
Abstract
Background
Research conducted on conflict between Registered Nurses (RNs) has established that it happens regularly within the hospital setting, that it adversely affects the health and well-being of RNs, impacts the effective functioning of the health care organization, and compromises quality patient care. In this article, the phrase conflicting working relationships (CWRs) is used to represent working relationships between RN peers that are non-collegial, uncaring, and non- supportive, and inclusive of the behaviours associated with incivility, horizontal violence, and bullying, among others.
Purpose
To examine how nursing, including nursing knowledge and practice, is socially organized within the hospital setting and how this organization is linked to CWRs between RN peers.
Methods
Interviews were conducted with 17 RNs, followed by text analysis and mapping guided by institutional ethnography (IE) as the research methodology.
Results
The intersections between should nursing, double domination, and the big picture threads shows work environments where RNs struggle to provide appropriate care and conflict has become institutionalized. The intersection between threads can be used as caution areas for RNs and individuals in leadership positions to reflect on nursing practice when conflict is being experienced.
Conclusions
The contextual variables surrounding professional nursing practice are very influential with respect to how RNs relate to each other. A new type of dialogue about the organization of nursing practice in the hospital setting is needed to support more relational practices between RNs.
Background
Conflict among Registered Nurses (RNs) is not a new topic and it has been extensively researched over the past three decades (Roberts, 2015). Many different labels have been used to describe the experiences of conflict between RNs (Roberts, 2015). Some of the most commonly used labels have included incivility (Alshehry, Alquwez, Almazan, Namis & Cruz, 2019; Laschinger, Wong, Regan, Young-Ritchie, & Bushell, 2013; Layne, Anderson,& Henderson, 2019; McNamara 2012; Oyeleye, Hanson, O’Connor, & Dunn, 2013), horizontal violence (Armmer & Ball, 2015; Dumont, Meisinger, Whitacre, & Corbin, 2012; Taylor, 2016; Walrafen, Brewer, & Mulvenon, 2012), and bullying (Bennett & Sawatzky, 2013; Berry, Gillespie, Gates, & Schafer, 2012; Gaffney, DeMarco, Hofmeyer, Vessey, & Budin, 2012; Roberts, 2015).
The phrase conflicting working relationships (CWRs) is used to represent working relationships between RN peers that are non-collegial, uncaring, and non- supportive, and inclusive of the behaviours associated with incivility, horizontal violence, and bullying, among others (Rauman, 2020). CWRs does not refer to conflict in the workplace as an expression of disagreements between RNs but instead, it refers to the escalation and perpetuation of conflict behaviours to where they become unacceptable and detrimental to healthy, productive, and collegial working relationships. The phrase CWRs are also meant to examine the experiences of conflict between RN peers more broadly and move away from attempting to generalize individual interpretations of events into categories. As every conflicting event is different depending on the local context, circumstances, and subjective interpretations; generalizations from the commonly used quantitative approaches do not provide an accurate understanding of what is happening.
Research on conflict between RNs has established that it happens regularly (Cleary, Hunt, & Horsfall., 2010; Dumont, Meisinger, Whitacre, & Corbin, 2012; Katrinli, Atabay, Gunay, & Cangarli, 2010), and most frequently within the hospital setting (Guidroz, Wang, & Perez, 2012; Taylor, 2016); that it adversely affects the health and well-being of RNs, negatively impacts the functioning of the health care organization, and compromises quality patient care (Cleary et al., 2010; Dumont et al., 2012; Roberts, 2015). Despite the introduction of remedial/corrective strategies (e.g., de-escalation training, conflict management, crucial conversation training, resiliency, and cognitive rehearsal training, etc.) (Cleary et al., 2010; Embree & White, 2010; Laschinger et al., 2013) and regulatory/restorative strategies (e.g., organizational policies, legislative changes, zero-tolerance position statements, etc.) (Walrafen, Brewer, & Mulvenon, 2012) to address the problem, only minimal progress appears to have been made (Taylor, 2016). This may be attributed to a research focus on personal or interpersonal explanations for the development of CWRs. There is a gap in research examining the broader systemic influences permeating ruling relations of nursing practice in hospital settings, beyond the boundaries of nurses’ everyday experiences (Campbell & Gregor, 2008; Hutchinson, Vickers, Jackson, & Wilkes, 2006).
Purpose
To examine how nursing, including nursing knowledge and practice, is socially organized within the hospital setting and how this organization is linked to CWRs between RN peers (Campbell & Gregor, 2008, p. 18). Specifically, the social relations in which RN peers were engaged when experiencing a CWR was explored, including how these relations were interpreted, manifested, and perpetuated within the hospital setting, thereby contributing to the development of unhealthy/escalating conflict.
Methods and procedures
Institutional ethnography (IE) was used as the research methodology to supplement the existing research on conflict between RNs and to shift the focus away from why conflict between RNs occurs to investigating how it occurs.
