
Abstract
There are rich data available from assessments like the interRAI Mental Health that may not be shared with patients in usable ways. We outline a co-design process as an example for health system providers interested in developing platforms for sharing interRAI information with care recipients. Persons with lived experience (current and past service users) identified design specifications for summaries of interRAI data over a series of co-design workshops, including visual and text representations of clinical information as well as processes for sharing summaries with patients. Graphic and text considerations were identified in workshops, including icons associated with key clinical issues and nuanced text summaries of assessment outputs and implications. Participants noted that persons in inpatient care should review this information once stable, and with assistance of a peer support specialist. This work affirms that it is not only desirable, but entirely achievable from an organizational perspective to prioritize and integrate patient voices in the design and use of clinical information.
Introduction
A comprehensive, complete, and accessible clinical record is a vital component of quality healthcare. In psychiatry, the clinical record often includes complex information from assessments completed by the clinical team, which may be difficult to understand for those without specific health training. The level of health literacy required for patients and their supports (e.g., family) to interpret much of the terminology and jargon may result in a complete lack of access to their own chart information without interpretation from a formal support team. 1 Patient portal systems can play an important role in facilitating access to chart information when presented in meaningful ways. 2 The need for information systems that promote meaningful community between formal providers, patients, and their supports is key to provision of person-centred care. 3
Assessments, including comprehensive and subject specific, are prolific in mental health systems. In Ontario, Canada, the Ministry of Health and Long-Term Care, in collaboration with the Ontario Hospital Association, mandated the use of the Resident Assessment Instrument-Mental Health (RAI-MH) 4 at admission, quarter, and discharge from designated inpatient psychiatry beds across the system. The RAI-MH that is mandated in Ontario, Canada, like the newer interRAI-MH,5,6 is a comprehensive assessment of clinical, functional, and social domains organized into outputs that can inform care planning, monitor outcomes, funding, and quality improvement. The assessment is completed by clinical staff whereby items are to be informed by all sources of information, including interview with the person, informal supports, other professional, and review of available records. The outputs from the assessment include summary scales of clinical symptoms, risk, and functioning, as well as care planning protocols. 6 Despite the widespread use and the depth of information these assessments generate, people receiving psychiatric care rarely have access to or meaningful engagement with their own RAI-MH data. 1 Even for those who access their chart, the RAI-MH may be difficult to interpret if summary information and score interpretations are not provided. This disconnect limits opportunities for shared decision-making, patient empowerment, and person-centred care.
Involving people with lived experience in the design and implementation of mental health interventions is critically important, particularly when developing digital tools and decision aids. Co-design methodologies, which actively engage end users as equal partners throughout the research and development process, are increasingly recognized as best practice in mental health innovation.7-10 These approaches move beyond traditional consultation by emphasizing power-sharing, valuing experiential knowledge alongside clinical and technical expertise, and fostering genuine collaboration between researchers, clinicians, patients, and supports.8,11,12 Evidence shows that co-designed interventions are more likely to be relevant, acceptable, and effective, as they are grounded in the lived realities of those they are intended to serve.7,10,13 Furthermore, co-design processes can enhance participants’ sense of empowerment, improve mental health literacy, and build trust between service users and providers.10,13-15 However, the literature also underscores several challenges in operationalizing co-design in mental health contexts, such as inconsistent terminology and frameworks, variable levels of inclusion, and persistent power imbalances.7,9,10 Effective co-design requires intentional strategies to flatten hierarchies, foster inclusivity, and ensure that diverse perspectives—across age, gender, race, and other identity factors—are meaningfully represented and integrated into all stages of intervention development.8,10,16
The “Ensuring Uptake of RAI Evidence and Knowledge by All” (EUREKA) project was established to address these gaps by co-designing accessible, personalized summaries of RAI-MH data with people who have experienced psychiatric hospitalization. The overarching aim is to develop personalized summaries of RAI-MH data that could support shared decision-making and empower service users by making complex clinical data understandable, actionable, and relevant to their care journeys. By centring the perspectives of people with lived experience the EUREKA project sought to advance how mental health assessment information and data could be optimized to enhance patient’s meaningful involvement in decision-making. In our prior work, we held focus groups in 3 specialized psychiatric hospitals across Ontario with a total of 35 current and past service recipients. 1 Participants identified the types of information they felt would empower them to more meaningfully participate in decisions about their care, namely: diagnoses, symptoms, strengths, medications, and clinician rationale. Participants also wanted to receive information in a narrative summary format that incorporated visuals (e.g., pictures and graphs) as well as numbers. 1
This article describes how we built on prior research about sharing RAI-MH data in practice, describing our process for understanding how to best present wanted information to persons receiving inpatient psychiatric services. We outline the co-design processes used to engage participants as an example for health system providers interested in developing platforms for sharing interRAI information with care recipients.
