
Abstract
Background
Maternal tobacco smoking during pregnancy is associated with adverse health effects for the woman, fetus, and child, including such serious effects as preterm birth, low birth weight, stillbirth, and neonatal and sudden infant death. Smoking cessation during pregnancy reduces health risks.
Purpose
In order to support pregnant women to quit smoking, it is essential to know determinants of quitting smoking in pregnancy. The purpose of this research was to examine women's understanding of maternal smoking, in terms of their beliefs, in relation to quitting smoking during pregnancy.
Methods
The study was a cross-sectional survey with anonymous questionnaires. The sample consisted of 161 pregnant and postnatal women who were continuing or had continued to smoke during pregnancy or had quit smoking during pregnancy. Logistic regression was used to determine the impact of women's understanding of maternal smoking on quitting smoking in pregnancy.
Results
A large majority of the women had low to moderate understanding of maternal smoking. Those with higher levels of understanding were more likely to quit smoking during pregnancy than were those with a low level of understanding. Not having children prior to the current pregnancy or childbirth also increased the likelihood of quitting smoking during pregnancy while being without a partner combined with having a longer duration of smoking decreased the likelihood of quitting smoking during pregnancy.
Conclusion
As a modifiable factor, pregnant women's understanding of maternal smoking can be readily targeted with informational interventions in an effort to help them quit smoking.
Background and purpose
Maternal tobacco smoking during pregnancy (MSDP) is a major public health concern (Bauld & Onchen, 2017). It is well established that smoking causes serious general health effects, including cardiovascular, cerebrovascular, and respiratory diseases and numerous types of cancer. In fact, smoking adversely affects nearly every organ in the body (United States Department of Health and Human Services [USDHHS, 2020]). It is a leading cause of morbidity and mortality worldwide (World Health Organization [WHO], 2021). MSDP poses additional serious risks: (a) pregnancy complications (i.e., ectopic pregnancy, premature rupture of membranes, placenta abruption and previa), (b) preterm delivery, (c) growth restriction and low infant birth weight, (d) stillbirth, (e) neonatal death, (f) sudden infant death, (g) cleft lip and palate, and (h) impaired lung function in infants (USDHHS, 2014). MSDP is also associated with (a) congenital disorders, such as clubfoot, gastroschisis, and heart defects; (b) childhood disruptive behavioral disorders, in particular, attention deficit and hyperactivity disorder (USDHHS, 2014); and (c) childhood overweight and obesity (Albers et al., 2018; Ino, 2010). Other effects of MSDP include intergenerational transmission of smoking and negative impact on maternal psychological health. MSDP increases the likelihood of smoking onset (Miles & Weden, 2012) and tobacco addiction among offspring (De Genna et al., 2017). Women who smoke during pregnancy experience feelings such as stress, anxiety, guilt, and shame as a result of knowing that their smoking could be harmful to the unborn baby and that smoking during pregnancy is socially unacceptable (Flemming et al., 2013; Goszczyńska et al., 2016; Wigginton & Lee, 2013).
In Canada, national data indicate a prevalence rate of 8.2% for MSDP (Centre for Surveillance and Applied Research [CSAR] / Public Health Agency of Canada [PHAC], 2020). In other high-income countries (HIC), similar rates of MSDP have been reported. For example, national data indicate prevalence rates of approximately 7% for the United States (Azagba et al., 2020) and 9% each for England (National Health Service [NHS], 2022) and Australia (Australian Institute of Health and Welfare [AIHW], 2022). In contrast, a national prevalence rate of 16.2% has been reported for France (Demiguel et al., 2021). Based on a pooled-prevalence study, several other HICs (e.g., Uruguay, Spain) had estimated prevalence of MSDP in excess of 20% (Lange et al., 2018). There is limited evidence about MSDP in low- and middle-income countries (LMIC). Studies in which prevalence data were pooled across a number of LMICs indicated rates of MSDP at 0.69% (Shukla et al., 2021) and 1.3% (Caleyachetty et al., 2014). LMICs are earlier in the epidemiology of tobacco smoking than are HICs. It is expected that MSDP will rise in LMICs with economic development and as a result of tobacco industry marketing, such as happened in HICs (Shukla et al., 2021).
It is important to note that population level prevalence of MSDP does not reveal differences in prevalence in subgroups of a population. In particular, specific regions within a country (e.g., provinces, states, geographical areas) may have considerably higher prevalence than indicated by national rates (AIHW, 2022; Daley & Phipps, 2021; Drake et al., 2018; NHS, 2022). For instance, within Canada, some provinces and territories have higher rates of MSDP than the national average. This includes the province of Newfoundland and Labrador with a recent prevalence of 12%. That rate is also high when compared with some other Canadian provinces, such as Ontario at 6.7% and British Columbia at 5.3% (CSAR / PHAC, 2020). Furthermore, prevalence of MSDP is generally higher in rural compared with urban locations (Al-Sahab et al., 2010; Nighbor et al., 2018). Within NL, past research in some rural areas indicated rates of 18% to 24% (Perinatal Program NL, 2013a, 2015). Of further concern is that typically, smoking rates for pregnancy are determined by self-report and therefore may be under-estimations of actual maternal smoking. It is well established that pregnant women may misrepresent their smoking status. As many as one-third of pregnant women who reported not smoking were considered to be actively smoking based on biochemical testing (Ashford et al., 2017; Emery et al., 2017). Reluctance to divulge their smoking may be a result of the psychological difficulty they experience because of their smoking in pregnancy (Wigginton & Lee, 2013).
