
Abstract
The islands of the West Indies are often considered the most dangerous places for eighteenth century British sailors. Contemporary sources maintain that the level of sickness and mortality in the West Indies crippled the Royal Navy's fleet to such an extent as to render it extremely ineffective during the American Revolutionary War. There can be no doubt that disease, accidents and naval action had an effect on the Royal Navy in the West Indies; however the true extent of the impairment has been grossly exaggerated. This paper seeks to examine the precise effects of disease and mortality on British sailors stationed in the West Indies during the American War of Independence.
Keywords
In the second half of the eighteenth century, the islands of the West Indies were vitally important to Britain's war efforts. They supplied much-needed financial support. Valuable commodities such as sugar, cotton, tobacco and coffee were grown on several British-held islands, all of which were transported to Europe and sold in the market. Following the Seven Years War, the principal islands under British control were Jamaica, Antigua, Barbados, Grenada, Dominica and St Kitts. In the years preceding the American War of Independence, import values from those islands ranged from £35,000 to £112,000 per annum. Although the money raised by the imports was considered essential, the real value to the British was the property and stock invested in the West Indies. At the outbreak of war in 1775, the value of the property and stock was estimated at £30 million, and by 1788, despite the ravages of war, the value was said to be £70 million. 1
In order to protect these lucrative islands and the valuable commodities plying the Atlantic waters, the Admiralty organised a system of convoys and maintained two West Indies bases – one at Jamaica and one at Antigua. At each location, the Admiralty constructed dockyards to ensure a reasonable degree of logistical support for visiting warships and entered into agreements for victualling with local contractors. The Admiralty divided the protection of the West Indies into two squadrons: the Jamaica Squadron and the Leeward Islands Squadron. Each had its own commander-in-chief, and each was under separate orders to protect a range of islands. Ships on the Jamaica station cruised between that island and the western Caribbean Sea as far south as Trinidad and as far north as Pensacola and the Mississippi River. Antigua had traditionally been the seat of the Leeward Islands station, although during the American War of Independence, ships repositioned to a base at St Lucia for a time. On that station, ships routinely cruised as far north as the Virgin Islands while also patrolling Barbados, St Lucia, Martinique and as far south as Grenada.
At the commencement of the American War, exportation of goods from the West Indies was not immediately disrupted as that region did not figure prominently in the hostilities. As a result, the quantity of naval seamen required on the station remained relatively low. Once France formally entered the war on the side of the rebelling colonies in 1778, Britain realized that its West Indies holdings were vulnerable to attack. Striking swiftly, Britain attacked and captured St Lucia from the French later that year, although France's navy quickly responded to Britain's aggression by capturing Dominica, Grenada, Montserrat, St Kitts, St Vincent and Tobago. In order for the British to defend against further invasion, the number of seamen in the West Indies increased substantially (Figure 1).
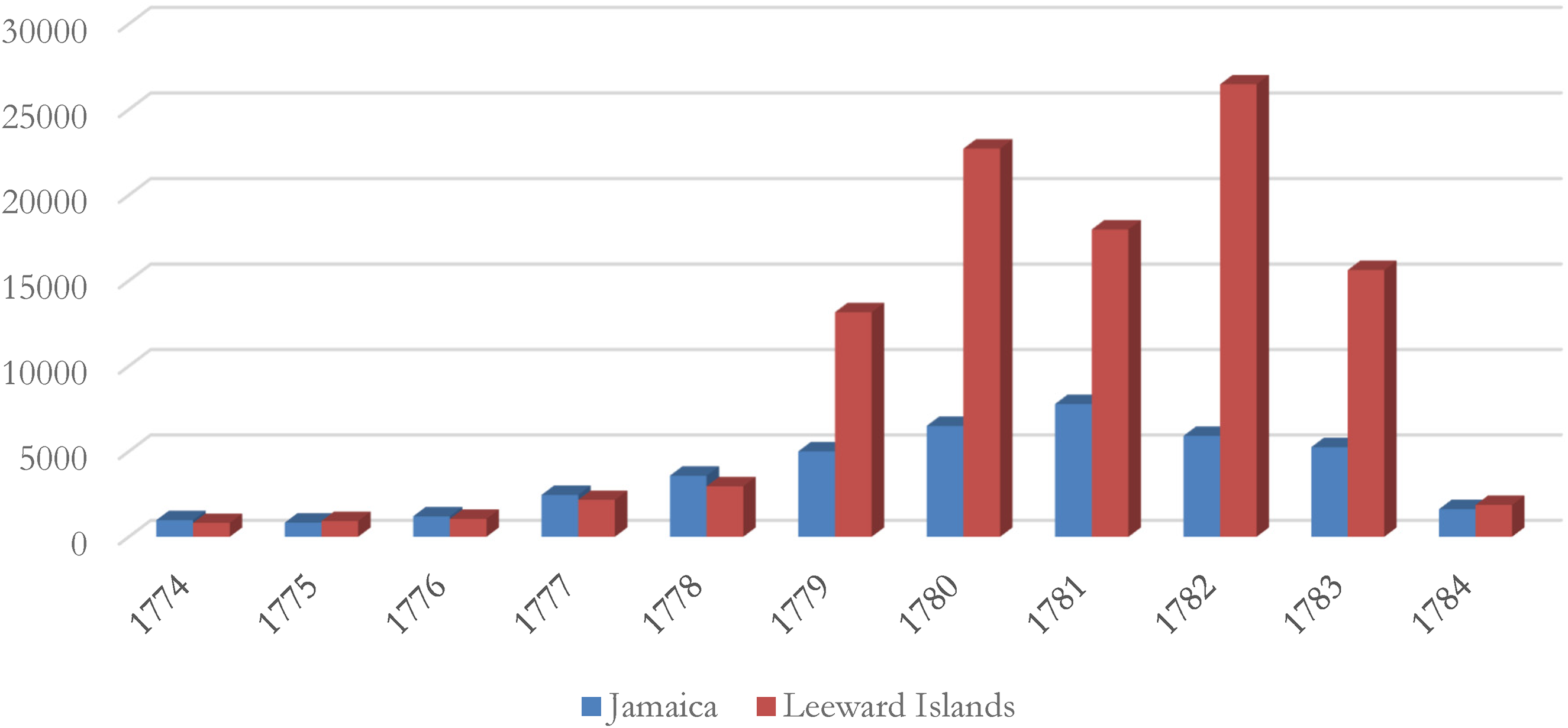
Number of British Seamen in the West Indies, 1774–1784.
