
Abstract
Background
Cancer incidence has increased for First Nations and Métis Peoples in Canada over recent years. Despite a growing cancer burden, there remain challenges to accessing culturally appropriate and quality care in Saskatchewan.
Objective
The study aimed to explore, from cancer survivors’ perspectives, the potential of Indigenous patient navigators to enhance the healthcare experiences of First Nations and Métis cancer survivors in Saskatchewan.
Methods
We conducted semi-structured interviews with 19 First Nations and Métis cancer survivors. Participants were interviewed by phone between May 2022 to March 2023. Thematic analysis was conducted to generate themes, categories, and codes reflecting participants’ experiences with patient navigators.
Results
Participants reported several supports to help patients with cancer through their cancer journey, including family, community, traditional ways, and First Nations and Métis health support services. Challenges to accessing care included language and communication barriers, logistical challenges, cultural differences, financial challenges, and gaps in care. Indigenous patient navigators may play a critical role in overcoming barriers by providing communication, translation, coordination, education, advocacy, and guidance to Indigenous cancer survivors. In participants’ view, the tasks of Indigenous patient navigators could vary, ranging from helping schedule appointments to advocating for the patient's treatment preferences. In addition, Indigenous patient navigators could be helpful bridging Western medicine with traditional medicine when supporting patients seeking cancer care.
Conclusion
According to study participants, Indigenous patient navigators could be beneficial to Indigenous cancer survivors in Saskatchewan.
Background and purpose
Cancer is the leading cause of death in Canada, accounting for 28% of all deaths. Similarly, 1 out of every 5 Canadians is expected to be diagnosed with cancer in their lifetime (Canadian Cancer Society, 2023). Cancer survivors face physical (e.g., decreased mobility, fatigue), mental (e.g., depression, anxiety), emotional, social, and financial challenges from diagnosis to treatment. Cancer survivors may require frequent access to care for treatment and follow-up; some may experience adverse side effects from treatment, with negative impacts on their quality of life (Centers for Disease Control and Prevention, 2023). The cancer care system can be difficult to navigate for patients and families. The emotional distress of a diagnosis and the physical symptoms of the disease and treatment can amplify the difficulty of cancer care navigation (Cancer Care Ontario, 2014).
Cancer is a greater burden among Indigenous Peoples due to factors such as health inequities, the lasting effects of colonization, and barriers to accessing healthcare. Indigenous Peoples experience a higher incidence of cancer and higher mortality rates than those of the general Canadian population (Mazereeuw et al., 2018a; Mazereeuw et al., 2018b). Another significant barrier stems from the effects of colonization (Cancer Care Ontario, 2014). For example, many Indigenous Peoples experience intergenerational trauma because of colonial policies (e.g., residential schools), which may have epigenetic implications, contributing to stress that can be passed down to the next generation (Moon-Riley et al., 2018). The increased stress linked to integrational trauma could lead to a higher risk of cancer among Indigenous Peoples (Dai et al., 2020). Further, colonization has resulted in the suppression of Indigenous cultural practices and traditional healing, which can impact individuals’ wellbeing and coping mechanisms (Beckett et al., 2021). An additional aggravating factor is that many Indigenous Peoples live in rural and remote areas; therefore, they may have challenges accessing cancer diagnoses and treatment, which is typically centered in urban regions (Beckett et al., 2021). Consistently, Sedgewick et al. (2021) explored service providers’ perceptions of support needs for Indigenous cancer patients in Saskatchewan. From the perspective of service providers, the authors identified gaps such as logistical barriers (e.g., reimbursement for medication and travel costs) and the need to provide culturally relevant care to Indigenous cancer survivors (Sedgewick et al., 2021).
The Truth and Reconciliation Calls (TRC) were created to address the legacy of residential schools and advancing the process of Canadian reconciliation. The calls were shared in a report, calling upon the federal government to, in consultation with Indigenous Peoples, develop interventions in six areas: Child Welfare, Education, Language and Culture, Health, Justice, and Reconciliation. In agreement with the TRC, there is a need to provide culturally appropriate healthcare for the Indigenous population that includes Indigenous worldviews and builds trust (Truth and Reconciliation Commission of Canada, 2015). A knowledge synthesis on trust and worldview in shared decision-making with Indigenous patients revealed that historical trauma, lack of system support, and lack of reciprocal respect contributed to a decreased trust in healthcare providers (Groot et al., 2020). A needs assessment study, entitled Sâkipakâwin, explored the barriers to cancer support for First Nations and Métis people in Saskatchewan and highlighted the need for better support for Indigenous cancer survivors (Witham et al., 2022).