There is substantial evidence that smoking cessation during pregnancy benefits the health of the woman, fetus, and child (USDHHS, 2020). Yet, quit rates in pregnancy are generally low to moderate across countries (Demiguel et al., 2021; Schilling et al., 2018); for example, from 23% in Australia (AIHW, 2022) to 54% in the United States (Rockhill et al., 2016). In Canada, a national quit rate of 53% has been reported (PHAC, 2016). In groups of women with particular characteristics, quit rates in pregnancy tend to be low (Gilbert et al., 2015; Riaz et al., 2017). For example, a quit rate of 25% was reported for women attending healthy baby clubs (HBCs) in NL (Perinatal Program NL, 2013b). HBCs are government funded programs for pregnant and postnatal women who may need extra support (e.g., prenatal and postnatal education, nutrition and breastfeeding assistance, baby supplies) to strengthen health outcomes.
Based on quit rates, it is apparent that many women continue to smoke into the postnatal period. Of women who quit smoking during pregnancy, from 36% to 82% across countries have been found to recommence smoking within a year after childbirth (Rockhill et al., 2016; Scheffers-van Schayck et al., 2019; Schilling et al., 2018). In Canada, a national postnatal relapse rate of 47% has been reported (PHAC, 2016). As with MSDP, maternal tobacco smoking postnatally (MSPN) is also associated with negative health consequences. For instance, children who are exposed to parental secondhand smoke are at increased risk of sudden infant death, impaired lung function, and acute and chronic respiratory and middle ear conditions (e.g., asthma, otitis media) (USDHHS, 2014). MSPN is also associated with a reduced rate of breastfeeding initiation and with early weaning from breastfeeding (Weiser et al., 2009; Wijndaele et al., 2009). Similar to MSDP, MSPN is associated with increased likelihood of smoking onset in offspring (Miles & Weden, 2012) and with negative psychological states in the women (Bottorff et al., 2000). Such states include worrying about possibly exposing their babies to tobacco contaminants in their breast milk, fearing being stigmatized as not good mothers, and feeling guilt about being negative role models and thereby putting their children at risk for future smoking.
In order to support pregnant women to quit smoking, it is essential to know determinants of quitting smoking in pregnancy. To that end, a myriad of influencing factors have been identified. For instance, women were less likely to quit smoking during pregnancy if they (a) had exposure to a partner, household member, or others who smoked; (b) had higher tobacco dependence; (c) were younger at smoking initiation; (d) had higher levels of stress (Riaz et al., 2017); and (e) had an unwanted pregnancy (Gilbert et al., 2015). Similar to the latter finding, another emotional response found to predict smoking in pregnancy is lack of maternal positive acceptance of the pregnancy (Širvinskienė et al., 2016). There is inconsistency in findings on maternal age, but in a number of studies older age was also associated with a lower likelihood of quitting smoking during pregnancy (Riaz et al., 2017). Women were more likely to quit smoking during pregnancy if they (a) had higher socio-economic status, including higher education, higher income, and current employment; (b) had a partner (married or cohabiting); (c) had support from a partner or others; (d) had smoked for a shorter duration of time; (e) were primiparious; (f) had intended to breastfeed; (g) had a planned pregnancy; and (h) had adequate prenatal care (e.g., early care, more prenatal visits) (Riaz et al., 2017).
Another factor considered important to MSDP is pregnant women's understanding (i.e., beliefs, perceptions, awareness, knowledge) of maternal smoking. Qualitative and quantitative research findings indicate that women who smoked during pregnancy had limited understanding of maternal smoking, perceived low harmfulness of the behavior, or had misbeliefs about it. For instance, generally, pregnant women who smoked were aware of the broad health facts; that is, smoking during pregnancy is potentially harmful to the unborn child (Emery et al., 2017; Levis et al., 2014; Naughton et al., 2013; Wen et al., 2015) and postnatal exposure of the child to secondhand smoke can cause health problems for the child (Mohsin et al., 2007; Naughton et al., 2013; Wen et al., 2015). However, many tended to not be aware of specific health effects of MSDP (e.g., preterm delivery, low birth-weight, sudden infant death, orofacial clefts, behavioral problems) and MSPN (e.g., impact on breastfeeding, effects on child's health) or tended to minimize the risk of specific health effects (Bauld et al., 2017; Dobbs et al., 2020; Griffiths et al., 2005; Mohsin et al., 2007; Naughton et al., 2013; Wen et al., 2015). Women also tended to lack awareness about the importance of smoking cessation and the methods to assist smoking cessation when pregnant, including pharmacotherapy (Goszczyńska et al., 2016; Naughton et al., 2013). Misbeliefs held by pregnant women who smoked during pregnancy, as revealed in their narrative accounts of their experiences, include these examples: (a) cutting down rather than quitting smoking (or quitting cold turkey) is better for the unborn baby, (b) withdrawal symptoms from quitting may be harmful to the unborn baby, (c) the stress of quitting smoking may be more harmful to the unborn baby than smoking (Graham et al., 2014; Small & Porr, 2022), (d) smoking a low number of cigaretes is safe for the unborn baby, (e) smoking is safe during the first trimester (Goszczyńska et al., 2016), and (f) smoking cigaretes during pregnancy is no more harmful than using the patch (i.e., nicotine replacement therapy) (Naughton et al., 2013). Factors that have been identified as negatively influencing pregnant women's knowledge of maternal smoking are low income (Oechsle et al., 2020) and low education (Esposito et al., 2015).
Few studies were found in which women's understanding of maternal smoking was examined as a factor influencing quitting smoking during pregnancy. Furthermore, findings from those studies are limited by use of single items to measure women's understanding. Nevertheless, the findings revealed that women who disagreed that quitting smoking during pregnancy reduces risk were more likely to be smoking during pregnancy than to have quit smoking during pregnancy (Meghea et al., 2012). As well, women who believed that MSDP will greatly harm the baby (White et al., 2014) or believed that MSDP poses risk to the fetus (Grangé et al., 2006) were more likely to quit smoking during pregnancy than were women who did not hold those beliefs.