Historians have long assumed that many of these men were sent to their deaths. Sickness and mortality levels in the West Indies during the eighteenth century, it is common to read, were acutely high. The consequences of the disease-ridden environment extended not only to the men doing the dying but also to the strategists responsible for coordinating operations in the theatre. This essay seeks to test these assumptions by measuring precisely the prevalence of disease and mortality amongst Royal Navy sailors onboard vessels operating in the region during that conflict. 2 It will establish that levels of sickness and mortality were not staggeringly high when taken as a whole, although there were isolated, sporadic exceptions. It is based on an analysis of ships’ muster books, and it assesses both the number of sick men onboard ships as well as overall mortality rates. Moreover, the essay will briefly discuss the factors that contributed to seamen's health by using the journals and correspondence of both vigilant admirals and the surgeons who administered effective medicines and supplies, both preventative and curative. These resourceful men kept the seamen healthy and demonstrated that they were fully aware of the benefits of maintaining sanitary conditions on Royal Navy ships.
Eighteenth-century commentators were nearly unanimous in proclaiming the West Indies to be deadly to seamen, and historians have too often uncritically taken their word for it. In the four volume series, Medicine and the Navy, authors Lloyd and Coulter refer to English Harbour, Antigua as the ‘grave of Englishmen’ while also maintaining that ‘to be sent out in a big line-of-battle ship to a tropical climate such as that of the West Indies [was], … under prevailing hygienic condition, to invite disease if not death’. 3 Similarly, Sir James Watt claimed that the entire West Indies region was the ‘white man's graveyard’. 4 N.A.M. Rodger's view more closely reflects the true situation: although ‘service in the West and East Indies was unpopular with many … heavy losses on several well-known expeditions should not lead us to exaggerate the real risks of ordinary service’. 5 This is not to suggest that the West Indies was not a deadly place – it certainly was for the army and the Royal Marines. Both branches were required to spend an abundance of time on shore, being exposed to ‘unhealthy airs’ or ‘miasmas’. Naval captains considered it essential to keep their ships as far offshore as possible in order to avoid ‘land air’, as it was deemed especially unhealthy. By putting a fair distance between the ships and stagnant bodies of water such as swamps and marshes, the favoured breeding ground of mosquitoes, seamen had virtually no chance of coming into direct contact with them unless they were ordered ashore. Unsurprisingly, the army and Marines suffered sickness and mortality to a greater extent, supporting the theory that the West Indies was deadly for one and all. 6
To Rodger's point that a few catastrophic expeditions led to inflated perceptions of overall mortality, one of the most recognised examples of a disastrous large-scale operation is Admiral Vernon's 1741 expedition to conquer Cartagena. He and the ships under his command departed Britain carrying some 26,600 men and almost immediately upon his arrival in South America, yellow fever seized his squadron. The disease caused Vernon to lose approximately 9000 men (both seamen and troops) and the entire mission was labelled a complete disaster. 7 Joint expeditionary forces like Vernon's forced naval personnel to spend more time on land than was customary. Thus, despite its best efforts, the navy was not always afforded the luxury of keeping its seamen off shore. The Grey-Jervis expedition of 1794 also saw heightened mortality among seamen for this reason. 8 Yet these were the exceptions to the rule. In fact, seamen's health in the West Indies throughout the second half of the eighteenth century, and more specifically during the American War of Independence, was comparable with that of other regions, both at home and abroad. 9 During that particular conflict, sickness and mortality were by and large under control and the majority of seamen ordered to the West Indies returned to Britain alive with most available for further service.
One reason the West Indies were not especially deadly to seamen was that death rates were high everywhere. In the eighteenth century, it is ‘easy to forget how small a proportion of Europe's adult population would have been healthy at any one time’. 10 Life on board a sailing ship was gruelling and injurious. Ships teemed with refuse, rotting provisions, rats, insects, dirt and unclean drinking water. It is not surprising that these conditions resulted in diseases becoming fairly prevalent. Provisions for seamen to bathe themselves and launder their belongings were not supplied by the navy, meaning that the men regularly slept in filthy hammocks and wore the same soiled clothing for months at a time.
Overcrowding was also a considerable problem. Seamen worked closely alongside one another, possessing very little individual space, which further encouraged the spread of disease. Moreover, ships generally sailed from Britain carrying more seamen than were needed to operate the sails and guns because the Admiralty calculated that a percentage would succumb to illness and wounds. If its estimations were correct and a certain percentage of seamen died, a sufficient number of seamen would still be able to man the vessel. In doing this, the Admiralty created a vicious circle. Initially, by placing an excess number of seamen on board, it made ships extremely overcrowded and promoted the spread of disease. Problems with overcrowding were especially true in larger ships-of-the-line. In those larger vessels, the calculated amount of space per seaman was substantially less than the allocated space in smaller frigates and sloops. As a rule of thumb, seamen in smaller ships were generally healthier because of the extra personal space; also, they were generally ordered on cruising duties which kept them offshore and away from disease-carrying insects.
It is the presence of those disease-carrying insects in the West Indies that explains why historians have long assumed that mortality rates were higher there than elsewhere. To help quantify the levels of sickness and mortality in the West Indies during the American War, a survey was carried out on the majority of ships on both Jamaica and the Leeward Islands stations, tallying up the total number of men on the sick list as well as the number who died, and compared them with the total number borne. The data was compiled using Admiralty muster books belonging to ships on both West Indies stations. 11 Once muster books were identified for each ship, figures were recorded from the summary page of each bi-monthly muster submitted to the Admiralty including the number of men ‘Borne’, the number ‘Mustered’ and those ‘Sick’. Ships’ companies were typically mustered four times per calendar month, meaning that each bi-monthly record had eight sets of figures. Within each bi-monthly muster record, each seaman's name was recorded along with their status on board ship (active, discharged, dead or run) as well as the ship's location at the time the muster was taken. When a seaman was recorded as having died during his service in the West Indies, the date and cause of death (if specifically noted in the muster book) were also recorded. 12 Following the assemblage of all this data, it was then possible to calculate the percentage of men who suffered from disease on the ships and those who died.
