
Abstract
Background
Existing research highlights the role of social determinants of health, such as education and housing, in predicting health outcomes and the challenges that arise from deficiencies in these areas, often linked to societal inequities. Gender and income are recognized as social determinants of health, yet the complexities of their interplay, particularly for women with low income seeking health and social services in Canada, need more exploration.
Objective
This study investigates how gender and income intersect to affect access to health and social services for Canadian women with low income.
Methods
Employing a participatory action approach with arts-based and interpretive methodologies, the study partnered with a non-profit organization to engage five women through photovoice, interviews, and a focus group, aiming to capture their experiences in accessing services.
Results
The analysis revealed three primary themes: the labyrinth-like complexity of navigating health and social service systems, the importance of mental health sanctuaries, and the value of supportive networks. Participants reported difficulties and frustrations in system navigation, often feeling ignored by service providers. Contrarily, community agencies provided essential non-judgmental support, including daily necessities and emotional care, with the companionship of pets also being a notable source of comfort.
Conclusion
The findings advocate for a shift towards more person-centred care in health and social service systems to better serve women in vulnerable positions, emphasizing the need to simplify the process of accessing services and ensuring that service providers recognize and address the unique challenges faced by equity-deserving groups.
Poverty is the single largest global problem of epidemic proportions (United Nations [UN], 2020). Being in poverty is defined as a lack of the income and resources to support one's living (Organisation for Economic Co-operation and Development [OECD], 2023). Hunger and malnutrition, limited access to basic services (e.g., energy and electricity, education), social discrimination and exclusion, and the lack of opportunity to participate in decision-making regarding economic choices are consequences of poverty (UN, 2020). Based on the Canadian Income Survey 2021, the proportion of Canadians living on a low income was 7.4% (or 2,762,000) (Statistics Canada, 2023). Further, in regard to those in low income and gender, 7% (or 1,306,000) are males, and 7.7% (or 1,456,000) are females (Statistics Canada, 2023).
Women contribute significantly to Canadian society and the economy, yet are more vulnerable to certain poor social and health conditions than men (Fox & Moyser, 2018; Socías et al., 2016; Statistics Canada, 2021). As an example, it has been found that certain groups of women (Indigenous, visible minority women, immigrants, women with disabilities, single older women, single mothers, 2SLGTBQIA + members) face additional systemic barriers that prevent financial stability, putting them at higher risk of living in poverty than others (Canadian Women's Foundation [CWF], 2022). Notably, single mothers had the lowest average adjusted income ($25,300) of all population groups in 2016 (Fox & Moyser, 2018). Further, in 2018 (March 1 to April 30), 61 communities across Canada participated in a one-day accounting of those experiencing homelessness, and although the results revealed 36% of those 19,536 surveyed identified as female and 62% as male (Government of Canada, 2019), it is a number that is critiqued as a significant undercount (Schwan et al., 2020) and nevertheless worrisome. Collectively, these findings are important to appreciate, as researchers have identified socioeconomic class, access to social support, and employment among the most important contributors to women's decline in well-being and health status (Chan et al., 2018; Lombardo et al., 2014).
To date, researchers have described how women living on a low income obtain (or not) health and social services and the associated personal and system challenges in doing so (Chan et al., 2018; Socías et al., 2016). The challenges include cultural barriers and stigma associated with mental health and experiences of domestic violence, with implications to (ineffective) patterns of health and social service utilization (Ferrant, 2014; Lombardo et al., 2014). Although the work regarding health care utilization continues to grow, the gendered experiences of those living in poverty and their access to health and social services remains limited. Gender is defined as the socially constructed roles and attributes deemed appropriate by society for women, men, and gender-diverse individuals (Morgan et al., 2016; Tadiri et al., 2021; Tannenbaum et al., 2016). As a powerful social determinant of health, gender leads to power imbalances, differential access to resources in society, and varying social positions (Morgan et al., 2016; Tadiri et al., 2021). Gender can be thought of as four constructs: a) gender identity—encompassing how individuals perceive themselves and are perceived by others; b) gender roles—defining individuals in family, work, education, and social systems; c) gender relations—involving interactions based on gender; and d) institutionalized gender—referring to the distribution of power in political, educational, health, and social systems, which in turn shapes societal norms and opportunities (Tadiri et al., 2021; Tannenbaum et al., 2016). It is crucial to examine the ways in which gender and income status influence and perpetuate social and health inequities for equity-deserving groups, as only then can we extend our understanding of how all Canadians can thrive in a rapidly evolving and shifting world. As such, research to explore women's experiences of access to health and social services associated with gender and income inequities is urgently needed. Our study addresses that crucial knowledge gap by describing the ways in which women living on a low income constructed and explained their experiences of accessing health and social services.
