
Abstract
Leadership is a core expectation of nursing practice, yet leadership development curricula in academia and healthcare organizations fall short of equipping nurses to lead in today’s complex healthcare environment. This article outlines a framework-driven approach to leadership education through two courses designed for undergraduate and graduate nursing students, developed and iteratively refined using the Knowledge-to-Action framework and annual Plan-Do-Study-Act cycles. Grounded in relational leadership theories, the RNAO model for developing and sustaining leadership, and the LEADS in a Caring Environment framework, courses integrate participatory learning strategies to bridge theory and practice. Students engage in team-based projects, reflective exercises, and experiential activities to build self-awareness and confidence. By aligning curricula with professional standards and practice-relevant frameworks, these courses cultivate leadership, positioning nurses to influence the quality of care and contribute to health system transformation. Organizations can build on this foundation to provide leadership development and support professional growth.
Introduction
Leadership is a cornerstone of professional nursing practice and a critical competency for navigating the complexities of modern healthcare systems. Nurses are expected to lead at all levels—whether at the point of care, within interprofessional teams, or in formal organizational roles—while simultaneously delivering the highest quality of care. 1 National and provincial/territorial regulatory bodies convey this expectation through standards of practice and entry-level competencies. 2 Despite these expectations, leadership development opportunities for nurses remain limited, leaving many to assume leadership responsibilities without formal preparation or based on seniority, or simply because they are the only available candidate. This gap is particularly concerning given the growing complexity of healthcare, staffing shortages, and overcrowded hospitals, which amplify the need for nurses to lead effectively in everyday practice. Academic nursing programs are uniquely positioned to address this need by integrating theory and practice into leadership education, equipping graduates with the knowledge, skills, and attitudes required to lead change and foster healthy work environments.
Leadership Development Within Nursing Education
The author conducted a cursory environmental scan to examine how Canadian nursing programs incorporated leadership education. Most baccalaureate programs included leadership content, typically offered as a standalone required course—such as Leadership in Nursing, Leadership and Management in Nursing Practice, or Professional Practice and Leadership—in the fourth year. In some programs, leadership was integrated throughout the curriculum as modules within clinical practice and professional issues courses. Leadership education was also a consistent component of general master’s programs in nursing; however, its delivery varied across institutions. Approaches ranged from dedicated leadership courses to integrated content within broader streams such as administration, health policy, or advanced practice. While most master’s programs offered at least one leadership-focused course, these courses were often elective, highlighting variability in how leadership preparation was prioritized across curricula. Overall, Canadian nursing programs demonstrate a strong commitment to leadership development, yet the leadership frameworks or the specific leadership theories and concepts in these courses are largely unknown or not agreed upon.
Synthesized research on undergraduate leadership education consistently showed that while leadership development was included in nursing curricula, its scope and depth varied widely.3-8 Studies emphasized that leadership courses should be grounded in strong theoretical foundations while remaining practice-relevant and applicable to real-world clinical settings. 6 Commonly prioritized content included interpersonal communication, delegation, conflict management, and collaborative teamwork.3-5,9,10 Although undergraduate leadership education aimed to build leadership skills, most programs prioritized technical competencies over self-awareness and relational capabilities, revealing gaps that underscore the need for evidence-based, practice-driven frameworks to prepare nurses for complex leadership responsibilities.4-6,8
Graduate nursing education shows promise yet remains underexamined. Master’s programs nurtured higher-order thinking, evidence appraisal/application, systems thinking, and transformative capabilities—communication, collaboration, problem-solving—and these were linked to improved patient outcomes/safety, staff retention, and satisfaction. 11 Still, clinical leadership was variably defined, and competencies were not uniformly specified. 11 D’Anna surfaced five competency domains with behaviours spanning communication/relationship-building, healthcare environment knowledge, leadership, and professionalism. 12 Collectively, these findings suggest that graduate curricula should orient to meso- and macro-level leadership (unit/department/organization), elevate critical thought, and prepare for formal leadership roles.
The literature consistently underscores the importance of intentional nursing leadership development within academic programs, emphasizing the need for experiential, theory-informed pedagogy. Despite this recognition, significant gaps remain. Research revealed considerable variability in curricular standards, limited specification of leadership competencies—particularly within graduate level—and an underemphasis on personal qualities, attitudes, and evidence-based leadership practices that support effective leadership. Addressing these gaps requires a paradigm shift from simply adding leadership courses—often shaped by textbooks or individual faculty preferences—to adopting evidence-based, practice-driven frameworks that make leadership teachable, measurable, and transferable across clinical contexts.
