurse (McClain et al., 2022), further demonstrating the importance of exploring strategies to prevent burnout and cultivate supportive environments that retain both seasoned and new graduate nurses (NGNs).
While studies have previously explored the experiences of mid and late career nurses, the experiences of NGNs in the current workforce are lacking (McClain et al., 2022). Considering NGNs are vital to sustain the healthcare system and ensure adequate patient care, understanding the practice experiences of NGNs as well as the motivators and drivers of their determinants to stay or leave the nursing profession will help with knowledge around retention of the NGN workforce to build a sustainable nursing workforce in Toronto, Canada. The aim of this study is to identify strategies that prevent burnout and massive resignation among NGNs (two to five years post-graduation). In this paper, we report on the results of this study including: 1) the practice experiences of NGNs in publicly funded healthcare settings in the Greater Toronto Area (GTA); and 2) NGNs’ perspectives on the personal, interpersonal, organizational, and structural determinants of their desire to stay or leave the nursing profession. We also offer action-oriented strategies that promote retention of NGNs.
Methods
This qualitative, exploratory, critical narrative study focused on NGNs’ professional experiences and perspectives on the multi-level determinants of nursing retention in Toronto, Canada. Focus groups were utilized to collect data versus individual interviews as the intention was for participants to recognize that they were not alone in their experiences as NGNs in the acute care system. Additionally, the intention was to provide space for elaboration by other participants on the various perspectives participants raised on the personal, interpersonal, organizational, and structural determinants of their desire to stay or leave the nursing profession. Such an approach could not be used with individual interviews (Guest et al., 2017).
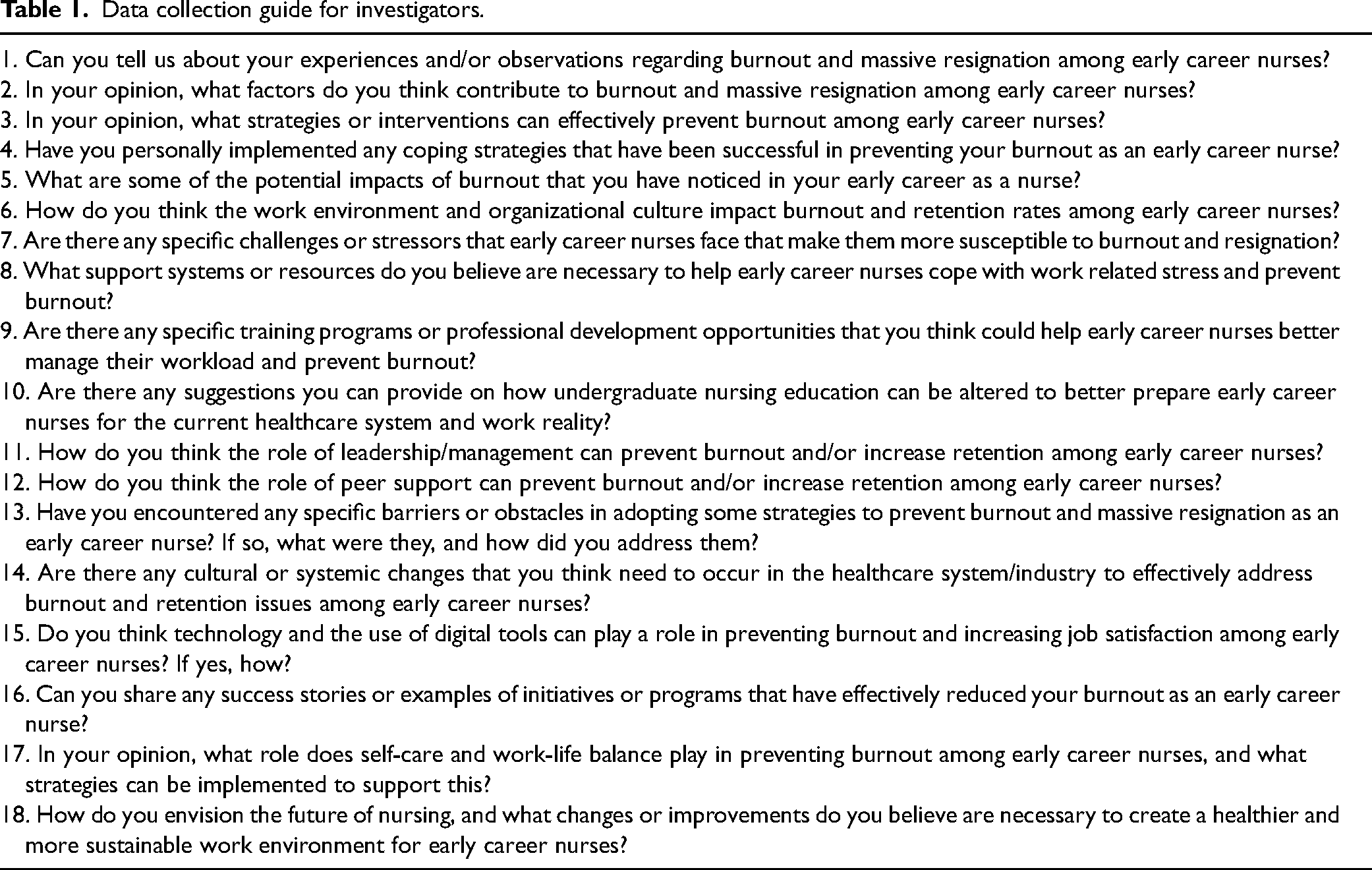
The study design was informed by the Social Ecological (SE) framework (Bronfenbrenner, 1979) and the Intersectionality (IS) framework (Carbado et al., 2013; Crenshaw, 2013). The SE framework provided structure to examine the practice experiences of NGNs at multiple levels: personal (social identity, experiences of health and wellbeing); interpersonal (relationships with patients, families, colleagues); organizational (workplace conditions, policies and resources); and structural (licensing and regulating nursing bodies, public policies, societal norms) (Sato et al., 2022). Specifically, the SE framework influenced the development of the data collection guide (see Table 1). Interview questions were structured to guide the direction of the focus groups, from discussions of the participants’ immediate stressors and workplace contexts to consideration of broader organizational and societal influences leading to burnout and massive resignation of NGNs (Bronfenbrenner, 1979; Sato et al., 2022). In compliment, the IS framework enabled us to explore how social identities like gender and class intersect with power relations to shape NGNs’ lived and professional experiences, and their perceptions of work satisfaction and quality. The IS framework provided a method and disposition towards the interpretation of findings, with specific attention paid towards the analysis of NGNs’ discourses of resistance to prevailing structures of power within nursing (Carbado et al., 2013; Crenshaw, 2013).
Data collection guide for investigators.
Recruitment