In two previous publications, we presented components of this work (Camargo-Plazas et al., 2022b; Waite et al., 2022). In the first publication, we completed an in-depth exploration of the initial one-to-one interviews to present the burdens of economic hardships, lack of understanding from health and social service providers, and the need for—and right to—dignity (Camargo-Plazas et al., 2022b). In the second publication, we articulated our participants’ views on their understanding of systemic barriers in accessing health and social services, as well as described their unwavering resilience and determination in overcoming adversity (Waite et al., 2022). Informed by these foundational, complementary findings, in this current paper we aim to further the discourse. Intent on broadening the analytical scope, we integrate the dense data from multiple sources tied to the same five women who participated in this study, amalgamating additional insights from follow-up interviews, photovoice data, and focus group reflections. This rigorous approach aspires to spotlight previously uncharted and non-disseminated themes, thereby making additional contribution to the understanding of the women's interactions with the health care and social systems. The findings reported herein, while unveiling novel themes, do not seek to eclipse the narratives in the preceding studies. Rather, we endeavour to uniquely contribute to the academic discourse, presenting additional nuanced layers to this profound societal issue. In so doing, the intricate, critical interplay of gender and income as determinants of health care access becomes evermore clear. This clarity includes gender as an essential dimension in addressing health and social inequities. These important findings will improve our understanding and ability to develop stronger practical, real-world strategies in support of this population. As such, in this paper, we offer additional findings from our qualitative participatory study aimed at understanding the experiences of access to health and social services for women living on a low income in Kingston.
The social determinants of health framework
We followed Loppie-Reading and Wien's (2013) conceptual framework, which classifies the social determinants of health into distal (e.g., historical, political, social, and economic contexts), intermediate (e.g., community infrastructure, resources, systems, and capacities), and proximal (e.g., health behaviours, physical and social environment) categories. We have used this framework successfully to explore diverse experiences of health and social inequities in other equity-deserving groups, such as the experience of diabetes self-management education for older persons in a rural setting (Camargo-Plazas et al., 2022a; Robertson et al., 2023). This conceptual framework guided our thematic analysis of the data and provided a more comprehensive understanding of social inequities for women living on a low income in the city of Kingston.
Methodology and methods
Our study followed participatory action research (PAR), arts-based research, and interpretive approaches to accessing health and social services in Kingston. PAR is a collaborative approach, in which the research process follows an equitable partnership between academic researchers and community stakeholders (Oetzel et al., 2018). Through PAR, community members, organizational representatives, and researchers work together to devise research questions, conduct the research, and mobilize findings (Oetzel et al., 2018). As researchers using PAR, we brought together and partnered with women and community members to address the unequal distribution of social determinants (e.g., income, access, and gender) that contribute to women's health and social inequities. Art-based research is a research methodology using artistic processes—artistic expressions encompassing all artistic forms—as a primary source to explore, understand, represent, and even challenge human action and experience (Wang et al., 2017). We used art-based research (photovoice) to explore the experiences of access to health and social services for women who were economically distressed to generate critical consciousness and social change. Additionally, our PAR approach included establishing an advisory committee to oversee the research process. This committee ensured the voice of women living on low income was central to all aspects of the research process, facilitating the generation of relevant knowledge for the target population. During the COVID-19 pandemic, our advisory committee recommended transitioning from in-person activities to telephone (primarily) or online interviews. As the restrictions were eased, we conducted our focus group activity at Saint Vincent de Paul Society of Kingston following required masking and distancing protocols. Those experiences, coupled with further conversations with members of the advisory committee, engaged us in self-reflection and dialogue about poverty and the heightened effects of the pandemic on women living on a low income in Kingston. They enabled us, as employed women, nurses, and researchers, to reflect on and acknowledge our own assumptions, values, and pre-understandings transcending our positions of privilege. It was a truly eye-opening journey that frankly uncovered the realities of poverty and access issues—real, not in some distant place, but right within the confines of our own city.
Setting and participants
Our community partner, the Saint Vincent de Paul Society of Kingston, is a non-profit organization offering assistance and support to individuals and families in need living in Kingston through three different programs: 1) The Saint Vincent de Paul Society of Kingston Loretta Hospitality and Meal Program offers a hot meal 5 days a week, year-round; 2) The Emergency Food Pantry program provides 2 days of food per month to individuals and families; and 3) The WearHouse program provides gently-used clothing, books, and small household items (Saint Vincent de Paul Society [SVDP], 2020).
