
Abstract
Background
Parish nursing is a specialized branch of professional nursing that promotes health and healing by integrating body, mind and spirit as a practice model. Parish nurses contribute to the Canadian nursing workforce by promoting individual and community health and acting as system navigators. Research related to parish nursing practice has not been systematically collated and evaluated.
Purpose
This review seeks to explore, critically appraise and synthesize the parish nurse (PN) research literature for its breadth and gaps, and to provide recommendations for PN practice and research.
Methods
A scoping review was conducted using Levac and colleagues’ procedures and Arksey and O’Malley's enhanced framework. The CINAHL, ProQuest and PubMed databases were comprehensively searched for original research published between 2008 and 2020. The final sample includes 43 articles. The Mixed Methods Appraisal Tool was used to critically assess literature quality.
Results
There is a significant gap in PN research from Canada and non-U.S. countries. Methodological quality is varied with weak overall reporting. The literature is categorized under three thematic areas: (1) practice roles of the PN, (2) role implementation, and (3) program evaluation research. Research that evaluates health promotion program interventions is prominent.
Conclusions
More rigorous research methods and the use of reporting checklists are needed to support evidence-informed parish nursing practice. Building relationships among parish nurses, nursing researchers and universities could advance parish nursing research and improve evidence-based parish nursing practice. Research into the cost effectiveness, healthcare outcomes, and the economic value of PN practice is needed.
Keywords
Background and purpose
As Canada's population is living longer than ever and the prevalence of people with chronic diseases continues to grow, the formal care system is less able to meet the increasing health and social care needs of people and families living in the community. There is a need for health care reform and other solutions that prioritize community-focused nursing care (World Health Organization [WHO], 2017). Parish nursing (or faith community nursing, as it is known in some jurisdictions) is a specialized branch of nursing and a health ministry of faith communities that enacts health, healing, and wholeness of body, mind, and spirit as a practice model (Canadian Association for Parish Nursing Ministry [CAPNM], 2021a). Its overarching philosophy is that “all faith communities are places of health and healing and have a role in promoting wholeness through the integration of faith and health” (CAPNM, 2021a, para. 1).
In Canada, all parish nurses (PNs) are registered nurses. PNs contribute to the Canadian nursing workforce, yet their impact is poorly understood. The number of Canadian nurses practicing as PNs is not known as many PNs practice in volunteer roles, the numbers of graduates from PN certification courses have not been collated, and there is no common registry for Canadian PNs. Nevertheless, PNs provide comprehensive individual and community assessments, promote and protect health, and act as system navigators for clients and families. As such, their practice positively influences individual and community health across many Canadian jurisdictions.
Brief history of parish nursing
The modern-day practice of parish nursing was founded by Granger Westberg, a hospital chaplain, professor, and pioneer who had an early vision for wholistic care across healthcare settings (Westberg Institute, 2020). In the 1960's he introduced “wholistic” health centers addressing whole-person needs: body, mind and spirit. Westberg learned that nurses helped bridge the gap in language between medicine and faith, making theirs a critical role in whole person health and health promotion. Thus, in 1984 he launched the first demonstration project of parish nursing. In 1997 parish nursing was recognized as a nursing specialty by the American Nurses Association, and in 1998 The Scope and Standards of Parish Nurse Practice was published (Westberg Institute, 2020).
Not aware of the developing movement of parish nursing in the United States, Barbara Craiger, in 1988, developed a “nurse in a church” ministry in Thornhill, Ontario, Canada (Craiger, 2006). In the 1990's, other Canadian nurses were led to this ministry first going to the United States for training and then developing education programs for parish nursing and church health ministry in Canada.
The first Canadian PN course was at the University of Alberta. It was joined by distance education courses through St. Francis Xavier University in Nova Scotia and Concordia College in Alberta. In 1996 a pilot project in health ministries in Oshawa, Ontario was the beginning of InterChurch Health Ministries (ICHM). This organization established a basic PN education program and later partnered with the Toronto School of Theology. The ICHM also spawned affiliate programs in Saskatoon and New Brunswick and held a program at Waterloo Lutheran Seminary in 2009. McMaster Divinity College and Tyndale Seminary held graduate level parish PN courses for a time. All of these courses waxed and waned based on need. In 2010 St. Peter's Seminary in London, Ontario developed the Foundations in Parish Nursing which continues today.
In the 1990s Canadian scholars began publishing their observations of the PN experience in journals and as a book chapter (Olson et al., 1999). In 1996 Lynda Miller developed a nursing conceptual model to help nurses link concepts of faith and health in practice, education, and research; this work was later published as a book (Miller, 2004). Her article in the Canadian Nurse (Martin, 1996) attracted many nurses from across the country to the ministry of parish nursing. Margaret Clark and Joanne Olson provided a description of their experience of teaching PNs using the McGill model of nursing (Clark & Olson, 2000).
In 1998, the Canadian Association for Parish Nursing Ministry (CAPNM) was inaugurated. The Core Competencies and Standards of Practice were developed and parish nursing became recognized by the national and provincial professional associations, although not as a specialty. With the core framework of the ministry established, CAPNM members turned their interest to the development of a body of knowledge for supporting evidence-based practice (EBP) in parish nursing. This interest is the impetus for this review.
Literature review
Research in parish nursing and faith community nursing is in its infancy. For consistency, we use the terms “parish nurse” (PN) and “parish nursing” throughout this review. Three reviews of the PN literature have been published in the last 17 years (Dandridge, 2014; Dyess et al., 2010; King, 2004). King (2004) published the first review of PN literature, the purpose of which was to map the nature and fit of PN work within the church. The major findings were reported in the areas of needs assessment, parish nursing care, and perceptions of parish nursing. Six years later, Dyess et al. (2010) published a review of the PN literature. Their findings highlighted new research related to the development and implementation of PN roles and practices, such as documentation. Dandridge (2014) review focused on understanding outcomes associated with PN interventions and the value of the PN in health promotion and disease prevention. The search strategy for Dandridge's review was limited to studies conducted in the United States. The aforementioned reviews (Dandridge, 2014; Dyess et al., 2010; King, 2004) lack clear reporting of search strategies, a systematic process for inclusion and exclusion of studies, and critical appraisal. To advance PN practice and research, there is a need to rigorously evaluate PN interventions and their outcomes (Dandridge, 2014: Dyess et al., 2010). Therefore, the purpose of this scoping review is to explore, critically appraise, and synthesize the PN research literature for its breadth and gaps, and to suggest recommendations for PN practice and research. In this review, we answer the following research question: What are the characteristics of the parish nursing research literature (type, quality, foci) and how can it inform PN practice and research in Canada?