Due to the lack of access to appropriate cancer care for Indigenous Peoples in Canada, Indigenous patient navigators have been introduced to assist Indigenous cancer survivors and their families with their cancer journeys. Indigenous patient navigators can assist with navigating cancer care in a variety of ways, including connecting patients with social services or financial supports (McBrien et al., 2018). They could also work to advocate for Indigenous cancer survivors or to evaluate the health of the patient in-between appointments with medical professionals. Finally, Indigenous patient navigators can help cancer survivors to bridge the gap between Western medicine and Indigenous cultural practices by connecting them with traditional medicine, while also assisting them with navigating the Canadian medical system (Rankin et al., 2022).
Although there are several articles about the role of Indigenous patient navigators (Bernardes et al., 2018; Burhansstipanov et al., 2015; Hiscock et al., 2022; Rankin et al., 2022; Sheppard, 2019; Vargas et al., 2008; Whop et al., 2012), studies that capture Indigenous cancer survivors’ perspectives about the role of Indigenous patient navigators in Canada are lacking. Given that Indigenous Peoples continue to experience trust issues with the healthcare system, the need to tailor Indigenous patient navigator programs based on cancer survivors’ perspectives is warranted.
Therefore, this study aimed to explore, from cancer survivors’ perspectives, the potential for Indigenous patient navigators to enhance the healthcare experiences of First Nations and Métis cancer survivors in Saskatchewan. Findings from the current study could inform the development of culturally safe cancer services, including an Indigenous navigator program for cancer survivors.
Methods and procedures
Study design
This is a qualitative and exploratory study designed to understand, from cancer survivors’ perspectives, the role of Indigenous patient navigators for cancer survivors in Saskatchewan.
Setting and sample
Participants were recruited from nine clinical offices in partnership with the First Nations and Métis governance as well as the provincial cancer agency. Nurses, surgeons, and administrators at each site were provided with study pamphlets to help recruit eligible participants, who then provided consent to be contacted by the researchers. We used a snowball sampling technique and connected with several Indigenous communities to recruit through their health clinics. Participants were also asked to share the pamphlet with other survivors and community members.
Patients living with cancer or those who hads finished cancer treatment were eligible to participate if they had at least one recent experience of cancer treatment or had completed their cancer treatment in the province within the past ten years. Patients in palliative care and those under 18 years old were excluded.
Protection of human participants
The project was approved by the Behavioral Research Ethics Board at the University of Saskatchewan (REB 3238). Participants were interviewed after providing informed consent. Interview transcripts were anonymized and stored on university encrypted computers.
Data collection
Interviews were conducted by two researchers (SW and JDMS) by telephone, as many participants were located across the province and phone interviews provided more flexibility regarding time, technological, and/or health-related constraints. A semi-structured interview guide was developed and used to ask participants about their perceptions of how an Indigenous patient navigator could support their cancer journey. To prompt participants to share their experiences in healthcare, we included initial questions about the impact of cancer on their lives and their key supports and challenges. Participants who had completed cancer treatment were asked to draw from their experiences while in treatment. All participants were provided with an honorarium for their time. The average interview time was 28 min, with minimum duration of 13 min and maximum of 70 min. Participants 12 and 15 preferred not to have their interviews recorded, but the interviewers took notes to capture their perspectives.
Data analysis
Researchers transcribed the interview audio recordings verbatim and housed the data in NVivo (Version 12). Thematic analysis was utilized to identify codes related to challenges, supports, and benefits of navigators. Two researchers independently coded and then collaboratively reviewed the codes iteratively to summarize them into themes, categories, and codes (Braun & Clarke, 2006). The perspectives of patients living with cancer and of those who had finished treatment were analyzed collectively as participants reported their experience while accessing cancer treatment in general (whether current or from within the past 10 years). The results of the analysis were reviewed by experienced Indigenous health and qualitative researchers to provide feedback about the results.
Results
A total of 21 eligible participants were contacted and 19 (90% response rate) were interviewed by phone between May 2022 to March 2023. Six (32%) participants were Métis and 13 (68%) were First Nations. Four participants identified as male and 15 as female. Participants ranged in age from 33 to 68, with an average age of 55 and a median of 57. Fifteen participants lived in rural areas, and four participants were urban dwellers. Nine participants had completed cancer treatment (breast = 4; lymphoma = 2; cervical = 1; lung = 1; and colon = 1). Ten participants were currently undergoing cancer treatment. Six participants were diagnosed with breast cancer, two with colon cancer, one with lung cancer, and one with stomach cancer. Participants described their experiences seeking cancer care including their supports, challenges, and the potential benefits of working with navigators.
As can be seen in Table 1, the thematic analysis generated the following three main themes: (1) barriers to cancer care, (2) facilitators in cancer care, and (3) patient navigator impact. Categories that were identified included challenges experienced by First Nations and Métis seeking cancer care, supports available to First Nations and Métis cancer survivors, and Indigenous patient navigator benefits, respectively.
Themes, categories and codes from the thematic analysis of cancer survivors’ perceptions of cancer care and Indigenous patient navigators.