Approval was granted by the institutional Research Ethics Board (REB#2023–268). Participants were recruited through convenience and snowball sampling; e-flyers were distributed through professional and personal social media accounts of the study team members (i.e., Facebook, Twitter and LinkedIn) as well as posted on several social media group pages (i.e., the groups “Remote and Nontraditional Nursing Jobs Canada” and “Ontario Nursing Jobs” on Facebook). After viewing the e-flyer, participants contacted the Principal Investigator via email to express interest. Follow-up contact was initiated (via email) by a member of the research team whereby participants were asked to self-verify eligibility to participate based on the inclusion criteria, and presented with the attached consent form; at this time, they were also encouraged to ask any questions regarding the consent form and what their participation in this study entails. The inclusion criteria for this study were as follows: participants aged 22–35 years old, who have graduated from a Canadian school of nursing, written and passed their National Council Licensure Examination (NCLEX) within the last five years (2018–2023), and are currently working as an RN or registered practical nurse (RPN) in an acute healthcare institution in the Greater Toronto Area (GTA). The exclusion criteria included participants who graduated from schools of nursing outside of Canada, who wrote and passed their NCLEX licensing exam more than five years ago, and those who are not employed in a publicly-funded acute care setting in the GTA. The inclusion criteria for participant age were based upon a report published by the College of Nurses of Ontario (2022) which indicated a disproportionate loss of RNs and RPNs in the health care system aged 25 to 34, compared to previous years.
Data Collection
After informed consent was obtained, participants were invited to take part in a virtual focus group session hosted through a video conferencing platform (Zoom) based on their provided availability. In addition to self-verification of eligibility upon first contact with the research team, an individual screening was completed with each participant prior to the initiation of the focus group to ensure that inclusion criteria were met, and to collect demographic information. A semi-structured interview guide was created to generate discussion on NGNs’ lived and professional experiences in publicly funded acute care settings (see Table 1). Four focus groups were conducted between December 2023 and January 2024, with the Principal Investigator leading all of them for consistency; the research assistant was also present at each focus group for support with technology and note-taking. Each focus group session lasted between 60–90 min, with three to five participants per session. Audio-recordings of the focus groups were captured and subsequently transcribed. Ethical considerations including participant confidentiality were addressed. Participants were not obligated to turn on their videos during the focus groups, share any specific information about the geographic area/organization they work for, and were only referred to by their Participant number(s) for the duration of the session.
Data Analysis
Guided by the SE and IS frameworks, we applied an interpretive approach to thematic analysis (Braun & Clarke, 2022). We examined the practice experiences of NGNs at the personal, interpersonal, organizational, and structural levels. The SE and IS frameworks, in tandem, enabled our team to interpret how diverse contexts and conditions influence NGNs’ decisions to stay within —or leave— the nursing profession. To gain an enhanced understanding of participants’ perspectives, repeated readings of focus group transcripts were undertaken. The IS framework was mobilized within this stage to reveal and connect shared experiences of challenges for NGNs (Carbado et al., 2013). Thematic codes were identified and developed inductively and deductively. Interpretive rigor was maintained through this hybrid process by contextualizing the participants’ subjective context and perspectives using direct quotations within the findings to strengthen the face validity of data interpretation (Fereday & Muir-Cochrane, 2006). A collective confirmation of results was reached via multiple rounds of discussion with study team members to ensure comprehensive interpretation (Braun & Clarke, 2022). The researchers also demonstrated reflexivity through documentation in field notes throughout the data analysis process. A balance of perspectives was presented in the findings, demonstrating the diversity of participant voices within the study.