Our study's recruitment strategy was carefully developed. We introduced potential participants to the study via PowerPoint or video presentations, accompanied by a study folder with the Letter of Information (LOI) and a Consent Form. The social worker at Saint Vincent de Paul Society of Kingston gathered contact details of interested women, which were then passed to our research team. Team members contacted these women by phone to discuss the study details, the LOI, and the Consent Form and to answer any questions. Interested participants gave their verbal informed consent, which was recorded in the Verbal Consent Log.
Participants were selected through purposive sampling. Eligibility criteria included women who were 18 years or older, received services from the Saint Vincent de Paul Society of Kingston, and self-reported as living on a low income. Our study involved five volunteers aged between 38 and 65 years, with a mean age of 53.4 years. To ensure confidentiality, pseudonyms were used throughout. Of these participants, only Gina (65 years) was married. Claudia (45 years) and Jane (62 years) were single, and Margaret (38 years) was a single mother. Four of the women—Margaret, Claudia, Elizabeth, and Jane—were beneficiaries of the Ontario Disability Support Program (ODSP), with Gina, being married, ineligible for ODSP.
Data collection
Our data collection methods encompassed follow-up individual interviews, photovoice, and a focus group activity, each meticulously designated to facilitate nuanced exploration and profound reflection on participants’ experiences (Liebenberg, 2018). Photovoice, a participatory research method, was used to capture intricate, non-verbal aspects of their experiences that conventional research approaches may overlook (Wang & Burris, 1997). We provided participants with iPads® or disposable cameras for documenting representative images illustrating their experiences of accessing health and social services. The participants selected five photographs for discussion during the individual interviews and focus group activity. Each participant was invited to two interviews (audio-recorded) by phone/online due to COVID-19 restrictions. Two in-depth interviews were conducted with each participant. The first open-ended interview lasted 40–60 min and explored broad experiences and attitudes. The second interview lasted approximately 30 min and focused on gaining deeper insights into previously expressed views and emotions. The two-stage approach yielded rich, detailed qualitative data.
Following COVID-19 protocols, we organized and completed a two-hour in-person focus group session with the five participants, during which we explored their chosen five photographs and the emerging general themes from their individual interviews. We used the Otter.ai® software to transcribe the audio-recorded interviews and focus group, and three researchers independently proofread the transcripts. Ethics approval was secured from Queen's University, General Research Ethics Board (TRAQ# 6024959). We followed the ethical principles of conducting research with human beings as outlined by the Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council (2018). A more detailed account of the characteristics of participants, data collection, and trustworthiness of the study, with a detailed account of our data analysis process, has been documented in our earlier publications (Camargo-Plazas et al., 2022b; Waite et al., 2022).
Data analysis
Our data analysis process, which encompassed the examination of follow-up individual participant interviews, photographs (photos) taken by participants (which included a brief descriptor/statement created by participants for each photo [photo-text]), and focus group discussion, adhered to the thematic analysis approach outlined by van Manen's (2016) thematic analysis, and it was guided by Loppie-Reading and Wein's (2013) social determinants of health framework. The process of analysis involved several iterative stages: a) an initial comprehensive review of the transcripts to capture the fundamental essence of the text; b) the identification of specific phrases that held particular relevance in conveying the experiences of women on a low income in their pursuit of access to health and social services; and c) a granular examination of the data, sentence by sentence to discern and delineate emerging themes. Furthermore, we conducted extensive iterations of writing and rewriting to effectively communicate the thematic analysis of essences (van Manen, 2016).
Throughout the study, several measures were implemented to enhance trustworthiness. For instance, to verify accuracy, three research team members cross-referenced all verbatim transcripts with the recordings. Analysis meetings were regularly conducted to ensure the identified themes accurately reflected the participants’ accounts and photographs. The core research team meticulously reviewed all data to confirm that our interpretations were directly linked to the collected data. We maintained a detailed log of our decisions and convened bi-weekly throughout the project's duration. While we did not keep a reflexive journal, our meetings with the advisory committee and core team meetings provided an opportunity to share our feelings, emotions, and thoughts about the research process. This practice was crucial in ensuring we did not suffer secondary trauma from the compelling stories shared by our research participants, fostering a culture of collective reflection. Notably, due to pandemic restrictions and constraints, community participants were not involved in the data collection and analysis.
Results
In complement to our previous findings as reported in the literature, and based on this additional analysis of the culmination of the follow-up individual interview transcripts, photos/photo-texts, and focus group activity, three new themes have been illuminated: (a) The Maze—Navigating the Health and Social Systems; (b) My Special Space—Mental Health; and (c) They Help You So Much—Support System.