Since the Admiralty maintained two separate stations, direct comparisons can be drawn between the two. Firstly, we can look at reported sickness figures for a year when Britain was not at war when the number of seamen on both stations was relatively low (Figure 2). Prior to the outbreak of war in 1775, the number of men suffering from illnesses averaged around 2% at the beginning of the year. Every August through January, the Admiralty anticipated and prepared for an intensification in sickness levels. Those particular months corresponded with the rainy season in the West Indies, during which time pooling of water and flooding of mangrove zones was commonplace. Those areas of standing stagnant water provided the perfect breeding grounds for fever-carrying mosquitoes and the rise in sickness in the course of those months is predominantly the result of seamen falling ill with either malaria or yellow fever. Even with the onset of the sick season in 1775, the Leeward Islands station, the sicker of the two, had less than 7% of its squadron on the sick list. Translated into actual numbers, that meant, for instance in the Leeward Islands, that out of the 563 men on station in March, 17 men were sick. At the peak of the sick season in October on the same station, 32 men were on the sick list out of 425.
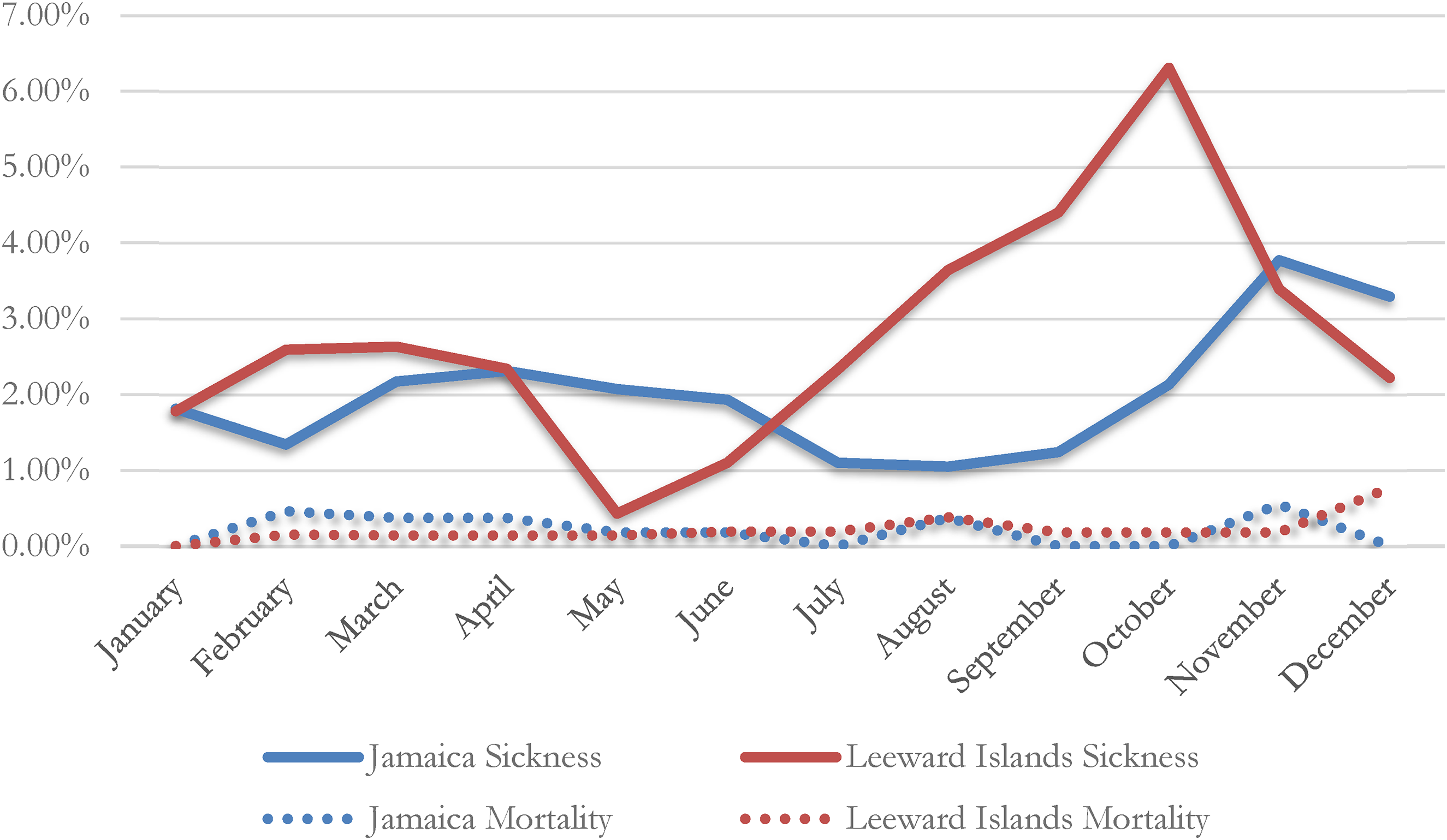
Sickness and mortality levels on two West Indies stations, 1775.
Using the muster books, it is also possible to ascertain the mortality rates on both stations (Figure 2). These figures are perhaps startlingly low given the reputation of the West Indies in the eighteenth century. Even during the sickly season, mortality rates remained well under 0.75%. That translates roughly to one person perishing per month per station; and it is worth bearing in mind that mortality figures also include death from battles and shipboard accidents. For instance, a total of 14 seamen belonging to all the ships of the Jamaica squadron died during that entire year. Two of them were not as a result of sickness: one drowned while the other was killed by a lightning strike. On the Leeward Islands station, of the 16 seamen who died on board during 1775, three of them drowned in separate incidents.