Methodology
Utilizing co-design approaches, we worked with partners who had lived experiences with psychiatric hospitalization to identify design specifications for summaries over a series of meetings; the study received approval through the University of Waterloo Office of Research Ethics (#40622). Using physical posters, we recruited 12 people with lived experience aged 18+ years from the Canadian Mental Health Association’s Centre for Excellence in Peer Support, a collaborating organization. The inclusion criteria included having lived experience with at least one prior mental health related hospital admission. Written informed consent was obtained prior to the first meeting. No names were collected or recorded during meetings and a pledge of confidentiality was a requirement for participation. Participants received an honorarium for each meeting attended.
A series of four, 2-hour working group meetings were facilitated in-person by members of the research team (Perlman, Martin): 1. Meeting 1: Introductions, project overview, overview of the RAI-MH assessment, and outputs. We reviewed the purpose, content, and outputs of the instrument, as well as the process for completing the assessment. 2. Meeting 2: Visual and narrative representation activity, where people worked individually or in small groups (3-4 individuals) to show how information on RAI-MH domains (i.e., diagnoses, symptoms, strengths, medications, and clinician rationale) could be presented both visually and narratively. We also asked participants to write brief statements, in lay language, that they would use to describe each of the domains. 3. Meeting 3: Co-drafting narrative statements that could be used to describe RAI-MH outcomes and discussion of visual representation of symbols representing domains assessed on the RAI-MH. We projected our working document on a screen so that participants could provide real-time commentary and suggestions for both graphics and narratives as they were developed. 4. Meeting 4: Implementation considerations, where we discussed with persons with lived experiences the timing, involvement of the care team, and mode of communication related to implementation of the final product.
Key Findings and Observations
Below we describe the results of the visual representation, co-design, and implementation activities. Across all meetings it was important to establish and reiterate an agreement on boundaries among partners and meeting facilitators. During introductions, it became very clear that there were varying degrees of lived experiences with hospitalization, including positive experiences and experiences described as being very traumatic. Boundaries were established as a group to help participants’ balance their desire to share personal experiences with consideration for a safer working environment for all participants. Inclusion of a trained peer support specialist in this activity was essential for maintaining this balance.
