
Abstract
Stroke can be a life altering event that necessitates considerable amounts of formal and informal care. The impacts of stroke often persist over time requiring ongoing support for stroke survivors. Family members provide the majority of care and experience many life changes as a result of their caregiving role including social, financial, employment and health impacts. Formal supports such as counselling, respite, and health promotion initiatives that directly benefit caregivers or benefit them indirectly through supporting the stroke survivor, are well-placed to help caregivers manage their caregiving role. However, to date little is known about formal service use by stroke caregivers and the factors that influence their service use. This scoping review provides a critique and synthesis of what is known about stroke caregivers’ access and use of formal services intended to support them. Findings suggest that while services are available, caregivers’ ability to use them are impacted by both facilitators and barriers. Facilitators included: sex, age, and having a higher household income (depending on services used). Barriers included: high cost, poor service quality and deficient knowledge/communication regarding service availability. This review highlights a significant gap in our knowledge of caregivers’ experience in accessing and using formal services.
Introduction
Approximately 405,000 people in Canada are living with the ramifications of a stroke (Canadian Institute for Health Information, 2012; Heart and Stroke Association, 2018; Public Health Agency of Canda, 2009). While advances in acute stroke care have reduced deaths due to stroke, the personal, societal and economic burden of stroke remains significant (Gorelick, 2019; Meisel et al., 2015). After a stroke, 25% - 50% of stroke survivors require support with activities of daily living for the long term and half of stroke survivors continue to live with limitations requiring continuing caregiver support (Gordon et al., 2004; Wolfe et al., 2011).
When stroke survivors return to the community the majority of their care is provided by family members (Heart and Stroke Association, 2017). Stroke caregiving has been shown to lead to adverse caregiver outcomes on psychological health (e.g., burden, stress and anxiety), social support (e.g., relationships with friends, family members and colleagues), finances, and employment (Anderson et al., 1995; Andrew et al., 2015; Camak, 2015; Gaugler, 2010; Lutz et al., 2011; Rigby et al., 2009). Family caregivers of stroke survivors, particularly those who are older adults, have reported feeling tired and chronically stressed, and have fears about the future (Coombs, 2007). Additional impacts of caregiving include poor health status and reduced quality of life, which can persist over time (Gaugler, 2010; Rigby et al., 2009).
The caregiving role often is time consuming, limiting opportunities for leisure, social activities or work (Rigby et al., 2009). Many family caregivers feel isolated with little chance to benefit from the support of others or to attain relief from their caregiving role (Lutz et al., 2011). Although many family caregivers receive help from other family members and community assistance, 88% of family caregivers still feel that caregiving leads to negative effects on their lives such as anxiety, frustration and fear (Anderson et al., 1995; Tsai et al., 2015). Family caregivers often overlook their own health needs in order to provide care to their family member, potentially compounding the negative effects of caregiving (Bakas et al., 2014).
While many studies corroborate the challenges experienced by family caregivers during the stroke survivors’ transition from hospital to home, recent work by Pucciarelli et al. (2018) suggests that caregiver anxiety and overall burden continue beyond this initial transitional period. A cross-sectional survey study from Australia investigating the long-term social impacts of stroke showed that 45% of family caregivers report moderate to extreme changes to their leisure lives, and up to 30% of family caregivers report moderate to extreme changes to their social lives (Andrew et al., 2015).
Few studies to date have directly investigated service use and access by stroke caregivers. Existing findings highlight the negative impacts of stroke caregiving on family caregivers and suggest that caregivers might benefit from formal services that can support their caregiving role (Simon et al., 2008). Such support services include services that are aimed at the stroke survivor because they can reduce care demands on the family caregiver. While there exists one systematic review on stroke survivor and caregiver service use (Pindus et al., 2018), it concentrates on the development of an evidence base for a primary care model, focuses on general practitioner services, and only draws on qualitative studies. Therefore, the purpose of the current review was to pull together evidence on the direct and indirect (i.e., through supports provided to the stroke survivor) use of formal health and social services by family caregivers and on the factors that influence their use of these services. The results from the current review have the potential to inform practice and policy leading to greater emphasis on supporting stroke caregivers in community settings. In addition, review findings could inform caregiver assistance such as the provision of funding to provide caregiver services, e.g., individualized education, tailored respite and health promotion activities.
The questions that guided this review were: 1) What formal health and social services do family caregivers make direct and indirect (i.e., through supports provided to the stroke survivor) use of, and what are their experiences in doing so? 2) What factors influence family caregivers’ direct and indirect use of formal health and social services?