Methods
We selected a scoping review methodology because of the nature of our research question, its rigor in synthesizing a variety of research, and usefulness in informing practice and future research (Colquhoun et al., 2014; Noble & Smith, 2018). We applied Levac and colleagues’ scoping review procedure that includes Arksey and O’Malley's enhanced framework (Arksey & O’Malley, 2005; Colquhoun et al., 2014) for supporting procedural consistency (Arksey & O’Malley, 2005).
Identifying relevant studies
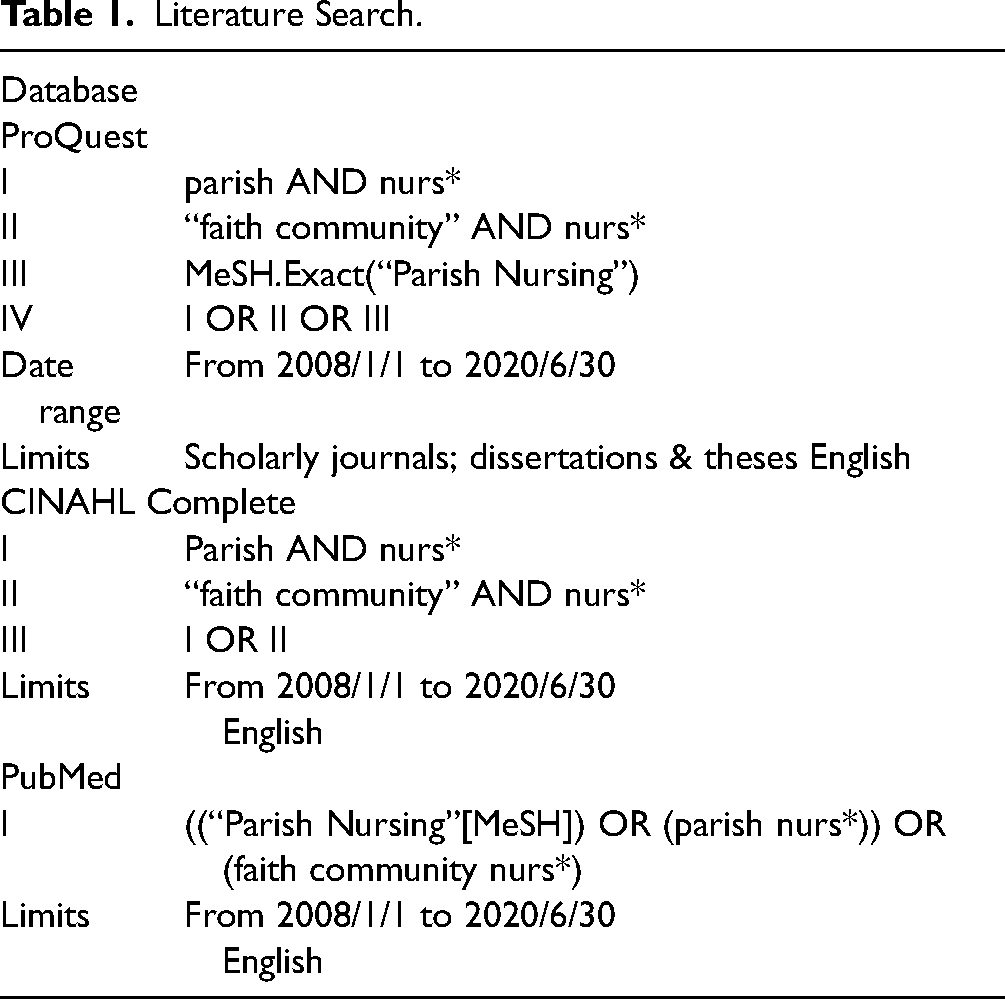
In consultation with a librarian, we conducted an iterative search strategy of the Cumulative Index to Nursing and Allied Health Literature (CINAHL), ProQuest and PubMed databases. To update the most recent reviews (Dandridge, 2014; Dyess et al., 2010) we searched articles published between January, 2008 and June, 2020. We also reviewed the reference lists of various articles for relevant studies that were retrieved and added to our database. Refer to Table 1 for the search terms.
Literature Search.
Study selection
To avoid overlooking potentially relevant articles, the eligibility criteria were broad. Original research articles and published and unpublished theses and dissertations written in English were eligible and included in the review. Literature reviews, editorials, commentaries, case reports, and articles that did not directly focus on PN practice were excluded. A three-phased review process was completed that involved title and abstract screening, full manuscript review, abstraction, and critical appraisal by two independent reviewers. The Mixed Methods Assessment Tool (MMAT), 2008 version was selected for its ability to appraise the methodological quality of qualitative, quantitative, and mixed methods studies (Hong et al., 2018). The appraisal criteria are unique to each type of study. The MMAT criteria and detailed explanations for their application are publicly available. Appraisal was conducted by five team members (EM, AF, JL, KP, CG). Two reviewers reviewed each study answering five appraisal questions specific to each study type (Hong et al., 2018) and by applying three possible responses: “yes,” “no,” or “can't tell.” A third reviewer was engaged to confirm/disconfirm the discrepancies.
Prior to in-depth appraisal, all studies were assessed against two screening questions: (1) Are there clear research questions (or objectives)? and (2) Do the collected data allow to [sic] address the research questions? (Hong et al., 2018). We appraised the first screening question as “yes” if the research question/objective was not explicitly stated but could be clearly inferred from the purpose statement or aim. Nine studies were excluded because their research question/purpose could not be inferred and/or we assessed the researchers’ data collection methods as not addressing the research/purpose. After completion of the review process, a total of 43 studies were included. The study selection process is depicted in Figure 1.
