
Abstract
Fragmented healthcare systems worldwide struggle to support patient populations with complex health and social needs. System integration requires a standardized clinical health information system to better care for these populations. This review describes how interRAI systems evolved into powerful solutions to support healthcare system integration. In response to a care quality crisis in long-term care homes in the United States, Congress mandated a standardized Minimum Data Set (MDS) from which multiple outputs were derived to support care planning, care quality, and case-mix assessment. This work drew international attention, leading to the creation of interRAI. Three decades of extensive international research, stakeholder engagement, and implementation have led to the creation of comprehensive cross-sectoral assessment systems for diverse populations, including older adults, mental health patients, and children and youth. The interRAI assessment systems, widely used in Canada and internationally, constitute comprehensive clinical assessment systems capable of supporting health system integration.
Introduction
Healthcare systems worldwide face substantial pressure from the rising burden of non-communicable disease. 1 Population ageing is associated with a notable prevalence of chronic disability, multimorbidity, cognitive impairment, and frailty.1,2 Younger populations experience a high burden of chronic mental health, developmental, and complex health conditions.3-8
Determinants of health outcomes include clinical, biological, social, economic, and environmental factors.8-10 People with chronic and complex health and social needs require continuing support services from diverse disciplines and providers. However, healthcare systems are poorly prepared to provide these because of poor coordination and communication, and regional disparities in resource allocation. The results are disjointed and reactive care, suboptimal health, and caregiver distress, leading to over-reliance on emergency services.2,8,9
Integrated healthcare combines health and social services to meet the needs of people with complex chronic health problems, by aligning financial and administrative incentives and modalities across care settings, delivering proactive care through interprofessional teams, and deploying a system-wide standardized, comprehensive clinically-based information system.11,12 The latter is required to (1) support risk stratification to direct further assessment and personalized care planning and prevention; (2) share information across sectors and populations to reduce assessment duplication and promote efficient interprofessional communication; (3) evaluate care outcomes and facilitate quality improvement; and (4) support equitable and optimal distribution of resources. 12
For context, interRAI is an international not-for-profit network of clinicians, scientists, and policy-makers whose mission is to support better lives for people of all ages, particularly the vulnerable, through excellence in assessment and research. This narrative review describes how, over 30 years, interRAI fellows responded to and collaborated with health system stakeholders to develop comprehensive clinical assessment systems capable of supporting health system integration to care better for people with complex needs.
Methods
The authors searched PubMed and the interRAI repository of peer-reviewed publications authored by interRAI fellows to highlight salient events leading to important instrument system design decisions. Ethics approval was not required. All authors are interRAI fellows.
Long-Term Care Crisis in the United States (US)
Concerns about care quality in US Long-Term Care (LTC) homes arose as early as 1959.13,14 Following prominent abuses in the 1980s, a review of LTC home quality was conducted by the Institute of Medicine, culminating in reforms mandated by the 1987 Omnibus Budget Reconciliation Act.14,15 This Act prescribed resident rights, roles of medical directors and physicians, care staff training and resources, limits to chemical and physical restraints, and improvements in care quality through the development of a standardized Minimum Data Set (MDS) for resident assessment. 14
A collaborative team of prominent clinicians, researchers, and resident advocates developed the MDS.13,14 Their project had four goals. First, the MDS replaced existing ad hoc assessment batteries usually limited to Activities of Daily Living, cognition, and diagnoses. 13 The MDS was designed to capture rigorously and comprehensively information elicited during routine clinical care to describe resident strengths, preferences, and needs. This included items related to health, mood, behaviours, sensory perception, psychosocial well-being, continence, falls, skin condition, symptoms, dental problems, nutritional status, and social engagement. 16 Second, the MDS supported care planning under a rehabilitative model to enhance resident quality of life. 13 Third, it provided a foundation for quality improvement and learning. 13 Fourth, its development process would support future refinements. 13
To enhance usability, assessment outputs were developed, including severity measures (e.g., Cognitive Performance Scale), 17 Resident Assessment Protocols (RAPs) to alert clinicians to active clinical concerns, case-mix measures (Resource Utilization Groups/RUGS), 18 quality indicators, and a user manual.17-19 Together, these components constituted the Resident Assessment Instrument (RAI), which over 90% of LTC homes in the United States had implemented by 1991. 20
These developments established essential design parameters for all subsequent interRAI instruments: 1. Inclusion of items directly related to care planning, quality measurement, or resource allocation; those solely for research are excluded; 2. Clear operational definitions of items with illustrative clinical examples; 3. Standardized look-back periods for clinical observations (e.g., “in the past 3 days”); 4. Fixed response sets with “open text” restricted to a limited set of items (e.g., person’s goals of care); 5. Clear exclusion and inclusion criteria to delineate the parameters of item definitions (e.g., vision “with glasses if worn”); 6. Assessor consideration of all sources of information, including direct interviews and observations of the person assessed; consultation with other informants (e.g., family and staff); and review of available clinical records; 7. Flexible order of assessment completion allowing for a conversational, person-centred and culturally appropriate interview; and 8. Rigorous development and testing to ensure reliability and validity.