Findings
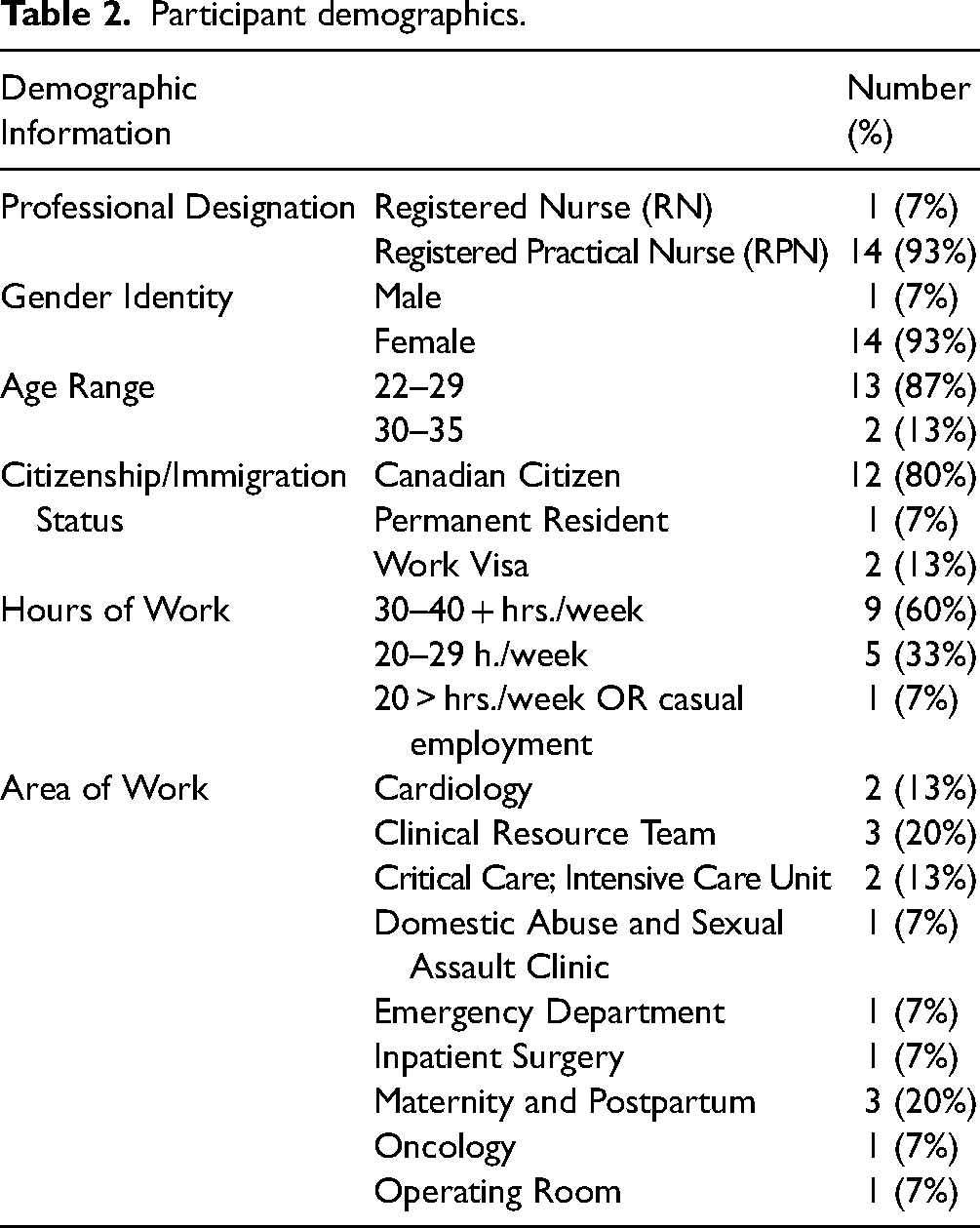
In total, the focus group sessions captured the lived experiences of 15 NGNs currently engaged in acute care nursing roles in the GTA. Participants included one RPN and 14 RNs, with ages ranging from 23 to 32 years old. Fourteen participants self-identified as female, and one as male. Nine participants reported working full-time hours (30–40 + hours per week), with six currently employed as part-time or casual status at their place of work. Detailed demographic information collected from the participants is available in Table 2.
Participant demographics.
Participants shared a wide breadth of perspectives regarding the current state of nursing education, clinical practice issues, and the future of the nursing workforce. The major themes and sub-themes which emerged from this study are identified and contextualized within four distinct professional developmental phases for NGNs: 1) Accessible Nursing Education and Practicum Placement; 2) Preparedness, Orientation and Mentorship during Entry to Practice; 3) Navigating Transition to Independent Practice and Multi-level Structural Violence; and 4) Perspectives on Professional Trajectory for NGNs. Additionally, COVID-19 related push-pull factors are highlighted within each theme. Participants’ individual and collective experiences are captured below and presented alongside illustrative quotes in participants’ own words.