Given the serious health effects of MSDP and the limited research on pregnant women's understanding of MSDP as a factor predicting quitting smoking during pregnancy, more research is warranted to further examine that factor. As a modifiable factor, pregnant women's understanding of maternal smoking can be readily targeted with nursing interventions to address informational needs. Hence, the purpose of this research was to address two questions: (a) What is the understanding of women who smoke in pregnancy and women who quit smoking in pregnancy in relation to maternal smoking (i.e., impact, specific harms, smoking cessation in pregnancy and postnatally)? (b) Is women's understanding about maternal smoking associated with quitting smoking during pregnancy? The focus of this research was part of a larger study (Small et al., 2020) to examine various aspects of maternal smoking in NL, a province with a relatively high rate of MSDP. No studies were found in which the subject of this paper, women's understanding of maternal smoking, had been examined in NL.
Methods and procedures
Research design and ethics approval
The study was carried out using a cross-sectional survey design and the data were gathered through anonymous questionnaires. The study was approved by the provincial Health Research Ethics Board. Information about the study, including purpose, voluntary participation, and participant rights, was provided to the participants. Participant consent was assumed by completion and submission of the questionnaire. Each participant was given a $30.00 retail gift card after returning the questionnaire.
Setting, recruitment, and sampling
The study took place in NL, specifically the island of Newfoundland. Women were recruited to the study through family resource centers (FRCs). These are community-based facilities that offer a variety of programs and services, including HBCs, to pregnant and postnatal women and to families with young children. Of 24 possible FRCs, women were recruited through 14, which represented all geographical regions of Newfoundland, including rural and urban locations. FRC personnel provided information about the study to women attending the FRCs. Women were invited to complete a questionnaire if they (a) expressed an interest in the study and were 16 years of age or older and (b) self-identified as pregnant and currently smoking or had quit smoking in the present pregnancy or self-identified as being within one year post-childbirth and currently smoking or had smoked during that pregnancy but was currently nonsmoking.
One hundred and eighty questionnaires were distributed to potential participants for the larger study. One hundred and seventy-five were returned for a response rate of 97%. Of those 175 women, 161 met the eligibility criteria for the focus of this paper concerning the influence of women's understanding of maternal smoking on quitting smoking during pregnancy. The N = 161 was considered adequate on the basis of sample size calculation. A minimum sample size of N = 146 was targeted to detect an effect size of 0.5 difference in understanding between women continuing to smoke during pregnancy and women who had quit smoking during pregnancy. The following were taken into consideration: (a) statistical power of 80%, (b) type I error rate of 0.05, (c) 17-item instrument to measure understanding, (d) plan for two-samples t test, (e) quit rate in pregnancy estimated at 25%, and (f) an additional 10% participants to account for possible missing values. The 161 women consisted of both pregnant and postnatal (within one year of childbirth) women who smoked in pregnancy, with some having quit smoking in pregnancy. More specifically, the women were (a) pregnant (n = 120) and currently smoking in pregnancy (n = 81) or had quit smoking in the present pregnancy and were currently nonsmoking (n = 39) and (b) postnatal (n = 41) and had smoked throughout the most recent pregnancy (n = 29) or had quit smoking during that pregnancy and remained nonsmoking during pregnancy (n = 12). In total, there were 110 women who were continuing or had continued to smoke during pregnancy and 51 who had quit smoking during pregnancy.
Data collection and analysis
The questionnaires had modified wording according to whether participants were pregnant or postnatal and currently smoking or had quit smoking. There were 40 to 42 main questionnaire items with some items consisting of groups of related questions. The questionnaires were developed by the research team based on a review of the literature and the team's expertise in the subject area and experience in questionnaire construction. The questionnaires were reviewed by an external professional, who was an expert in the field of smoking and smoking cessation, and by a FRC employee, who was an experienced support person for pregnant and postnatal women attending the FRC. The reviewers considered the questionnaires to be suitable in terms of content and clarity of wording. The questionnaires achieved a Flesch-Kincaid reading ease of 78 and a grade level of 5. During a trial period at the beginning of data collection, there were no difficulties reported by the individual women, who completed the questionnaires, in terms of understanding or completing the questionnaires.
Items on the questionnaires relevant to this paper were about participant characteristics (see Table 1) and participant understanding concerning maternal smoking (see Table S1, Supplementary material). The characteristics pertained to (a) socio-demographics (i.e., age, relationship status, number of children, education level, employment status, household income level), (b) pregnancy (i.e., pregnancy and postnatal length, first prenatal visit period, pregnancy wanted, pregnancy happiness), (c) breastfeeding (i.e., planning to breastfeed or had breastfed the current baby), and (d) smoking (i.e., age at smoking initiation, duration of smoking, nicotine dependence). Most questionnaire items were formatted as fill-in-the-blank or multiple choice. Nicotine dependence was measured by the six questions from the Fagerstrom Test for Nicotine Dependence (with permission of K. O. Fagerstrom). That instrument has been validated in prior research (Heatherton et al., 1991) and used extensively in studies on smoking. The questions on the instrument have set response choices. The total score ranges from 0 to 10, with scores of 0 to 2, 3 to 4, 5, 6 to 7, and 8 to 10 indicating very low, low, medium, high, and very high nicotine dependence, respectively (Fagerstrom et al., 1990). Understanding of maternal smoking was measured by 17 true and false statements about impact, health effects, and smoking cessation in relation to smoking in pregnancy and smoking postnatally. Nine statements were true and eight were false, based on prevailing knowledge in the literature. Participants were asked to indicate whether they believed each statement to be true or to be false. Possible total scores, based on correct responses, were 0 to 17.
Characteristics of the sample and understanding of maternal smoking scores.