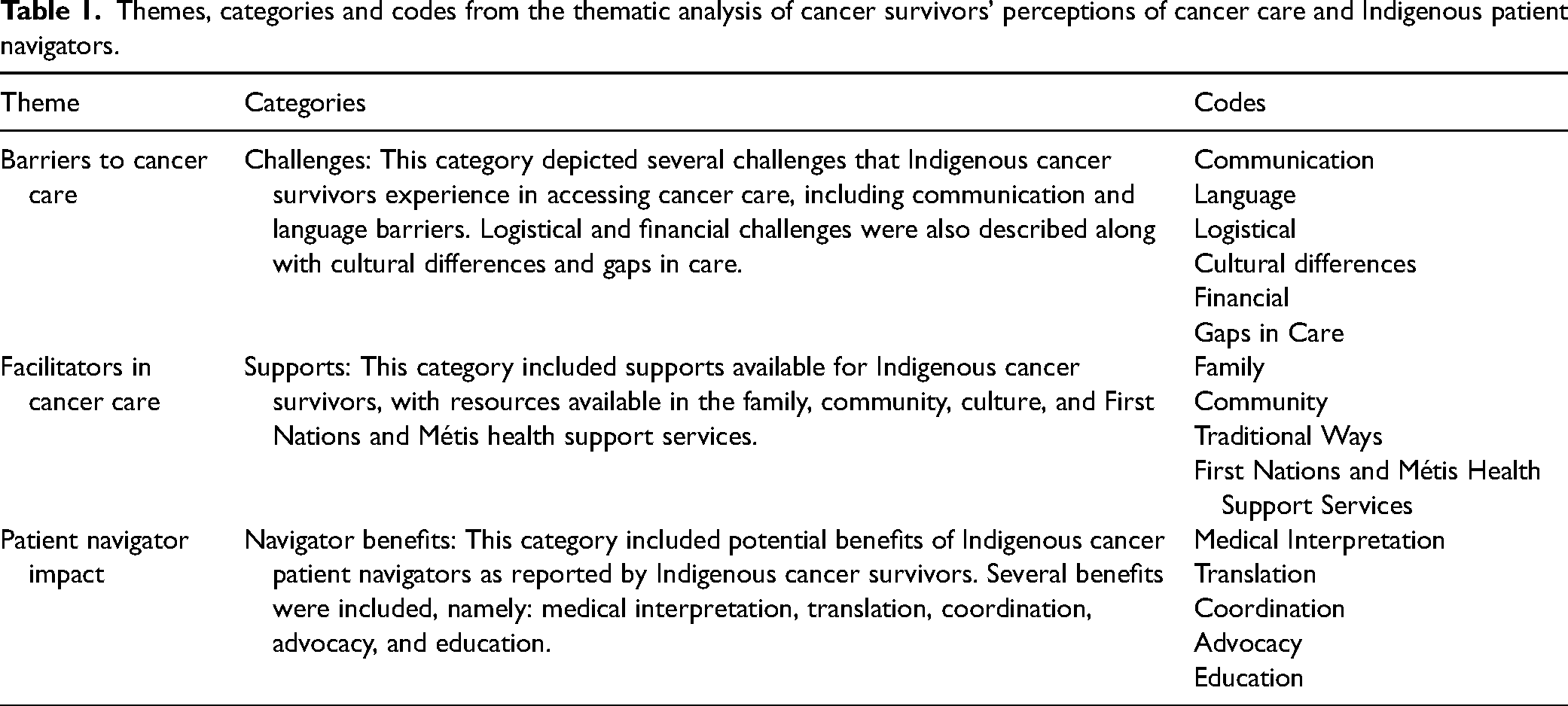
Challenges experienced by first nations and Métis seeking cancer care
Participants identified challenges they faced as they were navigating the health system. As shown in Table 2, these challenges included language and communication barriers, logistical challenges, cultural differences, financial challenges, and gaps in care
Representative quotations for each code in the three categories. Examples reflect the challenges and supports experienced by First Nations and Métis cancer survivors and the benefits of Indigenous patient navigators in cancer care.