Visual Representation Activity: Themes of Importance
The purpose of this process was to help participants centre these domains within their own experiences and to provide a free-form opportunity to express what this information represents to them. Figure 1 shows some of the drawings submitted by participants representing the various themes identified in the case study: diagnosis, physical and emotional symptoms, and strengths. Visual Representation of Themes of Importance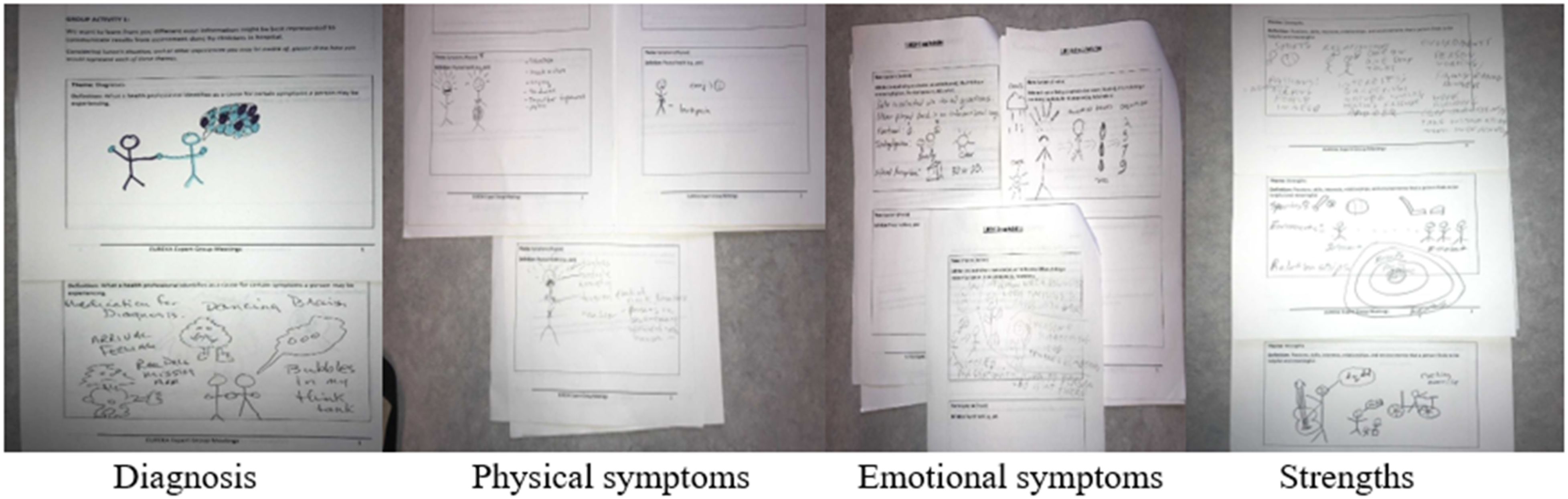
The need for help to understand what a particular diagnosis means was illustrated using bubbles with questions or feelings of confusion and showing individuals holding hands. Physical symptoms were depicted using sad faces, someone screaming/shouting/crying, as well as someone in pain (nausea, neck/back pain, and headache). Emotional symptoms were represented through use of a cloud to demonstrate negative feelings hanging over the individual, feeling of confusion/brain fog, while the sun was used to demonstrate someone experiencing clarity. There was also a depiction of someone thinking/having altered perceptions. Various areas of strengths were depicted in the drawings, including engagement in sports or hobbies, supportive relationships, positive environments, having a place to live, and ability to care for self or having independence.
Visual Representation Activity 2: Specific RAI-MH Outputs