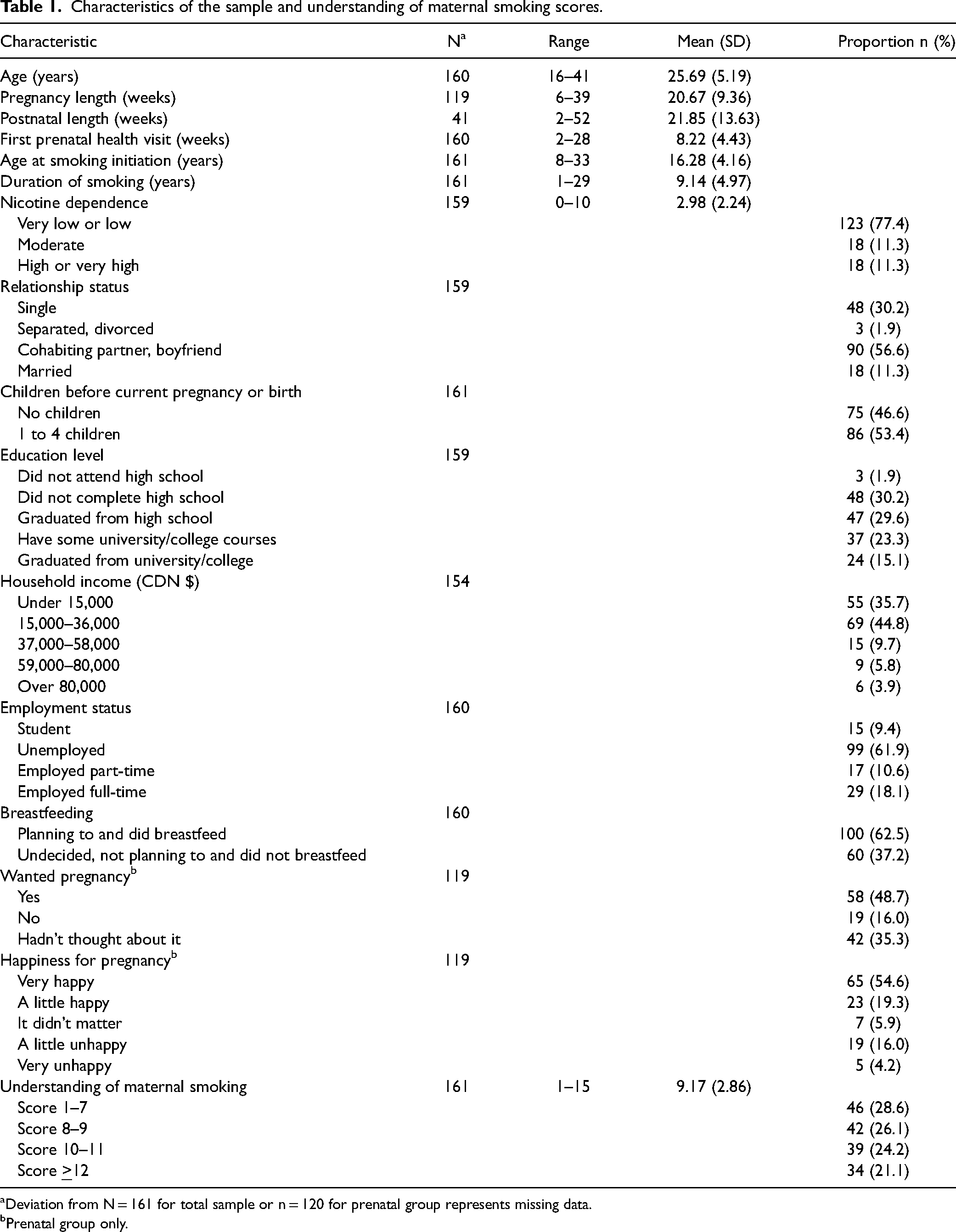
Deviation from N = 161 for total sample or n = 120 for prenatal group represents missing data.
Prenatal group only.
The data from the questionnaires were entered into and analysed with the Statistical Package for the Social Sciences (SPSS). The accepted level of statistical significance was p < .05. The characteristics of the sample and understanding of maternal smoking were analysed descriptively using ranges, means, frequencies, and percentages, as suitable for the data type, with valid percentages reported (see Table 1 and Table S1 [Supplementary material]). Pearson's Chi-squared and t test were used as appropriate to examine factor associations with quitting smoking during pregnancy (see Table 2). Logistic regression was used to determine the impact of women's understanding of maternal smoking on quitting smoking in pregnancy (see Table 3). The backward model selection method was used to select predictors from the factors examined in the bivariate analyses (see Table 2) and to determine predictor interactions. Income level and happiness for pregnancy were chosen as potential predictors and employment status and wanted pregnancy were excluded. That decision was made for these reasons: (a) income and employment would be associated and employment status had a smaller N (due to some participants having student status) and (b) happiness for pregnancy and wanted pregnancy are conceptually similar and the bivariate analysis indicated that wanted pregnancy had few participants in one category. The probability of retaining predictors in the model was 0.35, with age, first prenatal visit, income level, and happiness for pregnancy removed in the backward selection. Six women (3.7% of the sample) were removed from the logistic regression due to missing data. The final model included understanding levels, age at smoking initiation, duration of smoking, nicotine dependence, relationship status, number of children, education level, and breastfeeding, as well as the interaction between relationship status and duration of smoking, where duration of smoking was centered. Multicollinearity was checked and collinearity was not of concern because all variance of inflation factors were less than 4 in the final model. The Hosmer-Lemeshow goodness of fit test indicated a valid model (p = .271).
Bivariate analyses of differences between continuing smoking and quitting smoking during pregnancy.