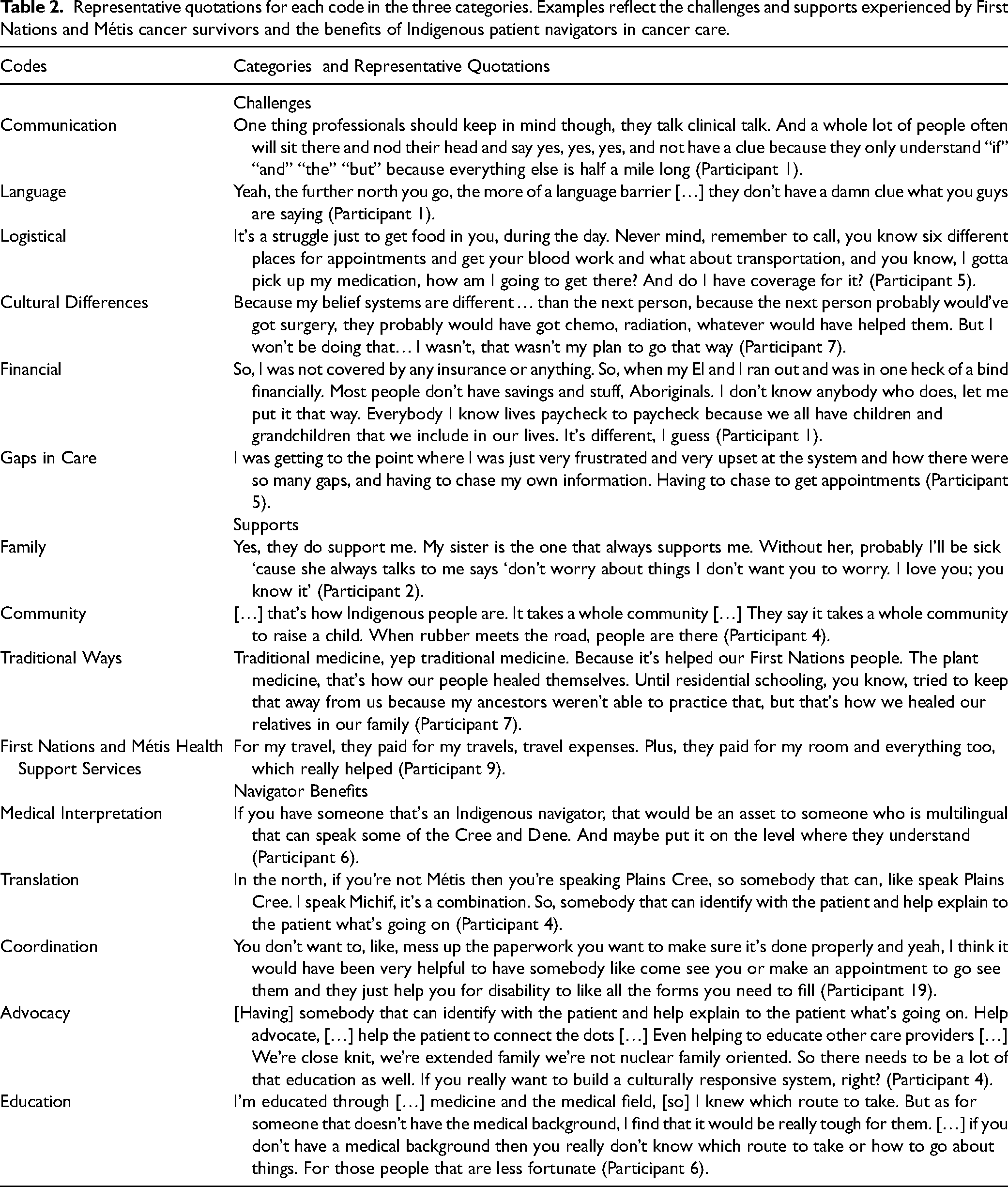
First Nations and Métis cancer survivors reported that communication issues were a major challenge when accessing cancer treatment. The communication barriers between patients and healthcare providers were related to the lack of communication between patients, lack of perceived relationship, lack of utilization of lay language by healthcare professionals, and prejudice. Additionally, issues with shared decision-making were reported. For instance, Participant 7 stated that: He [the doctor] kept asking me if I wanted surgery, and ‘this is how we are going to treat it’ and I said “No, that’s the way I’m gonna treat. It I don’t want your intervention”. You know what I mean? Like for them to say this is how we’re going to treat this thing on your breast. So, at the beginning I wasn’t happy about our conversations together. Some Indigenous people can talk choppy with English, and it causes misunderstandings. That's a barrier.
Logistical issues were also reported by First Nations and Métis cancer survivors. These issues were due to delays related to the COVID-19 pandemic, travel distance to treatment centers, scheduling appointments, picking up medication, and filling out forms. As noted by Participant 10: [I] had to wait a bit - COVID extended things for a period of time.
Participants indicated that cultural differences were considered a challenge when accessing cancer treatment. Because Indigenous ways of knowing and healing may differ from conceptualizations in Western medicine, some participants expressed concerns about being in a system that lacks consideration of Indigenous healing practices. For instance, Participant 13 explained that: A lot of First Nations people won’t talk about their medicines taken because they feel like they won’t be accepted.
Financial issues were also highlighted as a challenge for some participants. These issues arose from the lack of health coverage and disability leave. The financial burden of cancer can be particularly challenging for Métis patients since, unlike First Nations, Metis are not eligible for the Canadian Non-Insured Health Benefits Program. Consistently, a Métis participant stated that: We didn’t have any financial help and it cost, for six months, no I had six months of treatment and then I still have to continue going to Regina a few months after for the maintenance. And so that cost us around $10,000 for those eight months (Participant 18).