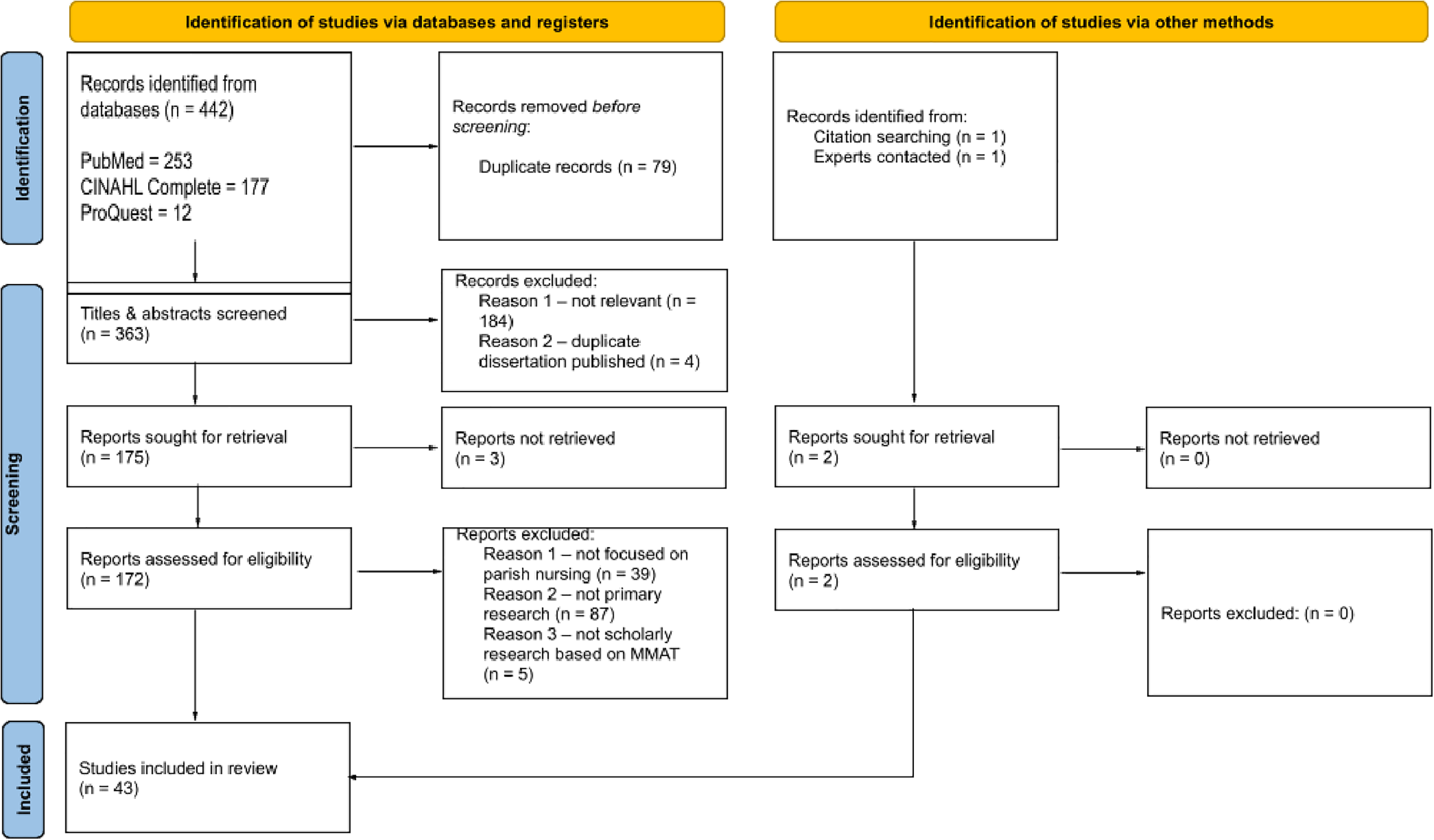
PRISMA flow diagram.
Data charting and sorting
Seven team members (EM, AF, JL, KP, CG, RT, CM) were involved in charting the literature characteristics and MMAT results to an Excel database and four (EM, AF, JL, KP) in data sorting/analysis. We began the analysis by iteratively reviewing the database to form individual insights about the nature of the literature sample. Strategies involved concept mapping and listing potential major and minor categories based on coding the literature table for details such as study design, findings, and reviewer insights. Information was inputted into a document to track the alignment of the studies with emerging themes/categories. Our team met 16 times to share insights and agree upon the final thematic areas and sub-categories. All decisions were documented.
Results
Overall characteristics of the literature sample
Forty-one of the 43 studies (95.3%) were conducted and published in the United States. Only one study emerged from Canada (Millerd, 2010) and another from the United Kingdom (Wordsworth, 2015). The majority of parish nursing research is published in peer-reviewed journals (n = 38), with one unpublished Master's thesis (Millerd, 2010), four doctoral dissertations (Bagley, 2011; Dyess, 2008; Tormoehlen, 2009; Ziebarth, 2016b), and one book (Wordsworth, 2015). Over half of the sample (n = 24; 55.8%) is published in the Journal of Christian Nursing (n = 15) and the International Journal of Faith Community Nursing (n = 9). Just over half (51.2%; n = 22) of the literature sample reflects quantitative research, with the majority in this category being descriptive (n = 16), and the remainder non-randomized (n = 5) and randomized controlled (n = 3) studies. Qualitative studies make up one-third of our literature sample (n = 14; 32.6%). Among the 14, two are grounded theory (Dyess & Chase, 2012; Van Dover & Pfeiffer, 2011) and two phenomenology (Dyess, 2008; Millerd, 2010). The remainder (n = 10) report using non-categorical qualitative methods. Finally, seven studies reflect mixed methods research designs (Bagley, 2011; Devido et al., 2017; Dyess et al., 2017; Newcomb et al., 2014; Rydholm et al., 2008; Wordsworth, 2015; Ziebarth, 2016b). Refer to Table 2 for an overview of the literature characteristics.
Literature Characteristics.