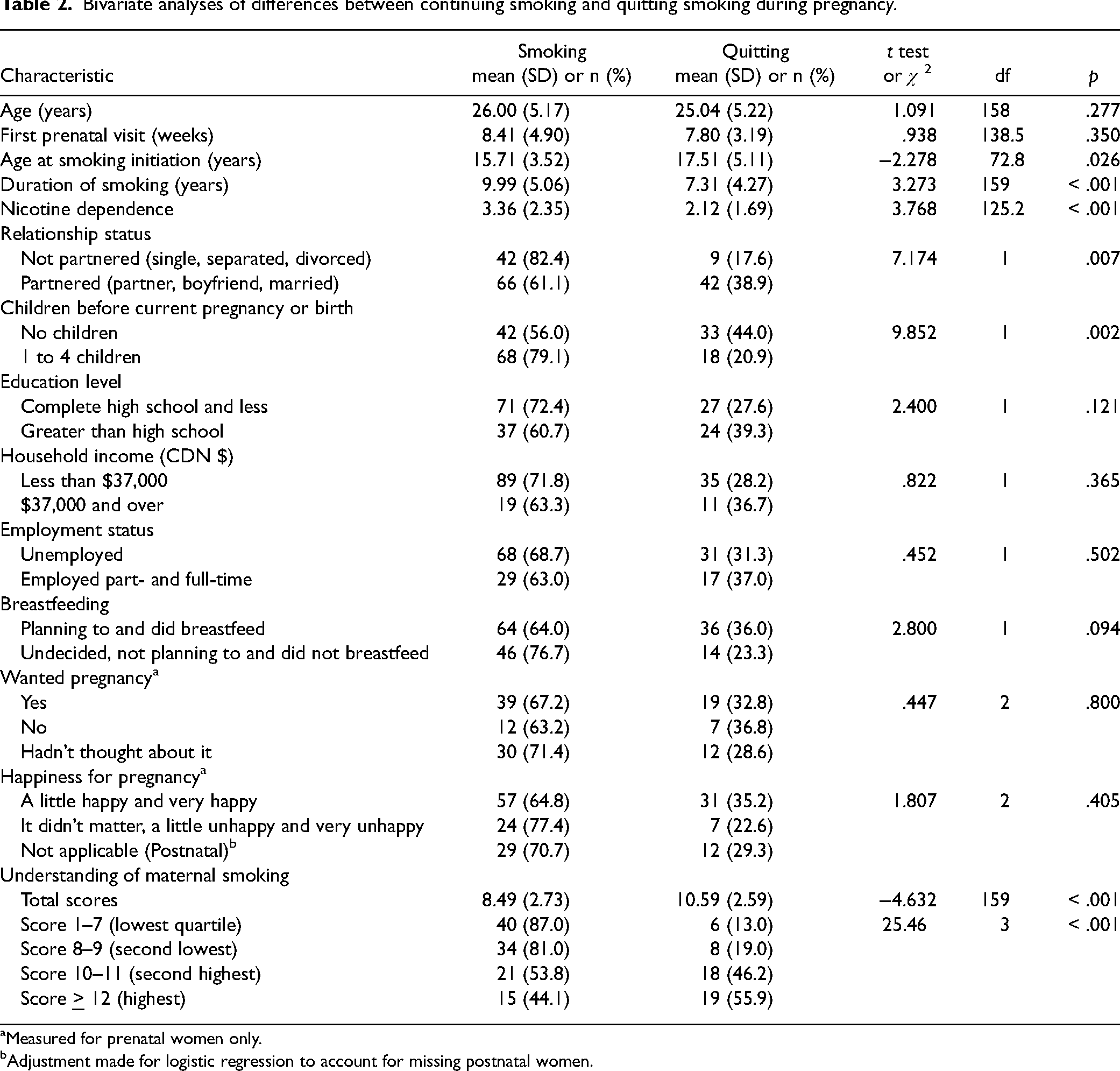
Measured for prenatal women only.
Adjustment made for logistic regression to account for missing postnatal women.
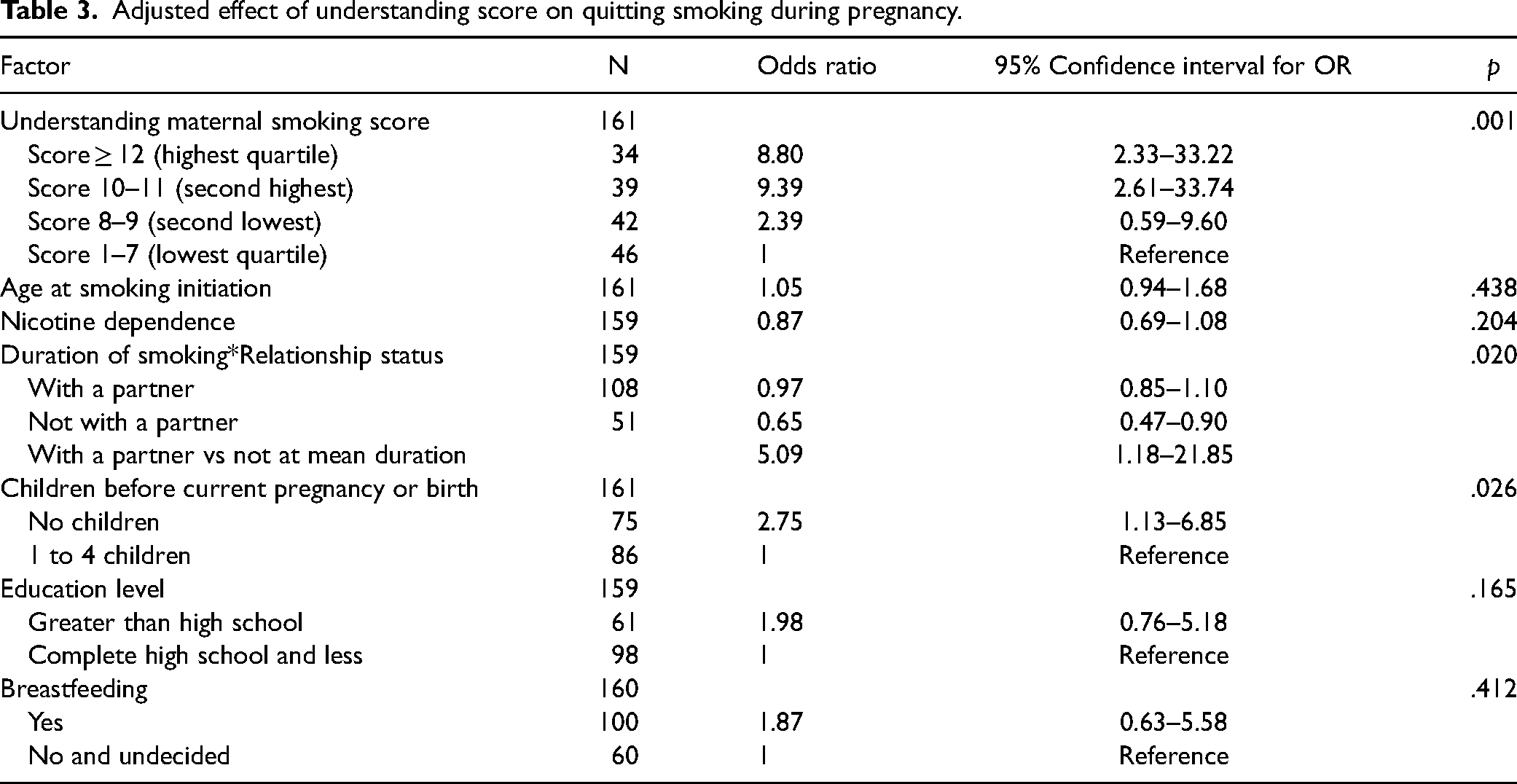
Adjusted effect of understanding score on quitting smoking during pregnancy.
Exploratory analyses were conducted to identify factors potentially associated with women's understanding of maternal smoking, given the little information in the literature on influencing factors. Spearman correlation and t test analyses were conducted using characteristics of the sample (see Table S2, Supplementary material).
Results
A full description of the sample characteristics is provided in Table 1. The women were on average 26 years of age. Most (68%) were in a relationship as married or living with a partner or boyfriend. Just less than half (47%) of the women did not have children prior to the current or most recent pregnancy and 53% of the women had 1 to 4 children previously. Sixty-two percent of the women had an education level of high school graduate or less. More than a third of the women (36%) reported a household income of less than CDN $15,000 and a large majority (81%) had a household income of less than CDN $36,000. Most women (62%) were unemployed.
The women were, on average, 21 weeks pregnant or 22 weeks postnatal at the time of completing the questionnaires. Most women had their first prenatal health visit within trimester one of pregnancy, at a mean of 8 weeks. When they found out they were pregnant, 16% did not want to be pregnant and 20% were a little to very unhappy about being pregnant. Sixty-three percent of the pregnant women intended to breastfeed their babies and 63% of the postnatal women had breastfed their babies. The women had been 16 years of age, on average, when they first began to smoke and had been smoking for a mean of 9 years. The majority of women (77%) had low to very low nicotine dependence (mean 2.98) when they were smoking during pregnancy.
Based on the bivariate analyses, several factors were associated with quitting smoking during pregnancy (see Table 2). Women were more likely to quit smoking if they had any of the following characteristics: older age at smoking initiation, shorter duration of smoking, and less nicotine dependence. As well, they were less likely to quit smoking during pregnancy if they were not in a partnered relationship (i.e., were single, separated, divorced) or if they were multiparous (i.e., had 1 to 4 children prior to the current pregnancy or current childbirth).