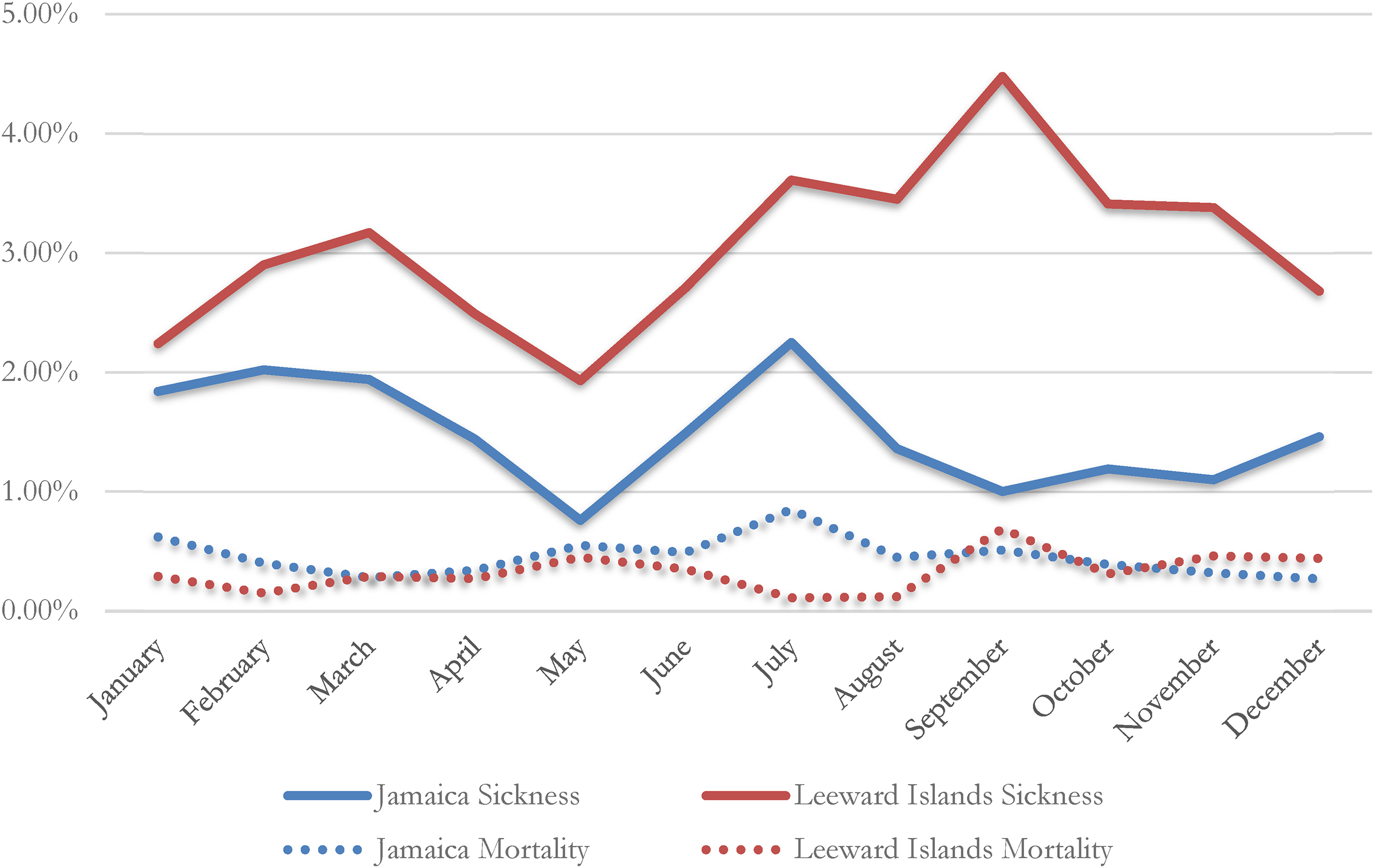
Those 1775 figures can be compared with a year at a time when the number of seamen on both stations was much higher and war was directly affecting islands in the West Indies. Here again sickness levels on both Jamaica and the Leeward Islands stations were relatively low (Figure 3). Instantly discernible is the identical spike in illness during the sickly autumn months on the Leeward Islands station. During that period, sickness levels reached nearly 5%, but this was lower than the figures for 1775. On the Jamaica station, it is clear from the figures that sickness was comparable during both years.
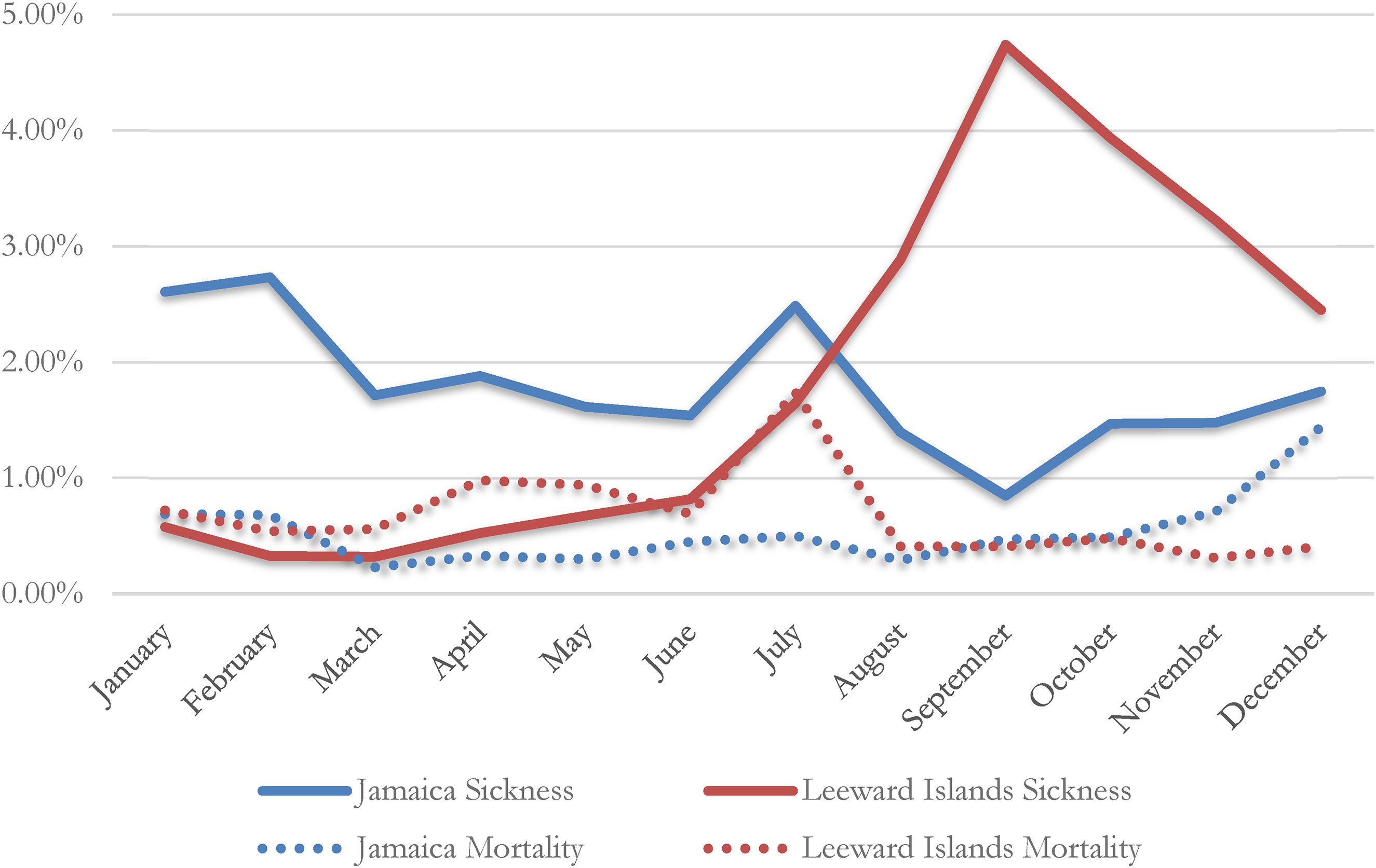
Sickness and mortality levels on two West Indies stations, 1779.