Based on the drawings of themes, the research team identified open-source icons and suggestions from meeting participants that could be used to represent different domains from the interRAI assessment (Figure 2). While some icons resonated with the group, others less so. This section outlines the feedback received for icons to represent 4 areas of the assessment that are also a focus of several outputs (e.g., scales and clinical assessment protocols): safety, suicidality and purposeful self-harm, substance use, and depression. Visual Representation of RAI-MH Output Areas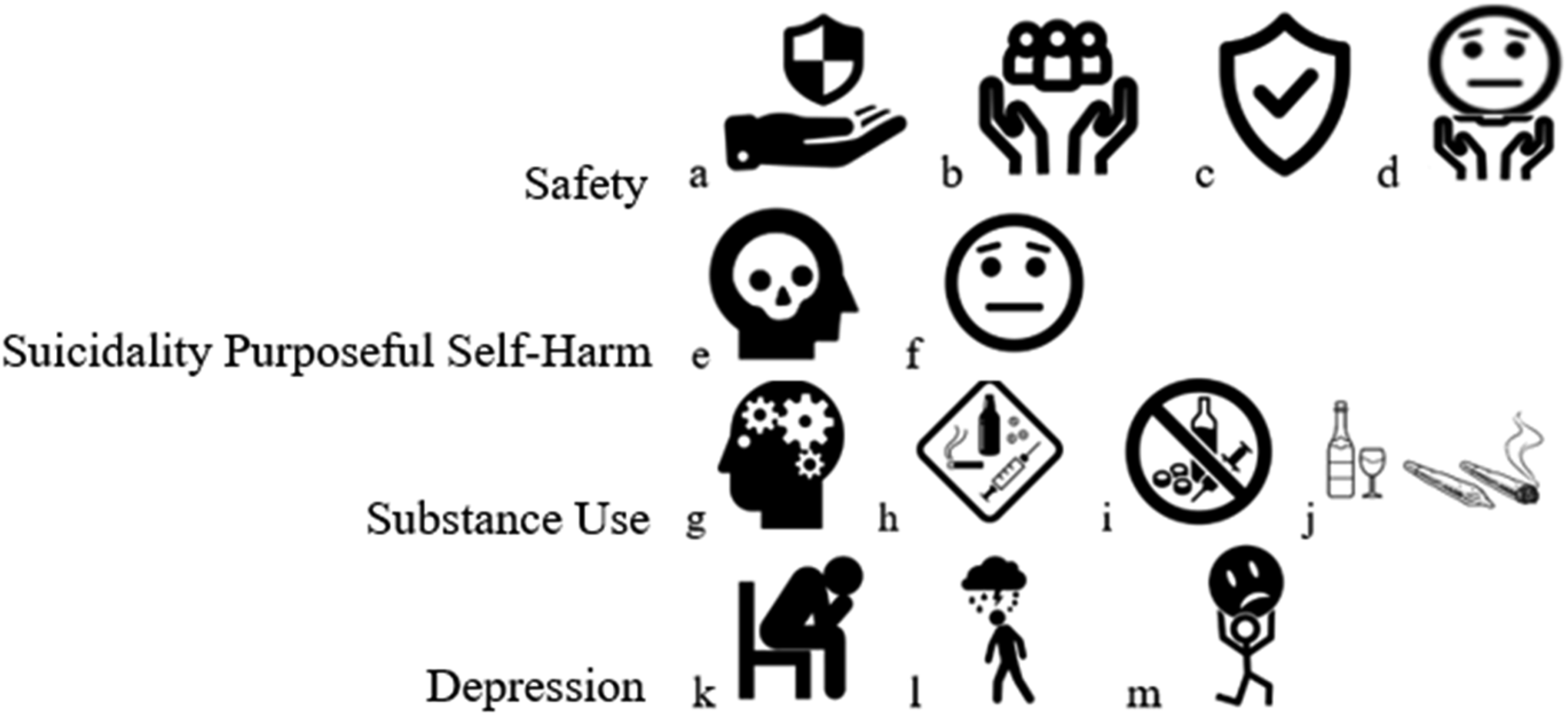
Participants were initially presented three icons related to Safety (a-c) and expressed a preference for icon b (hands with people), explaining that the use of a shield in icons a and c reminded them of the police or a badge, which they did not like. During the meeting, icon b was modified to include a face rather than a group of people (see icon d), and it was selected as the most appropriate.
Participants expressed a strong preference for icon f to depict Suicidality and Purposeful Self-Harm but were more divided on icons related to Substance Use. While some thought h was best, others viewed it as categorizing “substance use in a box,” highlighting the stigma associated with substance use. Icon i was not preferred, as it seemed to depict substance use as abstinence, which may cause those with addictions to feel judged or stigmatized. The group expressed a preference of a simple image of substances, and icon j became the preferred icon. For Depression, icon k was preferable due to its simplicity and direct representation of uneasiness and inward distress.