The women's understanding of maternal smoking is presented in Table S1 (Supplementary material). Almost all of the women (99.4%) responded to at least 10 of the 17 true or false statements about maternal smoking (one responded to only seven statements) and 94% responded to 15 or more statements. Correct scores ranged from 1 to 15 with a mean of 9. Fifty-five percent of the women had scores of 9 or less and 79% had scores of 11 or less, indicating that a large majority of the women had low to moderate understanding of maternal smoking. Low understanding of some specific outcomes of smoking during pregnancy, in particular, less maternal weight gain and the child effects of orofacial clefts and overweight, was notable. Only 10 to 29% of the women had accurate beliefs about these potential effects. Although considerably more women (63%) believed that babies may be small as a result of smoking during pregnancy, still 37% of women appeared to not know this long standing fact. Misbeliefs about smoking and quitting smoking during pregnancy were also common. As many as 30 to 64% of women believed the following statements to be true: (a) “smoking only a little during pregnancy is okay” (30%); (b) “it is harmful to the baby to quit smoking “cold-turkey” while pregnant” (64%); (c) “it is better to cut down smoking than to quit smoking in pregnancy” (47%); (d) “feeling stressed during pregnancy is more harmful to the baby than is smoking” (61%); and (e) “if you are going to quit smoking, it needs to be in the first half of the pregnancy to help the baby” (46%). Women's understanding of postnatal smoking seemed to be better. Fifty-six to 73% of women believed correctly the following to be true: (a) “mothers who smoke will have nicotine in their breast milk” (68%), (b) “children of mothers who smoke are more likely to have ear infections and asthma” (56%), and (c) “smoking around babies can lead to sudden infant death” (73%). Seventy-five to 95% believed correctly the following to be false: (a) “it is okay to smoke in the house as long as the smoking is away from the baby” (95%) and (b) “there is no sense in the mother quitting after the baby is born if she smoked during pregnancy” (75%). Similarly, most women (53 to 81%) had correct understanding of pharmacotherapy for smoking cessation. They believed true that (a) “women who have just had a baby can take Zyban or Champiz to help them quit smoking if they are not breastfeeding” (58%) and (b) “nicotine gum can be used to quit smoking during pregnancy if the doctor advises it” (53%). They believed false that “the nicotine patch is the best way for a breastfeeding mother to try to quit smoking” (81%).