Quality of the literature sample
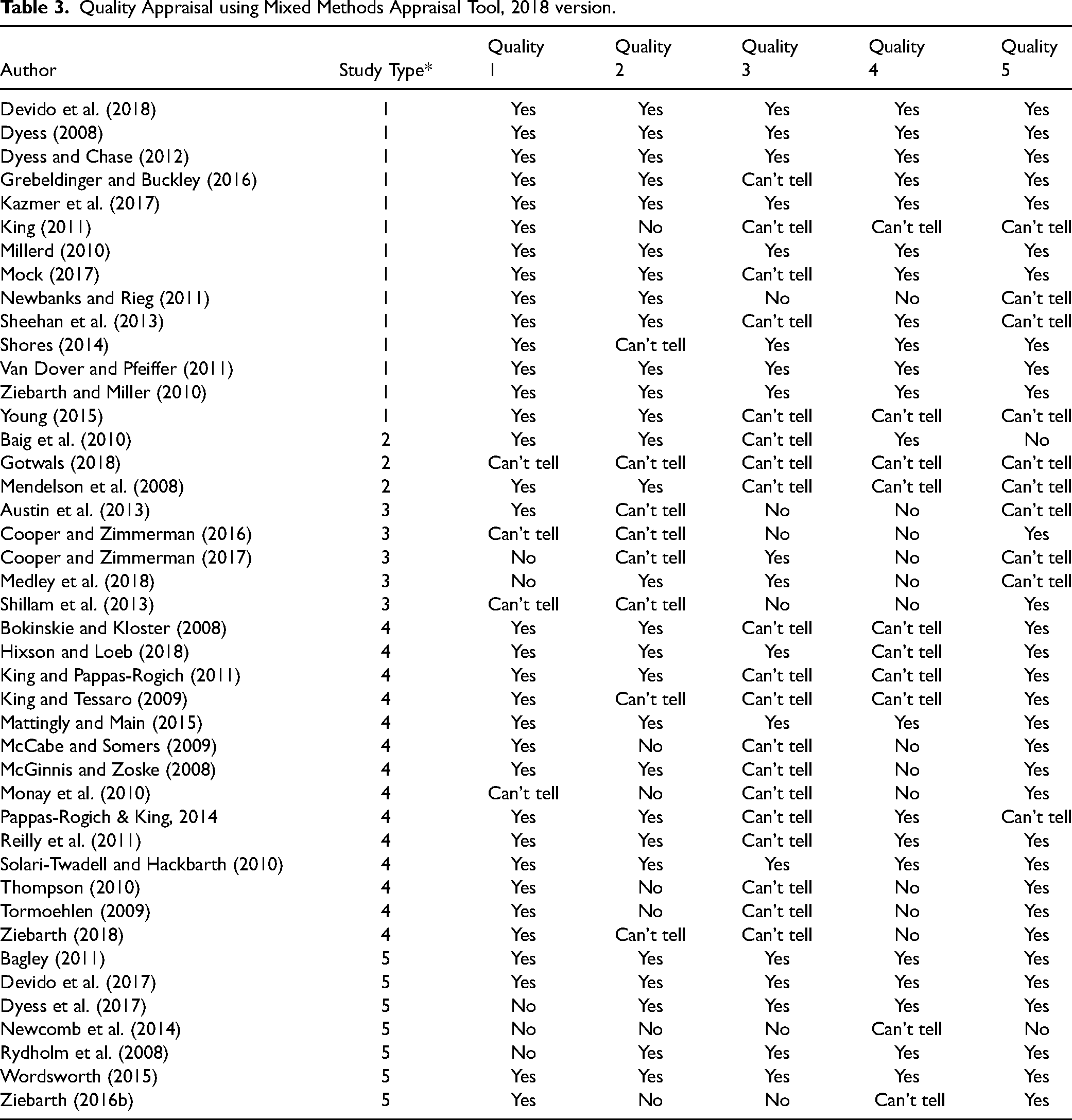
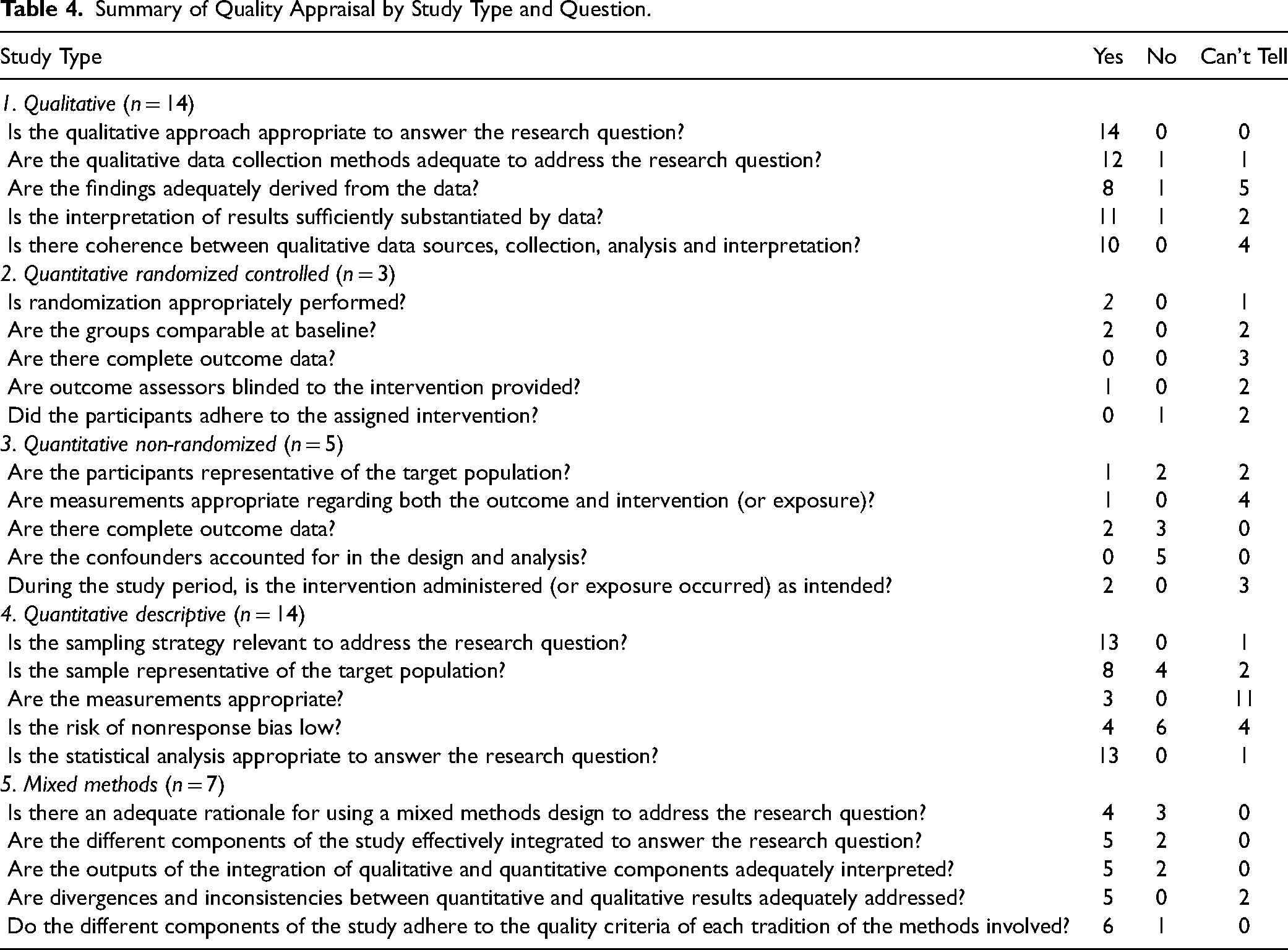
There is a wide variation in quality across all types of the documents. In this section, we briefly summarize the quality of the literature sample based on the results of the MMAT appraisal scores. Refer to Table 3 for a summary of scores and Table 4 for detailed quality appraisal scoring by study type.