Mortality levels in 1779 were slightly higher, but this is due in part to a handful of battles, most notably the Battle of Grenada that occurred on 6 July 1779 and involved the majority of the Leeward Islands squadron. Some ships suffered more than others during the battle and casualties were numerous. A breakdown of the number of men dying on each ship as a result of this battle is shown in Figure 4; the total dead numbered 106 men, although one of the most assailed ships, the HMS Lyon, has no muster book available and the total losses from that ship cannot be included.
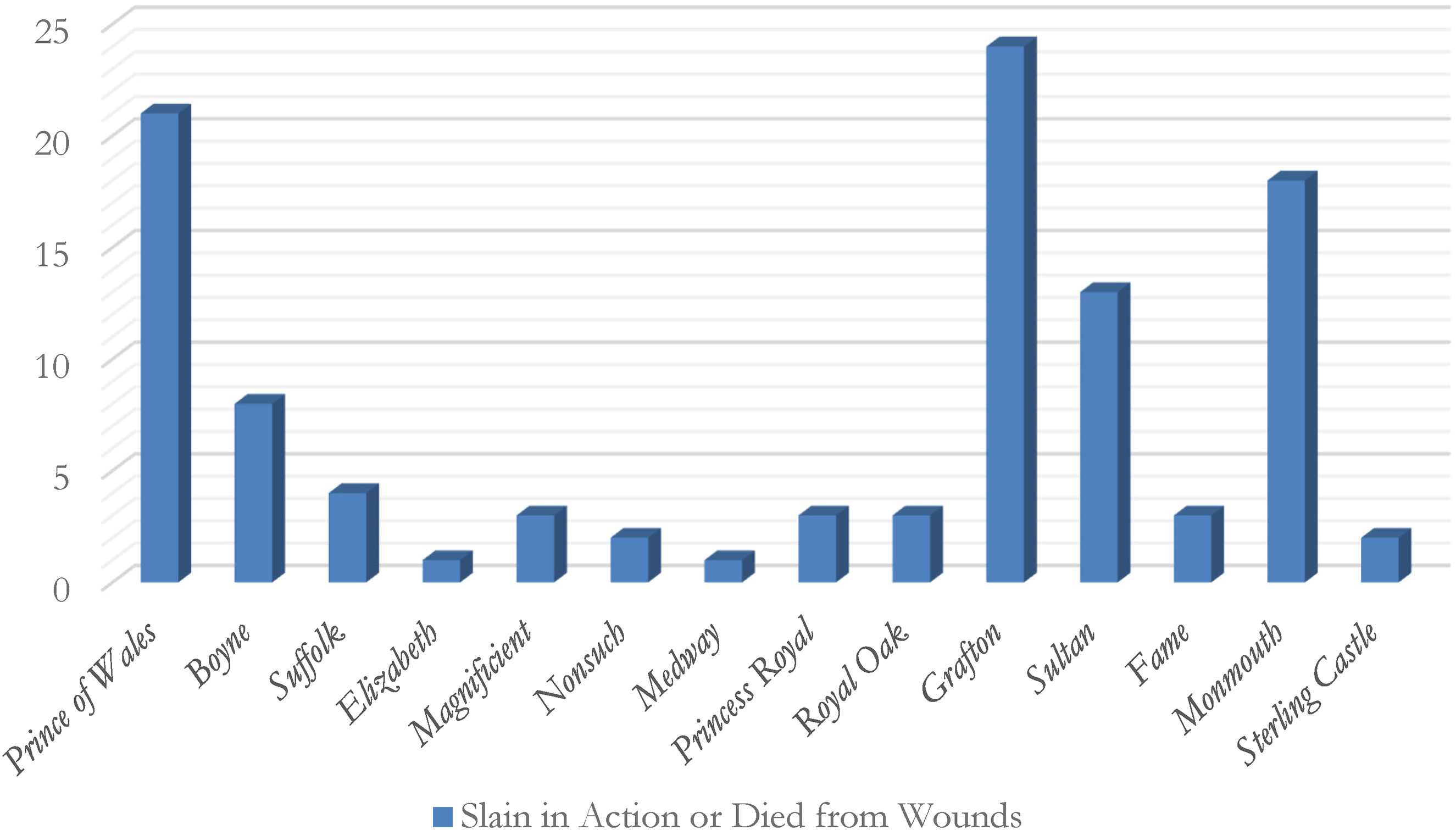
Mortality numbers from the battle of Grenada, 6 July 1779.
Despite the apparent low sickness figures in 1779, there were a handful of ships that suffered far more than others. On the Jamaica station, average illness during the sickly months remained below 3%, but as Figure 5 shows, sickness was not distributed evenly across the station. While HMS Resource had below-average sickness rates in July and August, by the time the rainy season set in, the rate of sickness more than doubled. HMS Hound was above average before the rainy season, and once September arrived, its sickness level also doubled. HMS Port Royal was consistently unhealthy during this six-month period.