The maze—navigating the health and social systems
The participants compared navigating the health and social systems to the frustration of negotiating a (unnecessarily) complex maze (Figure 1). Margaret is a single mother of a child with a disability. Her photographs highlight the problem of finding her way through the health and social systems; the maze image is reflective of her experiences. Maneuvering through a maze entails facing obstacles and challenges that can complicate reaching the desired outcome. Navigating services while parenting a child with severe autism can be overwhelming and can include completely losing one's way. Margaret explained, “It is a maze…You’re lost, and you think you’re going the right way. And then you keep coming into that same roadblock. Two and a half years later, my [child] still has not received services. The system is failing.” Margaret's story highlighted the challenges faced by single mothers who bear the dual responsibility of caregiving and navigating complex systems like health care and social systems. Furthermore, living on a low income and inadequate support networks intensify these challenges.

Navigating the health and social systems.
Claudia, a single woman, resonated with Margaret's image, saying, “When you go to a maze, you’re just confused, and you’re lost and, and you’re like, going – being upset because, okay, there's the starting point, but where's the ending point?” The participants believed their socioeconomic status heightened the roadblocks in the convoluted systems, and they often encountered barriers that required them to retrace their steps and try different paths. Claudia shared an experience about learning from a friend that bus passes were offered for Kingston beneficiaries; she expressed her irritation, saying, “I knew no – [expletive] about it. They said, ‘You can go to [name of place] and get a lifetime bus pass.’ Nobody said anything. Nobody brought it to my attention.” The participants’ stories exposed the obstacles that prevented them from accessing essential services for themselves and their families. Nevertheless, these women navigated these challenges with resiliency—phrasing we have chosen to use in support of a ‘rebalancing of power’ (National Collaborating Centre for Determinants of Health, 2023).
Another common experience of the participants was dismissal by health and social service providers. Some women in the study found this response exhausting and disheartening. Margaret depicted this experience by photographing a teddy bear, mouth tapped (Figure 1). The participants felt dismissed, invalidated, and ignored when service providers failed to hear them. Margaret recalled: I just had surgery 2 weeks ago. I’ve been waiting for like 10 years for this. It was a lot of – yes, it is a hernia. No, it's not. We can’t find it. I felt like I was going crazy. I was in pain. Nobody would listen.
Similarly, Jane, a single woman diagnosed with cancer, remembered her experience with a family physician: I go in there and tell him that I’ve got a problem that pops—something popped in my sternum. He said, ‘It's just an inflamed sternum. It’ll go away in 3 months.’ And this was maybe a little over 3 years ago. He just would not listen to me.
Participants highlighted the importance of health care providers listening to patients and emphasized the criticality of recognizing and respecting individual needs and preferences, regardless of age, gender, or sexual orientation. The participants shared these photographs with the main message their struggles must be addressed and not overlooked. Receiving token attention—which they easily discerned—is disrespectful, demeaning, leads to further social isolation and is not a long-term solution. Regardless of their (or anyone's) situation, women deserve to feel they have been heard and worthy of the services they require.
My special place—mental health
Living on a low income created many barriers and struggles for the participants. Gina recalled, “Some people think I don’t have depression. I do. My face [doesn’t show] how much I suffer.” A cancer diagnosis can be an overwhelming and life-changing experience. Spending alone time in her backyard was therapeutic and calming, conceivably a time for reflection and processing her feelings and emotions. For other participants, experiencing isolation and depression were particularly difficult. As Margaret recounted, “Autism is isolating. I don’t have any friends with kids on the spectrum. I have friends that will be a friend only if my child's gone. We’re a package deal. It's beyond isolating.” Despite these trying experiences, participants persisted, which Margaret described as follows: “I’m never giving up—like we will fight. There's a sign in my house that says in this home, or in this house—we do autism” (Figure 2).

Strategies to maintain mental health.
The mental health struggles faced by Gina and Margaret offered a poignant glimpse into the unique impact of societal and familial roles on women's mental health. For instance, Gina's experiences revealed the stress and emotional burden of traditional expectations of womanhood and caregiving. Margaret's situation highlights the intensified pressure on single mothers who juggle multiple roles. Consequently, the participants developed strategies for overcoming their adversities. Their photographs portray these strategies, revealing how they protect their mental health, maintain companionship, and embrace advocacy. Gina shared photographs of locations that bring her peace (Figure 2). For example, she captioned a photograph of her home as “My castle” and affirmed, At summertime, I spend a lot of time outside—the trees shade the sun, so it is Perfect. The leaves are beautiful, and the birds are plentiful—and they sing. Outside all day. This is how I take care of my mental health.
Several of Elizabeth's photographs captured her strategies for improving her mental well-being. She described a photograph of a tugboat (Figure 2), saying: That was one of my days where I was feeling cooped up. And I just sat there and saw the most amazing clouds and the view and the boat. It was amazing to watch. And it just calmed me down. It was like the busy, hectic world was gone.