In response to this need, the purpose of this article is to describe the design and implementation of two theoretically informed, evidence-based nursing leadership courses (undergraduate and graduate) developed at a Canadian university. These courses operationalized widely adopted frameworks to prepare nurses to lead effectively in diverse and evolving healthcare contexts. For the purposes of these courses, leadership is defined as “the process by which a self-aware, credible, and courageous person engages and influences others toward a collective vision and direction for the purpose of achieving measurable goals.”13(p.18) Although this definition applies to all nurses regardless of role or position, novice nurses may find such a wide conceptualization difficult to relate to. To address relevance for early-career learners, the concept of clinical leadership is also used, emphasizing leadership enacted at the point of care. Clinical leadership refers to the ability of staff nurses to guide and support the healthcare team in delivering safe, high-quality, patient-centred care. Leadership is a professional competency that enables nurses to influence patients, colleagues/members of the team members, and the broader organization to improve practice and outcomes through effective communication, collaboration, and decision-making.14,15 Moreover, leadership is understood as a flexible, interactive process shaped by the dynamic interplay between the leader, followers, and the context in which they work. 16 Together, these definitions anchor the courses described in this paper and provide a conceptual, theoretical, and practical foundation from which organizations can continue to cultivate mentorship, foster leadership capacity, and support continuous professional growth across the nursing workforce.
Program, Course Description, and Methods
Overview of Courses
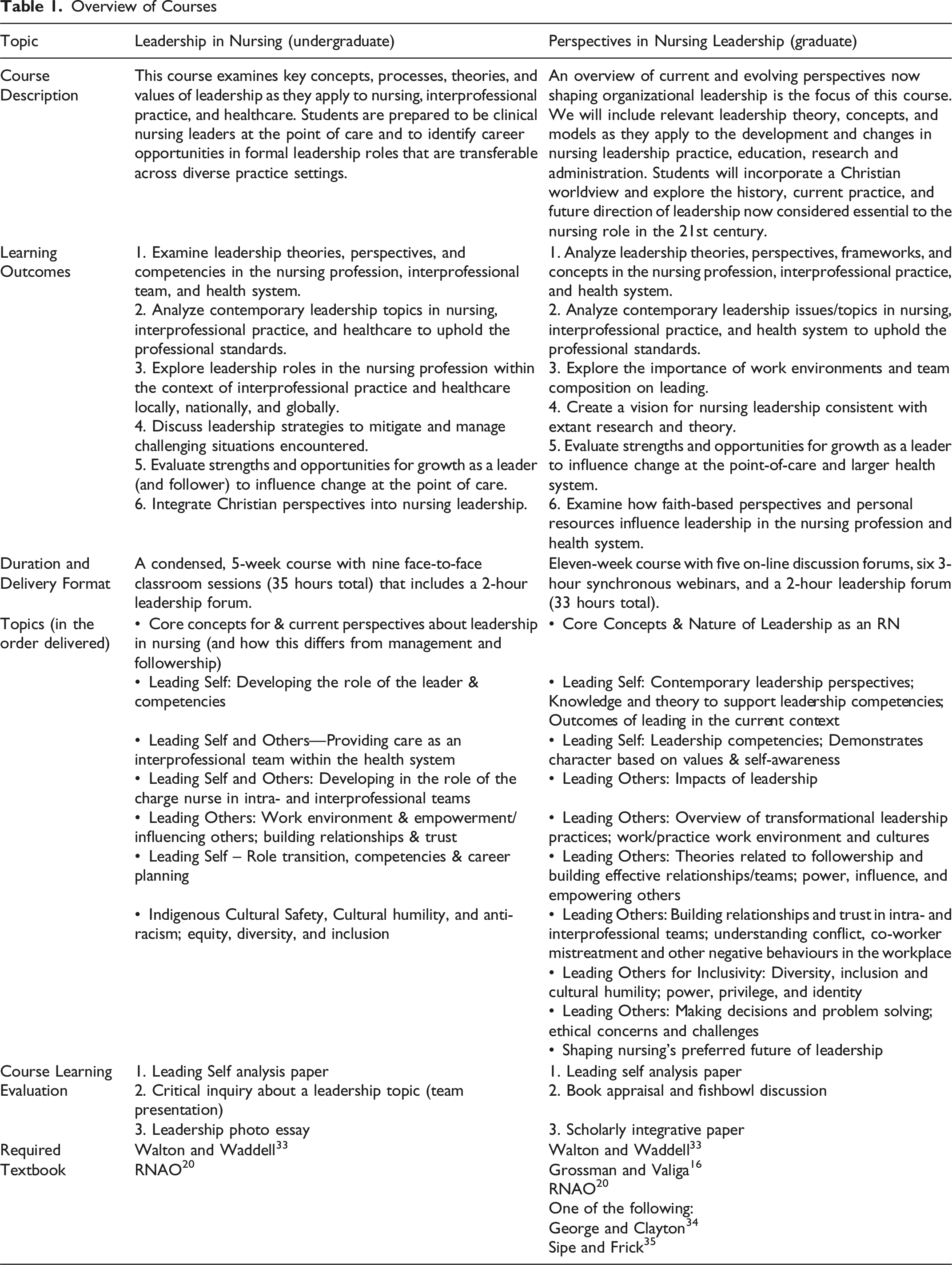
By achieving the learning outcomes identified in Table 1, these courses aim to strengthen leadership readiness and support nurses in navigating the complexities of modern healthcare. The outcomes emphasize developing knowledge of relational leadership theories, analyzing contemporary leadership challenges, exploring clinical leadership roles, and understanding