Quality Appraisal using Mixed Methods Appraisal Tool, 2018 version.
Summary of Quality Appraisal by Study Type and Question.
Qualitative studies
For the most part, all 14 qualitative studies meet the quality criteria for appropriateness of the methods and reporting of the data collection methods and sources (Devido et al., 2018; Dyess, 2008; Dyess & Chase, 2012; Grebeldinger & Buckley, 2016; Kazmer et al., 2017; King, 2011; Millerd, 2010; Mock, 2017; Newbanks & Rieg, 2011; Sheehan et al., 2013; Shores, 2014; Van Dover & Pfeiffer, 2011; Young, 2015; Ziebarth & Miller, 2010). According to MMAT criteria, there is insufficient evidence to confirm that the findings are adequately derived from the data in six of the 14 studies; we appraised this criterion as “can't tell” in five articles (Grebeldinger & Buckley, 2016; King, 2011; Mock, 2017; Sheehan et al., 2013; Young, 2015) and “no” in one study (Newbanks & Rieg, 2011). Our scoring is based on absent or weak reporting of data analytic procedures with rationale. There is insufficient information to determine coherence between data sources, collection, analysis, and interpretation in four studies (King, 2011; Newbanks & Rieg, 2011; Sheehan et al., 2013; Young, 2015).
Quantitative randomized controlled trials
There are three studies in this study type (Baig et al., 2010; Gotwals, 2018; Mendelson et al., 2008), and reporting is weak for all studies. We are unable to assess whether there were complete outcome data reported in all three studies. We are also unable to determine if outcome assessors were blinded to the intervention (Gotwals, 2018; Mendelson et al., 2008). We rated participant adherence to the intervention as “can't tell” in two studies (Gotwals, 2018; Mendelson et al., 2008) and “no” in one study (Baig et al., 2010).
Quantitative non-randomized studies
We retrieved five studies of this study type (Austin et al., 2013; Cooper & Zimmerman, 2016, 2017; Medley et al., 2018; Shillam et al., 2013). Our appraisal points to limitations related to confounding bias in all five studies. There are also limitations in reporting of measures (Austin et al., 2013; Cooper & Zimmerman, 2016, 2017; Shillam et al., 2013) and sample representativeness (Cooper & Zimmerman, 2016, 2017; Medley et al., 2018; Shillam et al., 2013). We are unable to determine if the intervention was administered as intended or whether there were unplanned co-exposures in three studies (Austin et al., 2013; Cooper & Zimmerman, 2017; Medley et al., 2018).
Quantitative descriptive studies
We retrieved 14 quantitative descriptive studies. The sample is not representative of the target population in four studies (McCabe & Somers, 2009; Monay et al., 2010; Thompson, 2010; Tormoehlen, 2009) and insufficiently reported to determine sample representativeness in two studies (King & Tessaro, 2009; Ziebarth, 2018). Measures are insufficiently described to determine appropriateness in 11 studies (Bokinskie & Kloster, 2008; King & Pappas-Rogich, 2011; King & Tessaro, 2009; McCabe & Somers, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Pappas-Rogich & King, 2014; Reilly et al., 2011; Thompson, 2010; Tormoehlen, 2009; Ziebarth, 2018). Non-response bias is not low in six studies (McCabe & Somers, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Thompson, 2010; Tormoehlen, 2009; Ziebarth, 2018) and indeterminate in four studies (Bokinskie & Kloster, 2008; Hixson & Loeb, 2018; King & Pappas-Rogich, 2011; King & Tessaro, 2009).
Mixed methods studies
There is variation in quality across the seven studies of this type (Bagley, 2011; Devido et al., 2017; Dyess et al., 2017; Newcomb et al., 2014; Rydholm et al., 2008; Wordsworth, 2015; Ziebarth, 2016b). Reasons for using a mixed methods design is not reported in three studies (Dyess et al., 2017; Newcomb et al., 2014; Rydholm et al., 2008). The quantitative and qualitative components are not effectively integrated and adequately interpreted in two studies (Newcomb et al., 2014; Ziebarth, 2016b) and we are unable to determine whether divergence/inconsistencies in the components are adequately addressed in these same studies.
Literature sample themes
The literature is categorized under the following three broad thematic areas: (1) practice roles of the PN, (2) role implementation, and (3) program evaluation research.
Practice roles of Parish nurses
Much of the literature (32 studies) reports the roles of PNs. To provide context to a Canadian audience, we mapped the literature to the roles identified in the CAPNM Standards of Practice (CAPNM, 2021b).
Professional practice and accountability
Three studies focus on professional practice and accountability with two studies reporting documentation practices of PNs (Dyess et al., 2017; Mattingly & Main, 2015) and one reporting the core practices of nurses that define parish nursing as a specialty (Solari-Twadell & Hackbarth, 2010).
Wholistic nursing care
Ten of 43 articles (23.3%) address the role of PNs in providing wholistic nursing care (Dyess, 2008; Dyess & Chase, 2012; Grebeldinger & Buckley, 2016; Hixson & Loeb, 2018; King, 2011; McCabe & Somers, 2009; Rydholm et al., 2008; Sheehan et al., 2013; Solari-Twadell & Hackbarth, 2010; Wordsworth, 2015). Wholistic PN practice involves physical, psychological, emotional, and spiritual support (Grebeldinger & Buckley, 2016; Sheehan et al., 2013; Solari-Twadell & Hackbarth, 2010; Wordsworth, 2015). It is reported to be a primary PN role (King, 2011; McCabe & Somers, 2009; Rydholm et al., 2008) that supports how clients derive personal meaning from life situations and in relationships with self, God, and others (Dyess, 2008; Dyess & Chase, 2012; Hixson & Loeb, 2018; McCabe & Somers, 2009)
Health promotion
Thirteen studies (30.2%) describe the PN role of promoting health (Austin et al., 2013; Cooper & Zimmerman, 2016, 2017; Dyess, 2008; Gotwals, 2018; King, 2011; King & Tessaro, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Newcomb et al., 2014; Sheehan et al., 2013; Young, 2015; Ziebarth, 2016b). Health promotion activities include conducting family histories (Newcomb et al., 2014), health screening, monitoring, teaching (Ziebarth, 2016b), coaching (Austin et al., 2013; Cooper & Zimmerman, 2016, 2017; King, 2011; King & Tessaro, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Young, 2015), and developing/implementing health promotion programs (McGinnis & Zoske, 2008).