Methods
A scoping review can be used to identify knowledge gaps and to determine what types of evidence are available on a given topic or field of research (Munn et al., 2018). The five steps of the Arksey and O’Malley (2005) framework informed this review and included: (a) identifying the research question, (b) identifying relevant studies, (c) study selection, (d) charting the data, and (e) collating, summarizing and reporting the results. For this review, formal health and social services were defined as those services that support stroke caregivers in their caregiving role, including services aimed at the stroke survivor. Examples of formal health and social services used to support stroke caregivers in their caregiving role included: (a) counselling, (b) caregiver support groups, (c) medical appointments (primary and specialist care), and (d) respite care. Examples of services that were directed to stroke survivors but benefit caregivers included: (a) care provided by personal support workers, (b) speech language pathology, (c) physiotherapy or occupational therapy, and (d) adult day programs.
Search strategy
The following electronic databases were searched: AgeLine, CINAHL, EMBASE, Medline, and PsychInfo. The search was conducted to locate eligible articles that described the following information: (a) Formal health and social services that family caregivers are directly and indirectly using; (b) Family caregivers’ experiences in directly and indirectly using formal health and social services; (c) Factors that influence family caregivers’ direct and indirect use of formal health and social services. Search terms were adapted as appropriate to each database, combined using Boolean operators and included: caregivers, carer, survivor, patient, stroke, cerebrovascular accident, brain infarction, CVA, cerebrovascular event, health services, community health services, health services for people with disabilities, health services for the aged, social work, suburban health services, urban health services, community networks, social, social support, social service, health services research, utilization, and usage. The initial search strategy informed by consultations with a research librarian, was run in MEDLINE and modified as necessary for the other databases (Appendix A). Where applicable, medical subject heading (MeSH) nomenclature was used. Studies were included that met the following criteria: (a) English language, (b) quantitative, qualitative and mixed-methods research studies or reviews, (c) published between January 2000 and June 2020.
The search also included hand searching of article reference lists and a Google search. Once all electronic databases were searched, duplicates were removed and the remaining articles were reviewed first by title, then by abstract and finally by a full reading of the remaining articles to identify those articles that met the inclusion criteria (Figure 1).
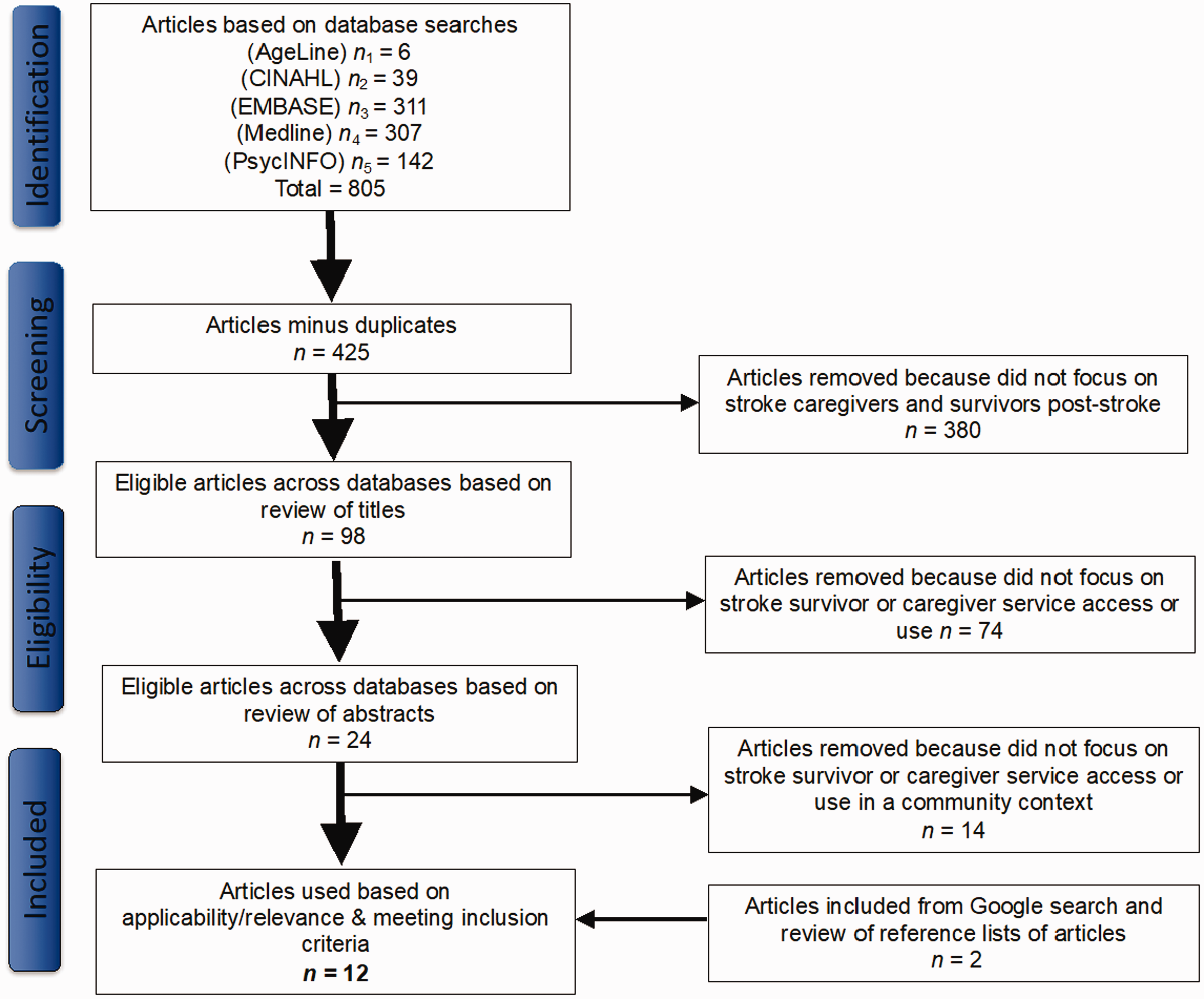
PRISMA flow diagram. Stroke caregiver use of health and social services.