the importance of psychologically safe work environments and team-based care. Students learn strategies to manage and mitigate negative workplace behaviours (including conflict, incivility, and bullying); apply strength-based approaches to leadership development; and integrate a faith-informed perspective into leadership practice. The undergraduate course prepares students to enact clinical leadership at the point of care upon graduation, while the graduate course equips RNs for both informal and formal leadership roles across diverse settings. Together, using a framework-driven approach, these courses provide a strong theoretical and practical foundation for leadership development, ensuring that nurses are prepared to lead effectively within complex, dynamic healthcare environments.
To ensure that the curriculum was evidence-informed, relevant, and responsive to changing practice realities, beginning in 2020, the courses were re-designed and taught by a Certified Health Executive and experienced nurse educator. The Knowledge-to-Action Framework 17 was adopted as an overarching structure to guide iterative course development. This framework supports a systematic, cyclical process for translating knowledge into educational practice and closing the gap between what evidence indicates should occur in leadership education and what is currently practiced within nursing education. Complementing this framework, annual Plan-Do-Study-Act cycles 18 were used to operationalize quality-improvement. Following the initial creation of the course syllabi and lesson plans, revisions were conducted each academic year based on student feedback, instructional experience, evolving healthcare challenges, and emerging evidence. This approach ensured that course content remained current, pedagogically sound, and aligned with leadership capabilities required in contemporary nursing practice.
Framework-Driven Approach
Theoretical Framework for Courses
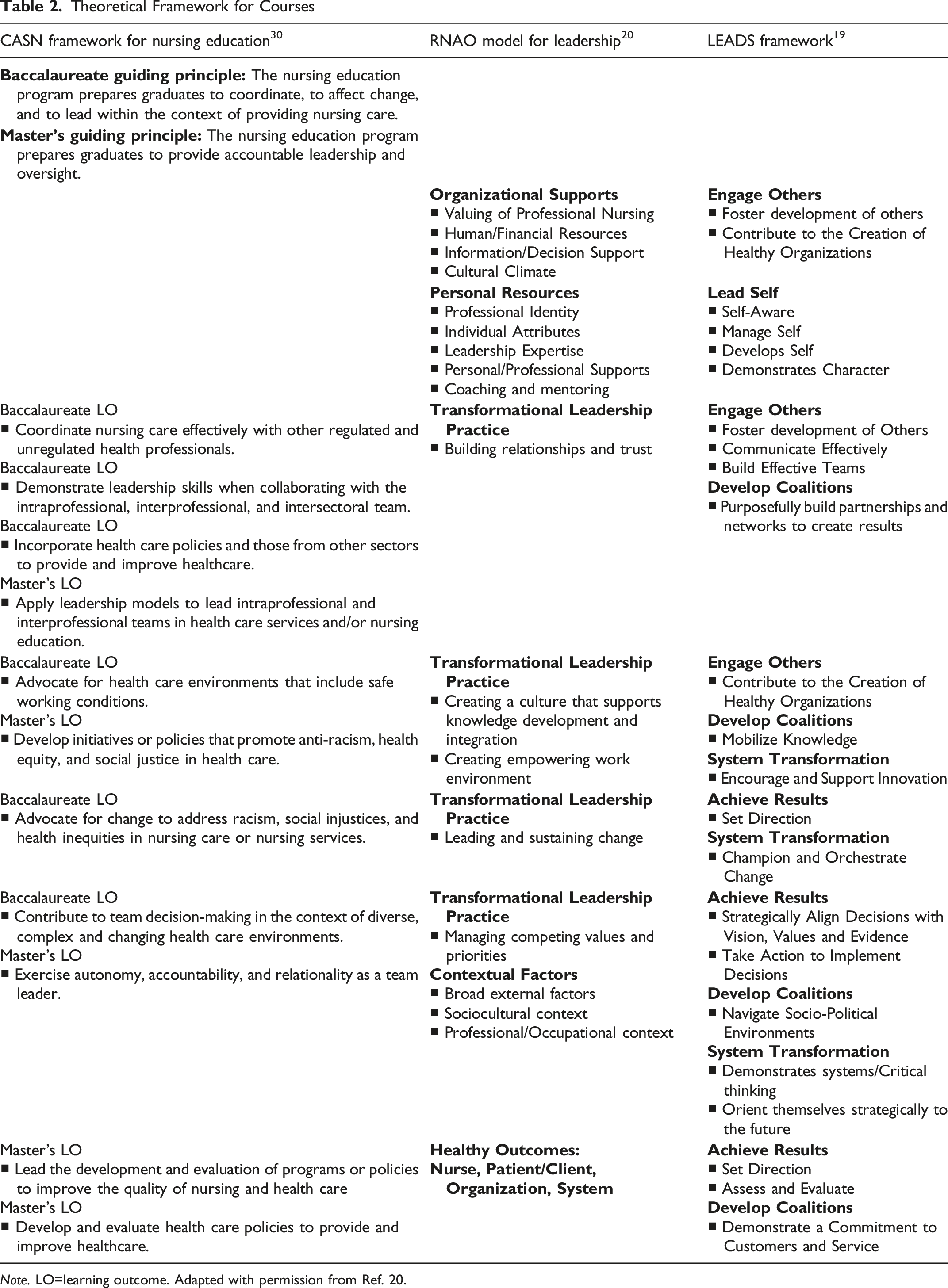
Note. LO=learning outcome. Adapted with permission from Ref. 20.
Leadership Framework
The Canadian College of Health Leaders LEADS in a Caring Environment framework offers a comprehensive model for conceptualizing leadership and driving change within complex health systems. It consists of five domains—