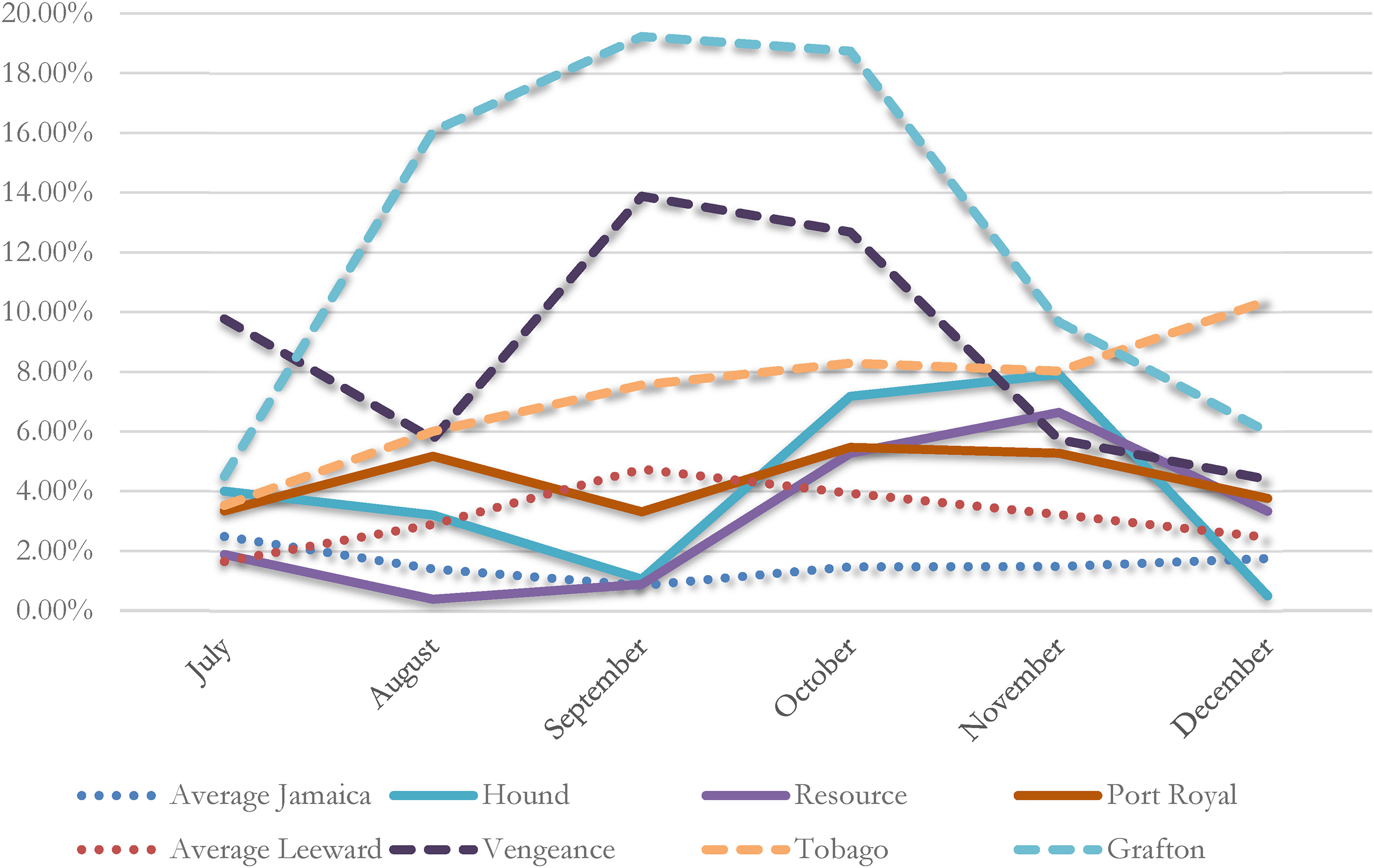
The unhealthiest ships at Jamaica and the Leeward Islands, 1779.
Individual ships on the Leeward Islands station fared much worse. HMS Vengeance arrived on station in mid-June from the Gambia River. While off the west coast of Africa, it had only a few men on the sick list, although it did experience a considerable number of deaths. Death was recorded in the muster books as unspecified ‘fevers’, most likely yellow fever. The fast-acting malaises usually connoted that those falling ill were not on the sick list for long periods, meaning that sickness levels would appear to be minimal. The instant the ship touched land at Barbados in early July, the crew immediately began to suffer extensively. A pattern which is perceptible in the muster books is that the number of men on the sick list increased every time the ship touched land at Barbados, highlighting the island's unhealthy nature.
Perhaps the most conspicuous statistic is the remarkably high level of sickness on board HMS Grafton during the last half of 1779. It was not uncommon for newly arrived ships in the West Indies to suffer to this magnitude when they reached the region, while ships that served longer on station by and large fared better health-wise. This was not the case for HMS Grafton, which despite its seamen having been exposed to the tropical climate for over six months, suffered a debilitating level of sickness. The ship was fortunate enough to lose its men only temporarily from active duty as its mortality level remained minimal.
The last figures to be surveyed are from 1783 (Figure 6). The principal intention in selecting that year is on account of sickness levels significantly declining owing to the efforts of two men: Admiral George Brydges Rodney and his personal physician Gilbert Blane. These individuals will be discussed later in detail. For the moment, the impact these two men had on the health of seamen in the West Indies during the conflict can be quantified. It is evident that sickness levels, even throughout the rainy months, remained under 4.5% – a similar figure to that calculated four years earlier. As with previous examples, the Leeward Islands station was sicklier than the Jamaica station.
Sickness and mortality levels on two West Indies stations, 1783.
Figures from the Jamaica Station remain fairly consistent across all three sample years, staying below 3%. Likewise, it is important to note that as the American War advanced, the levels of sickness did not worsen. This is an extraordinary feat considering that supplies and the quantity and quality of provisions diminished over time, particularly when the West Indies became the central theatre of the conflict.
****
How was the Royal Navy able to maintain such extraordinary degrees of health during a global war in a region with a reputation for sickliness? With France and Spain formally entering the war on the American side in 1778 and 1779 respectively, the Admiralty was forced to distribute its resources beyond North America. The quantity of men required to defend British West Indies colonies more than trebled, signifying that additional supplies were required to maintain both squadrons. The Admiralty faced the daunting task of organising shipments of men and supplies to various points around the globe and had very little time to concentrate on specific issues in particular regions, such as the levels of sickness and mortality. Several of the most favourable improvements were the product of hard work and dedication by individuals – that is to say admirals, captains, physicians and surgeons – stationed in the West Indies who ensured that all possible strategies were employed in order to secure the greatest level of health. These men went beyond the limits of their orders and were the principal catalysts for sweeping changes in health and sanitary practices in that region. Efforts to improve conditions in the West Indies involved persistent letter writing to officials in London to demand supplies be conveyed from Britain, the purchase of fresh provisions from local vendors, together with trialling various medicaments with the aim of ascertaining which were the most effective in combating disease. Some also demanded rigorous cleanliness regimens on board. These advances in hygiene and sanitation significantly reduced reports of shipboard typhus and other contagious diseases. A great number of their findings were later published and circulated widely.