IE is a method of inquiry located within the theoretical approach known as the “social organization of knowledge” (Campbell, 2006, p. 91; Smith 1987) and it refers to how “things [are] being put together systematically, but more or less outside a person's knowledge, and for purposes that may not be theirs” (Campbell & Gregor, 2008, p. 18). The aim of these investigations is to make clear how the purposeful organization of the activity of people relates to power structures (Campbell & Gregor, 2008). Therefore, institutional ethnographers (IE’ers) are interested in discovering the processes involved with the transmission of knowledge to people regarding how they understand the way they complete their work. This information is useful because there is a need to understand how CWRs between RN peers happen; how they are generated, interpreted, embedded, and normalized within power structures arising from interaction with local and extra-local contextual influences of the hospital setting.
Ethical approval
The study was granted ethical approval from Memorial University Health Research Ethics Board (HREB) (Portal #20170717). Approval was also obtained from the Eastern Health Research Proposal Approval Committee (RPAC).
Participant recruitment
Recruitment flyers were posted on bulletin boards in four acute care hospitals in Eastern Health, Newfoundland and Labrador, Canada. There was a participant from each of the four hospitals. Participants were included if they had experienced or witnessed CWRs in the acute care hospital setting at any time in their career, and they were not required to be working in the acute care hospital setting at the time of the interview. There were no exclusions with respect to employment status as permanent full-time, part-time, casual or float status. There was no distinction made with respect to the nursing unit where the participant was employed as in the current literature CWRs were found to happen on all inpatient units.
Additionally, there were no limitations placed on the amount of time since the CWR event. The review of the research literature supported that the impact of CWRs on nurses often remains with the nurse even after leaving the setting where the conflict occurred. Hutchison (2009) reported that nurses who left their nursing units because of bullying, despite being successful in their new work, still carried significant legacies of trauma from their bullying experiences.
Participants were excluded if they experienced a CWR while they were in a management or leadership role, as they would have not experienced the same contextual variables. Snowball sampling was also used as a recruitment strategy, as many RNs who volunteered knew of other nurses who may have wanted to participate.
Data collection
Consistent with IE methodology, interviews, text analysis, and mapping were the methods used for data generation.
Interviews
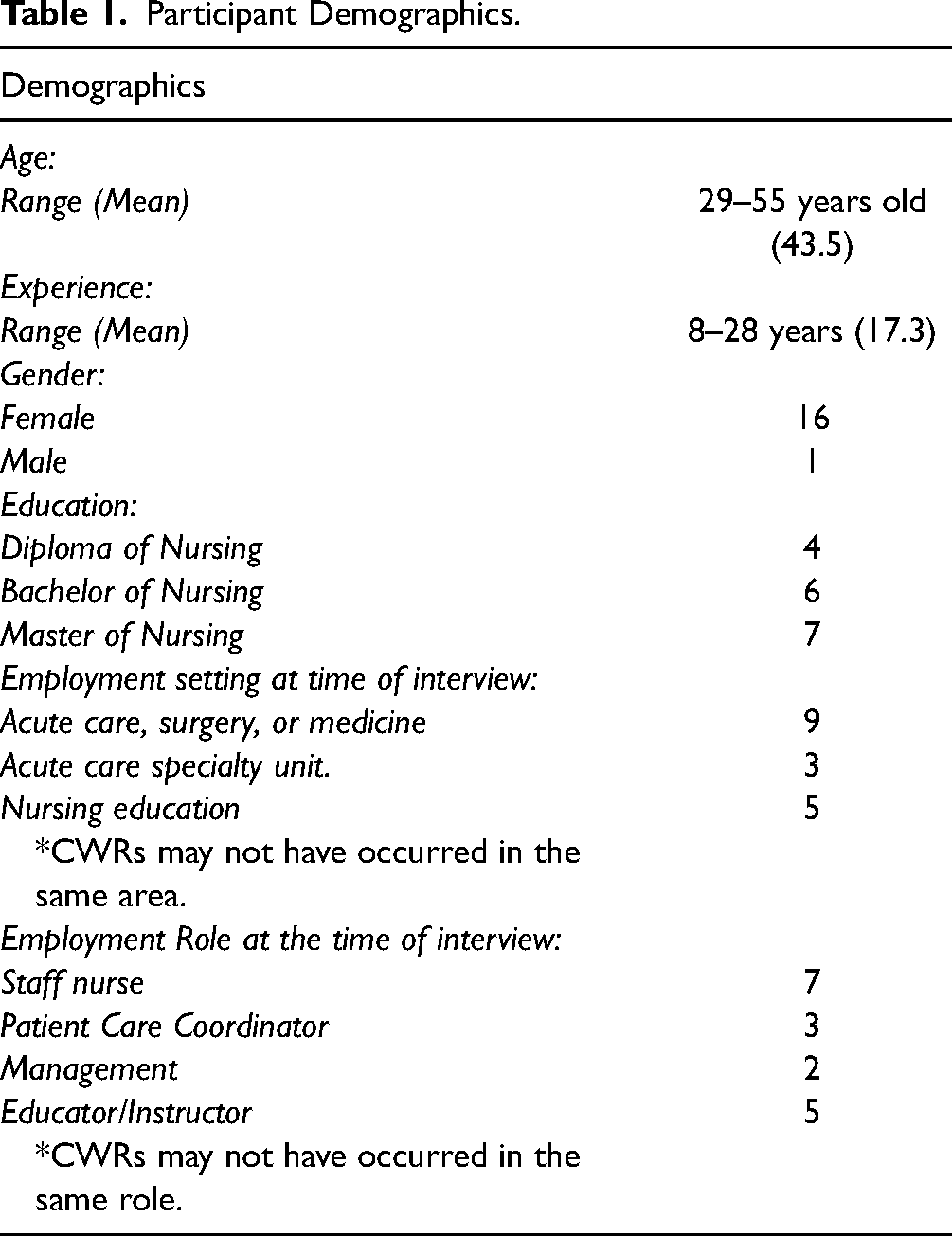
Interviews were conducted between November 2016 to September 2018. Seventeen nurses were interviewed. A formal, semi-structured interview guide was used to explore the social organization and/or the structures/forms of ruling of the work of nurses in relation to the participants experiences with CWRs. Interview questions began broadly by asking the participant about the activities of their shift surrounding their CWR experience, for example, “how did your shift begin?” Then the questions focused on the institutional work processes that were shaping their experience of conflict, such as, “can you tell me how you knew the morning medications needed to be given by 0830 h?” Each interview lasted between 40 and 120 min. Ten of the interviews took place in person, and seven of the interviews were completed by phone. Consent from the participants to record and transcribe the interviews was obtained. Following the interviews, the interview transcriptions were examined and all mention of texts and/or the use of texts was noted for text analysis.