Data extraction
In accordance with Arksey and O’Malley (2005) a data-charting form was use to extract data, including study contextual information, from each article using a descriptive analytic approach (Appendix B). The extracted data was then collated and summarized in table format. Subsequently, thematic presentation of findings from the literature was used in-text to represent an overview of the breadth of the literature (Arksey & O’Malley, 2005) (Table 1).
Characteristics of reviewed studies.

Quality appraisal
The methodological quality of the 12 included articles was assessed using: (a) the Critical Appraisal Skills Programe (2018) checklist that was applicable to the study methodology (qualitative, quantitative, systematic review) and (b) the mixed methods appraisal tool presented by Pluye and Hong (2014) for mixed-methods studies (Table 2).
Critical appraisal of included articles adapted from: Critical Appraisal Skills Programe (2018) Pluye and Hong (2014).
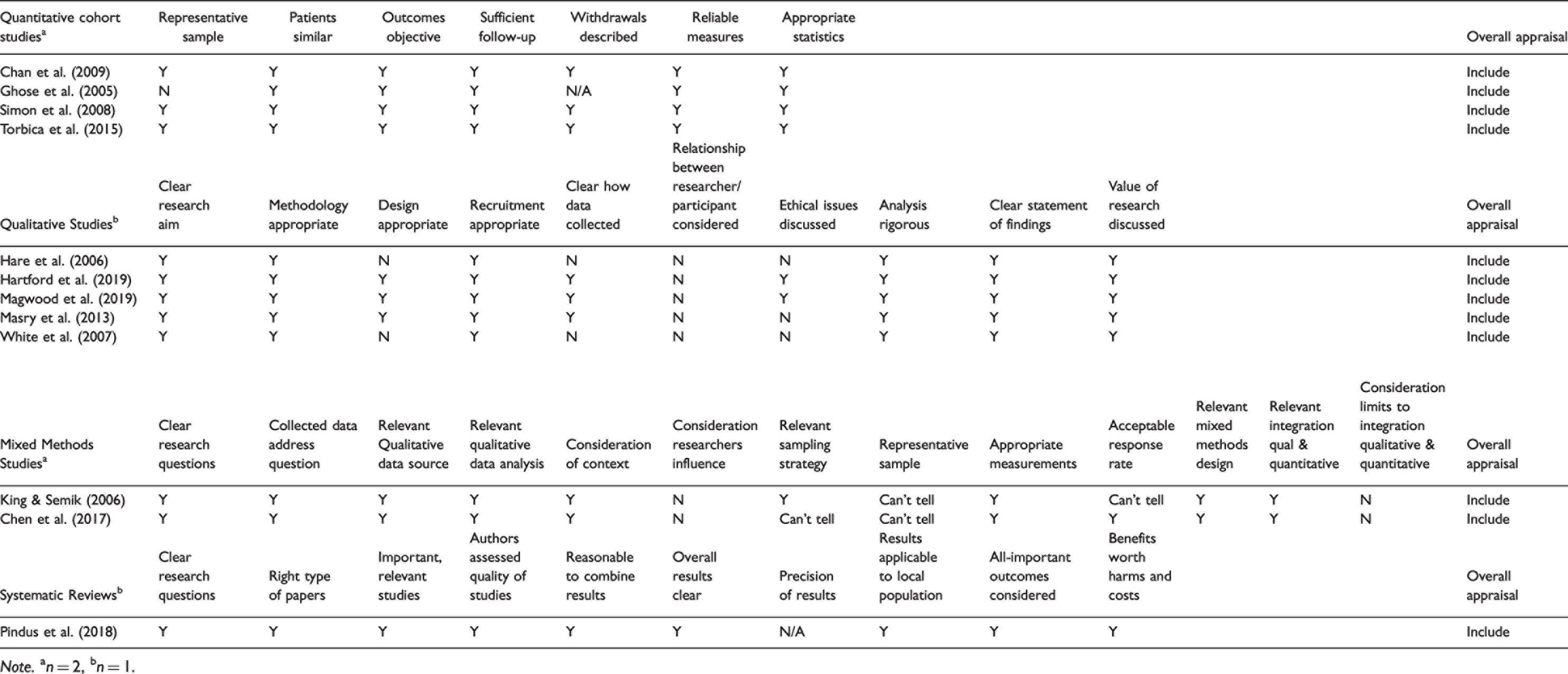
Note. an = 2, bn = 1.