Study participants reported many gaps in cancer care in the province. There were concerns about the lack of doctors in the province, power imbalances, racism, lack of more cancer treatment centers in rural communities, and lack of follow-up. Some participants demonstrated dissatisfaction with the primary care provided in their local communities, where some patients felt overlooked by the family physician. For example, Participant 18 described how: For your family physicians and stuff that were looking after me then, were terrible. Because it’s just that they don’t take cancer seriously. And it wasn’t like that was just me, like, cause like some of my son's friends. And if you’re an overweight person and Métis or Indigenous, they didn’t treat you the same way, especially if you’re overweight, because they always said, oh, you’re just fat.
Available supports when seeking cancer care
Participants emphasized the types of supports they relied on throughout their cancer journey. As illustrated in Table 2, primary supports included community, family, traditional ways, and First Nations and Métis health services.
The family support participants experienced was related to emotional support, advice, encouragement, and companionship. Additionally, study participants would also seek family members to support the iraccess to traditional medicine and ceremonies, as highlighted by Participant 8: I went to my grandpa. He's big into cultural, and he makes like the rain dances, sweats and stuff. He made a sweat for me and he prayed for me and everything. He gave me this medicine to take as well […] I was actually looking into that, like an outreach group. But I haven’t really got around to it so, but I actually think those it would actually help me because like what they’re going through is what I’m going to be going through. So that's why I want to know different ways to cope with this.
Traditional medicine was often highlighted as an option as opposed to Western medicine. Overall, participants commented on the desire to use traditional medicine; however, some acknowledged that the traditional medicine could interfere with the Western medicine and were advised by doctors not to use it, as demonstrated by Participant 11: It's a lot of the natural medicines that we use for other healing also. I did mention this to the doctors at the time, and they told me to quit actually drinking it because it was affecting their outlook I guess on my blood work and stuff like that. So, I understood that they had to go with the treatment and so they could have a good idea what their treatment it was working and so. Me going off my “Indian medicine” was something that I had to do.
Participants attested to the usefulness of First Nations and Métis health support services to alleviate the burden of seeking cancer care. Such programs offer coverage for expenses such as accommodation and travel costs. For example, Participant 1 described how: I was sure glad I was ‘Treaty’ (have First Nation status) and that I didn’t have to worry about the travel expenses.
Navigator benefits
As can be seen in Table 2, participants described how an Indigenous patient navigator could assist with language translation and coordinating appointments, transportation, and health coverage. Indigenous patient navigators could also help patients understand medical terminology and advocate on their behalf, linking them to available supports.
Many participants highlighted that the Indigenous patient navigator would be helpful in explaining medical terminology to Indigenous patients. By translating the medical information to lay terms, the Indigenous patient navigator would ensure that patients understand their diagnosis, exams, and treatment. This medical explanation would be particularly helpful to patients living in Northern and remote communities where English is not the first language. For example, Participant 19 stated: That would have been helpful. […] I still don’t know the differences between like the CT scan, the CAT scan, the MRI. It all seemed like kind of the same thing to me.
[…] if you have someone that's an Indigenous navigator, that would be an asset to someone who is multilingual that can speak some of the Cree and Dene. And maybe put it on the level where they understand (Participant 6).
According to the research participants, Indigenous patient navigators could provide coordination services to help overcome some of the logistical problems that Indigenous patients with cancer experience. Participants highlighted the need for coordination in transportation, accommodation, and scheduling appointments. Participants highlighted that coordination services are much needed, especially with the health conditions that the patients are facing. By providing coordination, Indigenous patient navigators could help patients with cancer find First Nations and Métis health support services, mental health services, and support groups. Additionally, participants could also trust that the Indigenous patient navigator will be available to talk to them and check on their treatment progress, as highlighted by two participants: I think the big [services] would be transportation, accommodation, navigating appointments (Participant 5). Support, maybe support groups that they can go to or for somebody to talk to (Participant 12).
Study participants emphasized that an Indigenous patient navigator could advocate on behalf of First Nations and Métis patients and consider the cultural differences. In this role, some participants mentioned that navigators could use good communication skills to help patients tackle sensitive topics related to their health needs and help patients develop relationships with healthcare providers. The navigator should have knowledge of cancer and treatment and help elaborate a model of care that meets Indigenous Peoples’ needs.
Some participants also reported that the Indigenous patient navigator should be able to understand the needs of the patients and meet them at their level. The relational or “intimate” aspect of the Indigenous patient navigator may help patients to feel more comfortable with the healthcare system, as discussed by Participant 19: This [is] like 100% effective and helpful because it's like someone that looks like you. Somebody that can meet you on your level. And just make it more like I want to say intimate because […] [it is] kind of more, personal like cause like, I don’t know, I feel like it would be a lot more comforting to have somebody that's been through it, you know? .
So, I feel like that would be beneficial to have that ceremonial option before you go on to talk to somebody. It just makes that connection better, understanding is a lot more clearer when you’re in that zone (Participant 19).