Textual analysis
Text analysis as a method of data generation that assumes the ideas, plans, and activities of participants do not happen haphazardly, but instead are coordinated to occur as they do through the use of mediating or governing texts (Campbell & Gregor, 2008, Rankin, 2017a; Smith, 2001 ; Smith, 2006, Turner, 2006). Texts are used to coordinate actions to achieve outcomes in specific ways and as such, establishes rules, routines and/or practices/cultures that groups of people within the same institution are expected to follow. In this way ruling is accomplished through the use and activation of texts by people. It is through the activation of texts that an individual (or individuals) knowingly (or unknowingly) uses a text to guide or influence their work (Smith, 2005). The coordination of activities of people across multiple settings is usually unseen from the standpoints of those within the local setting (Campbell & Gregor, 2008; Smith, 2006; Turner, 2006), meaning that people usually do not consciously consider how their activities are purposefully organized and for what purpose. Once texts and text-mediated discourses are identified, mapping is used to make the unseen coordination of the activities of individuals, and the purpose of that coordination visible.
Mapping
Mapping is the process whereby the researcher brings the unseen coordination of activities of people into conscious thought by making the organization of those activities visible. By mapping connections between time, place, and contexts, and drawing a map of those connections, researcher gains access to ruling relations (Campbell & Gregor, 2008). The ruling relations identified through the participants’ descriptions of how they conducted their work, including their collegial relationships, was traced back to the source of that information and the ideologies created. Through mapping, the implicit knowledge and ruling practices taken up and used by RNs are made explicit, bringing awareness to RNs of where these ideologies come from and how they influence their behaviours and interactions with peers.
Data analysis
Analysis in IE is an iterative process that involved moving back and forth between the data generated by interviews and the context/ processes/use of texts that produced the experience (Campbell & Gregor, 2008; Rankin, 2017a). Three tools proposed by Janet Rankin (2017b), writing accounts, indexing, and mapping were used to support the data analysis process.
Writing accounts
Writing accounts is a method of analysis whereby the researcher selects an instance of activity from the interview data, writes down and describes how the activity was socially organized from the participants standpoint. When writing accounts, the focus is on the details of the participant's work and the organization of their nursing practice surrounding their CWR experience. When writing accounts, it is important to take notice of occasions where the knowledge generated in a participant's everyday work is subordinated by, or is in tension with, specific texts, text-mediated discourses, and ideologies that were used, or were supposed to be used, to decide and act. These tensions would then be examined in relation to the development of the CWR experience. The writing of the participants accounts was grouped into accounts related to novice nursing practice, nursing practice in the hospital setting, and nursing practice within an evolving health care context.
Part of the process for writing accounts was noting how participants used institutional language. Institutional language refers to how the particular use of words, language, and text to build versions of what people say, do, or know within a specific setting (Campbell & Gregor, 2008). For example, participants understood the word “admission” to refer to a textual process, a series of steps to be completed, that directed the organization of the nursing work and the process required to admit a patient to the hospital (Figure 1).