The reviewed literature had some limitations and constraints: Some quantitative studies used study designs that while appropriate for the studies’ purpose were weaker in comparison with the gold standard of a randomized control trial, such as a retrospective cohort (Chan et al., 2009; Ghose et al., 2005), cohort (Simon et al., 2008; Torbica et al., 2015) and case control sub-study design (Ghose et al., 2005). Some study samples focused on a particular race or ethnicity (Chan et al., 2009) and professional background (included only veterans) (Ghose et al., 2005), or were of small size (Chen et al., 2017; White et al., 2007).
Some qualitative studies provided limited description of the research design (Hare et al., 2006), lack of detail about interview and focus group questions (Hare et al., 2006; Hartford et al., 2019; Magwood et al., 2019; Masry et al., 2013), and missing explanation of the theoretical framework (Hare et al., 2006; Masry et al., 2013; White et al., 2007). Several studies might have been affected by recall bias because of a long recall timeframe (Hare et al., 2006; Hartford et al., 2019; Masry et al., 2013; White et al., 2007). Sampled caregivers were mainly female spouses of stroke survivors (Hare et al., 2006; Hartford et al., 2019; Magwood et al., 2019; Masry et al., 2013; White et al., 2007) or had limited experience in their caregiving role (White et al., 2007).
The mixed-methods studies were limited by incomplete description of the qualitative and quantitative study arms and small sample size (Chen et al., 2017) and unclear weighting of the study arms (Chen et al., 2017; King & Semik, 2006). Generalizability of the results reported in the systematic review and meta-ethnography is limited by a lack of available data regarding stroke severity, long-term impairments, socioeconomic variables, and ethnicity (Pindus et al., 2018). Insights about the changing nature of healthcare needs over time were difficult to gain and the stated reaching of data saturation was not substantiated by evidence (Pindus et al., 2018).
Of the 12 articles, four fulfilled all the applicable quality appraisal criteria, and the remaining eight articles fulfilled between 60% and 90% of the applicable quality appraisal criteria. All articles met the majority of the specified quality appraisal criteria and were included in the review (Table 2).
Results
After excluding duplicates, a total of 425 unique articles remained. Of these unique articles, 380 were removed because they did not focus on stroke caregivers and survivors post-stroke; 74 were removed because they did not investigate family caregiver direct and indirect use; and 14 were removed because they were not centred on family caregiver or stroke survivor service use in a community context. Two articles were added after completing an additional Google search. Ultimately, 12 articles were found that met the inclusion criteria (Chan et al., 2009; Chen et al., 2017; Ghose et al., 2005; Hare et al., 2006; Hartford et al., 2019; King & Semik, 2006; Magwood et al., 2019; Masry et al., 2013; Pindus et al., 2018; Simon et al., 2008; Torbica et al., 2015; White et al., 2007).
Characteristics of the reviewed articles
The 12 articles included five qualitative studies (Hare et al., 2006; Hartford et al., 2019; Magwood et al., 2019; Masry et al., 2013; White et al., 2007), two mixed-methods studies (Chen et al., 2017; King & Semik, 2006), four quantitative studies (Chan et al., 2009; Ghose et al., 2005; Simon et al., 2008; Torbica et al., 2015), and one systematic review (Pindus et al., 2018). Details of each study including purpose, design, sample, methods, results are presented in Table 1.
Study participants included: (a) caregivers (Chen et al., 2017; King & Semik, 2006; Simon et al., 2008; White et al., 2014), (b) caregivers and stroke survivors, (Hare et al., 2006; Masry et al., 2013; Pindus et al., 2018), (c) stroke survivors (Chan et al., 2009; Ghose et al., 2005; Torbica et al., 2015), and (d) stroke survivors, caregivers and health providers (Hartford et al., 2019; Magwood et al., 2019).
Findings are discussed as they pertain to two guiding research questions: 1) family caregivers’ direct and indirect use of formal health and social services and their experiences using these services, 2) factors that influence family caregivers direct and indirect use of formal health and social services.