Drafting Narrative Summaries
Narrative Summaries
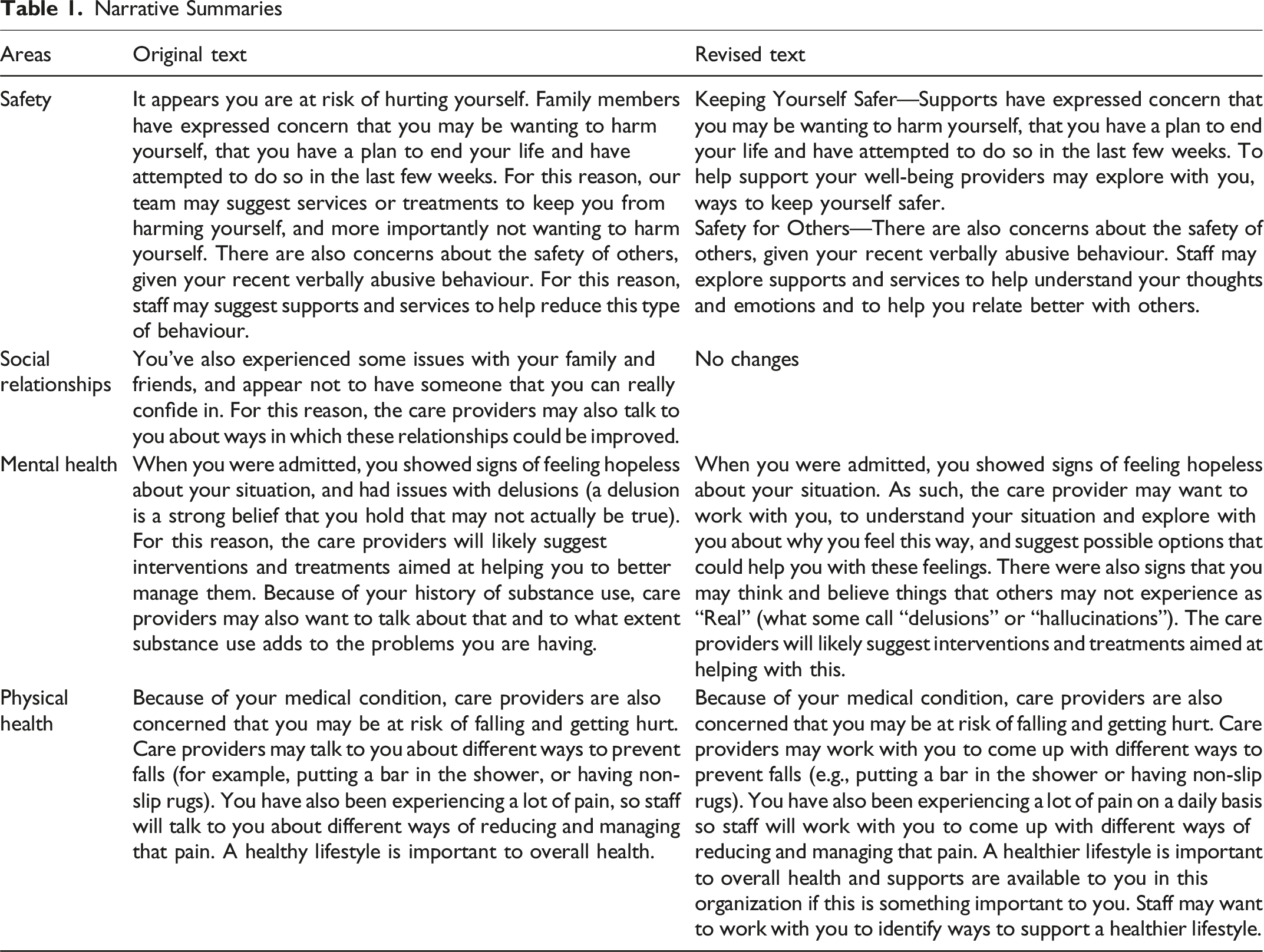
Overall, the edits focused on simplifying the sentences (e.g., turning one sentence into two sentences) and more closely aligning the possible steps by clinicians following description of issues. Some of the revisions also reflected a desire to minimize power differentials. For example, participants preferred use of terms like “work with you to find” or “explore with you” rather “talk to you about” when presenting information about possible treatment options. There were some specific important comments related to safety. Participants noted that safety exists on a spectrum and depending on the person’s situation they may never feel totally safe. As such, they suggested using the term “safer” over “safe.”