Evidence for the efforts of naval personnel to improve the health of the seamen in the West Indies can be found in their voluminous correspondence with the Admiralty. Men in charge of all naval squadrons routinely contacted the administrative leaders to provide news and intelligence. Oftentimes in these letters, commanders and captains also condemned the logistical support offered to squadrons, both conveyed from Europe and obtained locally. Grievances were numerous during peacetime, but with the threat of war and the increase in personnel, criticisms intensified and were dispatched more frequently. As early as 1775, Admiral James Young requested to supply his Leeward Islands squadron with fresh provisions as soon as he took up the post of commander-in-chief, realising that tensions between Britain and the American colonies were intensifying and that provisions from the latter might well decrease. 13 According to Young, he advertised locally to employ a contractor to supply fresh beef to the men, but every contractor's rate was deemed unacceptable by the Victualling Board on the basis that they were all too expensive. Young defended the contractors, pointing out that the advertisement required the contractor to provide fresh beef at several islands including Antigua, Barbados, Grenada and St Kitts. Also, there was a general scarcity of cattle among the nearby islands. Young alleged that there would be a great savings if the Victualling Board advertised for these principal islands separately, meaning that individual contractors would be engaged to supply ships in a specified port, rather than one contractor supplying ships irrespective of their locations. Young believed that the men were ‘deprived of a benefit’ by not being supplied with fresh beef and owing to the ‘unhealthiness of the climate’ the men in the West Indies were ‘more needful for them … than in most other places’. 14 If fresh beef was authorized by the Victualling Board and made available to ships’ surgeons, it could be utilised in the treatment of seamen on the sick list; the expense incurred by keeping them at a shore based hospital (1s8d per diem) would be a saving to the government.
Young was not satisfied waiting for a decision from the Victualling Board on this issue. Instead, the admiral placed his own advertisement ‘by way of trial’ at Antigua. He received tenders from two merchants, and without waiting for approval from the Admiralty or the Victualling Board, Young contracted with the lower of the two tenderers to supply the ships at Antigua with fresh beef for six months to ascertain what benefits would be had. 15
Following Young's departure from the Leeward Islands, he was replaced briefly by Admiral Byron. Most of his men had been exposed to the hardships of winter in North America prior to sailing to the Leeward Islands and therefore their immune systems were already weakened by the time they arrived at St Lucia. That particular island had emerged as one of the central bases of the Royal Navy following its capture from the French in 1778. As it had only recently been taken, Byron naturally complained about the lack of able men on the island that could be used to replace those in his squadron who were too sickly to perform their duties. There was also no place to deposit the sick men on shore for recovery. 16 In order to combat these issues, he ordered one of the ship's surgeons to erect tents and huts on shore to accommodate sick men temporarily, and in addition to their regular shipboard rations, Byron sanctioned the purchase of fresh vegetables and any other refreshments which could be procured without waiting for authorization from the Victualling Board or the Admiralty. 17
By February 1779, Byron claimed that although the sick were numerous, many of them were not dangerously ill and he had ‘reason to hope that most of them would in a short time gather strength and be fit for their duty if fresh meat and other proper nourishment’ could be secured for them in addition to the fresh vegetables already supplied by the surgeon. It was through the supply of fresh vegetables that Byron reported the levels of sickness had abated. 18
The Admiralty superseded Byron with Admiral George Brydges Rodney in late 1779. Rodney and Gilbert Blane, his personal physician, sailed to the West Indies and their presence on the Leeward Islands station resulted in sweeping changes to the navy's health and hygiene practices. Rodney had previously served in the West Indies on two occasions and was well acquainted with the effects of tropical diseases on a squadron. Rodney, an officer who enjoyed a reputation for being generally unprincipled and selfish, preferred to not forward complaints to the Admiralty and wait for it to address the shortages. Instead, he favoured taking action to avoid sickness among his squadrons. When it came to the health of his men, Rodney displayed a genuine and resolute concern.
Rodney was particularly distressed by the lack of cleanliness and hygiene throughout the navy. He believed that captains would benefit from implementing stricter levels of discipline and keeping their ships as clean as possible. Knowing how important it was to be well equipped with certain necessaries in the West Indies, he also insisted that if he was unable to obtain orders from London to authorise the purchase of fresh provisions, he would procure them on his own and submit the bills to the Admiralty for reimbursement, echoing Admiral Young's actions five years earlier. He habitually procured fresh provisions, medicines and necessaries from local suppliers without Admiralty approval periodically when he considered it crucial. In May 1782, Rodney was compelled to authorise the purchase of fresh beef and other refreshments for the use of the sick since the navy's administration failed to agree to his demands. During his time on the station, Rodney persisted in his writing to the Admiralty requesting medicines and necessaries to be conveyed from Britain rather than having to procure those items locally at a higher price. He claimed that ‘some of the most fatal diseases of that climate [arose] from the want of fruit and fresh diet’ which could be ‘prevented and cured by such an allowance of Peruvian Bark [quinine] as is provided for HM's ships serving on the Coast of Africa’. 19
Gilbert Blane arrived in the West Indies on board HMS Sandwich as Rodney's personal physician. He had received his MD from the University of Glasgow only a year earlier, where he was fortunate enough to study under a distinguished doctor who recommended him to Rodney. Rodney suffered severely from gout and was something of a hypochondriac. 20 Blane proved to be a valuable member of the flagship's company despite having no official naval duties, often going above and beyond his private responsibilities. Rodney immediately recognised Blane's determination and his ability as a man of medicine. Unlike most naval medical men, Blane was not content serving below deck during battle; he made himself available on deck, carrying with him a supply of tourniquets in order to quickly suppress bleeding. He attended to wounded men in the place they fell to reduce the amount of stress ordinarily experienced by carrying them down to the orlop deck. To reward him for these qualities and proactive measures, Rodney appointed Blane Physician of the Fleet in April 1780. 21
Serving in this official capacity, Blane, with Rodney's full support, was able to advance the health of the fleet in a short period of time by introducing several medical and hygiene reforms. According to one historian, the partnership between the admiral and the doctor was so successful that ‘never before had any British fleet a better health record – thanks to Rodney and Doctor Blane’. 22 The close relationship with Rodney afforded the physician an abundance of leverage when it came to compelling captains and surgeons of the fleet to follow his orders.