Family caregivers’ direct and indirect use of formal health and social services and their experiences in using these services
Seven of the 12 reviewed studies explored family caregiver direct and indirect use and experiences in using formal health and social services (Chen et al., 2017; Hare et al., 2006; Hartford et al., 2019; King & Semik, 2006; Magwood et al., 2019; Simon et al., 2008; Torbica et al., 2015) (Table 1). Several studies revealed that while family caregivers rated various services as important, few family caregivers used these services (King & Semik, 2006; Simon et al., 2008).
Services used
The limited research available indicates that stroke caregivers continue to access a variety of formal health and social services a considerable time after the stroke occurrence. Services used more frequently by family caregivers included: homecare services, peer support and general practitioners. Services used less frequently by caregivers included: counselling, inpatient respite and helplines.
Research from the UK determined that 96% of 105 stroke caregiver-survivor dyads were using an average of 4.1 services (e.g., general practitioner, physiotherapist, home carer, counsellor, speech therapist, or night nurse) at 15 months post-stroke (Table 1) (Simon et al., 2008). Family caregivers reported using the following services: general practitioner (77%), community nurse (73%), social services (42%), hospital outpatient (37%), day centres (31%), specialist stroke support nurse (20%), speech therapist (20%), voluntary support groups (18%), inpatient care or respite (5%), community psychiatric nurse (4%), and counsellor (1%) (Simon et al., 2008). An Italian observational study of 532 stroke survivors found that 6–12 months post-stroke, stroke survivors had used the following services: drugs (83%), visits to general practitioner or specialist (79%), imaging (39%), outpatient rehabilitation (21%), hospitalization (5%), nursing home (2%), and inpatient rehabilitation (1%) (Torbica et al., 2015). A qualitative study conducted in the UK determined that approximately half of the 27 study participants (caregivers and stroke survivors) received some type of service (e.g. private home care, social services and home care) on a regular basis (6 weeks - 22 years post-stroke) (Hare et al., 2006). A mixed methods study from the USA found that 80% of the 20 participating family caregivers wanted more rehabilitation for the stroke survivor (Chen et al., 2017) (Table 1).
A study of 93 family caregivers in the USA found that they continued to use services such as home health care (51%), spiritual support (49%), talking with peers (37%) and counselling (20%) up to two years post-stroke (King & Semik, 2006). However, very few family caregivers used services such as transportation, financial guidance and information on resources and survivor behaviours (King & Semik, 2006).
Services desired
Family caregivers report positive experiences and value in using services such as support groups and information services, but they also highlight barriers to use such as the limited availability of services, a generalized lack of communication regarding services and their availability and fragmentation of services. Furthermore, studies also revealed that family caregivers did not use services that they nevertheless deemed as important.
Family caregivers and stroke survivors cited the high cost of rehabilitation and the inconsistent availability of homecare services as reasons for the non-use or limited use of supportive services (Hartford et al., 2019). They also noted that suitability of available services and cancellations due to short staffing issues hindered their ongoing use of services (Hartford et al., 2019). Furthermore, poor communication and limited time given to family caregivers and stroke survivors led to feelings of mistrust and unhappiness with services used by both family caregivers and stroke survivors in one US study (Magwood et al., 2019) (Table 1).
Services used infrequently despite being rated as important were respite, stress management, and conversing with peers (King & Semik, 2006; Simon et al., 2008) (Table 2). Over half of family caregivers participating in a USA study rated counselling, support groups and stress management services as important; however, these services were only used by 20% of caregivers (King & Semik, 2006). Further, 34–74% of family caregivers in that study stated during in-depth interviews that services such as respite, stress management strategies and engaging with peers were important to them although they were not using these services (King & Semik, 2006). Canadian research by Hartford et al. (2019) also determined that support groups were valued by family caregivers and stroke survivors, but program coordinators emphasized that the success of such programs was often hindered by limited health system support. Several studies identified unmet family caregiver service needs that included services providing information on caring for stroke survivors, social-recreational supports and rehabilitation, and the fragmentation of community support services (Chen et al., 2017; Hartford et al., 2019; King & Semik, 2006; Magwood et al., 2019; Masry et al., 2013). However, an examination of family caregivers’ experiences in using these formal health and social services in the UK revealed that 74% of caregivers were satisfied with the few services they did use up to 15 months post-stroke (Simon et al., 2008) (Table 1).
Factors that influence family caregivers’ direct and indirect use of formal health and social services
All 12 of the included studies explored factors associated with direct and indirect formal health and social service use by family caregivers (Chan et al., 2009; Chen et al., 2017; Ghose et al., 2005; Hare et al., 2006; Hartford et al., 2019; King & Semik, 2006; Magwood et al., 2019; Masry et al., 2013; Pindus et al., 2018; Simon et al., 2008; Torbica et al., 2015; White et al., 2007) (Table 1).