Example of indexing.
Indexing
Indexing is a tool used in conjunction with the interview transcripts and the use of institutional language to cross-reference work processes, people, and settings, and organize the data into linked practices (Rankin, 2017a). Indexing begins during the interviews when the researcher takes note of what the participants state they “knew” was required from them for their nursing practice. The researcher would ask follow-up questions regarding how this information is know. Generally, the participant referenced a specific text, an ideology and/or text-mediated discourse which were further analyzed. All texts noted were subject to textual analysis.
Mapping
Mapping was a tool used during both the data collection, as previously described, and once completed for data analysis.
Findings
Reflections from novice nurses experiences
In these participants accounts, participants were often reflecting on their experiences as a “novice” nurse. The word novice in this study referred not only to new graduate nurses with limited experience, but it also referred to causal or float nurses, nurses new to a unit, or nurses newly hired to a unit, many of whom had years of nursing experience, but their CWRs happened when they were “novice” to a setting.
It was clearly articulated by the participants in these accounts that they had expectations for mentorship, for assistance, and support from their peers. These expectations were not met, as participants described their experiences with “nurses eating their young”, being left to “sink or swim” and having to pass at “rite of passage” into the nursing profession, as well as experiencing being “set up to fail”.
The participants also described that because they had preconceived ideas regarding how their peers/colleagues/mentors were to respond to them that their CWR experiences were particularly troubling for them. From the participants’ standpoint, their ideals/expectations regarding nursing practices were concrete and unquestionable. For example, when the participants stated how they did not expect to experience CWRs with each other, they could have supported their expectations for professionalism by referring to the texts governing nursing practice. When questioned about their expectations for professional nursing practice, the Standards of Practice for Registered Nurses and the Code of Ethics for RNs, and employer policy were provided as examples.
As an example of “sink or swim”, one participant spoke about how, as a casual nurse, she was often left to complete complex patient assignments on her own. She expressed feeling lost because as a casual nurse on that unit, she was not as organized as she normally would have been if she had been assigned to work on a unit that she was familiar with and that she was behind on her assigned nursing duties. She explained how her co-workers, although they could see that she was struggling [lost], would not freely offer her assistance. Lost, but not only that, they have not helped you. Nobody has gone to check on your patients, nobody has gone to probably administer something that should have been given at 8:00 - 8:30. They are just … they are going to do their own work. You can “sink or swim.”
In the preceding quote, there are examples of the ruling relations that exist in the hospital setting. For example, the statement “should have been given at 8:00–8:30” is evidence that there is a medication administration policy or procedure that describes how nursing practice is organized. The statement “going to their own work” provided insight into the value place upon being independent in nursing practice, and finally, the statement “sink or swim” is an indication of the culture of nursing in that area, at that time.
The word should was used by many participants to describe how they came to understand the way their nursing work ought to be completed in the hospital setting. Specifically, participants would describe their typical day or night shift by listing the activities they were “supposed to” do, what their role was “supposed to” be, how they were “supposed to” act, and how they “should” complete their work. Should statements are significant because they reflect the ruling ideas of those in positions of power and/or authority (Taylor, 1997). As such, should statements were also common in the participants accounts concerning the hospital setting and nursing in the evolving health care context.
Nurses’ accounts of nursing work in the hospital setting
When the participants were questioned about their CWR experiences and the details of nursing work in the hospital setting surrounding the conflict, all of the participants spoke about hitting the ground running; how there was very little time to complete all the nursing tasks they were required to accomplish; how any deviation from the routine structure of the day was unsurmountable, and about how they had to make decisions about what was the most important aspects of care to get done. It was evident from the interviews and the participants use of should statements that most nurses adopt biomedical and business attitudes of providing health care and incorporate the ruling ideals of completion of tasks as the only relevant way to demonstrate competence in their nursing practice.
At the same time, some nurses described how they felt the biomedical and business models of health are at odds with how they expected nursing to be practiced, creating an internal conflict regarding the conceptualization of the good nurse. When questioned about the disjuncture between the image of nursing as a kind, caring, and compassionate profession, and the embodied experience of practicing nursing in a context that is stressful, time constrained and technological, the participants described situations of accountability and documentation. For example, usually the technical (task-based, medical) aspects of care were completed because of the documentation required on those aspects of care (making nurses accountable) and the less technical aspects were more discretionary as whether to complete or not. As well, nurses implement the care they provide via the activation of hospital texts (i.e., policy, etc.) and text-mediated discourses (i.e., ideologies) regarding how nursing care ought to be completed. For example, when providing care for a patient with an epidural catheter, a nurse is required to follow the epidural protocol, which is a text that organize nursing work because it instructs the nurse to complete and document a focused physical assessment on the patient every hour or every four hours. A lot of times [a patient] has an epidural or a PCA [patient-controlled analgesia] so you have to check those [patients] either every hour or every 4 h depending on what [surgery] they have.