The need for more education was a major finding in most interviews, and participants emphasized how both patients and healthcare professionals would benefit from additional knowledge. Participants also suggested that an Indigenous patient navigator can help educate patients on their diagnosis and treatment. This approach would be complementary to patient educational materials and receiving medical explanations from a doctor or nurse. Indigenous patient navigators would provide a more detailed explanation of what was discussed during medical appointments and provide a more one-on-one session with patients about cancer treatment.
Based on the participants’ perspectives, we developed a framework describing the main roles of an Indigenous patient navigator when supporting cancer survivors (See Figure 1).
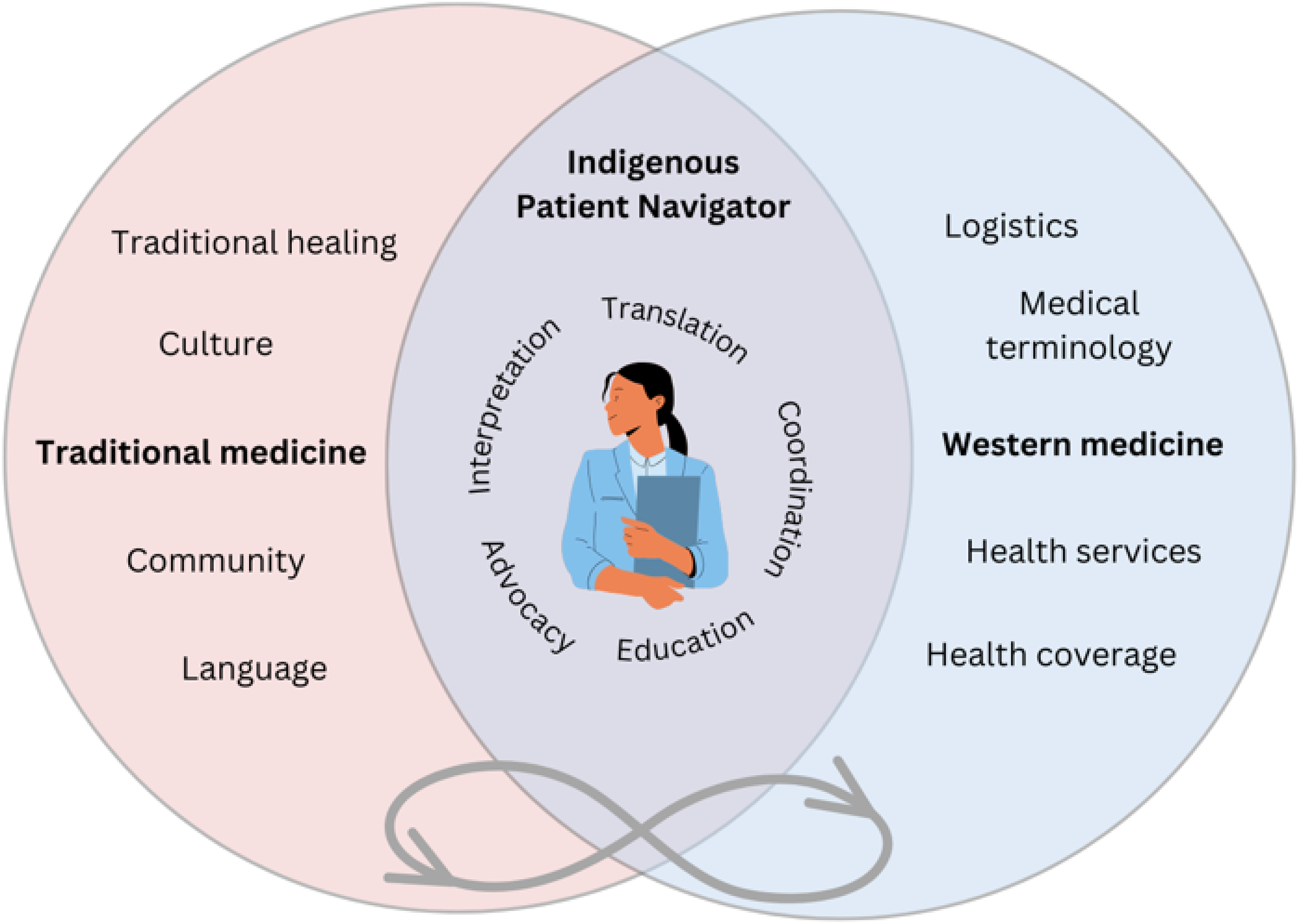
Indigenous patient navigator cancer care framework.
Discussion
In this study, First Nations and Métis cancer survivors identified cancer supports such as community, family, traditional ways, and First Nations and Métis health services. Language and communication barriers, logistical issues, cultural differences, financial issues, and gaps in care jeopardized access to cancer care. According to participants, Indigenous patient navigators can help Indigenous cancer survivors overcome barriers by providing support in communication, translation, coordination, education, and advocacy.