A number of factors impacted service direct and indirect use by family caregivers including socio-demographic factors such as age and sex (Chan et al., 2009; Chen et al., 2017; King & Semik, 2006; Simon et al., 2008; Torbica et al., 2015), financial factors (Chan et al., 2009), geographic factors (Chan et al., 2009; Simon et al., 2008; Torbica et al., 2015), racial factors (Chan et al., 2009; King & Semik, 2006), caregivers’ knowledge related factors (Hare et al., 2006; King & Semik, 2006; Masry et al., 2013; Pindus et al., 2018; Simon et al., 2008), social-relational factors such as marginalisation of caregivers (Hare et al., 2006; Pindus et al., 2018), service provision and accessibility factors such as type of available services (Masry et al., 2013; Pindus et al., 2018; White et al., 2007) and stroke survivor-related factors (Chan et al., 2009; Ghose et al., 2005; Simon et al., 2008; Torbica et al., 2015) (Table 1). Overall, the findings suggest that services for family caregivers and stroke survivors often are available, but a gap exists regarding our understanding of the reasons why these services are not always accessed and used.
Financial factors
Financial factors (e.g., household income, insurance coverage and service associated costs) impacted service use by stroke survivors and their family caregivers. Chan et al. (2009) reported that higher median household income was associated with higher use of outpatient rehabilitation in the USA, a finding echoed by Hartford et al. (2019) suggesting that these services require additional out-of-pocket expenses even if funded by health insurance plans. Compounding these income effects, increased service associated costs and lack of insurance coverage hindered family caregiver direct and indirect use of services (Chen et al., 2017; Hartford et al., 2019; King & Semik, 2006) (Table 1).
Torbica et al. (2015) explored the interplay of family caregiving and stroke survivors’ formal care utilization in Italy. They found that total healthcare costs were higher for stroke survivors who had a family caregiver, irrespective of the hours of support provided, compared to stroke survivors without family caregivers (Torbica et al., 2015). The authors suggest that the higher healthcare costs associated with family caregiving arise because caregivers facilitate stroke survivors’ use of rehabilitation and other services but potentially it is the severity of stroke that demands the support of a family caregiver in the first place (Torbica et al., 2015) (Table 1).
Demographic factors
Specific socio-demographic factors that were associated with service use included: age, gender, place of residence and race (Chan et al., 2009; Chen et al., 2017; King & Semik, 2006; Simon et al., 2008; Torbica et al., 2015) (Table 1).
Direct In a retrospective cohort study conducted in the USA, increasing stroke survivor age was associated with higher levels of service use in older female stroke survivors (Chan et al., 2009). However, the same study determined that decreasing stroke survivor age was associated with greater levels of outpatient rehabilitation service use (Chan et al., 2009). This study also reported that male stroke survivors were more likely to use outpatient rehabilitation services and female stroke survivors were more likely to receive homecare services (Chan et al., 2009). In a prospective observational study from Italy, a finding of note was that increasing age of caregivers was associated with lower service use by stroke survivors (Torbica et al., 2015). In these instances, older caregivers may have their own health constraints, therefore rendering them less able to support the stroke survivor in accessing and using services, for example, in assisting with transportation or mobility of the stroke survivor.
Researchers identified geographic location as a determining factor for service use, with those who lived in urban settings having greater overall service use (Simon et al., 2008) and greater use of outpatient rehabilitation (Chan et al., 2009; Torbica et al., 2015) (Table 1). These findings suggest that those who are situated in rural settings may experience challenges in using community-based services. Additionally, fragmentation of community services was determined to be a barrier to using services likely due to the increase in steps required to access services such going to multiple locations rather than have centralized services (Magwood et al., 2019).
Chan et al. (2009) reported that stroke survivors who were non-white made greater use of outpatient rehabilitation services than stroke survivors who were white in the USA (Chan et al., 2009). The authors hypothesized that use of rehabilitation services by non-white stroke survivors might be facilitated by increased cultural sensitivity among health service providers who have received unconscious racial bias training (Chan et al., 2009). Paralleling this finding is the observation in another study from the USA that non-white caregivers showed a lower incidence of unmet caregiver needs than white caregivers (King & Semik, 2006) (Table 1). Research by Magwood et al. (2019) suggest that cultural and racial differences may affect service with findings that African-Americans may not as readily seek services as Caucasians with similarly presenting symptoms.
Knowledge-related factors
Knowledge-related factors such as prior experience with stroke and time since stroke led to variable impacts on service use through several pathways. For example, when family caregivers had limited knowledge of available services this hindered their use of services (Hare et al., 2006; King & Semik, 2006; Magwood et al., 2019). The results of a UK study suggest that even in situations where the survivors’ stroke occurred several years earlier, family caregivers demonstrated a lack of knowledge of services available to them, suggesting that length of caregiver experience does not necessarily increase knowledge of and use of services (Hare et al., 2006). However, another study conducted by Simon et al. (2008) in the UK found that having caregiving experience and other care commitments led to an increased use of formal services for stroke survivors. Information on a broad array of topics, such as stroke management, employment benefits counselling and making community connections was felt to be lacking by both caregivers and stroke survivors and, of particular note, there was an identified lack of awareness of support groups like the Stroke Association by caregivers and stroke survivors alike (Hare et al., 2006) (Table 1).