The medication administration record, and several patient care protocols were some of the other texts mentioned and analyzed. Nursing work, as organized via the use of text/procedure/documentation has become commonplace and accepted as the only correct way to complete nursing care from an institutional perspective, which may be interpreted differently by different RNs in different contexts, a precursor to conflict between RNs. The organizing of practices via the written word are often interpreted as “what actually happened” (Smith, 1990 , p. 70). Since the practice is written down to be carried out in a specific way, this “textual reality” can be considered as a more factual account than the “lived actuality” of the person completing the practice (Smith, 1990a, p. 71). So, if disagreement exists regarding what happened versus what was documented, then the documented account is usually perceived as more credible, despite the textual reality being devoid of the contextual variables that were present and influential in the lived actuality.
Participant's also spoke about how most everyone was busy; therefore, you needed a good “skill set” and competence in your skills and the ability to work independently is valued. The ideology of the good nurse was often linked to the nurse's ability to independently manage and accurately complete all their assigned nursing tasks, including documentation, especially when the work at the unit was considered busy or heavy. The following is an example from the accounts of working in the hospital setting. [B]ecause I didn’t understand the [type of illness] map, you know, what would have been expected of me, everybody else was busy. I always understood their position, but I felt…the way units operate, you know, they kind of leave you to your own devices, you go figure it out, right? Which is dangerous for the patients.
The level of skill and competence of nurses was found to have created a hierarchy of nurses that was reinforced in the hospital settings organization of different units and categories of patient care, which fostered comparisons between RNs and contributed to CWRs. The participants said how this type of environment was stressful and frustrating for them, and how in such environments, a lot of nurses experienced burnout.
Burnout was described as a common occurrence and as a precursor for strained working relationships between RN peers. Instead of identifying the source of burnout as being located within the hospital setting and the conditions surrounding the work of nurses, some nurses perceived burnout as the nurse's personal flaw, such as their inability to handle the workload. …I would say that the biggest…, the issue probably is when people become burnt out [sic]. You can notice that [nurses who experience burnout] in their attitude towards others (co-workers), I guess kind of expecting them [co-workers] to do more because they (nurses who experience burnout) can’t handle it but can’t really admit that …
Although it is true that symptoms of burnout can definitely affect the nurse's performance (Guidroz et al., 2012; Oyeleye et al., 2013), the nurse experiencing burnout was being double dominated; first, by the organization of their work, and second, by RN peers who had fully embraced the domineering top-down institutional mindset.
Double domination was also apparent in how nurses frequently use the occurrence reporting system to resolve conflicts. However, it was noted that when working conditions were more manageable, disagreements between RNs still occurred but were more likely to be resolved between individuals. When nurses felt overwhelmed at work (e.g., too busy, too stressed, burned out, etc.), the occurrence reporting system (also a text) was also used to vent frustrations. With limited resources left to give, some participants described the occurrence reporting system as preferred over trying to resolve the issue on their own, indicating how in the hospital setting conflict has also become an institutional process or institutionalized.
Nurses’ accounts of nursing work in the broader evolving health care context
In these accounts, the participants’ spoke about how there was an expectation for nurses to deal with changes in their practice and disruptions of their routines without any interruption in patient care. Participants described how they felt changes to nursing practice were often implemented without adequately consulting RNs about how these changes would increase their workload, impact their routine, and practice, and adversely affect their work-life balance. Due to these factors, changes to nursing practice were often met with resistance because nurses feared changes would lead to greater demands on their time and more work. we sat down [with management], we said okay, it [the lean process implementation] wasn’t working for nurses because they were busy as it is…that was the issue, when are we going to have this time?…see we went from 11 o’clock, that didn’t work, we were trying to drag the girls in but they were so swamped out there [on the floor], they didn’t want to come in to do their round [referring to “bullet round”]
At a national and provincial level, the value of care is regarded as a matter of the appropriateness of services being delivered at a manageable cost. The participants’ accounts highlighted how nursing work, when conducted in this way, has created struggles for nurses to provide quality care within a task-based, results-focused, continuously monitored and evolving, complex health care system (Day, 2013). The big picture thread extends the organization of nursing practice beyond the participants’ immediate unit to include the other units in the hospital setting and the influence of the broader evolving health care context in Canada.
The connections and the intersections between should nursing, double domination, and the big picture were mapped and made visible in Figure 2. By making visible how nursing practice is concerted to happen in a certain way shifts the focus of strategies for prevention of CWRs from looking exclusively at individual behaviours to also looking at the broader systemic issues influencing such behaviours.