Facilitation of spiritual care
Spiritual care activities of PNs are described in 13 of the 43 studies (Dyess & Chase, 2012; Grebeldinger & Buckley, 2016; Hixson & Loeb, 2018; Kazmer et al., 2017; King, 2011; McCabe & Somers, 2009; Millerd, 2010; Mock, 2017; Newbanks & Rieg, 2011; Shores, 2014; Solari-Twadell & Hackbarth, 2010; Van Dover & Pfeiffer, 2011; Ziebarth, 2016b). Two grounded theory studies explore the meaning of PN spiritual care practices (Dyess & Chase, 2012; Van Dover & Pfeiffer, 2011). PNs affirm that spiritual care is very important (Newbanks & Rieg, 2011), and interpersonal skills and spiritual maturity are viewed as necessary PN characteristics (McCabe & Somers, 2009). PNs engage in spiritual care practices among members of their faith communities (Hixson & Loeb, 2018; King, 2011; Mock, 2017), and spiritual support is a frequently documented PN intervention (Solari-Twadell & Hackbarth, 2010; Ziebarth, 2016b). Spiritual support is facilitated by being fully present (Dyess & Chase, 2012; Grebeldinger & Buckley, 2016), active listening, prayer, instilling hope, providing touch, comfort, care, compassion, and kindness (Shores, 2014), and by providing a safe place to release burdens and change perspectives (Van Dover & Pfeiffer, 2011). PNs may experience spirituality as connectedness, centrality in one's being, empowering action, presence in solitude and quiet, and feelings of peace (Millerd, 2010).
Communication and collaboration
Communication and collaboration are described in 12 studies (Kazmer et al., 2017; King, 2011; King & Pappas-Rogich, 2011; McCabe & Somers, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Rydholm et al., 2008; Shillam et al., 2013; Shores, 2014; Solari-Twadell & Hackbarth, 2010; Young, 2015; Ziebarth, 2018). Communication is enacted through health education, active listening and presence (Solari-Twadell & Hackbarth, 2010; Ziebarth, 2016b), and referrals to community resources (McGinnis & Zoske, 2008; Young, 2015). PNs engage in interprofessional care (Rydholm et al., 2008; Shillam et al., 2013), such as with pharmacists to promote medication safety for older adults (Shillam et al., 2013).
Advocacy and ethics
Only four studies specifically address advocacy in PN practice (Dyess, 2008; King, 2011; King & Pappas-Rogich, 2011; Young, 2015). Advocacy is described as a supportive intervention for chronic illnesses management (Dyess, 2008), health promotion (King & Pappas-Rogich, 2011), and healthcare system navigation (Young, 2015). There are no studies that address ethics in PN practice.
Research and evidence-informed practice
There are no studies in our sample that explicitly evaluate the extent to which PNs participate in research and evidence-informed practice. Nevertheless, PNs are reported as being involved in research activities, such as the implementation of research intervention protocols (Austin et al., 2013; Baig et al., 2010; Cooper & Zimmerman, 2016, 2017; Kazmer et al., 2017; Mendelson et al., 2008; Newcomb et al., 2014; Shillam et al., 2013), participant recruitment (Grebeldinger & Buckley, 2016; King, 2011; King & Pappas-Rogich, 2011; Mock, 2017; Shillam et al., 2013; Van Dover & Pfeiffer, 2011; Ziebarth & Miller, 2010), and data collection (Monay et al., 2010; Shillam et al., 2013).
Role implementation
There is a large body of evidence (n = 21 studies) that provides insight into what and how the PN role is implemented (Austin et al., 2013; Bagley, 2011; Bokinskie & Kloster, 2008; Cooper & Zimmerman, 2016, 2017; Devido et al., 2017; Devido et al., 2018; Dyess, 2008; Dyess et al., 2017; Dyess & Chase, 2012; Gotwals, 2018; Grebeldinger & Buckley, 2016; Hixson & Loeb, 2018; Millerd, 2010; Mock, 2017; Pappas-Rogich & King, 2014; Rydholm et al., 2008; Shores, 2014; Solari-Twadell & Hackbarth, 2010; Young, 2015; Ziebarth, 2016b). We categorized this body of evidence into two sub-categories: barriers to PN role implementation and opportunities to enhance PN role implementation in two areas. They are reported below.
Barriers to PN role implementation
Eight studies identify barriers to PN role implementation (Bagley, 2011; Bokinskie & Kloster, 2008; Devido et al., 2018; Dyess et al., 2017; Mattingly & Main, 2015; McCabe & Somers, 2009; Thompson, 2010; Ziebarth, 2018). These barriers relate to time and scheduling challenges (Bagley, 2011; Bokinskie & Kloster, 2008; McCabe & Somers, 2009), insufficient financial support (Bokinskie & Kloster, 2008; Mattingly & Main, 2015; Mock, 2017), isolation from colleagues (Devido et al., 2018), poor systems for documentation (Dyess et al., 2017; Mattingly & Main, 2015), and lack of congregational, volunteer, and clergy support (Bokinskie & Kloster, 2008; McCabe & Somers, 2009; Mock, 2017; Thompson, 2010). Poor leadership, organizational change, and lack of strategic planning for PN programming can result in involuntary PN termination (Ziebarth, 2018).