Family caregivers also faced challenges in finding out about training that could support their role. For example, family caregivers reported that many service providers discussed the importance and requirement for caregiver training, but not necessarily how caregivers were going to acquire this training, which contributed to caregivers’ levels of anxiety (Pindus et al., 2018). Moreover, family caregivers and stroke survivors alike expressed dissatisfaction about the inadequate information available on stroke, particularly regarding post-stroke health and symptom management (Magwood et al., 2019; Masry et al., 2013; Pindus et al., 2018) (Table 1).
Socio-relational factors
Examining the impact of social-relational factors on service use, family caregivers stressed their role as advocates for the stroke survivor (Hartford et al., 2019). However, many family caregivers experienced marginalisation and fear of stigma around stroke and some caregivers did not dare to speak out about service shortcomings for fear of losing service access as repercussion (Hare et al., 2006; Pindus et al., 2018). In a UK study, family caregivers felt they had to be care experts with little opportunity for respite and in some cases were worried about asking for help for fear of upsetting the stroke survivor (Hare et al., 2006) (Table 1).
Service quality and availability
Several factors related to the quality and availability of services influenced use of services. The literature suggests that family caregivers were frustrated by the lack of ongoing care provision or acknowledgement that more care was required once the stroke survivor returned to the community (Hartford et al., 2019; Magwood et al., 2019; Pindus et al., 2018). Family caregivers also felt that the prevailing attitude from the health system was that they would be the primary caregivers for the stroke survivor with few or no formal services being provided to assist them (Pindus et al., 2018). In addition, the low quality of some available services (Masry et al., 2013) as well as the lack of availability of some services such as respite and accessible community services constrained family caregivers’ direct and indirect access and use of services (Pindus et al., 2018; White et al., 2007) (Table 1).
Stroke survivor disability
Higher use of services was associated with higher levels of stroke survivor disability (Simon et al., 2008; Torbica et al., 2015), longer acute care hospitalization of the stroke survivor (Chan et al., 2009), post-stroke depression (Ghose et al., 2005), having an ischemic stroke (Chan et al., 2009), and having spatial neglect (Chen et al., 2017). A positive association between the extent of the stroke survivor’s disability and caregiver service use has been shown by a study from the UK (Simon et al., 2008) (Table 1).
Discussion
Family caregivers can experience many direct and indirect benefits from formal health and social services delivered in the community, but their use of these services is often hindered by multiple factors. Primary care services and community-based rehabilitation services were designed to support stroke survivors and family caregivers in their recovery and integration into the community but are underutilized. (King & Semik, 2006; Simon et al., 2008). However, research findings suggest that though caregivers also value other services such as respite, such services are used by limited numbers of caregivers (King & Semik, 2006; Masry et al., 2013).
Potential barriers to their use could be related to the availability of information and communication which often decrease once the stroke survivor returns to the community and caregiver needs are further realized (Eames et al., 2010). Findings from a multi-disease focus caregiver study in Canada echoed these findings, determining that caregiver respite was the most needed but least accessed service (Lin et al., 2016). Suggested reasons included: financial costs of services, challenges in access (time or location, waitlist, not culturally suitable) as well as difficulties in using the system (Lin et al., 2016). Nurses and care-coordinators would be well-placed to support caregivers in these situations, providing telephone follow-up to address education, caregiver physical and psychosocial health as well as providing direct referrals to services such as respite (Cameron et al., 2016; Grant et al., 2014; Plank et al., 2012). Offering programs in parallel, such as stroke rehabilitation and caregiver wellness programs, could also help overcome the time demands frequently faced by caregivers. Furthermore, reasons for non-use of services such as respite and support groups should be included in service evaluation measures. Data forthcoming from these evaluations could inform policies and initiatives that would promote use of valued services that are currently underutilized due to factors such as high cost, bad timing, or lack of communication.
The review findings indicate that stroke severity and stroke complexity, the presence of post-stroke depression (Ghose et al., 2005), higher level of post-stroke disability (Simon et al., 2008; Torbica et al., 2015) or prolonged acute care hospitalization of the stroke survivor (Chan et al., 2009) are associated with increased caregiver service use. Therefore, it is important to screen caregivers who are supporting survivors with complex post-stroke needs at key intervals post-stroke, so that their needs continue to be met (Cameron et al., 2013). The toll of caregiving may only become apparent after considerable time has passed making it less likely that the caregiver will be connected with community supports once this toll materializes. Therefore, caregivers and health providers need education on issues such as self-care, signs and symptoms of caregiver burden and caregivers need to be encouraged to reach out to health providers as their health requires (Reinhard et al., 2008). Prior research suggests that caregivers who were able to continue participating in activities they cared about were more likely to report psychological well-being (Cameron et al., 2014). As such, both short and long-term care plans for stroke survivors should consider strategies to address caregiver health and well-being.