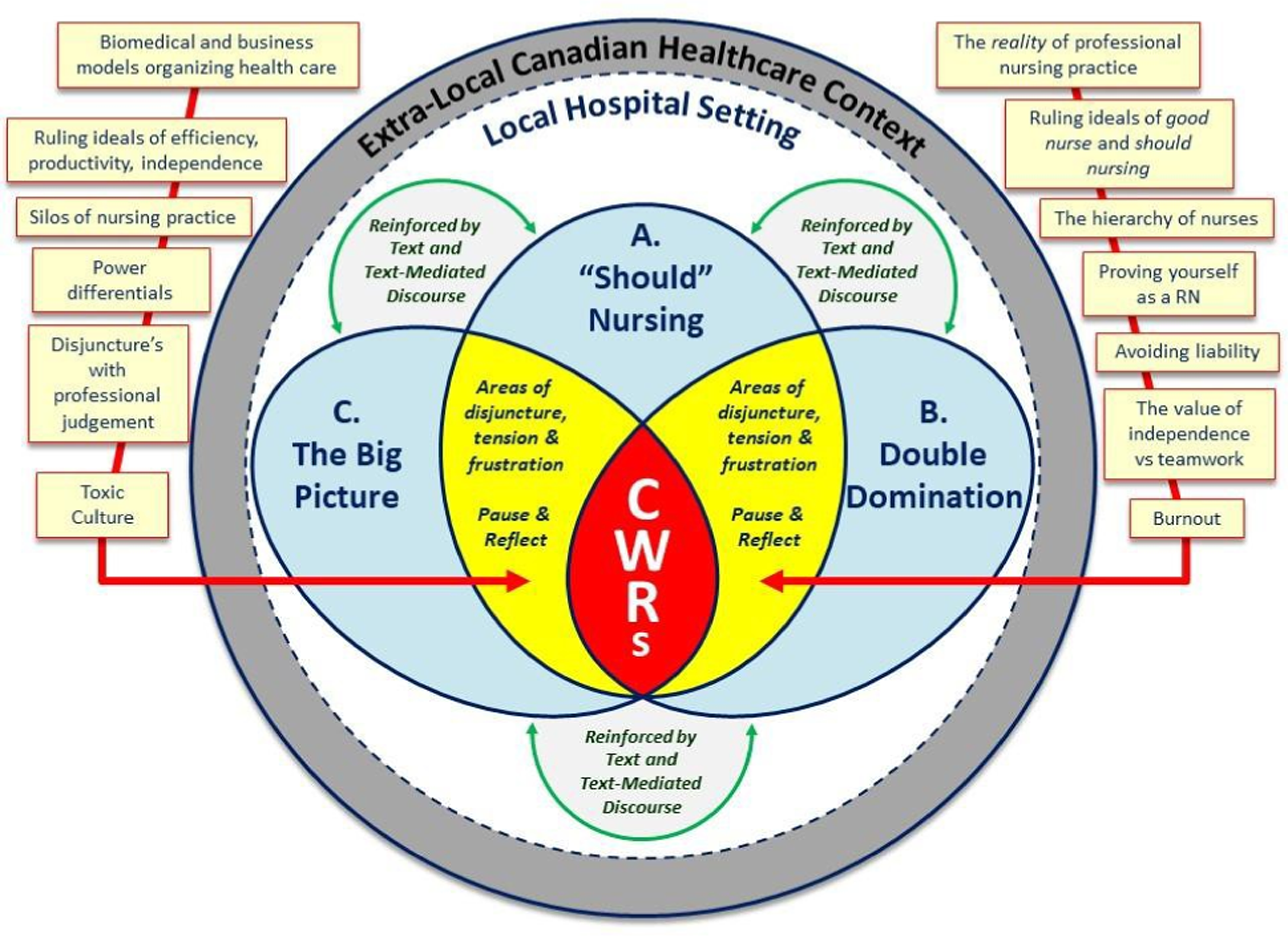
A map of the social organization of nursing practice in the hospital setting and its relationship to the development of CWRs between registered nurse (rn) peers. Taken from: Rauman, (2020). The Social Organization of Nursing Practice in the Hospital Setting and the Influence on the Development of Conflicting Working Relationships between Registered Nurse Peers. Unpublished doctoral dissertation.
Discussion
In this research, CWRs were described differently that what is found in the research literature on bullying, where it is usually defined as repeated behaviours by a perpetrator to a recipient over an extended time frame (Anusiewicz, Ivankova, Swiger, Gillespie, Li, et al., 2020; Bennett & Sawatzky, 2013; Berry, Gillespie, Gates, & Schafer, 2012; Gaffney, DeMarco, Hofmeyer, Vessey, & Budin, 2012). In contrast to the bullying literature, the participants in this study noted how CWRs did not necessarily involve a single nurse repeatedly starting a conflict with a specific peer. Instead, participants expressed CWRs as being a part of the atmosphere of nursing practice, and as such, were widespread within their professional work experience and linked to the social organization of nursing in the hospital setting. This is consistent with recent research which has found the nursing workplace environment as being foundational for positive nurse, patient, and organizational outcomes (Anusiewicz et al., 2020).