Theme 1: Accessible Nursing Education and Practicum Placement
The participants cited several hurdles associated with completing their nursing education during the height of the COVID-19 pandemic. These organizational and structural challenges deeply affected NGNs’ personal feelings of readiness, serving as push factors to leave the profession before actually starting their career. Barriers included the loss of in-person acute care clinical practicum and preceptorship opportunities: P9: I actually graduated with an expedited preceptorship. So, I only graduated with 160 h instead of doing about 300. P8: I think one thing that would really help is nursing programs having better relationships and connections with acute care placements.
This finding highlights a significant discrepancy between outlined requirements in nursing education and the availability of resources necessary to support students’ clinical placements. Having their practicum hours reduced by nearly half, NGNs missed critical learning opportunities to refine their clinical judgment and skills under supervision: P12: For one whole semester during my fourth year, I actually had a virtual semester where we did simulations online. I didn't really feel like I learned a lot from that “placement”… I kind of felt like I started from nothing.
Further, participants questioned the adequacy of virtual placements vs. in-person learning. Limited exposure to patients and interdisciplinary teams negatively impacted the readiness and confidence of NGNs to navigate real-world healthcare settings.
When asked to discuss potential reasons for the nursing shortage, participants emphasized the academic requirements of nursing education as a prominent barrier to enter the profession: P2: Those second entry programs in Ontario… are extremely competitive to get into. I know a lot of fantastic people that applied and didn't get in. My class has 30 people in it… and so it's very limited.
The highly competitive acceptance rates of Canadian nursing education programs were mentioned by NGNs who completed direct entry nursing degrees, accelerated/second entry nursing programs, and RPN bridging programs.
Notably fewer participants shared about positive student experiences (pull factors) keeping them engaged and motivated: P23: For me, I did my consolidation where I'm working right now, so I felt like my student experience really had a big impact on why I'm still in nursing and why I decided to go back there.
Only one participant shared about a successful transition from their consolidation placement to their current workplace. They cited helpful colleagues, a supportive work environment, and an interesting patient population as interpersonal factors affecting their work satisfaction.
Theme 2: Preparedness, Orientation and Mentorship during Entry to Practice
NGNs frequently voiced inadequate or inconsistent training associated with the COVID-19 pandemic as push factors. Conversely, personal experience in healthcare, interpersonal relationships with experienced nurses, and organizational programs to support NGNs served as protective factors during entry to practice.
The most prominent issue raised by NGNs in this study was receiving inadequate or inconsistent orientation in their first acute care nursing position as RNs: P1: I've never had any sort of postpartum experience, so what they gave me was they gave me eight preceptor shifts…I didn't feel ready by the end of that. So, I was like, begging management, “Please, I just want a couple,” so they gave me 11 preceptor shifts in the end. This is when I started working full time in October. There was something about the orientation that they wanted us to start working on the floor earlier, and then we had the hospital and unit orientation after.
For NGNs working in specialized units without prior exposure, orientation shifts with an experienced nurse were an important steppingstone to independent nursing practice. NGNs described engaging in self-reflection and advocating for their learning needs as necessary actions to ensure patient safety. P12: I got a basic orientation, one that every new employee would get. And even that orientation, I got pulled off of it early, saying that I would get these orientation shifts back afterwards, we're just way too short right now… And fast forward, it's almost been three years, I've never gotten those orientation shifts. P3: I was ideally supposed to be with two different mentors…I actually ended up being paired with 20 different nurses altogether over three months…Especially as a new grad, I felt alone a lot of the time, I just had to figure out my own problems a lot.
Participants were forthcoming about the inconsistencies between the orientation experience that was promised to them and the reality that they received. In this study, feelings of isolation and being overwhelmed due to high patient workloads were frequently mentioned as contributors to burnout during this career stage.
However, some NGNs attributed an ease in transitioning to the role of an acute care nurse to additional work experience: P10: I would say I had a comparatively smooth onboarding compared to a new nurse who was freshly graduated working in a hospital setting…I felt that my previous experience as an RPN prepared me well. I'm not sure if I was somebody who just completed my four-year program and had the placements that are part of the program, I'm not sure how I would have handled that situation. P11: I knew what it would be like, even working as a [Personal Support Worker] PSW in university, so I was used to the 12 h [shifts] and the physical labour of nursing. But sometimes people don’t know that, and I think it is also because of certain placements.
When prompted to discuss positive experiences during the onboarding process, the majority of participants shared receiving support from their collaborative team members; specifically, clinical educators were identified as protective forces in the workplace: P13: There have been challenges —like transitioning in from being a student— but what really made it helpful was having a really supportive team. A team where I could go ask questions when I needed to, and I didn't feel intimidated to do that. P5: We did have a manager who was accusing [staff] of things before even speaking to them beforehand, but that clinical educator took on the protector role and was always trying to help new people in the unit. P2: The educators do need support as well; they are very overwhelmed. There's two of them for hundreds of nurses. They’re also in charge of all the onboarding and transitioning the new grads - which honestly was happening every three months. P1: Our unit did something called clinical scholar. We have so many new hires that need a lot more help and support throughout the day, right?… a senior staff that doesn't have any patients, but they're just there to support anyone that needs help. P9: One hospital had a specific educator that helped with orienting new grads, and another educator that helped with the general unit. I think separating those two would be very helpful, too.