Older, female stroke survivors are more likely to use services including homecare while male stroke survivors are more likely to use outpatient rehabilitation (Chan et al., 2009). Furthermore, increasing age of caregivers was associated with less use of services by stroke survivors suggesting an increased need to support both older caregivers and older stroke survivors (Torbica et al., 2015) (Table 1). Overall, these findings raise important issues around age, sex, and caregiving. The finding that female stroke survivors are more likely to receive homecare than male stroke survivors suggests there are sex differences in assuming caregiver roles. The literature supports this finding, showing that overall, women provide greater amounts of care and subsequently also experience greater negative outcomes when compared with their male counterparts (Pinquart & Sorensen, 2006; Yee & Schulz, 2000). Additionally, women are more likely to experience multiple pressures from work, home and care for family members (Doyal, 2001; Swinkels et al., 2017). In addition, women may experience greater difficulty in accessing supports than men (Doyal, 2001). The literature also suggests that population-wide, females have greater unmet health needs than males, indicating that access and use of services needs to be better understood (Socias et al., 2016).
A limitation of the review was the inclusion of only English language articles that may have led to the omission of relevant articles published in other languages. Additionally, the inclusion of grey literature may have also pointed towards emergent research in this nascent field of inquiry.
Areas for further research
Most research to date has explored approaches to support caregivers and caregiving related issues such as caregiver burden, decline in health or inability to continue in a caregiving capacity. However, few studies have directly explored direct and indirect service use and access by stroke caregivers. Further research is warranted to explore the population, health system, community and individual level factors that influence direct and indirect service use by stroke caregivers, and to understand what factors individually or in combination predict service use. A qualitative study design could be used to identify other factors and to understand the influence of context on decision making regarding service use. This would be particularly important given that the variable geographic context of the studies included in the review suggest that caregivers’ choice to use services may be in part based on variation in health infrastructure among countries, as well as between urban and rural regions. Additional research to explore service use at defined periods of time post-stroke could also help inform the development and delivery of services that meet caregiver needs across a continuum. Furthermore, the findings would be well-placed to inform optimization of current service provision and to develop targeted initiatives directed towards addressing stroke caregiver needs.
Conclusions
Few studies have investigated the direct and indirect use of formal health and social services by stroke caregivers and some of these studies had methodological limitations. The limited research available indicates that caregivers continue to use formal health and social services in the community after the stroke survivor is discharged. Caregivers often used services that included: homecare services, peer support and the services of a general practitioner. Less frequently they used: counselling, respite and helplines. Importantly, studies found that there were some services that caregivers evaluated as important but that they did not use.
The results of this review demonstrate that some caregivers benefit from services long after the stroke survivor experienced their stroke such as homecare services, peer support and the services of a general practitioner. However, other caregivers made no use of services even if they found them important such as counselling, support groups and stress management services. The results of this review suggest that several factors are important in limiting caregivers’ direct and indirect use of services while also potentially increasing caregivers’ need for services to support them, such as higher age and residing in rural areas. Nevertheless, to date we have limited understanding of caregivers’ experience in accessing and using these services, and of the healthcare system contexts that impact both the availability and caregivers’ use of services.
Footnotes
Appendix A
Literature search strategy
MEDLINE (OVID) Search Strategy: January 2000–June 2020
ID
Concept
Search
1.
Caregivers
caregivers/
2.
carer*.ti,ab.
3.
caregiver*.ti,ab.
4.
care giver*.ti,ab.
5.
1 or 2 or 3 or 4
6.
Stroke Survivors
survivors/
7.
surviv*.ti,ab.
8.
survivor*.ti,ab.
9.
6 or 7 or 8
10.
Stroke
exp stroke/
11.
stroke*.ti,ab.
12.
cerebrovascular accident*.ti,ab.
13.
brain infarction*.ti,ab.
14.
CVA.ti,ab.
15.
cerebrovascular event*.ti,ab.
16.
10 or 11 or 12 or 13 or 14 or 15
17.
Services
health services/
18.
exp community health
19.
health services for persons with disabilities/
20.
health services for the aged/
21.
exp rural health services/
22.
exp social work/
23.
exp suburban health services/
24.
exp urban health services/
25.
health service*.ti,ab.
26.
17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25
27.
Supports
community networks/ or social support/
28.
support*.ti,ab.
29.
social service*.ti,ab.
Appendix B
Scoping review question
Study title
Author(s)
Year of publication
Country where study published or conducted
Study purpose
Study context
Study population and sample size
Methods
Study design
Outcome measures
Key findings – pertaining to purpose of review
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.