The common behaviours and attitudes noted in the participants’ accounts included yelling, belittling, denial of assistance, ignoring, withholding information, and the phenomena of nurses eating their young, being left to your own devices, and being set up to fail. These hostile behaviours echo the previous research literature on bullying and horizontal violence, as well as a variety of other labels. However, most of the participants did not use the terminology specific to bullying or horizontal violence. Instead, most of the participants described how these behaviours from their peers were unexpected; how they impaired their working relationships, and how they made them second-guess their understanding of nursing. The outcomes of impaired working relationships and self-doubt have been commonly described in the current research literature (Anusiewicz et al., 2020; Rosi, Contguglia, Millama, & Rancati, 2020). This research was different in that it explored the participants’ expectations regarding working relationships and professionalism and found it to be related a number of guiding texts.
Two commonly referenced texts included the Standards of Practice for RNs and the Code of Ethics for RNs. These two documents (among others) represent the minimum expectations for professional nursing practice while providing the criteria against which RNs are held accountable in their practice. For example, with respect to CWRs, the expectation for mentorship is reflected under standard two – knowledge-based practice, indicator 2.7 which states that “RNs support their colleagues and students by sharing their nursing knowledge and expertise” (ARNNL, 2013, p. 8) 1 . Additionally, the Code of Ethics for Registered Nurses directs nurses to reflect upon all components of their practice, including the quality of their interactions with others (CNA, 2017). Provided that the Standards of Practice for RNs and the Code of Ethics for RNs are legislative requirements and must be observed by all nurses in all practice settings, it is reasonable to expect that CWRs should not occur at all. However, this was not what is happening in the hospital setting.
The should nursing thread makes visible the potential for dysfunctional power dynamics between nurse peers with different levels of knowledge and experience. Through the should nursing thread, it was demonstrated that knowledge and experience can be misused to criticize, demean, and belittle colleagues, especially in settings that value independence, and foster competition. The ideology of the good nurse was so commonplace within the hospital setting, that phenomenon's such as having to pass a “right of passage” are not easily recognized as influencing conflict (Rosi, Contiguglia, Millama, & Rancati, 2020).
Double domination was evident in the acceptance of dysfunctional power dynamics, and by the creation of toxic work environments where burnout occurs. Texts used to govern nursing practice could also be used to legitimize CWRs, through the supporting of competition and hierarchies between nurses on different units, and through using the occurrence reporting system to manage interpersonal conflict. Some of the previous research has found that efforts to change nursing behaviours that focus only on communication skills and becoming more comfortable with conflict have little effect (Padgett, 2013). According to Padgett, it is easier to use an online reporting system and the email system because it removes the actual personal connection to the CWR, and the reporting individual feels less accountable. Such a practice is worrisome for the profession because a crucial part of collegiality is taking accountability for one's actions, which is a professional expectation for a self-regulating profession like nursing. Although most of the research participants emphasized the importance of open communication, peer support, and teamwork to safely practice nursing, the reality for the participants was that nursing practice had become organized in a way that promotes individualism and competition between nurse peers. It became evident that within the hospital setting, RNs unconsciously supported competition among themselves, which has been detrimental to the formation of team-based and supportive practice environments.
Additionally, as the hospital setting is organized into different units, with different sets of nurses working on scheduled shifts, nurses are working within a type of “micro-society.” The micro-level social-construction perspective views social norms as being established by only those within a setting, where face-to-face dialogic interaction between individuals and the use of texts, establish the identity of the self and the norms of the social environment (Cruicks 2012 hank, ). Within a micro-level perspective, it is difficult for RNs on different units to envision and appreciate their involvement, and the involvement of others in the big picture.
Further, should nursing, and double domination were concerted by the big picture. Not only have nurses been obscured of the valuable contribution that all nurses make, they also are practicing nursing in a setting that has been shaped by the wider social, political, and economic trends influencing the evolving health care system, and health care reforms as implemented at the provincial level. Within the Canadian health care context there are pressures associated with accessibility, efficiency, and cost containment, as evidenced by the models of nursing care implemented. Health care changes/reforms have been implemented to respond to these pressures in the form of management and cost containment processes that are very evident in the hospital setting and highly influential on nursing practice.
Efficiency monitoring and outcome measurements organize the hospital setting so that nursing practice (and the practices of other health care providers) can be easily measured and controlled. As well, the coordination of nurses and their everyday practice allows for their nursing practice to be supervised, ensuring conformity and standardization. Organizing nursing practice in this manner has resulted in nursing practice being judged as appropriate or satisfactory by those in positions of power and under the terms they describe (Hutchinson, Vickers, Jackson, & Wilkes, 2006) ), which may be at odds with what nurses deem as more appropriate in the context of their everyday professional practice. However, as nurses become accustomed to working within the system, they are coordinated and conditioned to adopt the same fiscal and efficiency attitudes as the correct/most appropriate way to practice nursing. These attitudes are supported and reinforced within the hospital setting by texts directing nursing practices/procedures to ensure conformity (Hutchinson, Vickers, Jackson, & Wilkes, 2006) ). Further, nurses may be disciplined or have sanctions applied to their practice should they operate outside of this authorized discourse, which reinforces the belief that nursing practice should be completed in this way.