The five domains of the LEADS framework are both distinct and interdependent, reflecting the need for continuous change in a complex adaptive system such as healthcare (see third column in Table 2). 19 Together, they provide a comprehensive approach to leadership development. Lead Self emphasizes personal leadership capabilities such as emotional intelligence, self-awareness, and resilience. It focuses on mindset, habits, and mental models, grounded in the belief that effective leadership begins with self-management and can be developed/learned through intentional effort. Engage Others addresses leadership as a relational process, highlighting communication, teamwork, and performance management. Leadership exists only when there are followers, and this domain draws on theories of communication, engagement, leadership styles, teamwork, emotional intelligence, and strength-based development. 19 Develop Coalitions extends relational leadership to a strategic level, requiring leaders to build partnerships and networks across organizations and sectors. It involves mobilizing knowledge, navigating socio-political environments, and achieving shared goals through collaboration. Systems Transformation focuses on strategic capabilities for navigating complexity and driving change. Leaders apply systems thinking and change management principles to influence policy, structure, and culture, shaping the health system of the future. Achieve Results, the outcome domain, centres on creating a compelling vision, setting measurable goals, making evidence-informed decisions, and taking accountability for outcomes. 19 Success in this domain depends on integrating the other four domains. LEADS equips leaders with interconnected capabilities to foster healthy work environments, teamwork, and communication, ultimately driving system-wide transformation and improved health outcomes. To that end, the LEADS framework provides a roadmap for leadership education in academic and health organization settings by equipping nurses with the capabilities needed to drive meaningful health system change; by embedding caring as a core value and aligning practices with evidence-based principles, it serves as a powerful foundation for preparing future leaders.