Individual, system, and structural level barriers to cancer support
Participants described the difficulties they encountered navigating the healthcare system. These difficulties included language and communication barriers, logistical challenges, cultural differences, financial challenges, and gaps in care. These results align with previous studies that identified barriers in access to cancer care. A number of barriers to accessing cancer care among Indigenous Peoples in Canada have been identified. These barriers can be at the individual level (individual patient or healthcare provider barriers), at the systems level (the healthcare system and its structure), and at the structural level (political, historical, social, or economic structures) (Horrill et al., 2019). Individual barriers include communication, knowledge and awareness, and experiences in care (Horrill et al., 2019) These barriers highlight the need for culturally appropriate care to tackle the lack of trust and disempowerment of Indigenous patients and families in healthcare (Horrill et al., 2019). System-level barriers include the availability of healthcare providers, accessibility and location of healthcare services, the types of services provided, and interactions between various system components of care (Horrill et al., 2019). These issues stem from the fragmented and complex nature of the Canadian healthcare system (Horrill et al., 2019). Structural-level barriers include the federal/provincial division of responsibility for healthcare services, socioeconomic conditions, colonization, oppression, racism, and intergenerational trauma (Horrill et al., 2019). Addressing the system and structural level barriers will require more initiatives that focus on self-governance and self-determination in healthcare, including political, social, or economic structures (Horrill et al., 2019).
Facilitators for accessing cancer care
Despite facing several barriers, Indigenous cancer survivors stressed the importance of support systems in accessing cancer care, including resources available in the family, community, culture, and First Nations and Métis health support services. The support systems for Indigenous cancer survivors are well documented in qualitative research, and the important role of the family is evident (Carr et al., 2020; Gifford et al., 2019; Roberts et al., 2020). In Witham and colleagues’ study, Indigenous patients, survivors, and family members highlighted the value of kinship (Witham et al., 2022). The authors identified that family could play an important role in providing support for those who need to travel to attend medical appointments by hosting family members and attending appointments with them (Witham et al., 2022). In a study with Indigenous patients with cancer and their families using an Indigenous method of sharing circles, participants emphasized the role of the family in “staying strong” for the survivor while also strengthening Indigenous identity and connection to culture (Carr et al., 2020). Therefore, family plays a large role in supporting Indigenous cancer survivors. However, Indigenous patient navigators can provide further support, especially when considering the complex barriers that patients experience in accessing healthcare.
Role of Indigenous patient navigators
Indigenous patient navigators could work to alleviate the challenges faced by Indigenous cancer survivors at the individual, system, and structural levels. At an individual level, the benefit of having an Indigenous patient navigator to help with language translation and explain medical terminology to patients was a major finding in this study. Several authors have claimed that Indigenous patient navigators could provide translation services and improve the overall communication experiences of Indigenous cancer survivors (Hiscock et al., 2022; Sheppard, 2019; Whop et al., 2012).
Similar to our study findings, Phillips et al. (2019) stressed the role of patient navigators in facilitating culturally sensitive cancer care. The authors found that patient navigators worked as intermediaries between patients and providers, transmitting information in both directions to promote a common understanding (Phillips et al., 2019). In a pilot study of an Indigenous patient navigator intervention in Queensland, Australia, most patients were “extremely satisfied” with the communication with the Indigenous patient navigator and their responsiveness to requests for support and guidance (Bernardes et al., 2018). Patients also reported extremely high satisfaction with the information (cancer pamphlets) and assistance provided in scheduling appointments with clinics or supportive services (Bernardes et al., 2018). Patients also testified that navigators also played a fundamental role in formulating some questions to be used at their subsequent doctor's appointment (Bernardes et al., 2018). Navigators have the ability to facilitate treatment options that are agreeable to patients, solve misunderstandings, and build a bridge to connect Indigenous and Western worldviews (Phillips et al., 2019). Across the Regional Cancer Programs (RCP) in Ontario, Indigenous navigators worked to meet cultural and spiritual needs of First Nations, Inuit, Métis and urban Indigenous survivors and families (Sheppard, 2019). For example, Indigenous navigators coordinated access to spiritual support and traditional medicines and connected patients with Elders and traditional knowledge keepers (Sheppard, 2019).
Participants in this study reported that Indigenous patient navigators could provide coordination services to assist in overcoming some of the logistical challenges faced by First Nations and Métis cancer survivors. For example, it highlighted the need for coordination in transportation, accommodation, and scheduling appointments. At a systems level, it has been claimed that Indigenous patient navigators should address the geographical barriers faced by many Indigenous communities (Rankin et al., 2022). The logistical support that Indigenous patient navigators can provide should not be overlooked, as shown in a study that conducted in-depth interviews with 40 American Indians/Alaska Natives (AI/AN) (Grimes et al., 2017). Participants most commonly relied on the navigator's services (most effective navigation services) to overcome logistic barriers, including housing, transportation, appointment scheduling, and completing paperwork (Grimes et al., 2017).