Blane took an unorthodox approach when he wrote directly to the Sick and Hurt Board because he believed that the situation of the Leeward Islands' squadron warranted addressing. In his letter of July 1780, he explained to the Board that he was amassing monthly sickness returns from each ship of the squadron and intended to use those returns to ‘form some judgement of the comparative state of sickness at different times, and of the success of the means to be employed in preserving health’. 23 He believed that figures such as those should be compiled by the Sick and Hurt Board on a regular basis (this was not the practice at the time) and examined regularly to better calculate the distribution of medicines and necessaries in advance. Blane described the plight of naval surgeons and their inability to afford the inflated costs of medicines when the Board failed to transmit regular supplies. 24 The most advantageous medication, Peruvian Bark, never retailed for less than 30 shillings per pound in the West Indies, a great sum of money to surgeons whose wages were 6 shillings and 8 pence per man per cure. 25 Even those surgeons who arranged for repeated supplies of medicines from home by a private commission as opposed to procuring them locally were gambling on account of the distance, risks and credit necessary to do so.
Six months after Blane arrived in the West Indies he printed, at his own expense, A Short Account of the Most Effectual Means of Preserving the Health of Seamen. He drew largely on his experiences in that region and specifically addressed issues of hygiene and victualling. In it, he stressed that the prevention of disease was just as important as curing it. As rational as that concept seems, most surgeons were unable to think in terms of prevention since the majority failed to comprehend efficacious cures. Blane, echoing Rodney's opinion, endeavoured to make captains and officers more accountable for the health of their men by suggesting that if discipline on each ship was enforced to a greater degree, it would ‘extirpate diseases from the navy’. 26 Blane's book was well-received and distributed to all captains and surgeons in the Leeward Islands squadron.
To further convince the Admiralty that changes were required across the Royal Navy, Blane presented mortality figures from the squadron from July 1780 to July 1781. According to his data, a total of 715 seamen died on board ship, of whom only 59 died during battle or from wounds sustained in battle while a further 862 died in naval hospitals on shore during the same period. Of the 12,109 men needed to man 20 ships of the line, 1577 of them perished largely owing to disease. A further 350 were sent back to England as invalids during this period and most of them were never again fit for service. 27 Through Rodney and Blane's hard work and dedication to cleanliness and the procurement of fresh supplies and medicines, the health of the fleet improved in a short time. In 1782, when the fleet consisted of 40 ships-of-the-line with crews numbering nearly 24,000, Blane reported that there were only 350 deaths from disease in six months and no more than 1000 men were sent to hospital. 28 Blane's measures for reducing sickness and mortality had been so successful that of the 36 ships-of-the-line present at that Battle of the Saintes on the 12 April 1782, ‘every ship, except two, might be said to be healthy’. 29 Rodger considered the men in Rodney's fleet to ‘have been the healthiest body of British subjects in the world’. 30
During their time together in the West Indies, Rodney's faith in Blane's abilities, his willingness to take aggressive action and Blane's medical prowess made this pair the most successful in the West Indies during the eighteenth century. The changes implemented in the early part of their service together laid the groundwork for the squadron's subsequent naval victories. Rodney's insistence on strict discipline amongst both the officers and men gave rise to considerable advantages over the French fleet. At the Saintes, Blane reported the total number of men killed at 234 and the number of wounded at 789. 31 Although their dead and wounded numbers were never published, Blane estimated that the Ville de Paris, de Grasse's flagship, lost 300 men. Considering that there were 5400 French troops on board in addition to the seamen of the fleet distributed among the vessels, the French casualties would have been proportionally more numerous. 32
Rodney and Blane returned home separately in 1783. 33 In 1785, Blane completed his influential work on naval hygiene entitled Observations on the Diseases of Seamen. 34 The work largely summarised his experiences in the West Indies with Rodney and provided unique insights into the incidences of tropical disease. Figures submitted to Blane by surgeons from ships during his term as Physician of the Fleet were compiled and analysed in a precise way in order to ‘acquaint the commander in chief, from time to time, of the state of sickness, or the predominance of particular diseases, in order to recommend such articles of diet, or other means, as might tend to cure them, or to check their progress’. 35 These figures were included in Blane's book, giving the Sick and Hurt Board its first comprehensive study of disease in that region. Using these figures, the navy was better able to calculate the quantity of medicines and necessaries required in the West Indies throughout the year, particularly during the sickly season.
****
Quantitative investigations into the health of seamen on board ships demonstrate that for the latter part of the eighteenth century, particularly during the American War of Independence, sickness in the West Indies has been largely overestimated. By investigating individual ships’ muster books, data can be extracted allowing for a comprehensive survey. Not only do the figures provide the number of men on the sick list four times per calendar month, but they can also be used to track patterns of mortality. Analysis of that data provides an overall representation of sickness and mortality prior to war breaking out in 1775, during the intense levels of fighting in the West Indies after the French entered the war, and as the war ebbed in 1783. By and large, the average percentage of sick seamen was relatively low and manageable so long as supplies of medicines and fresh food were procured by vigilant naval officers. Sickness levels during these sample years remain below 8% with the highest figures existing during peacetime. These figures also demonstrate that, although the quantities were low, there existed a small number of ships that were more susceptible to contracting diseases than others. Ships had the potential to suffer quite severely and, in some cases, individual ships’ sickness levels neared 20%. Yet these ships are not representative of the overall state of health. Realistically, most men ordered to serve in the West Indies were not likely to succumb to disease or injury and, more importantly to the navy, they remained healthy enough to serve the fleet.
Naval medical practices improved during this period, with the main impetus coming not from London but from the dedication and determination of the Royal Navy officers and surgeons who had first-hand experience serving in the West Indies. Their personal observations compelled them to change the health practices in that region, and when it proved manageable, medical care went from being curative to chiefly preventative. Several individuals serving in the region during the conflict are especially noteworthy for the work they carried out. Both Admiral Young and Admiral Byron were committed to keeping seamen healthy and on active service. They took proactive measures to procure fresh vegetables and fresh meat for distribution to men on the sick list and in hospital. With the arrival of Admiral Rodney and his personal physician Gilbert Blane to the West Indies, sweeping changes to the health management system occurred. Through stern discipline imposed on captains in Rodney's squadron and the demands made upon their surgeons by Blane, the pair reduced sickness and mortality levels considerably. Through the vigilance and dedication of these individuals, favourable changes in health and hygiene practices were gradually rolled out across all naval ships in the West Indies, thereby reducing the overall percentage of death and debility from disease and increasing the overall effectiveness of the fleet towards the close of the American War of Independence.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.