Examples of successful workplace initiatives noted by NGNs frequently addressed the need for additional human resources and hands-on support tailored to new RNs. P2: I'm very thankful that I did the New [Graduate Guarantee] program. I honestly don't think I would have survived in [the emergency department] as a new grad nurse, had I not done that program. It gave us an extended orientation.
Ontario's NGG program, which provides newly graduated nurses with temporary full-time employment above staffing complement, was created to support the transition to practice with adequate workforce planning (Government of Ontario, 2024). Participants in the study who participated in the NGG praised the initiative as a key factor in a positive onboarding experience.
Theme 3: Early Independent Practice and Multi-level Structural Violence
The transition to independent practice during and immediately post COVID-19 was marked by push factors including the massive resignation of middle seniority staff, in addition to longstanding issues in nursing regarding heavy workloads, burnout, and understaffing. Participants also offered insights on pull factors, including interpersonal, organizational, and structural level strategies to improve staff wellbeing.
During the focus groups, participants pointed out that most of the nursing staff on their units were NGNs or RNs 30 years of age or younger: P2: Because a lot of senior nurses quit during the pandemic or moved to another area (such as public health), all of our staff were under the age of 30, pretty much, which is not a good thing in terms of safety for patients… [with one and a half years of experience] some nights, you're the most senior nurse, which is pretty scary.
In addition to filling staffing gaps meant for more experienced or senior RNs, NGNs also mentioned being put in roles like charge RN, or coordinator positions not typically offered to novice nurses due to a shortage in personnel. P5: We really don’t have any middle seniority staff. Like, those people that could become good mentors. We have staff that's awaiting their retirement, and they don’t want to take any additional roles, or we have people who just graduated [from] nursing school. P1: Traditionally, a lot of times, new grads would go into… float [nursing teams] or medicine-type of roles, and then transition to something more specialized. Then for my year -people who graduated in 2022- most of my friends just went directly into some sort of specialty. I was able to go straight into postpartum. A lot of my friends were like, going straight into ICU, that sort of thing. And that probably is only because COVID created those openings.
Participants attributed the mass resignation and migration of middle seniority and experienced RN staff to several factors, including burnout related to the context of the COVID-19 pandemic. A considerable number of NGNs in this study also identified burnout as a specific challenge for NGNs navigating the transition to independent nursing practice: P11: I believe it's all the burnout, just not only from COVID… I think it's just the dangerous working conditions, the heavy assignments, sometimes the lack of [personal protective equipment] PPE, which then spreads from the nurse to their family members when they go home, right?
Additionally, chronic understaffing and excess workloads were highlighted as probable antecedent factors to the nursing shortage in GTA, Canada: P15: I do think burnout plays a really big role in terms of the emotional turmoil of being separated and segregated from your friends and family during the pandemic… Burnout played a big role, I find, because of the increased workloads and frequent short staffing that contributes to it.
Themes of moral distress and hopelessness were reported as current work-related challenges faced by NGNs. They also identified new challenges associated with entering independent practice, including horizontal violence from colleagues: P15: Coming into the ICU, a lot of the more experienced nurses weren't welcoming, or they frequently talked behind your back. They would give you the toughest assignments to kind of let you gain experience, like trial through fire. And they kind of throw you in and they say, “Oh, like if you make it, you make it. If you don't, then you're not meant for the ICU”.
Gossiping, mean-spirited comments, and being talked about “behind your back” were cited as common examples of bullying in the workplace. P7: A lot of the older nurses kind of glorify how nursing used to be, versus what it is now. They say, “nursing used to be such a rewarding profession, a lot - a very respected profession.” I feel as though now, it's like, just everybody's so frustrated with the healthcare system that nurses are kind of the people that they target mainly and will say whatever to us.
P3: Sometimes there can be abuse: like verbal abuse, physical abuse, emotional abuse from patients or their families…sometimes it can just feel really isolating. Almost like, you feel really powerless.
While discussions of independent practice experience revealed many insights on issues negatively affecting NGN retention, participants also offered numerous suggestions, or pull factors, to help support nurses to stay in their acute care practice roles. On a systemic level, NGNs voiced that they believed mandatory RN to patient ratios were an effective strategy to address burnout and retention issues among NGNs: P2: I’m not sure…if it's even possible, but a cap on how many patients we can have? There's so many instances in the ER when we had way too many patients, and some days I thought, “man, my license is in jeopardy.” And there's literally nothing I can do about it, because we’re understaffed, the patients keep coming into the ER…it was a huge worry for all of us every time we went to work. P15: I think what you're talking about is mandated patient-to-nurse ratios. I think that would be kind of helpful, but also just… I think more research and publication in terms of nursing workload and just time management. I recently heard a presentation where it accumulated the amount of expected times for nursing tasks, and the tasks that we have within a 12-h day, we would have needed 18 h.