Another key aspect of coordination is to help patients locate solid support services and cope better with cancer. Indigenous patient navigators can help patients access First Nations and Métis healthcare services, mental health treatments, and support groups, also providing follow-up support in cancer treatment. Service coordination can help overcome significant healthcare system barriers to assure cancer and other conditions are timely diagnosed and treated (Burhansstipanov et al., 2015; Freeman, 2006). Kelly et al. (2019) identified in their scoping review that patient navigators can help patients and their caregivers find financial support/assistance. Additionally, patient navigators can provide psychosocial support for patients, including mental health, identity, and community supports.
Additionally, Indigenous patient navigators can provide education to cancer survivors. Given low health literacy levels reported in the Canadian population (Canadian Council on Learning, 2008; Szasz, 2023; Vamos, 2013), it is crucial that Indigenous cancer survivors receive adequate support with medical terminology and understanding of the disease and treatment. This support can help reduce the system and structural barriers experienced by Indigenous cancer survivors in healthcare.
Interestingly, some participants in our study stressed that the role of Indigenous patient navigators should be relational, meeting patients “at their level”. The need for a relational role of patient navigators is related to the fundamental aspects of working with Indigenous Peoples, which is to build relationships. In addition to cancer, many Indigenous cancer survivors have complex and traumatic personal stories and there is still mistrust in the medical system (Sheppard, 2019). Valuing family in the Indigenous worldview, involving family and community in decision-making, and respecting Indigenous ways of health healing are factors that may increase trust among Indigenous patients (Groot et al., 2020). Such factors should be considered in the relational and psychosocial support provided by Indigenous patient navigators to build trust and reduce anxiety and fear during the cancer care experience.
Our study results also speak to the advocacy and educational role that Indigenous patient navigators can play. A scoping review mapped the role of Indigenous patient navigators internationally within Canada, United States, Australia, and New Zealand (Rankin et al., 2022). The results showed that advocacy/building capacity was a key role of Indigenous patient navigators (Rankin et al., 2022). In this role, Indigenous patient navigators can educate patients, support communication with healthcare providers, and explain cultural practices to health professionals (Rankin et al., 2022). The advocacy work of Indigenous patient navigators will assure that the patient's needs, preferences, and perspectives are communicated and considered while navigating the Western healthcare system.
Limitations
Our study is limited by recall bias. As the inclusion criterion was that participants were cancer survivors from the past ten years, it could have been difficult for some participants to recall some of their experiences and imagine the role of patient navigators. To address this, the interview guide first invited participants to think about their general healthcare experiences before asking specific questions about patient navigation. Additionally, the small sample size prohibited the ability to make meaningful distinctions between patients who were currently undergoing treatment and those who had experienced treatment in the past. Consequently, the possibility of challenges specific to stages of the cancer journey was not explored. Further, the study was limited to Saskatchewan, a province where patient navigation programs for cancer survivors are lacking. Therefore, the results of this study may not be extrapolated to other Canadian provinces where cancer care navigation programs have been established. Finally, our results and discussion apply a pan-Indigenous approach. There has been a growing need for more Métis- and First Nations-specific studies that can understand the experiences of each population group separately and produce evidence that is tailored to each populations needs. However, although the results appeared similar, where possible, we attempted to depict the experiences of First Nations and Métis participants separately. Future studies could develop different interview questions that can capture the unique experiences and needs of First Nations and Métis navigating cancer care.
Conclusion
This study explored the perspectives of First Nations and Métis patients and survivors in Saskatchewan to better understand how an Indigenous patient navigator could improve aspects of their cancer journey.
Several challenges identified by participants included communication barriers, language barriers, logistical challenges, cultural differences, financial challenges, and gaps in care. On the other hand, the role of the community, family, traditional ways, and Métis and First Nations health services acted as supports throughout the cancer journey. Bridging the gaps between these challenges and supports could enhance the healthcare experiences of Indigenous cancer survivors.
Overall, participants explained that an Indigenous patient navigator would be beneficial to themselves and other survivors to ameliorate common barriers. A navigator could support survivors by connecting them to cultural, financial, and medical supports, translating information into Indigenous languages, and advocating for them. Indigenous navigators can also support patients and families by directing them to culturally appropriate care where available. In practice, we anticipate these findings will help to inform and guide culturally safe policies and services, including the implementation of an Indigenous patient navigator program for cancer care in Saskatchewan and beyond. Future studies could also evaluate the development and implementation of navigation programs for Indigenous cancer survivors in other jurisdictions.
Footnotes
Acknowledgements
We would like to thank all study participants for sharing their stories and insights. We would also like to thank the Irene & Leslie Dubé Centre of Care, the Saskatoon Surgical Oncology Groups, the Saskatchewan Cancer Agency, Métis Nation – Saskatchewan, and the Prince Albert Grand Council for their support during recruitment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Saskatchewan Health Research Foundation (SHRF) 4518 Establishment Grant.
Saskatchewan Health Research Foundation, (grant number 4518 Establishment Grant.).