Additional strategies Elizabeth mentioned for improving her mental health included going to the park and feeding the birds: I’m a bit of a hermit. I normally stayed in the house…a lot of time. And my friend helped me go to the park, and I became healthier. You know, and it gives me a good spirit…and there is entertainment with the birds.
They help you so much—support system
Within this theme, the women shared photographs representing their need to feel safe and valued in their environment. Their photographs illustrated how they created spaces they wanted to live in by helping others, giving back, avoiding judgement, and caring for their companions, including pets. During the focus group, Elizabeth showed the group a photograph of Saint Vincent de Paul. She discussed how it provided her a hot meal, but so much more than that, including emotional support, clothing, and guidance on accessing other community resources when needed. Gina agreed, sharing her experience receiving help, such as pads for bladder control, food, and clothes. The conversation continued as follows: Elizabeth: Today, I went and got my lunch from Saint Vincent de Paul. And I'm gonna have it for supper tonight. I’ve got my boots here. I got a jacket from here. I got emotional help when I was in trouble. I got directions. Anytime I need something, I can always talk to any of the ladies here. Gina: That's why I call it family. They help you so much. Like today, I'm gonna have diapers for bladder control. Elizabeth: And you know what they don't ask you for your income.
Elizabeth and Gina's exchange sheds light on the value of Saint Vincent de Paul in their lives (Figure 2). Elizabeth stressed Saint Vincent de Paul does not discriminate based on income. Overall, the participants’ dialogue highlighted the significance of community agencies in supplying not only material resources, but sometimes more importantly, emotional support and a sense of belonging for those who may be at a more vulnerable point in their life. Gina said: When I'm depressed. [name of the person] knows. Cuz [she] keeps saying, ‘If you like that, you come over.’ That's why I come too many times. Not because I need stuff [but] because if you [need to] talk to somebody, they're gonna listen to you.
The participants, who struggled every month to make ends meet, deeply appreciated the assistance of staff at Saint Vincent de Paul Society of Kingston and the local food banks in Kingston. They detailed the challenges of living on a limited income and budgeting for basic needs. The following is the dialogue between Jane and Margaret about Saint Vincent de Paul Society of Kingston support: Jane: I have to do without a whole heck of a lot just to have a roof over my head. And uh, that's just not right for anybody who needs assistance or help. Margaret: They don't give us basic needs for our children. Nobody gets basic needs for their kids anymore. You get shelter. That's it… As a single parent, you get a little bit more for basic needs, but it's not like, ah, common-law partner. Even that gets more, yeah.