NGNs in this study pointed out a need for further extensive research into nursing workloads and expectations. They articulated that they frequently forgo their breaks during shifts to care for their patients’ needs to the best of their abilities, but commented that this practice is unsustainable: P15: I wasn't able to take my breaks, I was so busy… the pace at which we're going is not sustainable for us as nurses. Even working night shifts all the time, that is physically demanding, and documented to be detrimental. And so, a greater acknowledgment and work to prevent those very real health consequences is needed.
To mitigate the other outlined challenges, participants suggested specific ways for unit leadership to look after new staff: P13: More check-ins by the managers and educators: even during team huddles, just to ask us if there's any educational in-services that we need more on —for some specific topics— or how they could support us, to make the work feel better.
Participants also suggested strategies to support the wellbeing of now-practicing RNs in acute care settings: P15: Schedule flexibility is a really big one, especially for those with kids. There was a question about self-scheduling at one point in my ICU, however… as a less experienced nurse, you frequently get the bottom-of-the-barrel pickings for these kinds of things. It's the same thing with vacation as well.
Equitable opportunities for NGNs to engage in mental and physical respite were a popular request amongst the NGN participants in this study to improve workplace satisfaction on an individual level: P7: getting your vacation paid would be more rewarding to go to work rather than just, “Oh, I'm going into this toxic environment, can't wait for these 12 h to be done”.
Theme 4: Perspectives on Professional Trajectory for NGNs
This study also explored NGNs’ personal intentions to stay, or leave, the acute care or bedside setting in the future. While several participants discussed a desire to leave acute care nursing practice in pursuit of higher paying roles created by the demand of the COVID-19 pandemic, advanced nursing education, or different careers entirely, NGNs also noted pull factors like enhanced clinical leadership opportunities and additional supportive roles for experienced nurses as retention strategies to keep them engaged in acute care settings.
Participants expressed a generational shift in the traditional career trajectory for RNs: P15: Historically, there isn't very much career progression when it comes to being a nurse. You just go bedside and then you stay bedside for 20 or 30 years, and I think the new generation is realizing that you're physically tired, you're mentally tired, emotionally tired, and these things, whether you want to or not, it does bleed into your personal life and just there's very little work-life balance.
Some NGNs pursued professionally-related certifications and training to advance their skills within the nursing profession: P3: I got to do a lot of different courses offered through the hospital… ACLS, PALS, and some other courses that really helped, that I could use moving forward.
The participating NGNs also listed graduate degrees in Nursing, Public Health, Health Informatics, or Health Systems Leadership as popular choices for NGNs to advance their knowledge and skillset. Citing burnout, participants voiced that they personally intended to leave bedside practice after completing their graduate education: P1: Because I'm going to school, I'm not going to be in clinical practice - I'd just rather focus on school. So, I guess I'm going to be quitting clinical nursing… Probably not [returning to] bedside, I don’t think it's really for me.
However, they also considered pursuing non-healthcare related education, to work in another profession entirely. P3: I can save up and go back to school, and do a different Masters- just kind of, transition to a different career.
When asked to elaborate further on future plans, NGNs listed travel nursing and working for RN agencies as more favourable and lucrative options to working as bedside RNs: P12: A lot of [senior nursing staff] left for non-bedside nursing jobs… left for travel nursing, or for agency [positions], because they just don't want to work at our hospital anymore. P10: Nurses are still practicing as nurses, but they're not doing the traditional bedside role. So, I have friends who we all started with in the hospital, but as over time progressed, we've all moved on to a non-bedside role within an acute care facility.
Participants shared about their colleagues’ experiences of improved work-life balance, scheduling flexibility, and higher pay for similar work through these alternative avenues of RN employment. To retain NGNs in acute care nursing practice, participants proposed the following strategies: P15: I do recognize our clinical educators are quite underappreciated and understaffed as well. I feel like they need support as well; that also gives you a window of opportunity… some kind of a pathway for career progression.
Creating additional supportive roles for experienced and/or advanced practice RNs was suggested as a tool to encourage NGNs to stay engaged in the acute care setting: P5: I think that working in the ICU just gives me a lot of opportunities for the future and so this is the main reason why I'm still holding to that position. Definitely taking additional roles within my unit also helped a lot. Like, I became a part of the nursing practice council, so I got more into leadership positions, could run my own projects, and it helped to shift to focus a little bit…When you do one thing all the time, it can get kind of boring and stressful at the same time…I think that taking on additional educational roles helps a lot.
Some NGNs who expressed interest in continuing education were encouraged to stay in their acute care nursing roles due to clinical leadership opportunities in their workplaces, which were well-received. Lastly, participants named competitive compensation and benefits as a key strategy to retain RNs at the bedside: P10: I think financial incentives make a big difference; that is a major motivation for somebody to come into work. And we could see a huge decline in people picking up once they stopped offering the double pay. So, you know, like if we're looking at retaining our nurses and keeping them within the system, then we have to provide some financial incentives, and that would make a huge impact.