Based on the bivariate analyses, a greater understanding of maternal smoking was associated with quitting smoking during pregnancy (see Table 2). The logistic regression analysis revealed that understanding levels remained significantly associated with quitting smoking (p = .001) after adjusting for the following: (a) age at smoking initiation, (b) duration of smoking, (c) nicotine dependence, (d) relationship status, (e) number of children, (f) education level, and (g) breastfeeding (see Table 3). Women with understanding scores in the highest and second highest quartiles were more likely to quit smoking than were those with understanding scores in the lowest quartile. The odds ratios of quitting smoking were 8.80 (95% CI: 2.33–33.22) and 9.39 (95% CI: 2.61–33.74), respectively. There was not a significant difference in quitting smoking between women in the second lowest and those in the lowest quartile of knowledge scores (OR 2.39 and 95% CI: 0.59–9.60). The likelihood of being in the quit smoking group for women with no children prior to the current or most recent pregnancy was higher than for those with previous children (OR 2.75 and 95% CI: 1.13–6.85). The interaction between duration of smoking and relationship status was significant (p = .020). Women without a partner who smoked for a longer period were less likely to quit smoking than were women with a partner regardless of duration of smoking in the partnered group (OR 0.65 and 95% CI: 0.47–0.90). Although age at smoking initiation and nicotine dependence were related to quitting smoking in the bivariate analyses, the effects of those factors on quitting smoking became not significant after adjusting for knowledge levels and other factors in the model. Education level and breastfeeding remained not significant in logistic regression.
On exploratory examination, two factors were revealed as associated with women's understanding of maternal smoking (see Table S2, Supplementary material). Women who were less nicotine dependent (compared with women who were more nicotine dependent) and women who were planning to breastfeed or had breastfed their infants (compared with women who were not considering breastfeeding or had not breastfed) had more correct responses to the statements about smoking in pregnancy and smoking postnatally.
Discussion
Overall, many women in this study had low to moderate understanding of maternal smoking. In particular, many women did not know of specific effects of smoking in pregnancy, such as child orofacial clefts and overweight, and many held misbeliefs about smoking and quitting smoking during pregnancy. In general, women's understanding of postnatal smoking and smoking cessation pharmacotherapy seemed to be better, with most women indicating correct understanding. Still there were women with responses indicating incorrect understanding of such information. Of prime importance is that women's understanding of maternal smoking was strongly associated with quitting smoking in pregnancy. Women with higher rather than lower understanding were more likely to quit. These findings are consistent with findings from previous studies. Women who smoked during pregnancy had limited understanding of maternal smoking, including about specific health effects and smoking cessation, and had misbeliefs about smoking and quitting smoking in pregnancy (Bauld et al., 2017; Dobbs et al., 2020; Goszczyńska et al., 2016; Graham et al., 2014; Griffiths et al., 2005; Mohsin et al., 2007; Naughton et al., 2013; Small & Porr, 2022; Wen et al., 2015). Furthermore, pregnant women who believed that MSDP carries risk and is harmful to the unborn baby had increased likelihood of quitting smoking during pregnancy (Grangé et al., 2006; Meghea et al., 2012; White et al., 2014).
In this study, less nicotine dependence and breastfeeding (planned and actual) were associated with greater understanding of maternal smoking. Explanations for such associations were not examined but it may be that less nicotine dependence makes it easier for women to consider quitting smoking and therefore easier to seek or be open to information about maternal smoking. Whereas, it may be that higher nicotine dependence makes it harder for women to consider quitting smoking and thereby inhibits efforts to access information or inhibits openness toward information about maternal smoking. Similarly, it may be that intent to breastfeed and actual breastfeeding motivates pregnant women to learn about the harm of maternal smoking for the breastfed baby and how to avoid it. In this study, other factors, including income and educational levels, were not associated with women's understanding of maternal smoking. This is inconsistent with prior findings that low income and low education had a negative impact on pregnant women's knowledge of maternal smoking (Esposito et al., 2015; Oechsle et al., 2020).
In addition to understanding of maternal smoking, various other factors were examined in this study for effect on quitting smoking during pregnancy. Being without a partner in combination with longer duration of smoking predicted less likelihood of quitting smoking during pregnancy. As well, not having children prior to the current or most recent pregnancy predicted increased likelihood of quitting smoking. This is consistent with findings in previous studies whereby having a partner, having smoked for a shorter duration of time, and being primiparious were predictors of quitting smoking in pregnancy (Riaz et al., 2017). However, other variables examined in this study (i.e., age, time period of first prenatal visit, age at smoking initiation, nicotine dependence, education level, household income, breastfeeding, happiness for pregnancy) did not have an effect on quitting smoking. In previous studies, similar variables had been shown to predict smoking cessation in pregnancy (Gilbert et al., 2015; Riaz et al., 2017).
Study limitations and strengths and implications for practice and research
The lack of significant associations between variables in this study may be due to study limitations. The homogeneity in the sample (i.e., convenience recruitment of participants through family resource centers, high proportion of socioeconomic disadvantage among the participants) and the relatively small sample size may have precluded all but the strongest associations from reaching statistical significance. Those limitations prohibit generalization of the findings at the population level. The questionnaires used in this study were new and without established psychometric properties. However, the questionnaires were (a) based on a literature review and known facts about maternal smoking, (b) developed by a research team with expertise in the substantive area and experience in questionnaire construction, (c) externally reviewed for content and readability, (d) at an appropriate reading level, and (e) trialed with study participants. That may have strengthened questionnaire validity and reliability. Smoking status in this study was self-reported and it is well acknowledged that self report of smoking status in pregnancy may not be accurate. But, the questionnaires were completed anonymously, which may have enabled the women to respond freely to the questions. The anonymous questionnaires and high participant response rate may have strengthened the findings of the study. Nevertheless, representative and larger samples, psychometrically tested questionnaires, and biochemical validation of maternal smoking would better future research.