By establishing an objective account of how CWRs experiences between nurses may be generated through the conditions of their work and institutional practices, nurses can use this information to stimulate a new type of dialogue about the working conditions needed to help support more positive relationships between nurse peers.
This research has several limitations. First, some CWR accounts as told by participants took place years prior to the interview date, introducing the potential for recall bias. As well, because of the differences in timelines, some participants may have been referring to different versions of the Standards of Practice and Code of Ethics, and perhaps, different sets of expectations for professional behaviours. Therefore, it was necessary to review the previous versions of these texts for any revisions that may have influenced participant experience and/or their expectations on how to behave professionally. Despite revisions and/or updates to the standards of practice and the code of ethics documents, overall, nursing continues to be defined as a caring profession. Hence, the overarching expectation for nurses to have a caring attitude and to act professionally did not significantly change over time.
Secondly, the absence of interviews with nursing managers and administrators was another limitation. Although some nurses were managers at the time of the interview, their experiences with CWRs took place when they were not in a management position. In the place of interviewing managers and administrators, text analysis of hospital policy was used as the entry point into the second level data generation. Additionally, access to texts was limited (e.g., the online occurrence reporting system). Therefore, the policy(s) used to articulate the purpose of the text was analyzed instead.
Recommendations and conclusions
Although the experiences of the individual participant's were not all the same (due to different standpoints, different timeframes, and different values and interpretations of reality), the analysis of the social relations that contributed to the development of the CWR were generalizable and will resonate for all those who have faced similar tensions and contradictions in their everyday work. This is because the theory upon which IE relies tells us that institutions are ruled and organized in definitive ways.
The should nursing, double domination, and big picture threads represent the social organization of nursing practice in the hospital setting and how the authorized discourse has contributed to individualized and competitive work environments where nurses struggle to provide appropriate care, and where conflict has become institutionalized. The environment in which nurses work needs to assist nurses to switch their thinking away from linear, one-sided thinking to critical, reflexive thinking and away from individual practice to collective practice.
As made visible in the framework, the intersections between should nursing, double domination, and the big picture are caution areas for RNs and individuals in leadership positions to reflect on during their nursing practice and when experiencing conflict. Recommendations for senior RNs, managers, RNs in charge, regulators, union leaders, educators, researchers, and government would begin with using the findings of this research to advocate for changes with respect to the hierarchy of nurses within the hospital setting, to reflect a more balanced (horizontal) organizational system of nursing care, making it transparent, fair, and consistent across sites, shifts, and providers. Part of this process may include changing the value of independence as the indicator for the status of the good nurse to mean one who is relational and strives to support a team dynamic. Perhaps rewarding nursing teams and collegial practices, instead of individuals. A relational inquiry approach maybe an alternative way to organize nursing practice.
Another recommendation would be to revise the format/wording of policies concerning the organization of nursing practice to be broad and principle based so that contextual variables can be taken into consideration, and RNs can be supported through the use of texts to use their professional judgement. Also, conflict resolution policies may be reworded to better reflect the importance of relational approaches.
Wherever there is a toxic environment, a conversation must begin by questioning nurses about their work: what works well, what does not work, and where disjunctures, tensions, and frustrations are experienced in the context of their work environments. A third recommendation is for nursing leaders to open a dialogue about a common ground for nursing practice, one that meets the expectations for nurses, the public, the organization, and the government. Most importantly, the knowledge stemming from these conversations with nurses must be incorporated into texts (e.g., hospital policy, procedures, governing documents, etc.) so that the texts will be taken up and activated by nurses, ingraining into everyday practice, positively influencing the atmosphere of professional nursing practice.
As it is now, when faced with a conflict, nurses are directed to raise questions about the specific practices of their peers with their managers. This leads to a range of problems and recriminations as discussed earlier. In the future, instead of only questioning the practices of our colleagues, nurse leaders need to open an arena for discussion on the ways nursing practices are organized and how it contributes to the development of CWRs.
By making RNs aware of how the organization of nursing practice influences their thoughts, actions, and behaviours towards each other provides RNs with an additional knowledge resource to draw upon when making decisions regarding CWR events, creating the space to potentially choose different responses/behaviours. Additionally, this knowledge can be thought of as complementing the existing strategies of emotional resilience and cognitive rehearsal training, which have been shown to decrease occurrences of CWRs (Embree & White, 2010; Sergeant & Laws-Chapman, 2012; Stagg, Sheridan, Jones & Speroni, 2011). Secondly, the same awareness may provide leaders with a platform to open a dialogue and begin the process of change in the ways nursing practice is organized. An organization that promotes an environment that supports healthy and productive working relationships between RNs.
Participant Demographics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.