At a systemic level, participants also discussed the feasibility of privatization within the healthcare system as a potential solution to ease some burdens from the public healthcare system including long wait times and unit “gridlock” due to admission volume: P3: It seems like a lot of issues are due to so much demand and pressure on the healthcare system, like, you know, 10-h wait times in emerg, hospitals are gridlocked because of all the admissions, everyone stays in [the Emergency Department] for three days…I think a lot of people are afraid of the word privatization, but I think there's a way to do it, in some cases, where it actually would be helpful.
Discussion
This study aimed to examine the practice experiences of NGNs and their perspectives regarding the desire to stay or leave the profession, as well as their suggestions to promote the retention of NGNs within the nursing profession. The findings from this study contribute to the growing body of literature that explores the health of the Canadian nursing workforce (Baumann & Crea-Arsenio, 2023; Bourgeault, 2021). In the present study, NGNs discussed complex push-and-pull factors that affect their decision to continue caring for patients at the bedside including: the adequacy of nursing education and training, burnout, heavy workloads, and varied levels of support in the workplace. The experiences of these phenomena have been well-documented in previous studies of NGNs and their transition into independent practice, resulting in calls to action to create healthier and more sustainable workplaces (Catarelli et al., 2023; Hussein et al., 2017; McMillan et al., 2023).
Nursing education institutions hold great responsibility in preparing NGNs to enter practice with satisfactory nursing knowledge and critical decision-making skills. Chachula et al. (2015) studied eight Canadian NGNs who permanently exited the nursing profession within five years. The participants described that the process of letting go began when they were students and only intensified as they entered professional practice, citing poor working conditions, heavy patient workloads, hierarchical and horizontal violence (in nursing school and the workplace) as factors weighed in their decisions to leave the practice (Chachula et al., 2015). While the experiences and perspectives of NGNs in this study are uniquely affected by an unprecedented pandemic, we suggest that a partnered approach — which considers the student's self-assessment of knowledge — is warranted in the context of evaluating the adequacy of clinical practicum placements. NGNs in the present study shared candidly about their experiences of clinical practicum hours cut short and being required to perform skills or act in roles that were beyond their perceived capabilities or educational preparation. This is consistent with other recent Canadian research on NGNs who entered the profession during the COVID-19 pandemic. McMillan et al. (2023) study of eight NGN who entered the profession during the COVID-19 pandemic revealed that five participants had their final student consolidation placements fully canceled, while the remaining three participants’ placements were cut short. Similarly, Trepanier et al. (2024) and Smith et al. studied nurses who entered the profession during the COVID-19 pandemic in the United States. These NGNs reported significant disruptions to their learning, including the experience of having multiple preceptors during their residency programs and a desire for more “hands-on orientation time” (Trepanier et al., 2024). Therefore, clinical placement partners and coordinators should ensure frequent, regular check-ins with their students, and support them in advocating for their learning needs.
NGNs in this study also voiced several suggestions for employers to promote the wellbeing and retention of nurses within their acute care facilities, including balanced ways of working; self-scheduling, flexible rostering, and individualized orientation plans may be beneficial to support new nurses during this transition. Participants voiced the need for increased control over their work schedules, and a desire for flexibility that addresses their individual needs and lifestyle preferences. This aligns with previous research which highlighted the importance of work-life balance and autonomy for nursing students (Brook & Kemp, 2021). In a qualitative study of 13 nursing and midwifery students in England, Brook and Kemp (2021) explored the impact of a flexible rostering system for nursing students completing their clinical placements; students reported increased focus, reduced anxiety, and improved sleep when able to choose clinical shift days, shift length, and the number of clinical shifts per week. The findings also suggest that NGNs value accessible mental healthcare and wellbeing initiatives. In light of contextual stressors including entering the nursing profession during the COVID-19 pandemic, NGNs require meaningful support and mentorship from preceptors and unit leadership to thrive (Romano & Rodrigue, 2023). When this occurs, team cohesion improves, as Romano and Rodrigue (2023) found in a study of NGNs undergoing a revised orientation pathway on step-down and mixed surgical inpatient units. Organizational aspects, including comprehensive onboarding procedures, introductions to managers and co-workers, and building an understanding of facility policies, procedures, missions, and values (Hussein et al., 2017) were amongst the most frequently cited challenges by NGNs transitioning to independent nursing practice to lack of an adequate coaching period during the COVID-19 pandemic (Bani et al., 2023). Aukerman et al. (2022) employed an interpretative phenomenological approach to study the lived experiences of 12 NGNs in the United States who graduated during the COVID-19 pandemic and found that nurses expressed pride in their teamwork, profession, and personal resilience. This has important implications for unit staff and management to identify and empower emerging RN leaders to advance within the organization and role-model healthy workplace culture, with the intended outcome of improved retention of RN staff (Health Canada, 2024). Additionally, participants in the present study suggested that the opportunity to take on advanced educational roles kept them engaged in their acute care practice. We suggest that the integration of more leadership opportunities for experienced nurses, or the implementation of more advanced practice nursing roles may serve as a tool to help retain NGNs through the fulfillment of a desire for nurses to progress and utilize the full breadth of their knowledge, skills, and gained experience. This aligns with a study of the implementation of advanced practice nursing in Europe by Unsworth et al. (2022). In this study, key informants frequently cited a need for a professional career structure for nursing as the driver behind the development of advanced practice roles (Unsworth et al., 2022).