Opportunities for PN education
Nine studies address gaps in PN education and offer opportunities for curriculum development (Bagley, 2011; Devido et al., 2017; Devido et al., 2018; Gotwals, 2018; Grebeldinger & Buckley, 2016; Newbanks & Rieg, 2011; Solari-Twadell & Hackbarth, 2010; Tormoehlen, 2009; Ziebarth & Miller, 2010). Among these, three studies examine PN perceptions of the quality of their basic course (Newbanks & Rieg, 2011; Tormoehlen, 2009; Ziebarth & Miller, 2010). The literature identifies the need to revise basic courses to better address curricular gaps, including confidentiality (Tormoehlen, 2009), spirituality and spiritual care practices (Bagley, 2011; Tormoehlen, 2009; Ziebarth & Miller, 2010), community nursing knowledge (Ziebarth & Miller, 2010), organizational leadership (Bagley, 2011), and caregiver self-assessment, goal setting, and monitoring (Grebeldinger & Buckley, 2016). Experiential learning needs include enhancements to role modeling, practice hours, and peer support (Ziebarth & Miller, 2010). Finally, the need for post basic training to increase PN self-efficacy in knowledge and counseling in health promotion and disease prevention is also identified (Devido et al., 2017; Devido et al., 2018; Gotwals, 2018).
Opportunities for enhanced PN ministry support
Seven studies (Bagley, 2011; Devido et al., 2017; Dyess et al., 2017; King & Pappas-Rogich, 2011; McCabe & Somers, 2009; Mock, 2017; Wordsworth, 2015) identify opportunities to enhance support for PN ministries. Opportunities exist in five key areas including improved community support for PN programs (Mock, 2017), emotional support for PNs (McCabe & Somers, 2009; Mock, 2017), documentation technology and outcome tracking (Dyess et al., 2017), health promotion and disease prevention (Devido et al., 2017; King & Pappas-Rogich, 2011; McCabe & Somers, 2009), and volunteerism (Bagley, 2011; Wordsworth, 2015). With additional support, there are opportunities for PNs to promote more seamless and efficient health and transitional care services (Devido et al., 2017; King & Pappas-Rogich, 2011; Mock, 2017) and bereavement care (Mock, 2017).
Program evaluation and research
There are nine studies in the literature sample that report outcomes related to the implementation of various health promotion programs and interventions (Austin et al., 2013; Baig et al., 2010; Cooper & Zimmerman, 2016, 2017; Medley et al., 2018; Mendelson et al., 2008; Reilly et al., 2011; Sheehan et al., 2013; Shillam et al., 2013). The majority evaluate educational interventions about specific health concerns, such as: hypertension (Austin et al., 2013; Baig et al., 2010; Cooper & Zimmerman, 2016, 2017), diabetes (Austin et al., 2013; Sheehan et al., 2013), gestational diabetes (Mendelson et al., 2008), colorectal screening (Medley et al., 2018), infection prevention (Reilly et al., 2011), and polypharmacy (Shillam et al., 2013). Kazmer and colleagues (2017) report a cognitive-behavioural and spiritual counseling intervention for dementia caregivers. Five of the nine programs were implemented among sample populations aged 50 and older (Austin et al., 2013; Baig et al., 2010; Medley et al., 2018; Newcomb et al., 2014; Shillam et al., 2013). Age was not reported in three studies (Cooper & Zimmerman, 2016, 2017; Reilly et al., 2011).
Discussion
This scoping review of the international PN research reveals a significant gap in PN research from Canada and non-U.S. countries. It is also the only published review that reports the findings of a critical appraisal of the PN research. The only Canadian study found in the time period was an unpublished thesis (Millerd, 2010). Research that explores the roles of PNs and how they are implemented has continued. Our review specifically highlights the significant roles of PNs in facilitating spiritual care, providing wholistic nursing care, and in health promotion. It also suggests a gap in understanding how PNs engage in spiritual care and advocacy and how they apply ethics and evidence-informed decision-making in their practice. Similar to the findings of Dandridge (2014) review, research that reports the implementation and evaluation of health promotion interventions is prevalent in our literature sample.
Spiritual care
Spirituality is a broad concept that is recognized as a fundamental component of compassionate health care (Puchalski et al., 2009). It refers to the way individuals seek and express meaning and purpose and how connectedness to the moment, to self, to others, to nature, and to the sacred is experienced (Puchalski et al., 2009). Accumulating research evidence suggests that a person's belief in religion or spirituality has a significant impact on health (Mueller et al., 2001). An estimated 5,000 articles are written every year on the positive impact of religion or spirituality on health (Lipton, 2015). Spiritual beliefs also have a direct, positive influence on the activity of the immune and endocrine systems that are important for health maintenance and disease prevention (Lipton, 2015). According to a systematic evidence-based analysis (Bonelli & Koenig, 2013), religious involvement is correlated with better mental health in the areas of depression, substance abuse, and suicide.
The focus on spiritual care practices distinguishes parish nursing from other nursing specialties. Facilitation of spiritual care is one of the CAPNM standards and its indicators describe care expectations (CAPNM, 2021b). In this review, 13 studies describe a range of PN spiritual care practices (Dyess & Chase, 2012; Grebeldinger & Buckley, 2016; Hixson & Loeb, 2018; Kazmer et al., 2017; King, 2011; McCabe & Somers, 2009; Millerd, 2010; Mock, 2017; Newbanks & Rieg, 2011; Shores, 2014; Solari-Twadell & Hackbarth, 2010; Van Dover & Pfeiffer, 2011; Ziebarth, 2016b). Although spiritual presence is noted as a practice (Grebeldinger & Buckley, 2016; Millerd, 2010; Shores, 2014), the ‘what’ and ‘how’ of spiritual care and its integration with other domains of PN practice has not been rigorously studied. A qualitative study by Canadian researchers (LeBlanc-Kwaw et al., 2020), published after our search, examines the process PNs use to develop the spiritual practice of presence. The basic social process involves cultivating the soul to become a channel of God through steps of presence that involve the self, God, and others (LeBlanc-Kwaw et al., 2020).
Health promotion
This review emphasizes the significant health promotion role of PNs within churches and communities. Promoting healthy lifestyles and healthy behaviors prevents health problems and reduces health risks and threats (Public Health Agency of Canada, 2017). In the PN research, health is largely promoted through activities of health screening, teaching, coaching, and referral, based on physical factors of health (Austin et al., 2013; Cooper & Zimmerman, 2016, 2017; Dyess, 2008; Gotwals, 2018; King, 2011; King & Tessaro, 2009; McGinnis & Zoske, 2008; Monay et al., 2010; Newcomb et al., 2014; Sheehan et al., 2013; Young, 2015; Ziebarth & Miller, 2010).
This is a narrow view of a PN's opportunities to promote health. According to the WHO (2021), health promotion “moves beyond a focus on individual behavior towards a wide range of social and environmental interventions” (para.1).