The participants also described pets as a special source of strength and company. Pets provide emotional companionship, unconditional love, and a sense of purpose that can be difficult to find elsewhere. Even when staying in the emergency shelter, Claudia never abandoned her cat (Figure 3). Her cat, as pictured in a photograph, was her reason for waking up each day. While she “hoped” for reassurance she might meet her basic needs, the reliance on and relationship with her cat gave her hope to persevere. Claudia became emotional when explaining her love for her cat, Jess, that had been with her since kittenhood: “I just don’t know where I’d be without my animals.” According to Claudia, Jess had accompanied her and helped her cope with two failed marriages, stress, diabetes, and depression; she elaborated:
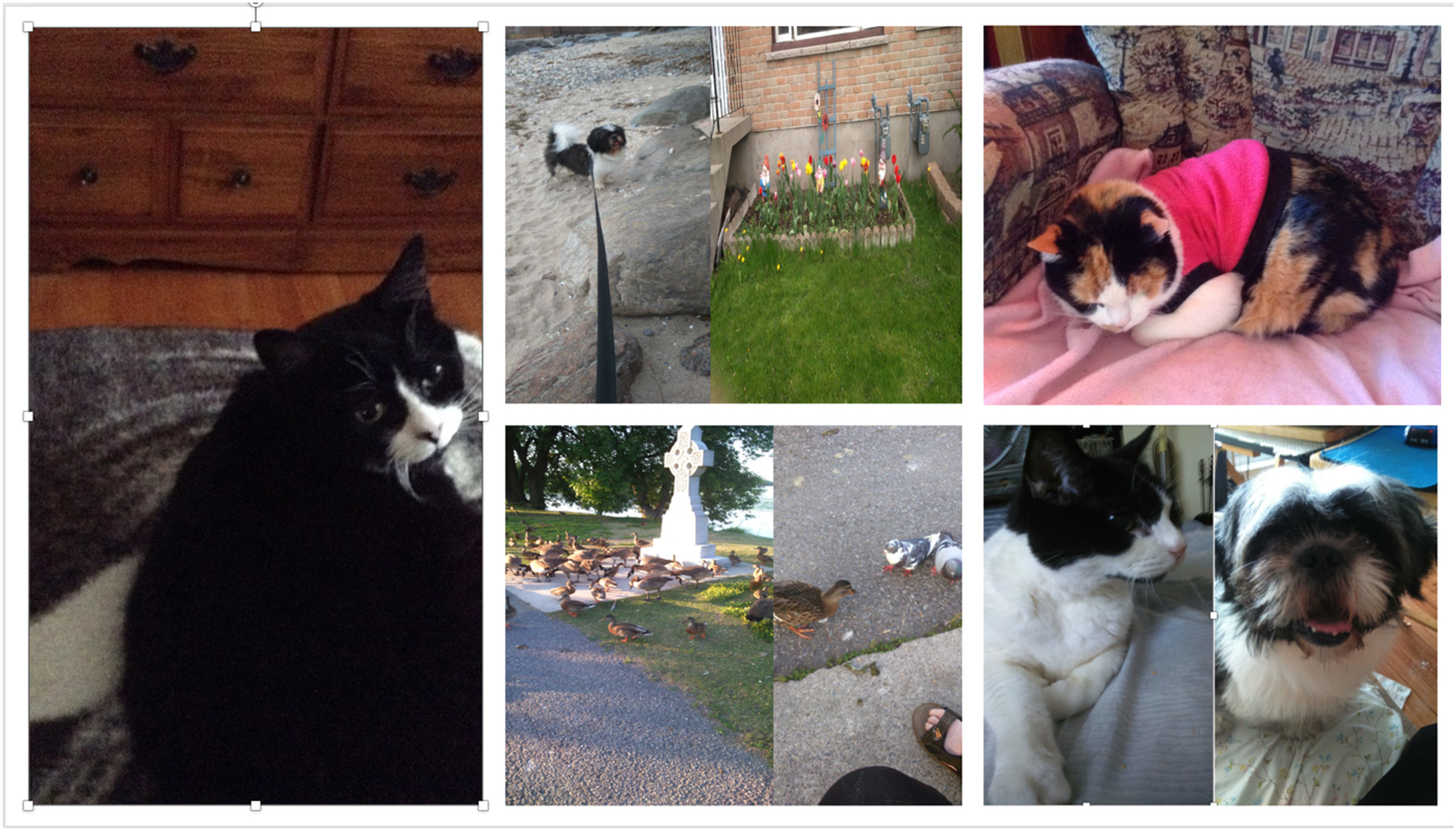
They help you so much.
Jess was my support system [participant crying]. And she was all I could count on it when I had suicidal thoughts. I’m diabetic. I have depression. I have anxiety, and she's my support system. And she was there when nobody else would be. Thus, Jess alleviated Claudia's depression and suicidal thoughts.
Claudia further added, “My life revolves around [Jess], and she is like everything. When I come home from anywhere, she's right at the door. So, she's my support system. I can’t imagine my life without her. She's everything that I ever imagined.”
Similarly, Elizabeth brought photographs of her dog Sasha and cat Mia (Figure 3). She shared with us the story of a previous stray cat she took in, now deceased, depicting the strong sense of companionship she has with her pets. She also described her thankfulness for her health care resources that help her continue caring for her pets. When asked how the images relate to her experience of accessing health and social services, she responded: “I’m a mother to these animals. Sasha, he's my baby, you know, and if it wasn’t for the people in the health care helping me, I wouldn’t be a good mother to them.” For Elizabeth, pets were family, and she was like their mother. She talked about going to great lengths to ensure the health and well-being of her furry companions, treating them as she would any other family member. Elizabeth said: It helps you through the hard times, too; I’m always constantly alone. Having Sasha, I know Mia is now deceased since August. Having Sasha is a wonderful thing. Even though I used to have Mia, I miss her to pieces. But she lived a full life.
Sasha, Mia, and Jess filled a void, providing Elizabeth and Claudia with a unique sense of purpose and belonging. Pets brought participants joy and enriched their lives, creating a special and unique relationship. Nevertheless, Elizabeth described being criticized by a social worker for having pets; she recalled: I got a lot of grief from the social worker about getting Sasha because you have to pay for vet bills and stuff. It's another burden on my budget. But he gives me so much back in the long run and keeps me going.