Implications
On an individual level, NGNs have a responsibility to mobilize and advocate for themselves as agents of change to address the nursing shortage. In this study, the participants have demonstrated a clear understanding of their needs and wants, as well as feasible recommendations to strengthen retention amongst nurses in acute care settings. Connecting with nursing organizations and lobbying groups should be a priority for NGNs to engage in political advocacy and voice their concerns. With the support of fellow nurses, nursing educators, and leadership, they have the opportunity to thrive and become leaders in their own right. NGN empowerment is critically important to the sustainability of the acute healthcare system.
Participants in this study were also asked to reflect upon how work-related challenges can be addressed from an organizational level. Findings revealed that NGNs require more support during transitions, consistent follow-up from clinical leadership, and meaningful opportunities to gain experience in their clinical practice. Nurse managers, educators, preceptors, and informal mentors should be aware of NGNs’ strengths and areas for improvement to assist with the integration of their new colleagues into the workplace. This knowledge can inform more effective human resources planning and management.
From a systems-level perspective, participants provided their thoughts on provincial policies and initiatives (including the NGG). User feedback should be considered by decision-makers to promote the retention of NGNs and make improvements to existing programming, while considering what new programming can be implemented for further support for this population.
Additionally, the study findings can also be used to inform the development of evidence-based nursing curriculum changes; specifically, NGNs shared that their clinical placement experiences were limited by pandemic measures, and that some did not feel adequately prepared to enter acute care nursing practice without relevant clinical experience in these settings. Nursing education institutions may benefit from strengthening relationships with community partners and teaching hospitals to create more diverse placement options for students. Future studies would also benefit from prompting explicit discussion of gender-, race-, and class-based inequities to further explore how these social identities shape NGNs’ lived and professional experiences in nursing practice.
Limitations
The study's sample presents a challenge to the transferability of findings because of it being represented by a group of nurses working in a specific healthcare setting in one of the largest cities in Canada. All participants were recruited from acute care institutions across the GTA, where a high concentration of teaching hospitals is located. However, our study did seek to capture experiences from a variety of care settings within these acute care organizations to allow for broader perspectives on widespread issues that impact NGNs.
Next, although the research team did not seek out equal representation of new graduate RNs and RPNs to participate, there was a disproportionate representation of new graduate RN experiences. Therefore, the findings from this study may not be fully applicable to RPNs or second-entry NGNs since their perspectives were not interpreted separately from the contributions of RNs. The results of this study can serve as a benchmark for future researchers to compare how different hospitals or settings impact the experiences of NGNs. Finally, through the lens of the IS framework, gender-based inequities in modern nursing practice and the undermining of labour rights and workplace safety through neoliberal policies are also a concern; however, these issues were not discussed during the present study's focus group.
Conclusion
This study examined a comprehensive exploration of the various challenges faced by New Graduate Nurses (NGNs) in publicly funded acute healthcare settings across the Greater Toronto Area (GTA), Canada and proposed actionable strategies focused on nursing education institutions and employer facilities to improve NGN retention within the nursing profession. The findings reveal that NGNs experience a series of critical challenges across various stages of their professional development. During their nursing education, inadequate practicum hours, especially during the COVID-19 pandemic, significantly obstruct clinical practice and skill development. As NGNs transition to their roles as RNs or RPNs in acute care settings, they encounter further obstacles due to insufficient or inconsistent orientation, unfamiliarity with specialized units, burnout from heavy workloads, and a lack of workplace support. The study further highlights the impact of the nursing shortage, which leads to excessive workloads and increases burnout, particularly during the COVID-19 pandemic. Additionally, facing violence from colleagues and patients contributes to mental health problems among NGNs. Addressing these issues requires ensuring equitable opportunities for mental and physical health support to improve workplace satisfaction and resilience. Furthermore, NGNs’ career development aspirations often lead them to seek further education in specialized fields or consider alternative career paths such as travel nursing or working for RN agencies. To support these transitions and retain NGNs within the profession, it is essential to forge educational development and advanced practice career opportunities within acute care.
Addressing these challenges necessitates collaborative efforts from nursing education institutions, healthcare organizations, and regulatory bodies to ensure resources, supportive orientation programs, and opportunities to advance their knowledge and skillset. This study offers valuable insights for policymakers, healthcare administrators, and educators to develop targeted interventions aimed at promoting NGN retention and well-being within the nursing profession.
Footnotes
Acknowledgements
This study was funded by the Social Sciences and Humanities Research Council Explore Grant.
Authors' Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada,