
Abstract
In the early months of the COVID-19 pandemic in 2020, vessels were suspended across the oceans, unable to dock and with passengers and crew denied local permission to disembark. These scenarios were another way in which the effects of this virus were understood to be ‘unprecedented’, seemingly disrupting existing protocols, regulations and lines of authority. However, this article historicizes the stranded cruise ship in examples from the late nineteenth and early twentieth centuries along Australia's coastline. By focusing on the finer processes of maritime quarantine that have shaped this nation, the authors argue that maritime quarantine routinely worked across and between multiple authorities, almost always crossing jurisdictional boundaries. Furthermore, these processes engaged with rapidly changing information between domestic and international ports to effectively manage outbreaks of infectious diseases, frequently using the vessel's mobility as part of the quarantine strategy.
After the severe acute respiratory syndrome in 2003, Convery, Welshman and Bashford asked ‘Where is the border?’ Just before COVID-19, Graziano asked ‘What is a border?’ 1 In the light of the global pandemic, it is germane to wonder what new answers to these questions have arisen. We know that responses to the virus worldwide were crudely spatial in the first instance. The management of sometimes highly local intrastate borders came strongly to govern conduct and to serve as the key preventive strategy before vaccination. Indeed, this prominence and governance of internal borders has challenged a historiography of disease management that has long problematized international borders. 2 Yet there is another kind of medico-legal border that was in operation early in the coronavirus moment, one that raised a particular and peculiar historical geography: the ambiguous space between coastlines and cruise ships.
In this article, we reconsider the early months of 2020 when vessels with suspected or infected passengers or crew were suspended in the Caribbean and the Mediterranean, and in the Pacific and Indian oceans. Adjacent to key ports, cruise liners found themselves unable to dock, with passengers and crew denied local permission to disembark. These vessels were caught between much more than ‘the devil and the deep blue sea’, as one journalist popularized the predicament of the Artania, for example, which was stranded off the coast of Western Australia. 3 In the chaos of early 2020, multiple authorities were unclear and conflicted about which regulations governed that permission, and at what risk to which populations. Tightly packed cruise ships could turn overnight from clean to infected zones – from ‘healthy’ to ‘hospital’ ground, to use antiquated quarantine terminology – to become some of the least safe confined localities on the planet.
Retrospectively obscured by the massive global crisis that was about to unfold, the phenomenon of the stranded cruise ship was one of the most historically resonant elements of early 2020. But how do we place these episodes in the long history of disease, maritime quarantine and medico-legal border control? What old geographies and established legalities were raised and refreshed as cruise ships were suspended and even sequestered along global coastlines? Were such ‘coronavirus’ ships like old quarantine hulks or the ‘diseased’ ships that sailed aimlessly through the eighteenth-century Mediterranean, unable to dock once plague or cholera was declared? Or were they more like the later steamships, caught between race-based immigration jurisdictions – notably, the Komagata Maru taking Indians via Hong Kong to Canada in 1914, where they were denied permission to leave the ship, which was forcibly escorted out of Canadian waters and back to India, with fatal consequences? 4
To some extent, the Komagata Maru comparison is a true one: cruise ships across the world's waters in early 2020 were caught between sea and land; between jurisdictions, including those of the various nationals on board; between domestic law, international health conventions, maritime regulations and unregulated prejudices. Indeed, recent scholarship on the plight of cruise ships in the early months of the pandemic has highlighted the ambiguities and loopholes present in the international frameworks regulating the maritime world, the rights of seafarers in comparison to travellers, and the rights of port states. 5 Yet, in historicizing the stranded coronavirus vessels, we argue that comparison with such extraordinary and (rightly) sensational precedents sidesteps the more direct and even obvious precedent of routine maritime quarantine. By focusing on historical events along Australia's coastline, we show how the governance of ambiguous terraqueous space, and negotiation of swiftly changing intelligence on disease, was the everyday business of quarantine in a maritime world that extended well into the twentieth century.
While the world was seemingly thrown into disarray with the adjustments in the management of coronavirus, maritime quarantine procedures were specifically designed for just such contexts. The scale of the pandemic certainly highlighted the capacity limitations of maritime quarantine, but the procedures and adaptations have long been in place for potential microbial and viral incursions. By turning to the finer process of maritime quarantine in Australia, we investigate what these adaptive processes relied on to function reasonably well. Rather than understanding the early months of 2020 as an unprecedented crisis, the historical instances analysed here demonstrate that maritime quarantine routinely worked across and between multiple authorities, almost always crossing jurisdictional boundaries. The three historical instances – one in 1899 and the other two in 1938 – were responding to smallpox and cholera, diseases that had an established scientific and cultural identity. But we have chosen these instances as they show how quarantine typically functioned by responding to, and engaging with, the problem of rapidly changing information, including confirmation of disease through diagnostic tests and epidemiological intelligence between one port and another (Figure 1).
We reconsider the history of ships, disease, coastlines and quarantine through the geography of the large island nation of Australia. In their study on disease management and migration in the United Kingdom and Australia from 1950 to 2000, Convery, Welshman and Bashford show how polities have different sites for the implementation of medico-legal border control. 6 Australia had long been globally atypical, with practices defined by its island status in a maritime century. Key health borders were firmly located outside its own territory, at the point of departure, at a time when most polities operationalized such borders (as health checks) at the port of arrival. In such processes, borders were, and are, a function as much as a place, but the globally typical place was coming to be the territorial edge. 7 The United States, for example, performed quarantine at the domestic islands where customs and immigration were also governed – famously, Ellis Island in New York City or Angel Island in San Francisco. In the United Kingdom, medico-legal border control did not even operate at the point of entry (port or airport) but within its own territorial borders: at-risk travellers and immigrants would be referred by various border authorities to the local health authority of their final destination. 8
There is a well-established scholarship that has explored and explained how biosecurity and national (and nationalist) governance have been folded together in the Australian instance, including the strong racialization of biosecurity. The foundational White Australia policy was implemented through the Immigration Restriction Act, which had a disease clause. Conversely, maritime quarantine powers were used to refuse entry to non-whites. 9 This was not unique over the nineteenth and twentieth centuries, but it was geopolitically intense. The need for a critique stands, but the race–immigration–biosecurity triad is now well known and strongly researched. What, then, if we press, and even substantiate, the challenge to move ‘beyond quarantine critique’? 10 On the one hand, highly problematic social inequities prevail in the twenty-first-century maritime world, and intensified during the COVID-19 pandemic, especially regarding the different treatment of classed and racialized crew and passengers. 11 On the other, we are interested here in how the circumstances that threw authorities, ship's captains, crew, passengers, and local and national governments asunder in early 2020 were akin to the everyday port business of an earlier maritime world. In short, we wish to de-exceptionalize the events of early 2020 on Australia's Indian Ocean and Pacific Ocean coastlines by contextualizing them within three historical instances sparked by the different diseases of smallpox and cholera.
Coronavirus, 2020
On 19 March 2020, between the early hours of six and seven in the morning, 2,700 passengers disembarked from the Ruby Princess, ‘scattering’ onto Sydney's foreshores. 12 This cruise vessel had been cleared by the Australian Border Force, Australian Commonwealth Department of Health and New South Wales Health Department to enter and berth in Sydney Harbour, deeming the 128 reported instances of illness, of which 120 were in quarantine on board, low risk. On that same day, the Australian government announced that Australia would be closed to all non-residents and non-citizens as of 9 p.m., 20 March, after weeks of escalating travel restrictions. This ‘unprecedented step’ was taken by the Australian government because ‘80 per cent of coronavirus cases in Australia’ were people who had just returned from overseas or had had direct contact with someone who had returned from abroad. 13 The virus had to be kept out of the country. However, the virus had already entered via the Ruby Princess. The routine testing of two passengers who were taken to a Sydney hospital for other medical complications returned positive results for COVID-19 at 9.04 p.m. on 19 March. But the test labelling did not identify the patients as Ruby Princess passengers. It was also decided that the 13 swabs collected on board for testing on land could wait for the ‘10 a.m. run’, after being transported to the testing facility at 3 a.m. These samples were not tested in that run because they were not labelled as a priority. This unfortunate series of events meant that it was not until mid-morning the next day that health officials were made aware that passengers, now on land and in the wider community, had contracted the virus.
What ensued was one of the largest outbreak clusters in Australia in the early months of the pandemic, when the novelty of the virus provoked alertness, anxiety and alarm. According to the Ruby Princess's Human Health Report, a required document for port entry submitted at 7.21 p.m. on 18 March, 128 persons had reported ill in the previous 14 days. Eventually, tests showed that 21 of these 128 (17.5%) had COVID-19. As a result, 1,682 passengers from Australia and 663 other passengers from overseas residencies (39.4%) contracted the virus. Out of a crew of 1,148, 191 (16.6%) also became infected. When the Special Commission of Inquiry report was published in August 2020, there were 28 deaths (20 in Australia and 8 in the United States) associated with the Ruby Princess, while the extent of the related cases and deaths amongst the international passengers, which made up a third of the passengers on board, is unknowable. 14 The Inquiry report details the multilayered ‘lack of communication and coordination between various agencies’ in this episode, as well as highlighting the complexities that exist in the process of docking a cruise ships in Australian ports. 15 Peter Hobbins compared this incident with a contained outbreak of smallpox discovered after the landing of passengers from the Aorangi in 1929, calling that voyage the Ruby Princess’s ‘prequel’. Certainly, the comparison reveals how ‘medical misdiagnosis, slipshod paperwork, conflicting jurisdictions, and a clash of powerful personalities’ can combine and expose the vulnerabilities of a quarantine system. 16 However, what we want to highlight in our historical comparisons are the adaptive ways in which maritime quarantine would routinely deal with outbreaks and slippages in diagnosis.
The Ruby Princess was neither the first nor the last cruise ship to be scrutinized for the spread of COVID-19 in the first few months of the pandemic. In early February that year, the Diamond Princess came into the international spotlight when she was placed under quarantine off the port of Yokohama with 712 people infected and 14 of those people dying during the 39 days at sea (all the while the crew continued to work untested). 17
Closer to Australian shores, the Ruby Princess incident was used as a warning by the Western Australia government. When the Artania, Vasco da Gama and Magnifica all sought to dock in Fremantle a few days after the Sydney incident, the state premier Mark McGowan referred to the ‘complete and utter disaster’ of the Ruby Princess and promised that he would ‘not allow what happened in Sydney to happen here’. 18 The Magnifica had been given permission to dock in Hobart on 14 March, the same weekend that Tasmania closed its ports to cruise ships, but the liner's management would not permit passengers to disembark if they wished to continue on the cruise. 19 The ship's captain decided that it was safer for his passengers to remain on board because Tasmania had recorded six cases on land. Indeed, the Magnifica would retain her clean bill of health, remaining completely COVID-free as she journeyed across the Southern Ocean, Indian Ocean and Mediterranean Sea seeking an open port, before she was finally allowed to dock in Marseilles on 20 April, six weeks after her passengers had last been on land (Figure 1.

Map of Australia showing the relevant ports discussed in this article.
The concept of the ‘clean’ or ‘infected’ status of vessels has long been a guiding principle of maritime quarantine. How a vessel is designated takes into account the disease type, disease incidence during the journey, vessel type, and health status of the port of departure, as well as the type of passengers. 20 The process was codified in the International Sanitary Conventions of the late nineteenth century, and the subsequent International Health Regulations formed the basis of Australian quarantine procedures for granting vessels pratique. Under Australian practices, cruise vessels have negative pratique until their Pre-Arrival Report, which is completed 12 to 96 hours before their estimated arrival at their first Australian port and assessed by a biosecurity officer. Should the paperwork report one individual passenger or crew member presenting with signs or symptoms consistent with a Listed Human Disease (human coronavirus was included on 21 January 2020), the vessel must await further assessment by either a biosecurity officer or a human biosecurity officer. 21 There is a low bar, and understandably so, for a vessel to be treated as ‘infected’ or at least suspected of being infected. This sense of suspicion, in light of the consequences of the Ruby Princess, fed into the Western Australia government's commitment to deny the Magnifica permission to dock. In the routine information provided by the Magnifica, there were 298 recorded passenger visits to the vessel's medical team in the previous 14 days, but the report maintained that ‘none of these individuals suffer from any respiratory disease or present any flu-like symptoms’. 22 However, it was not a risk the Western Australia government was willing to take because, ‘in this environment [it could not] take risks and [would] always put the Western Australian community first’. 23 Being designated as a ‘healthy’ or ‘infected’ vessel was, and is, not simply about disease presence; rather it is a contingent classification that reveals an alertness towards the risk of particular microbes.
Despite a clean bill of health (not having a suspected or current Listed Human Disease on board), the Magnifica was not permitted to disembark any of her 1,700 passengers or crew, none of whom were Australian citizens or residents, in Fremantle. The Swiss-owned vessel anchored off the coast while she tried to find a port at which to dock. 24 While the West Australia state government and the Australian federal government were not compelled to provide further assistance to the Magnifica, the German-owned cruise ship Vasco Da Gama was carrying 800 Australians on board, with 150 other nationals, and 550 crew. At first, the Western Australia government had directed the Australians on board to quarantine for two weeks on Rottnest Island, just off the coast, but it became clear that the 800 passengers exceeded the island's capacity, and all passengers and crew were required to remain on board or until repatriation flights could be arranged for any non-Australians. 25 This public health directive was taken even though no passengers had reported illness or tested positive for COVID-19. The Artania, which was also German-owned but had no Australian nationals on board, reported illness amongst her 800 passengers and eventually returned seven confirmed cases. She was then allowed to dock under customary international law, whereby port states must provide assistance to ships in distress. 26 Several passengers were evacuated for hospitalization, and the majority of the passengers disembarked directly to board a plane back to Germany (which was more than Australian nationals abroad could do under the Commonwealth's no-right-to-return policy). 27 The 450 crew, however, and a handful of passengers remained on board as arrangements were not made until mid June to repatriate the last of the passengers and some crew while the ship was docked in Bremerhaven. The remaining crew stayed on board awaiting further instructions about crew changes. 28
The variety of experiences encountered by these ships with a suite of national and state governments, managing different nationals, reflects the speed of change to regulations that characterized the early months of the COVID-19 pandemic. However, procedures and responses were not simply being invented, even if they were ineffective or even positively harmful: they relied on well-established maritime procedures that governed the cruise and shipping industries nationally and internationally. And these procedures were well established historically. The treatment of the Artania, whereby sick patients were quarantined on land, was routine practice and familiar, for example, in Australian ports throughout the nineteenth and into the twentieth century. The treatment of the Vasco Da Gama, whereby the ‘clean’ ship was not permitted to land, was more unusual, although similar to eighteenth-century Mediterranean quarantine practices in which suspect ships often had to sail from port to port, seeking permission to dock. 29 Yet this all unfolded in a context declared to be chaotic. Of course, the presence of a wholly new microbe accounts for the declaration of a crisis. But there was also a disconnect with, or forgetting of, an earlier maritime world in which such circumstances were, if not routine, at least to be expected and certainly planned for. As with so many other elements of the COVID moment, such apparently unprecedented events were, in fact, recognizable in earlier times, not least in the history of cruise shipping itself.
Smallpox: the SS Afric, 1899
The complexities of law and authority evident in the coronavirus cases, and the confusion over what action would best mitigate the threat of disease, were not uncommon in historical instances of maritime quarantine. Scholars have generally focused on how intersecting regulations affected the mobility of migrants through race-based practices when disease was suspected or erupted on board. 30 Here, we focus on how various legal and administrative complexities were being handled and interpreted by quarantine and health officers across the Australian colonies that, in 1901, federated into the Australian states.
In 1899, the SS Afric sailed on her maiden voyage from Liverpool to Albany in Western Australia. On 18 October, she entered the port flying a yellow flag, signalling that she had illness on board. The Afric had sailed via the Cape, picking up just over 100 passengers and most likely the variola virus. The inspecting health officer, Dr Ingoldby, confirmed that the six reportedly ill passengers had, indeed, developed smallpox, and two others were suspected cases. 31 The ship was placed in strict quarantine, anchored off the coast, and no one was allowed to board. The vessel itself was the border between clean and unclean zones. However, the 19 passengers who had booked a ticket to Albany were allowed to disembark, and they entered land quarantine for a minimum stay of 21 days – the three weeks typically stipulated for smallpox. This would be the first use of the new quarantine buildings at Albany. 32
The different interests of the stakeholders emerged almost immediately – a perennial problem that quarantine systems were designed to alleviate, but not always successfully. The Afric's captain requested to offload the confirmed smallpox cases in Albany, indicating that ‘he [would] not continue the voyage unless he [was] allowed to do so’. 33 His concern was to reduce the ‘danger of infection spreading amongst the other passengers’. 34 However, the local health officer ‘had no power to do anything, and ha[d] to wire Perth for information’. 35 The colony was subject to the Quarantine Ordinance 1868 and the Quarantine Act of 1888, but neither law stipulated where the sick on board should quarantine or be isolated – rather, that it was at the discretion of the appointed medical officer. 36 However, the Western Australian Immigration Restriction Act 1897 defined anyone suffering ‘from a loathsome or dangerous contagious disease’ as a prohibited immigrant. 37 And any prohibited immigrant found in the colony would be ‘liable, in addition to any other penalty, to be removed from the Colony’. 38 With no other caveats providing for infectious-disease carriers, there was ambiguity as to whether these smallpox sufferers could land. This conundrum did not escape one commentator, who saw this as evidence of a pressing need to implement a federal (that is, national) quarantine service beyond ‘shaking hands’ and ‘agree[ing] that such co-operation was necessary’. 39 In a not dissimilar way, even with a national quarantine regime in place, cruise ships during the 2020 moment required individual state permission to dock. 40 But this was not a result of unclear ordinances, as it was for the Afric; rather, it was the assertion of a state’s rights through the declaration of emergency powers, which Western Australia had put into effect on 18 March 2020. 41 When the Magnifica arrived at Fremantle on 23 March after disembarking a few passengers in Sydney and Melbourne, the Western Australia government refused her request to dock in order to refuel, stating publicly, but erroneously, that 250 passengers on board had upper-respiratory illnesses. Eventually, working with the national Australian Border Force, the Magnifica was permitted to refuel under state and federal supervision to ensure that no one could ‘wander the streets’. 42
In 1899, while clarification was sought between the Western Australian departments, Messrs. Dalgety and Co., the agents for the Afric, received instructions from their Sydney branch to sail to Adelaide, which she did that evening. 43 But at the same time, the undersecretary of the Western Australian Medical Department intercepted Dr Ingoldby's request and decided that the Afric was allowed to land the smallpox patients into the quarantine hospital, provided that the ship's agents supply the medical attendance to look after them. Dr Ingoldby could not find an available doctor and did not want to board the Afric himself at the expense of his other duties. 44 In light of this shortage, the acting principal medical officer in Perth arranged for a doctor to go to Albany the next day, but the Afric had already sailed at 10.30 p.m. the night before. 45
We see here the extent to which the docking of ‘unhealthy’ ships was complicated by multiple and sometimes competing authorities. In this 1899 instance, the smaller regional health district of Albany was subject to vague colonial laws, directed towards immigration regulation rather than public health. White Star Liners took it upon itself to manage its own vessel through their agent by seeking an additional medical opinion from another Australasian colony, Victoria. When the company's agent consulted Dr Gresswell, chair of the Victorian Board of Public Health, he advised that a ‘medical man’ be sent to Adelaide to join the vessel, where he may start vaccinating the passengers and crew, reducing the quarantinable time. 46 Whether to keep the smallpox cases on the Afric thus became a multi-sited and multi-authority question about disease risk management.
We might assess this 1899 instance as chaotic, but in fact it points to the generic complexity inherent in maritime quarantine procedures. They were handled in better and worse ways, but the declaration of an infectious disease on a vessel moving between jurisdictions, especially when it was foreign-owned, was always a difficult procedure, quickly changing as new information came to light. And in the particular case of smallpox, the already long-standing and well-documented procedure of vaccination, including fair knowledge of how well and after how long a vaccine provided immunity, added another level of management and time process for the declaration of safe or clean, or risk-free passengers.
In a similar way, when the Ruby Princess docked in Sydney, she was subject not just to the federal immigration and customs requirements affecting her passengers and crew, but also to several other Commonwealth and New South Wales Acts relating to biosecurity. On the national scale, the Biosecurity Act 2015 outlines the management of ‘diseases and pests that may cause harm to human, animal, or plant health or the environment’ of Australia, with consideration of the nation's obligations to international regulations such as the International Health Regulations and the United Nations Convention on the Law of the Sea. 47 The administration of the Act is split between the Department of Agriculture, Water and the Environment (responsible for ‘biosecurity’ matters) and the Commonwealth Department of Health (responsible for ‘human biosecurity’). This bifurcation means that there are also two directors, one for each portfolio – the Director of Biosecurity and the Director of Human Biosecurity – with biosecurity officers and human biosecurity officers working in each state and territory under their respective divisions. The Director of Human Biosecurity, who is also the Commonwealth's Chief Medical Officer, is empowered to declare a disease a Listed Human Disease, which human coronavirus was declared with pandemic potential on 21 January 2020, two months before the Ruby Princess docked in Sydney. Under the Biosecurity Act 2015, all vessels, including cruise ships, fall under the responsibility of the Department of Agriculture, Water and the Environment to grant pratique or permission to ‘allow things to be unloaded from, and persons to disembark from, aircraft or vessels’. 48 Pratique is automatically granted to incoming vessels unless a ship has declared even just one case of a passenger or crew with symptoms indicative of a Listed Human Disease, as defined by the International Health Regulations. In such a case, a biosecurity officer will need to grant pratique on a case-by-case basis, but there is no clarity on whether this is to be granted by biosecurity officers from the Department of Agriculture, Water and the Environment or the Department of Health. 49 While this is just one instance of the multiple authorities to which ships are subject, the intersecting, overlapping and competing interests of state, national and company bodies are a constant in border biosecurity, and have long been so.
When the Afric arrived in Adelaide on 23 October 1899, seven additional smallpox cases had developed since leaving Albany and were ‘sickening every day’, and there was ‘no more room in the hospital’ on board. 50 Like quarantine stations, ships have demarcated hospital spaces to isolate the sick from the healthy. The regulations for these spaces on board were dependent on where the vessel was registered and, at times, the route they sailed. 51 The variability of regulations internationally was emphasized in a 1917 study by the Australian Quarantine Service as an impediment, but also a reality, of the maritime world. 52 According to the Service’s publication, the Afric's hospital accommodation consisted of two cabins – one for men and one for women – with four bunks in each to cater for a maximum of 506 passengers and crew. 53 With 13 cases of smallpox in 1899, it was already five beds short. Not only was there an overflow of smallpox patients, but the hospital cabins on the vessel were adjacent to the passenger accommodation, and thus ‘suitable only for non-infectious cases’. 54 The spatial arrangements of these cabins put other passengers at risk. This is one design element that sets the 1899 and 2020 examples apart. Cruise ships like the Artania have individual purpose-built units, and when passengers on this cruise ship reported a respiratory-like illness, they were isolated in their cabins, as per the ship’s protocol. 55
However, the variability of ship protocol was a factor in the case of the Ruby Princess. Even as isolation and non-essential travel rules were being issued by the Australian Commonwealth government and communicated to the Ruby Princess on its altered return journey to Sydney, passengers were not required or asked to isolate and ‘the ship operated as normal’, with ‘all shows and entertainment continued’. 56 Yet there were notifications throughout the voyage, reminding travellers of ‘good personal hygiene protocols’ as part of the ‘[e]nhanced cleaning protocols’. 57 Focusing on disinfecting humans and the surfaces of a vessel is an extension of what Engelmann and Lynteris envision as ‘hygienic fumigation’ – practices for population health aimed ‘against a disease in the knowledge of its ability to kill its agent’. 58 While the fumigation of ships is no longer practised, sanitizing and making a show of ‘disinfecting’ a ship still relies on specialized chemicals and procedures to attain certification before the next departure. This may be simple hygiene, but the materiality of cruise ships and their linens, carpets and surfaces were thrown into suspicion in 2020 as being conveyors of disease. In 1899, the ‘hygienic fumigation’ of a ship could only take place once all humans had disembarked.
While, in early 2020, the rules and expectations regarding close contact and ‘social distancing’ seemed highly novel and strange, these, too, had their antecedents in ports. Given the high risk of infection in 1899, no one was permitted to make contact with the Afric herself or ‘even touch the ship's gangway’. 59 Instructing them verbally, the crew on board the Afric prepared and lowered the sick patients and their luggage down on the ship's boats. The three boats, with the passengers in the last one, were towed to the quarantine station on Torrens Island. The only exceptions to the no-contact rule were the inspecting doctor and Dr Howard, the ‘medical man’ from Melbourne, who was instructed to board the Afric and vaccinate the remaining passengers.
The borders between ship and shore were also closely monitored in 2020. The Magnifica, although initially denied pratique in Fremantle, was eventually permitted to dock and refuel under the guard of state police and national border officers to ensure that there was no human contact with land, before being escorted offshore to anchor. 60 In this process, the spatial movement and contact of both seafarers and port workers was subject to regulation too. As the pandemic wore on, and as the importance of keeping ports open and classifying seafarers as essential workers became clear, state governments issued their own regulations to permit maritime work with the least risk. On 27 March 2020, Maritime Safety Queensland introduced a process to identify Essential Maritime Service Workers, so that maritime services to the far north of the state could continue. 61 By contrast, Western Australia was still being petitioned in October 2021 by the Maritime Union of Australia to include seafarers in the essential workers list. The state permitted international maritime crew changeovers, but domestic seafarers were not permitted to move interstate or intrastate to join vessels offshore. 62 While these restrictions focused on human movements onshore and offshore, New South Wales’ COVID-19 Maritime Quarantine Order of 11 December 2020 stipulated that any work that required a seafarer to be on land must be completed within ‘13 metres from the wharf at which the vessel was docked’. 63 Such micro-borders around ships in maritime quarantine were mobile zones that extended and contracted around the vessel, and were dependent on the microbe, state regulations and the temporal distance from the initial outbreak. Both historically and in 2020, it was never just the vessel itself, but also the space around it, that came under suspicion and regulation.
Cholera: the Kamo Maru, 1938
There were, and always are, many variables in any maritime quarantine event. The journey of the Kamo Maru in 1938 illustrates that while inconvenient, quarantine was an adaptive and flexible system that not uncommonly worked. She sailed from Nagasaki on 23 August, arriving in Hong Kong on 27 August, where she was in stream tied to a buoy. 64 None of the third-class passengers were allowed onshore, and no water was taken on board. 65 Eleven passengers, who were originally on the Hakusan Maru and had not been onshore in Hong Kong, boarded the Kamo Maru to continue their journey to Australia. The contact and the passage was ship to ship. They were also third-class passengers – Russian emigrants with inoculation certificates, honouring Australia's offshore health requirements. 66 The vessel then arrived in Manila on 30 August ‘at the usual quarantine anchorage’ and, upon medical inspection, all passengers and crew were found to be well. 67 The first- and second-class passengers were granted permission to go onshore, but the third-class and steerage passengers were kept on board because of the trans-shipped passengers at Hong Kong. 68 Eight of the steerage passengers disembarked at Manila because it was the end of their ticket and, as per routine quarantine procedures, were taken to hospital for further checks. 69
On 3 September 1938, the chief quarantine officer of Queensland, Paul Mitchell, informed Australia's federal director of quarantine, J. H. L. Cumpston, that Manila had telegrammed to alert him that those eight disembarked steerage passengers were confirmed cholera-carriers: they were asymptomatic and were doing well. 70 To deal with a potential outbreak on board, epidemiological knowledge was needed, and a plan of action was put in place. First, Cumpston requested intelligence about the ship's movements in Manila with regard to ‘what actions taken at Manila re ships [sic] water, foodstuffs, disinfection of steerage bedding or other sanitary precautions’. 71 Manila telegrammed a day later, stating ‘no suspicion [of] ship origin’ and assuring him that ‘those removed [at] Manila [were] not engaged in handling ships [sic] water or foodstuffs [and] all bedding belong[ing] to passengers … [was] removed’. They ‘believe[d the] ship [was] safe on sailing’ to Australia. 72 We see here a continuation of the early modern and eighteenth-century suspicion of goods and materials as much as human bodies. 73
With this reassurance that the ship itself was clean, a plan of action was put in place to ensure there were no more human carriers. The vessel continued to Thursday Island but was denied pratique by the federal administration directing the Kamo Maru to Brisbane for medical inspection. Coordinating medical inspections between land and a ship was not straightforward in March 2020 either. Testing for coronavirus was not yet widespread, unlike for cholera, and the testing infrastructures that were available were already stretched. The batch mislabelling and testing delays in the handling of the Ruby Princess samples attests to this difficulty. When the Kamo Maru sailed to Thursday Island in the Torres Strait, two second-class passengers with tickets for this port were allowed to land, despite the vessel not being given pratique. But four third-class passengers with tickets to Thursday Island were ‘treated as steerage and [directed to] proceed to Brisbane. These passengers [were] virtually steerage’. 74 It was not until the Kamo Maru arrived in Brisbane on 14 September that an inspection of the third-class and steerage accommodation was made, and the earlier decision to permit one class of passengers to land but not the other was retrospectively justified because the accommodation for third class and steerage ‘was so intimate that no distinction from a health point of view could be made’. 75 What becomes apparent in this episode is that continual hygienic vigilance alternated between the ship, the passengers and the materials on board. This was facilitated by international and cross-border epidemiological communication not just for disease surveillance as a precautionary mechanism, but also for the microbial scrutiny of specific parts of a ship.
Knowing who did and did not have an infectious disease was an obvious but complex element of quarantine decisions. By the 1930s, diagnostics had moved far beyond the basics of clinical diagnosis from signs and symptoms. Now, for some diseases, even asymptomatic ‘carriers’ could be diagnosed, but the techniques involved multiple steps and the equipment was specialist. On 14 September, 60 people – 17 third-class and 43 steerage passengers – were tested and placed under quarantine in Brisbane until the results were returned. While the Kamo Maru journeyed from Thursday Island to Brisbane, a doctor and his assistant themselves travelled quickly to Brisbane to set up the testing laboratory by 13 September, a day before she was due to arrive. Diagnostic tests for cholera had largely been standardized in the 1910s, after Robert Koch identified the bacterium responsible for cholera in 1883. 76 The procedure involved a rectal swab collection being incubated in peptone water or agar. The former medium was able to return preliminary results in six to eight hours, and further testing would be done to confirm, using the Dieudonne method or a cholera red reaction. Between the overseeing doctor, his assistant and a female nurse, they collected and processed the 60 samples within six hours. The preliminary results were available by 6 p.m. that evening, clearing 48 of the passengers. They were allowed to continue their journey on the Kamo Maru, which, during that same time, had her third-class and steerage accommodation and bedding fumigated. Boat, bedding and bodies were cleared, gaining the Kamo Maru permission to sail for Sydney, leaving 12 passengers behind awaiting further results by the Dieudonne method, which would come back negative for cholera the next day. 77 In this historical instance, a temporary laboratory, medical personnel and a ship were efficiently moved to the port best equipped to run the essential diagnostics in service of successful quarantine.
The experience of the Kamo Maru in 1938 shows how routine maritime quarantine relied on quick decision-making, using the mobility of a vessel to facilitate the best course of action to identify, and thus prevent, further cases. In the 2020 moment, these characteristics of maritime quarantine led to two different scenarios. In the case of the Ruby Princess, the rapid decision to disembark her passengers led to an outbreak. Indeed, the diagnostics had not yet caught up with the new coronavirus in February and March 2020, so the testing contexts for cholera and coronavirus are dissimilar. COVID testing still required a laboratory, and cruise ships only carried equipment to take samples or testing kits for Influenza A and B, which could have suggested a case of COVID-19 but not diagnose it. But we saw that the Artania and Vasco Da Gama used their mobility, or rather lack of mobility, to deal with suspicion of disease. They were suspended in time and space, waiting not just for protocol to be agreed upon, but also for laboratory results to slowly come in, and indeed for diagnostic testing to be refined.
Smallpox: the P&O liner Strathaird, 1938
Although the elaborate procedures for maritime quarantine historically developed in and around intercontinental travel and migration, both in the Age of Sail and the Age of Steam, they extended into the emerging twentieth-century industry of maritime tourism and leisure: the cruise. On 25 March 1938, a Miss Adams, sailing across the Indian Ocean from Bombay to Perth, developed haemorrhagic smallpox on the Strathaird. It was unsuspected on arrival, and she was only placed into quarantine two days after she had disembarked. She died on admission. The Strathaird was en route to Adelaide when the federal government alerted the captain of her death and informed him that his ship was ‘refuse[d] permission’ to embark the 100 plus tourist passengers waiting for them at the next port. 78 The second action, and indeed Australia's second line of defence against imported diseases, was the vaccination of any of the close contacts – those who had disembarked at the same time – and the federal government instructed the vessel to proceed with the vaccination of unvaccinated persons, ‘starting with the tourist class’ – Miss Adams’ class of travel. 79 The chief quarantine officer of South Australia, Dr Ponsford, boarded the vessel in Adelaide to inspect and vaccinate the remaining 119 unprotected passengers. 80 Furthermore, the cruise segment from Brisbane to Fiji was cancelled, with over 1,000 passengers affected, and arrangements were made to refund their fares and return them to their port of embarkation.
Like the Kamo Maru that same year, the mobility of the vessel itself was productively deployed. The Strathaird's journey around the Australian coastline from Adelaide to Melbourne, and then Sydney to Brisbane, was used to oversee and decide which passengers were eligible for disembarkation at each port under quarantine, under surveillance or without restrictions. Three medical officers from the quarantine service were on board consecutively to direct the operation. Aside from administering and monitoring the vaccinations, these officers inspected the vessel's accommodation, disinfected the necessary zones and decided which passengers could disembark at each port, processing them into different categories of mobility on land. How this was decided largely stemmed from Dr Ponsford's examination of the vessel's accommodation and facilities in Adelaide, where he concluded that there was ‘only a small degree of contact between tourist and saloon [first-class] passengers’ on board. 81 First-class passengers booked to disembark in Adelaide were released under surveillance, but tourist-class passengers were held in quarantine either on the vessel or on land for the remainder of the quarantine period, or until medical officers were certain of their immunity. Upon hearing that first-class passengers were able to disembark without entering quarantine, another 12 first-class passengers disembarked in Adelaide, choosing to travel by rail interstate – a pattern that was repeated by other first-class passengers bound for Sydney and Brisbane when the Strathaird arrived at Melbourne. While these non-contacts had greater freedom of movement, passengers bound for Brisbane who were considered ineligible for release under surveillance were ‘retain[ed] in Q[uarantine] station’ when they arrived in Sydney. They would be sent ‘by rail next Tuesday on expiry of Q period’. 82 The idea was for the Strathaird to sail from Sydney in quarantine but be out of quarantine by the time she arrived in Brisbane; by sailing on with only ‘clean’ contacts, the risk from the vessel was neutralized.
The apparent discriminatory decision-making was communicated to the press by some tourist-class passengers. As with COVID detention on cruise ships, the inconvenience and the rationales for the decisions were publicly questioned. ‘This quarantine is stupid humbug’, complained one Reverend Mr Blackmore in 1938, as he ‘could not understand why they [traveller-class passengers] were detained and those in the first-class released’ because it was ‘incorrect to state that there was no mixing between the tourist and first-class travellers’, as all classes mingled throughout the vessel. 83 Although not fully explained in the media, the distinction between the contact status of passengers allowed the quarantine service to operate a staged release of passengers, which was praised by the ship's captain and by P&O. 84 In Melbourne, for example, while all tourist-class passengers were first quarantined, many were released under surveillance from the vessel a day after the first-class passengers (29 March), when it was clear that their vaccination certificates were valid.
In the processing of the Strathaird in 1938, we can also see how Australia's national quarantine procedures and processes were evaluated by government bodies, similar to the Ruby Princess, but on a smaller scale. At the conclusion of the Strathaird's quarantine, G. A. Murray, the chief quarantine officer of Western Australia, wrote to Cumpston, the director of quarantine, drawing attention to ‘certain aspects [that] call for careful consideration’ in the design of the nation's biosecurity. All three suggestions sought greater surveillance of, and action on, passengers and vessels coming from Indian ports in particular: (1) any passengers coming from Indian ports exhibiting symptoms of fever for less than four days should be placed into land quarantine; (2) the incubation period surveillance should be increased because the current 14-day period was the ‘bare minimum of safety’; and (3) recent successful vaccination certificates should be required for mail ship lines departing from Indian ports because there was ‘apparently permanent adoption of local cruises’ by that class of vessel, and to bring it in line with the aviation requirement. 85 In 1934, certificates of vaccination against smallpox were required for anyone flying into Darwin, then the only airport in Australia. 86 While medical checks, and in particular smallpox vaccination certificates, were required of certain classes of workers and migrants entering Australia by boat, these regulations relied on health checks in domestic ports. For example, Miss Adams stated in the hours before she died that she had only been vaccinated a week before leaving Bombay, but according to the attending doctors, this was ‘without result and there was no sore of any kind detectable’. 87 Interestingly, in responding to the question raised by Western Australia, the federal department stated that it ‘could not be made a requirement by this Department’ to ask shipping companies to ‘obtain vaccination certificates in respect of passengers embarking from Indian ports’. This was a ‘voluntary action’, but ‘suggesting some such action to shipping companies’ would ‘receive consideration’, particularly as ‘it would not be equitable to place on the shipping companies the cost of maintaining’ the extended quarantine of passengers. 88
Recognizing the limitations of its jurisdiction, the Commonwealth Department of Health turned towards evaluating domestic processes after the Strathaird incident. Responsibility was pushed back onto the chief quarantine officers of each state, stating that personal communication between these state officers ‘as the vessel proceeded from port to port in quarantine was insufficient. Too much was left to the Central Office’. It recommended that ‘all points of epidemiological interest’ should pass directly between each state’s chief quarantine officer to ‘greatly facilitate … the quick and smooth handling of the vessel and all persons in it’. 89 The second matter requiring consideration was ‘allowing passengers released under quarantine to travel by road’. This period was a ‘critical time of the surveillance period’ and, from the experience of the Strathaird, many ‘failed to report’ to authorities after starting their journeys on land.