Despite study limitations, the findings of this study contribute to what was known about women's understanding of maternal smoking and have implications for practice. Possible reasons for women's restricted understanding of maternal smoking, including having misbeliefs, are apparent in other research. Pregnant and postnatal women lacked initiative in accessing information about smoking and quitting smoking in pregnancy (Small et al., 2020). Women who smoke during pregnancy may not look for such information because of the cognitive dissonance and psychological difficulty they would experience in knowing the facts about the harmfulness to the baby of smoking in pregnancy and in knowing they should not smoke during pregnancy while being unable to quit smoking (Naughton et al., 2013; Wigginton & Lee, 2013). Furthermore, health care providers may fail to offer women who smoke in pregnancy adequate information about smoking and quitting smoking in pregnancy (Baxter et al., 2010). Women have reported that the topic of smoking in pregnancy was not raised by HCPs in their prenatal visits. Other women have reported that aside from being told smoking in pregnancy could be harmful to the baby or that they should quit smoking, they were not given details about the harm, information about how to quit, or information about resources or pharmacotherapy to assist quitting (Small et al., in press). By not intervening and not intervening fully, HCPs miss an opportunity to help pregnant women to quit smoking. Furthermore, by providing misinformation or inappropriate advice about smoking and quitting smoking in pregnancy, HCPs may be a source of women's misbeliefs about smoking and quitting smoking in pregnancy (Small et al., in press). HCPs have identified time and other resource constraints and inadequate knowledge and skills for smoking cessation interventions as barriers to their provision of appropriate support to women who smoke in pregnancy (Baxter et al., 2010).
Based on the findings from this study and in accordance with clinical practice guidelines (e.g., American College of Obstetricians and Gynecologists, 2020; National Institute for Health and Care Excellence, 2022), it is essential that HCPs routinely offer interventions to assist pregnant women to quit smoking. HCPs should assess pregnant women's understanding of maternal smoking; dispel any misbeliefs; and provide comprehensive information about harms of smoking (i.e., to the woman, fetus, and child) and about pharmacotherapy and resources (e.g., group, internet, or helpline support; digital aids) that may be used to assist quitting. HCPs should also assess pregnant women who smoke for other factors that may impede smoking cessation, including already having children and non-partner status, as identified in this study, and provide smoking cessation interventions with tailored support at every health care encounter. For women with children, it is imperative to discuss with them the harmful effects of secondhand smoke and the importance of preventing their children's exposure to it. There is evidence in the literature that pregnant women who smoke expect that HCPs will address their smoking (Small et al., in press). There is also evidence that psychosocial interventions are facilitative of smoking cessation in pregnancy (Chamberlain et al., 2017). Hence, HCPs should ensure that they have the necessary time to address smoking with pregnant women and have requisite knowledge and skills to intervene appropriately. Health care policy makers should ensure that HCPs have adequate resources for smoking cessation care in pregnancy. Nurses are ideally situated to promote smoking cessation among pregnant women and support the women in their efforts to quit smoking. Nurses have competencies in health education and psychosocial interventions, subscribe to patient-centeredness and individualized care, and have contact with pregnant women through the many settings in which they provide maternity care (e.g., prenatal health clinics, prenatal education classes, inpatient units, community).
More research is warranted to continue to strengthen the knowledge base concerning the influence of women's understanding of maternal smoking on their quitting smoking during pregnancy. As well, research is needed to further examine factors associated with pregnant women's understanding of maternal smoking.
Conclusion
In this study, many women who smoked during pregnancy had low to moderate understanding of maternal smoking in that often their beliefs about smoking and quitting smoking in pregnancy and postnatally were inconsistent with known facts. Furthermore, women's understanding of maternal smoking strongly predicted quitting smoking in pregnancy. Pregnant women's understanding of maternal smoking is a modifiable risk factor. Therefore, it is essential that HCPs intervene by offering pregnant women who smoke comprehensive information about smoking and quitting smoking in pregnancy and postnatally. HCPs should also be aware of other barriers to quitting smoking during pregnancy and provide interventions to address such barriers. Because of their competencies and relational approach and the opportunity afforded them in maternity nursing practice, nurses are particularly well positioned to addressing smoking with pregnant women in an effort to assist them to quit smoking.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621221125062 - Supplemental material for The Understanding of Maternal Smoking among Women who were Smoking or had Quit Smoking during Pregnancy
Supplemental material, sj-docx-1-cjn-10.1177_08445621221125062 for The Understanding of Maternal Smoking among Women who were Smoking or had Quit Smoking during Pregnancy by Sandra Small, Andrea Brennan-Hunter, Yanqing Yi and Caroline Porr in Canadian Journal of Nursing Research
Supplemental Material
sj-docx-2-cjn-10.1177_08445621221125062 - Supplemental material for The Understanding of Maternal Smoking among Women who were Smoking or had Quit Smoking during Pregnancy
Supplemental material, sj-docx-2-cjn-10.1177_08445621221125062 for The Understanding of Maternal Smoking among Women who were Smoking or had Quit Smoking during Pregnancy by Sandra Small, Andrea Brennan-Hunter, Yanqing Yi and Caroline Porr in Canadian Journal of Nursing Research
Footnotes
Acknowledgement:
Cynthia Murray RN, PhD participated in the conception and design of the study; Joanne Smith-Young RN, PhD(c) coordinated participant recruitment and data collection and conducted data entry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded by the Newfoundland and Labrador Centre for Applied Health Research through a research grant (#210875) awarded to the research team.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.