Relational Leadership Theory and Evidence-Based Leadership Practices
Nurses are leaders in every setting, and improving care quality depends on empowering those who deliver it. 20 Leadership education must go beyond skill acquisition to instead provide foundational theoretical knowledge about relational leadership styles that shape the attitudes, beliefs, and values of effective leadership. Evidence underscores that relational leadership styles—rather than purely task-focused approaches—are necessary.21-23 In contrast to transactional leadership, which is task-oriented and primarily leader-centric, relational approaches prioritize engaging team members and fostering meaningful connections.23,24 The quality of relationships among leaders, followers, teams, and organizations is pivotal; work is accomplished through these relationships and the environments in which they occur. 16 Accordingly, leadership curricula—particularly at the MSN-level, should emphasize relational theories and incorporate evidence-based leadership practices which are essential for leading in today’s complex healthcare system.
Three relational theories provide complementary guidance for nursing leadership: transformational, authentic, and servant leadership.16,25 Each theory offers a distinct perspective on how leaders engage and influence others, which can be translated into relevant, actionable strategies for effective leadership. Transformational leadership encourages, inspires, and motivates followers through four behaviours—idealized influence, inspirational motivation, individualized consideration, and intellectual stimulation—so leaders model integrity, communicate a compelling vision, attend to individual needs, and spark innovation.16,21 Authentic leadership builds legitimacy through self-awareness, relational transparency, balanced processing, and an internalized moral perspective; leaders align values and actions, invite diverse views, and make integrity-based decisions. By committing to personal growth and embodying core values, authentic leaders foster trust and respect, enabling them to guide teams through change and navigate complex healthcare environments.16,26 Servant leadership positions service to others as the leader’s primary responsibility, emphasizing an other-oriented mindset that prioritizes followers’ needs over self-interest. Leaders share power, act as stewards, and develop people. By maintaining integrity and demonstrating humility, servant leadership creates a culture of caring and enhances followers’ well-being, ultimately improving care outcomes.16,24,27
The Registered Nurses’ Association of Ontario (RNAO) Conceptual Model for Developing and Sustaining Leadership integrates the best available evidence to define leadership practices essential for creating healthy work environments and achieving quality patient outcomes (see second column in Table 2). 20 Grounded in transformational leadership research, the model identifies core competencies supported by actionable strategies, sample behaviours, and practical statements that demonstrate relevance to point-of-care leadership. It emphasizes both organizational supports and personal resources that enable effective leadership, ensuring practices are not only evidence-informed but also practice-relevant. 20 By linking leadership behaviours to concrete outcomes, the model provides a clear rationale for implementation and offers nurses a roadmap for influencing care environments through collaboration, trust-building, and psychological safety. Ultimately, embedding content from this framework into these courses equips nurses with the tools to lead confidently and effectively.
These contemporary, relationship-based leadership theories provide valuable insights into what makes an effective leader and offer a lens for viewing transformational leadership practice. Relational leadership styles share an other-oriented focus, reinforcing values such as integrity, respect, and caring. 16 By promoting transparency and collaboration, these styles strengthen relationships and build empowering work environments where shared goals and continuous improvement flourish.21-23,25,27 Their ripple effects extend beyond leaders and followers to patients, teams, and organizations. Moreover, relational theories align closely with the LEADS capabilities for Lead Self and Engage Others and underpin the RNAO leadership model, specifically the transformation practices for building relationships/trust and creating an empowering work environment (Table 2). Therefore, embedding relational leadership across undergraduate and graduate curricula is essential to prepare nurses for point-of-care and formal leadership roles, and to enable evidence-informed practice that improves outcomes for patients, staff, organizations, and health systems.
Leadership Professional Requirements for Nurses and Nursing Education
Leadership requirements for nurses and nursing education are grounded in national and provincial/territorial standards, which informed the development of these courses. The Canadian Nurses Association Code of Ethics provides the foundation for ethical nursing practice across Canada, reinforcing values such as caring, respect and civility, integrity, diversity and inclusion, and evidence-informed practice—core tenets essential for leadership. 28 Alongside provincial/territorial professional standards of practice (e.g., Ref. 29) and entry-level competencies, 2 these resources define minimum expectations for professional practice and serve as a framework for leadership curriculum design. Furthermore, to ensure academic institutions address leadership preparation, the Canadian Association of Schools of Nursing (CASN) National Nursing Education Framework offers six domains, including leadership, which reflect current and future expectations for nursing practice. 30 The guiding principles and learning outcomes of the leadership domain shaped course objectives and content, emphasizing graduates’ ability to coordinate care, collaborate with team members, and drive change (see first column in Table 2). 30 While this domain applies universally, its depth and complexity increase by level of preparation: BSN graduates typically lead at micro and with more experience at meso levels (e.g., unit charge nurse for a given shift), whereas MSN graduates assume leadership roles at meso or macro levels (e.g., care coordinator, educator, and manager). Together, these professional requirements underpin the courses developed, ensuring graduates are equipped with the competencies to lead effectively in providing nursing care, coordinating teams, and managing care across diverse healthcare settings.