Similarly, the on-land repercussions of quarantine (or lack thereof) of the Ruby Princess in 2020 expose the confusion created by multiple authorities with regard to the prevalence of interstate travel. Within days of disembarking the 2,700 passengers from the Ruby Princess on 19 March, it was clear that COVID had spread interstate (Figure 2). The Special Commission of Inquiry found that the directive permitting onward interstate and international travel ‘did not appropriately contemplate or comply with’ the New South Wales public health order that was effective from 17 March. 90 This order required anyone who had been outside Australia in the two weeks immediately before arriving in the state to self-isolate for 14 days. However, passengers were told on 16 March the advice from the Australian Border Force, stating that the isolation period was dated to the vessel's last port of call at Napier, New Zealand, on 15 March. Although this advice was updated by the Commonwealth Department of Health to the date of arrival and communicated to the Ruby Princess when she docked in Sydney, the Inquiry found that what some passengers understood was consistent with the lapsed Australian Border Force instructions. 91 To compound the issue, passengers were informed they were ‘close contacts’ on 20 March, but at the same time were incorrectly advised by NSW Health that they could travel between states and beyond. When the state authority realized this mistake late on 21 March, it was already too late to stop the spread. Unlike the Strathaird, the reviewers of the Ruby Princess episode recognized that ‘occasionally someone will make a mistake’, given the pace of procedural and advisory changes. 92 Thus, the suggested recommendations to bolster pre-arrival health checks and procedures were to address ‘this perennial aspect of human (including bureaucratic) behaviour’ as part of maritime quarantine. 93
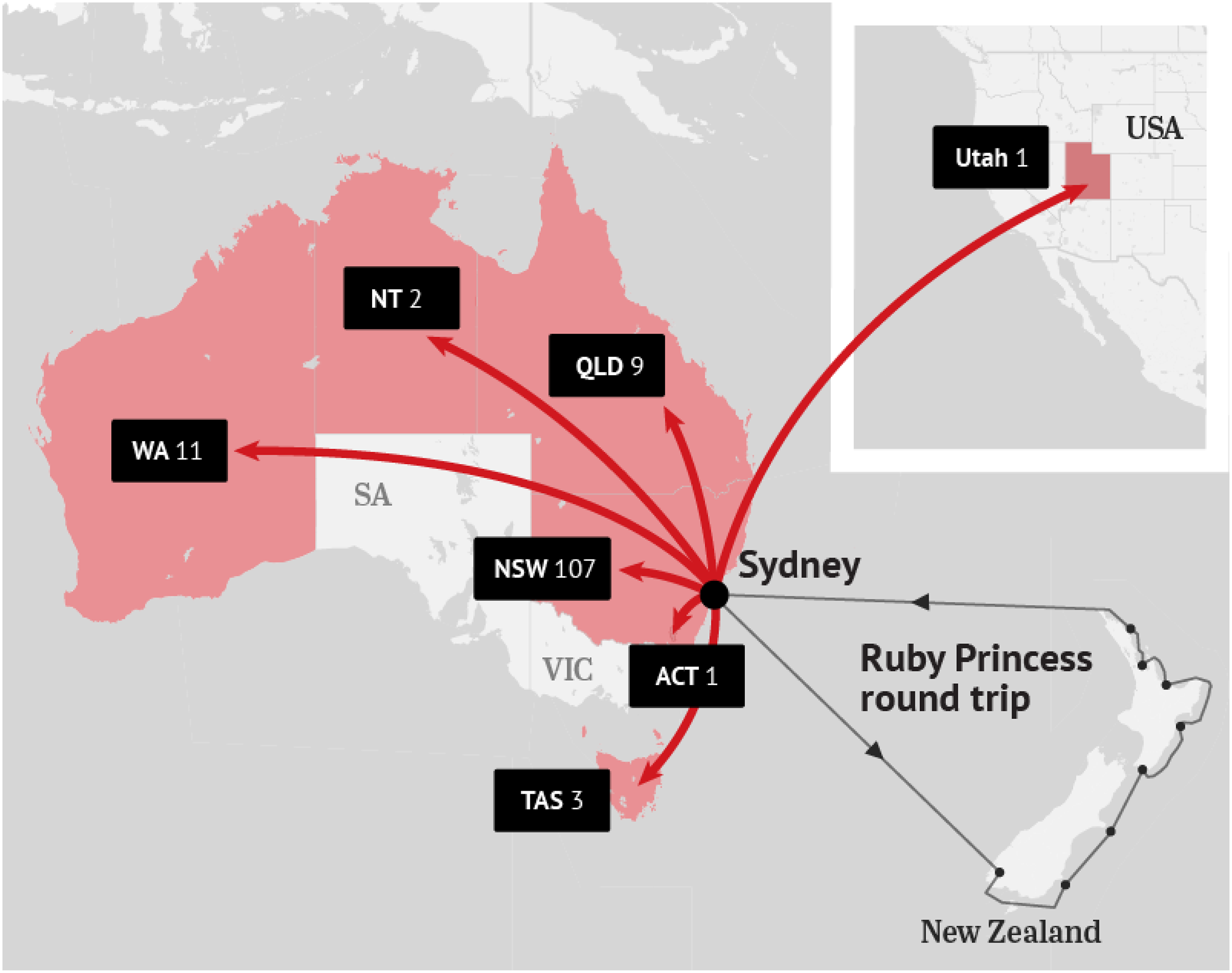
COVID-19 cases originating from the Ruby Princess according to NSW Health.
Conclusion
What unfolded on Australian coastlines in March 2020 was duplicated in oceans and seas across the world. Like everything else that the new coronavirus unleashed, the response to stranded cruise ships was assessed as chaotic. Between Hong Kong and Japan, for example, the Diamond Princess was in no-man's-land. ‘As contagion swept through the Diamond Princess’, the Guardian reported, ‘its crew had to carry on working … they recall the climate of chaos and fear that prevailed during the ship's two-week quarantine’. 94 Without diminishing the fear, and indeed the chaos, and while recognizing the precarious novelty and danger of the new virus, and the mortality and morbidity that was even then apparent, the situation of the cruise ships was not dissimilar to the three historical cases explored here. Any number of other historical instances, in Australian waters alone and not just that of the Spanish flu in 1919, could be analysed similarly. Perhaps of all the coronavirus-inspired changes, this was the least ‘unprecedented’ – the word constantly used to assess COVID-19. Logistically and even legally, the regular quarantining of vessels and people formed clear precedents, in which the complexity of jurisdictional authority and decision-making according to time, distance and disease was standard business. The procedures, policies and experience of maritime quarantine were all long-standing, even if the many variables and officials meant ill-judged decisions, and even if discrimination between passengers and crew was problematically tolerated.
In many ways, the management and managers of COVID-19 had to catch up with historically well-established practices like quick, in-situ diagnostic technologies and the expectation that isolated sailing days could serve as quarantine. The history of maritime quarantine in these instances shows us how the mobility of the vessel itself, as it travelled between ports and jurisdictions, was not aimless confusion but a productive mobility. The captain of the Afric, in consultation with health officials in other colonies, decided to move the vessel to a port that was better equipped and experienced in dealing with smallpox in 1899, while maintaining her ‘social distance’. In 1938, the redirected voyage of the Kamo Maru facilitated efficient disease diagnostics that required a coordinated movement of personnel and a laboratory to meet with the ship, as seen with Western Australia's management of cruise ships in 2020. Similarly, in order to manage a potential outbreak of smallpox, the Strathaird's health professionals boarded to vaccinate passengers, while her disembarked passengers were located and vaccinated, highlighting how maritime quarantine can also reach inland. But in each historical instance, the ship's mobility was put to use in disease management itself, with varying success, much like the experiences of the Ruby Princess, Artania and Vasco da Gama off the Australian coastline. While coronavirus itself was ‘unprecedented’, the maritime quarantine procedures and logic deployed were routine.
Footnotes
Acknowledgements
We would like to thank the peer reviewers for their helpful guidance and our colleagues who have helped to refine this article at various stages.
Funding
The research for this article was funded by the Australian Research Council's Special Research Initiative (SR200200683).