Discussion
In this study, and the supplementary analyses, we addressed limitations in evidence about access to health and social services from the perspective of women who are economically challenged, and it illustrates how stories can serve as means to enhance one's understanding of phenomena on a deeper level. To our knowledge, it is one of the first to focus on understanding access to health and social services by women on a low income and provides significant insights into their experiences navigating often-non-friendly service systems. Our work extends previous research by uncovering how gender and income influence the use and avoidance of health and social services for participants in Kingston. Such knowledge is vital to advancing improvements in access to health and social services by women on a low income—an equity-deserving group—that they may attain, maintain, and promote their overall health and quality of daily living.
The participants discussed health and social services as crucial to their survival and to their efforts maintaining their health and well-being, and basic needs., Yet, they often faced significant barriers when attempting to obtain those services. Previous researchers have reported income-related barriers to accessibility despite the existence of universal health care coverage (Angus et al., 2013; Lombardo et al., 2014; Socías et al., 2016). Finding one's way in the Canadian health and social systems can be complex, especially for people living in poverty who may not have access to the same resources and support as others (Angus et al., 2013; Lombardo et al., 2014; Socías et al., 2016) or feel confident in advocating for themselves. The systems can involve numerous agencies, programs, and services, each with its own set of rules and requirements (Socías et al., 2016). For the participants, knowing where to turn or whom to consult for help was exceptionally difficult, sparkling frustration and anxiety. They detailed how finding one's way and learning the health and social systems processes could be time-consuming and exhausting, requiring determination, persistence, patience, and resilience; this finding is echoed by Angus et al.'s (2013) and Lombardo et al.'s (2014) reports of poverty as a countervailing force limiting women's access to health care services in Ontario. The participants in our study revealed their struggles of living on social assistance, underscoring the urgent need for increases in such programs. Further, our finding lower socioeconomic status negatively affects ease of access and use of health and social services corroborates previous descriptions of the dynamic interaction of gender and poverty (Burnett et al., 2016; Sinclair et al., 2022; Socías et al., 2016). Addressing these issues requires a genuine, concerted effort from policymakers, health care providers, and community leaders to ensure women on a low income have their rights of access to the care and resources upheld, that they may lead healthy lives and thrive.
Accessing health care involves a process where individuals identify their health or social needs, actively seek services, and ultimately receive effective care to address those needs (Morgan et al., 2016; Socías et al., 2016). When examining access to health care and social services, it is crucial to consider the intersection of gender and socioeconomic status. The combination of gender and income can significantly influence one's ability to access health and social resources (Bryant et al., 2009; Cerceau, 2012; Morgan et al., 2016; Socías et al., 2016). The stories shared by participants in our study vividly showed how these factors impacted their ability to obtain health care and social services. One common issue raised by participants is the disregard of their health concerns, potentially because of their gender, their life circumstances living on a lesser income, and the challenges that come with that, or both. This finding aligns with the research conducted by Yates et al. (2021), which highlighted the added challenges faced by women with disabilities in receiving diagnoses, having their symptoms acknowledged, and accessing services. Additionally, Socias et al. (2016) and Bryant et al. (2009) noted that women, living on a low income are more likely than men to have unmet health needs.
Moreover, the behaviour of service providers emerged as a notable factor in service utilization in our study. The participants often felt unheard by service providers, leading to a lack of trust and communication and resulting in suboptimal health outcomes. Similarly, Loignon and colleagues (2015) and Memon et al. (2016) demonstrated how unsatisfactory communication between service users and providers impedes the development of a therapeutic relationship. In Afulani et al.'s (2020) study, service providers admitted verbal abuse, lack of privacy and confidentiality, and discriminatory behaviour, despite their emphasis on treating women with respect. Addressing this problem requires a shift in the culture of health care and social services to prioritize listening to and acknowledging the experiences of women who live on a low income and working with them in ways that are right for them and their context. To effectively confront these inequities in access, comprehensive training in gender-sensitive medical, and trauma-and violence-informed care practices for health and social providers is essential. Such training must include depth information regarding how factors like income and gender can influence health access and outcomes, and emphasize the importance of integrating patients’ life experiences—whatever those circumstances might be—into care delivery, which respect and pragmatic considerations. This approach is pivotal in enhancing patient engagement, treatment adherence, and overall health outcomes (Government of Canada). Making the experiences, needs and contexts of women living on a low income the focal point from which everything is centred, can facilitate improving the quality of care and support received from health and social services providers.