Pedagogical Approach and Learning Strategies
While a detailed account is beyond the scope of this article, in both leadership courses, I employed evidence-based pedagogical strategies for teaching and assessment.3-8,31 Students were randomly assigned to small teams for the duration of the course, and a flipped-based classroom approach required completion of readings prior to class. Lecture time, kept to a minimum, reinforced salient concepts and provided context for multi-method, participatory/active learning strategies, many of which were team-based, designed to foster practical application. These included self-assessments, leadership challenges, critical-thinking scenarios, liberating structures, student-led presentations, video-based sessions, structure reflection, role-modelling, a leadership forum, and career-day activities. Formative assessment further integrated theory and practice. For example, one assignment used self-assessment tools to identify leadership strengths and apply them to relational leadership theory. Another required collaborative teamwork: undergraduate students applied leadership concepts to address real-world healthcare system issues, while master’s students critically analyzed a book on relational leadership and engaged in a fishbowl discussion on its applicability to nursing practice. Collectively, this dynamic, integrative approach promoted self-awareness, professional growth, and collaborative learning, enabling students to test leadership practices and apply theories in real-world contexts.3-8,31 By cultivating peer learning and confidence, these strategies aimed to develop self-efficacy and prepare nurses to lead effectively in complex healthcare environments.
Summative Evaluation of Student Outcomes
Both courses underwent annual summative evaluations using the university’s Student Evaluation of Teaching and Learning. All students were invited to complete the standardized 22-item anonymous on-line survey at course end. The evaluation assessed course design, teaching, assignments, and the learning environment on a 7-point Likert scale. Four open-ended questions asked students to identify key takeaways, factors that supported their learning, and suggestions for improvement. Although detailed analyses of these data are beyond the scope of this paper, across all evaluations, students consistently described gaining a deeper understanding that leadership is a relational, developmental process rather than a fixed role, emphasizing that any nurse can lead when grounded in self-awareness, emotional intelligence, and authentic engagement with others. Many students reported newfound confidence in their capacity to enact leadership in both formal and informal contexts, highlighting how the courses helped them recognize the complementary nature of leadership and followership and the importance of cultivating both to support effective teamwork and patient care. Exposure to diverse leadership theories, personality or strengths assessments, and real-world examples from nursing leaders further shaped students’ appreciation for how leadership influences workplace culture, career satisfaction, and the broader healthcare system.
Limitations
While the framework incorporates both Canadian and international research, it is not exhaustive. Integrating additional evidence on the relevance of key conceptual areas, together with input from health-region stakeholders, could further refine and strengthen the weekly course topics. Although this framework currently supports undergraduate and graduate leadership education for RNs, it could also be adapted for leadership development among licensed/registered practical nurses, registered psychiatric nurses, and allied health professionals. Given the growing evidence for simulation-based leadership education, an important next step is to embed simulation activities that enable learners to apply leadership principles in realistic practice contexts and deepen experiential learning.5,6,31 An ongoing longitudinal evaluation of graduates using a clinical leadership questionnaire is also needed to better understand the courses’ potential long-term influence on leadership development throughout a nurse’s career trajectory.