Implementation and Practice Recommendations
The working groups had in-depth discussions about the processes for accessing the “EUREKA Personal Profile” in hospital. Peer supports and patient advocates were identified as key members of the care and support team who could facilitate information sharing. While some hospitals are integrating electronic portal systems, the working group felt that a hard copy should be available to patients who may lack access to a portal device. The hard copy would allow patients to review the information in a preferred setting and make it easier to bring the information to meetings or share with supports.
In terms of timing of providing a clinical summary, some participants felt that it might be overwhelming if shared too early in an admission, as people may be experiencing acute mental health symptoms or instability. The group recommended that, once stable, the person should meet with a peer support specialist to access and review the RAI-MH summary; the peer support specialist could also help the person interpret the information.
Discussion
The EUREKA project demonstrates that meaningful patient engagement in the design and dissemination of clinical assessment information is not only feasible but essential for advancing person-centred care in mental health settings. By co-designing summary outputs of the RAI-MH with individuals who have experienced psychiatric hospitalization, this initiative highlights the transformative potential of involving patients in the interpretation and application of their own health data.
Patient engagement in summarizing clinical data is a critical step toward improving health literacy and empowering individuals to participate actively in their care and care planning. The complexity of standardized assessments like the RAI-MH often renders them inaccessible to service users and their caregivers without formal clinical training. The co-designed visual and narrative summaries developed through EUREKA offer a model for translating technical outputs into formats that are understandable, relevant, and actionable for patients. This approach not only enhances transparency but also fosters trust and collaboration between patients and providers.
Shared decision-making is a cornerstone of high-quality mental healthcare, yet it remains underutilized in inpatient settings. The EUREKA findings underscore that when patients are provided with clear, personalized information about their diagnoses, symptoms, strengths, and treatment options, they are better equipped to engage in decisions about their care. Importantly, the language and framing of information—such as using terms like “explore with you” rather than “talk to you about”—can help reduce perceived power imbalances and promote a more equitable therapeutic relationship.
Patient-oriented discharge planning is another area where co-designed summaries can have significant impact. Discharge from psychiatric care is a critical transition point, often associated with uncertainty and risk. Working with patients to design accessible summaries of their assessment data, including safety concerns, social supports, and physical health needs, can support continuity of care and improve post-discharge outcomes. 17 The EUREKA Personal Profile, particularly if it is designed to incorporate changes from the admission to discharge assessment, could be a key resource for patient empowered communication with community care partners. Moreover, involving patients in the timing and format of information sharing (e.g., printouts vs. digital access, peer support involvement) ensures that the process is tailored to individual preferences and capacities.
While the EUREKA project offers a promising model, several considerations must be addressed to support broader implementation. These include the need for clear guidelines on managing disagreements between patients and providers, ensuring data privacy and security, and working with Electronic Medical Record (EMR) vendors to operationalize patient-facing outputs. Our discussions on the implementation process did not include providers. For a fully realized system that maximizes the use of instruments like the RAI-MH, co-design between providers and patients is essential. Additionally, future research should explore the replicability of this approach with other populations, including youth, individuals with intellectual and developmental disabilities, and those from culturally diverse backgrounds.
Ultimately, this work affirms that supporting patients to meaningfully participate in shared decision-making processes is not only desirable—it is entirely achievable from an organizational perspective. Health systems must prioritize the integration of patient voices in the design and use of clinical information to realize the full potential of person-centred care.
Footnotes
Ethical Approval
Institutional review board approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.