In Canada, the determinants of health include: income and social status, employment and working conditions, education and literacy, childhood experiences, physical environments, social supports and coping skills, healthy behaviors, access to health services, biology and genetic endowment, gender, culture, and race/racism (Government of Canada, 2020). A greater understanding of how these dimensions of health are being addressed by Canadian PNs would add value to the nursing literature and PN practice. Future exploration should employ more wholistic and population health definitions of health promotion and consider relevant frameworks, such as the Ottawa Charter for Health Promotion (WHO, 1986) and the Population Health Model (Hamilton & Bhatti, 1996).
Although advocacy is a key process for promoting health, the work of advocacy among PNs is not well reported. The Ottawa Charter for Health Promotion (WHO, 1986) states that the “fundamental conditions and resources for health are peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice and equity” (p.1). It also states that health promotion must aim to make these conditions favorable through advocating for health, enabling people to control determinants of health, mediating between differing interests of society for the pursuit of health, building healthy public policy, creating supportive environments, strengthening community action, developing personal skills, and reorienting health services. These are ways in which PN ministries in Canada should seek opportunities to advocate for the health of faith communities and broaden the impact of parish nursing by implementing more upstream approaches to health promotion.
Recommendations for education and practice
The findings of this review reveal several areas which should be better addressed in PN certification and continuing education programs. As integration of spirituality into nursing care is integral to the PN's practice, more time needs to be given to the development of this skill in basic PN programs, mentoring programs, and continuing education courses. PN courses should include a focus on EBP. To enable PNs to more rigorously evaluate their interventions and programming, curricula in PN certification programs should foster competency in EBP, research, and quality improvement methods. Cultivating relationships with faculties/schools of nursing in Canada as well as health organizations that have resources to support EBP, such as libraries and health databases, would support PNs to remain up-to-date in best evidence and offer continuing education and research opportunities for Canadian PNs.
The review also highlights the need for increased support for PN ministries in Canada and internationally. Self-efficacy and empowerment as leaders were identified in several studies (Bagley, 2011; Devido et al., 2017; Devido et al., 2018; Gotwals, 2018). PNs identify participatory education, mentoring, and a relationship with a higher power as means for supporting their empowerment (Weis et al., 2006). Volunteerism is another area for PN ministry support. According to Wordsworth (2015), churches in the United Kingdom with PNs have twice as much volunteer coordination and support and increased time to address the wholistic care needs of people who do not normally go to church, thus positively affecting the mission of churches. Finally, financial, clergy, and parish leadership support affirm the contributions of the PN and promote PN wellbeing (Bokinskie & Kloster, 2008) and are therefore, important for retaining PNs in the nursing workforce.
Recommendations for research
There is a need to support international research in parish nursing. Parish nursing is practiced in 29 countries around the world (Westberg Institute, 2021); yet, there is a dearth of research published outside of the United States. Funding to support PN research and collaborations with nurse researchers would advance PN research in Canada. More rigorous methods are also needed to evaluate the outcomes of PN interventions in populations across the lifespan, especially children and youth. There is no research that assesses the impact of parish nursing on healthcare system outcomes, such as primary care and hospital utilization. The cost effectiveness of parish nursing for faith communities, the broader community, and the healthcare system is also not known, although a model to measure its economic benefits in prevention has been proposed (Ziebarth, 2016a). Improved reporting of methods and findings would improve the credibility of PN research for evidence-informed practice. Publication checklists are readily available in the public domain from the UK EQUATOR Centre (n.d.) to support the reporting of various research study types. Because the economic value of a resource often helps organizations determine whether or not the resource is of value and should be maintained, these latter research foci would be helpful in demonstrating the importance of funding and retaining PNs in the community sector.
Research related to the ethical practices of PNs is lacking. Given the new and changing ethical issues in contemporary healthcare and the reality that many PNs practice in their own faith communities, it is expected that PNs experience ethical dilemmas in their practice. In Canada, the legislation of Medical Assistance in Dying (MAiD) necessitated the generation of guidelines for PN practice related to MAiD (CAPNM, 2017). Because federal legislation “does not change the PN's commitment to the people he/she cares for” (CAPNM, 2017, para. 1), it is important to explore how PNs navigate client and family decision making about MAiD and other ethical issues. Participation in client decisions and discussions about end-of-life and assisted dying are likely to have a direct personal and professional impact on PNs. They can lead to moral distress (Rice et al., 2008) and moral residue (Kopchek, 2020) among nurses and have a potentially negative influence on PN retention in the nursing workforce.
Limitations
This scoping review focused on available English articles through the searches identified. There is a possibility that the authors have not identified published material that was available through other data sources; therefore, they are missing from this review. We eliminated nine articles that did not meet methodological screening criteria and that may have added useful information to this review. The elimination of these articles points to further methodological weaknesses in PN research than documented in this review. Although the authors of the MMAT (Hong et al., 2018) provide clear quality criteria/indicators, and we implemented a two-reviewer scoring process, we acknowledge that there was subjectivity and therefore bias in our scoring.
Conclusion
This scoping review of the PN research literature highlights the specialized practice of PNs. There is a significant gap in PN research in Canada and in high quality research internationally. The literature is organized around three themes: practice roles of the PN, role implementation, and program evaluation research. PN practice roles include professional practice and accountability, wholistic nursing care, facilitation of spiritual care, health promotion, advocacy and ethics, communication, collaboration, and evidence-informed practice. Role implementation opportunities exist for PN education and ministry support. Health promotion is a dominant research area, particularly the evaluation of PN educational interventions programs related to health education and screening for chronic disease. Researchers undertaking PN research should consider using more rigorous methods where appropriate and reporting checklists to increase the validity and reliability of research for evidence-informed PN practice. PN alignment with ethics boards and university researchers could advance PN research. Research into the cost effectiveness, healthcare outcomes, and the economic value of PN practice is needed.
Footnotes
Acknowledgments
The authors acknowledge the following members of the original CAPNM research team: Rosalyn Thompson, BN, RN, Cheryl Gibson, PhD, RN, and Claudia McCloskey MEd, RN, for their contributions to the original analyzes of articles. Keith Thompson helped to manage the numerous articles by merging the original literature spreadsheets.
Committee member Laura Van Loon supported our analysis work and reminded the team of the importance of this research. The documentation support of Faith Cormier, CAPNM Board Member Liaison, kept us on track, always with her signature wit and humour.
This scoping review and the work behind it would not have been possible without the spiritual support and direction from Mark Miller, PhD. He often provided the ‘big picture’ motivation we needed to navigate through the details and keep our eyes on the goal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.