The study participants, who experienced depression, discussed how low-income living created barriers and struggles that affected their mental health. They faced a range of stressors and challenges related to their socioeconomic circumstances, including financial instability, lack of access to resources, and social isolation. These stressors led to feelings of anxiety, depression, and loneliness, which profoundly impacted their mental health and overall well-being. Nevertheless, they developed strategies for addressing their mental health difficulties. For example, finding solace in self-identified sacred spaces provided a much-needed break from the stresses of daily life and promoted mental clarity and relaxation. Community support systems were also crucial in improving participants’ health and mental well-being. Social networks were fundamental to the participants, which is echoed in previous research (Memon et al., 2016). These support systems can provide various resources, including financial assistance, food security programs, housing support, and access to health care and mental health services (Scholes et al., 2022). Community support systems can offer a sense of belonging and social connection, which can be especially critical for women who may face social isolation and stigma due to their economic circumstances (Memon et al., 2016; Scholes et al., 2022; Socías et al., 2016). Building and strengthening community support systems can improve the lives of women living in poverty and promote social and economic justice for all.
Another noteworthy finding in our study is how pets are an invaluable support system for the participants. Pets provided companionship, emotional support, and a sense of purpose and responsibility and they were also comfort and stress relief during difficult times, such as when dealing with financial hardship or social isolation. Other researchers have indicated how the human–animal bond positively impacts mental health, including reducing anxiety and depression symptoms (Pikhartova et al., 2014; Rauktis et al., 2017). However, women on a low income may need help in providing adequate pet care, including access to veterinary care and pet supplies (Pikhartova et al., 2014; Rauktis et al., 2017). In our study, social workers considered pets a source of financial stress for the participants and (direct/indirectly) questioned the choice to manage such a responsibility; nevertheless, pets were an undeniable and non-negotiable source of support and companionship for the women. Recognizing the importance of pets in the women's lives and addressing the barriers they face in caring for them can improve the quality of life for women and their animal companions—indeed, the significance of this relationship cannot be overstated and warrants more attention to enable individual well-being.
Strengths and limitations of this study
In this study, we addressed a notable gap in the existing literature by focusing on the experiences of women living on a low income in accessing health and social services. It provides a unique perspective on the intersection of gender and income as social determinants of health and their influence on service utilization. The use of qualitative methodologies, including photovoice, interviews, and focus group discussions, and particularly the amalgamation of data sources reported herein, allowed for an in-depth exploration of participants’ experiences. This approach yielded rich and nuanced insights into the challenges and barriers faced by this group of women. It is recognized the research was conducted in a specific urban area in Kingston, which may have unique characteristics and service systems. Consequently, the findings may not fully capture the experiences of women living on a low income in other regions (e.g., rural or remote settings) with different health care and social service structures. The study relies on participants’ retrospective accounts of their experiences, which may be susceptible to recall limitations. This potential constraint may impact the precision of their recollections, especially regarding past interactions with health and social service providers.
Conclusion
In summary, ease of access to health and social services for women with a low income is a critical issue that requires action from health care providers, policymakers, and communities. This population faces unique hardships related to their economic circumstances that can impact their physical and mental health, as well as their ability to access resources and support networks. Addressing these necessitates a multi-faceted approach, including improving access to health care and social services, and building community support systems, as well as the root causes of economic inequality. Prioritizing the needs and experiences of women on low income can facilitate promoting social and economic justice, reducing health disparities, and creating a more equitable, inclusive society for all.
Footnotes
Acknowledgments
We would like to express our gratitude to the Executive Director and staff of our partner organization, SVDP, for their unwavering support and encouragement throughout the study. The Advisory Committee, consisting of SVDP Board members and community representatives, played a pivotal role in guiding our research efforts. Finally, we extend our sincere appreciation to the women who participated in the study, generously sharing their personal experiences and insights.
Author contributions
The authors confirm contribution to the paper as follows:
- Study conception and design: PC-P and LD - Recruitment and data collection: MS and JW - Analysis and interpretation of results: MS, JW, PC-P and LD - Draft manuscript preparation: PC-P - Review critically for important intellectual content: LD, MS, and JW - Approved the version to be published: LD, MS, JW and PC-P - Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: LD, MS, JW and PC-P
Consent to participate
Informed consent was obtained from all women participating in the study. We used pseudonyms and blurred photos where they could be easily identified.
Consent for publication
The authors affirm that all women in the study provided informed consent regarding publishing their data and photographs.
Availability of data and material
Derived data supporting the findings of this study are available from the corresponding author (PC-P) on request. The data are not publicly available due to containing information that could compromise the privacy of research participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Social Sciences and Humanities Research Council (SSHRC) – Insight Development Grants program of Canada (File # 430-2018-00371). Dr. Pilar Camargo-Plazas was the Nominated Principal Applicant, and Dr. Lenora Duhn was the Co-Applicant of this project. Ms. Michaela Sparringa was a research fellow, and Ms. Jennifer Waite was a research assistant for the project.
Ethical approval
Ethics approval was obtained from Queen's University General Research Ethics Board (TRAQ# 6024959). We adhered to the ethical principles of conducting research with human beings outlined by the Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council (2018).