Conclusion
Areas for Leadership Curricula
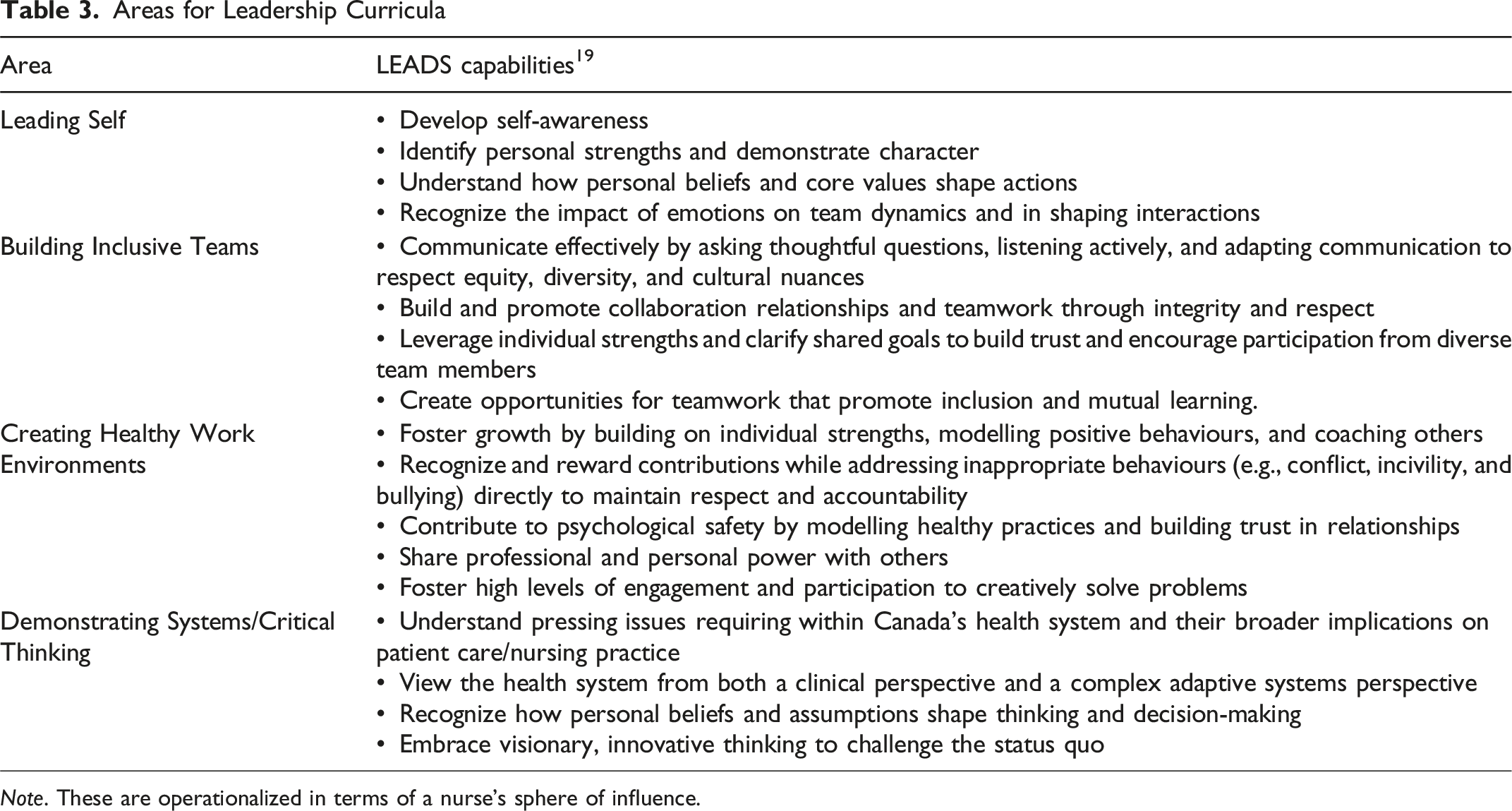
Note. These are operationalized in terms of a nurse’s sphere of influence.
This article describes how integrating a multi-framework approach into academic leadership courses provides a comprehensive roadmap for bridging the gap between classroom learning and real-world leadership practice. Through active teaching and learning strategies, these courses equip nurses with foundational knowledge, skills, and attributes to lead effectively at the point of care and beyond. Ultimately, such courses strengthen competence and confidence, shaping leadership identity early and enabling nurse leaders to flourish. Amid the complexity of modern healthcare, cultivating nurse leadership through academic courses and ongoing organizational professional development is a critical investment in the future of patient care and health system transformation.
Footnotes
Author’s Note
I am the lead professor teaching the courses and employed by Trinity Western University. The views expressed do not represent those of the university.
Acknowledgements
I extend sincere gratitude to the students with whom I have been fortunate to come alongside during their leadership journey. I appreciate the valuable lessons and insights I gained from the learners.
Ethical Approval
Institutional review board approval was not required.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.