Expansion Across Nations and Care Sectors
The development of the RAI caught the attention of like-minded researchers in Europe and Japan. In 1994, the US developers collaborated with these international colleagues to establish interRAI as a not-for-profit corporation dedicated to the application of rigorous scientific methods and cross-national comparisons to improve the care of LTC residents. Canada joined shortly thereafter, as did many other nations. International ownership and copyright of the RAI was assumed by interRAI, enhancing control of the content and validity of its assessment systems. In 1997, a landmark special issue of Age and Ageing reported the first results from direct comparisons of LTC homes based on the RAI in 10 countries and three continents.21-26 Key findings included remarkable heterogeneity in care quality (e.g., restraint use), differential access to rehabilitation, the utility of RUG systems, and the frequent premature institutionalization of persons with low care needs.23-25 These findings, and those from subsequent multinational studies, firmly established the value of standardized person-level clinical data and cross-national comparisons of health system performance.27-31 In Canada, these results prompted successful national efforts to reduce restraint use in LTC homes. 32
Requests from Europe, where community-based care was more developed than in the US, prompted the application of interRAI methodology to design a home care assessment system. While home care clients often have levels of disability and medical complexity like those of LTC residents, new items on the central role of informal caregivers and additional clinical issues (e.g., home environment and instrumental activities of daily living) were needed. 33
In 1996, Ontario, Canada, was the first jurisdiction beyond the United States to mandate the adoption of the RAI.
34
Spurred by that decision, the Ontario government partnered with interRAI to develop an assessment system for inpatient psychiatry, expanding the application of interRAI systems to adults of all ages who receive hospital-based care for serious mental health and addictions issues.
35
New substantive content specific to mental health was developed in partnership with mental health experts; this work confirmed that the methodologies to develop assessment systems for one population were transferrable to others. A deliberate design decision to ensure a core set of items in all systems provided novel insights on the mental health needs of older adults and the physical health of persons with mental health problems. This success created opportunities for interRAI to work with governments in other new assessment areas, broadened interRAI membership, and promoted greater engagement with diverse professional, advocacy, and government experts outside of interRAI. Additional systems were developed to support adults in acute care, post-acute care, assisted living, and palliative care (see Figure 1).36-39 Timeline for Development of interRAI Assessment and Screening Systems Note 1: Yellow: Initial Systems; Blue: Revised Legacy Systems; Green: interRAI Suite. Note 2: RAI: Resident Assessment Instrument; LTCF: Long-Term Care Facility; HC: Home Care; ID: Intellectual Disability; AL: Assisted Living; CHA: Community Health Assessment; PAC: Post-Acute Care; Rehab: Rehabilitation; MH: Mental Health; CMH: Community Mental Health; ESP: Emergency Screener for Psychiatry; Y: Youth; BMHS: Brief Mental Health Screener; PC: Palliative Care; AC: Acute Care; CGA: Comprehensive Geriatric Assessment; CA: Contact Assessment; ED: Emergency Department; CPCA: Community Paramedicine Contact Assessment; CCA: Corrections Contact Assessment; PEDS-HC: Paediatric Home Care; CY: Child Youth; ChYMH: Child Youth Mental Health; DD: Developmental Disability; QoL: Quality of Life; SCaN: Self-reported Carer Needs; SAMH: Self-reported Assessment for Mental Health; PAMHY: Parent Assessment for Mental Health in Youth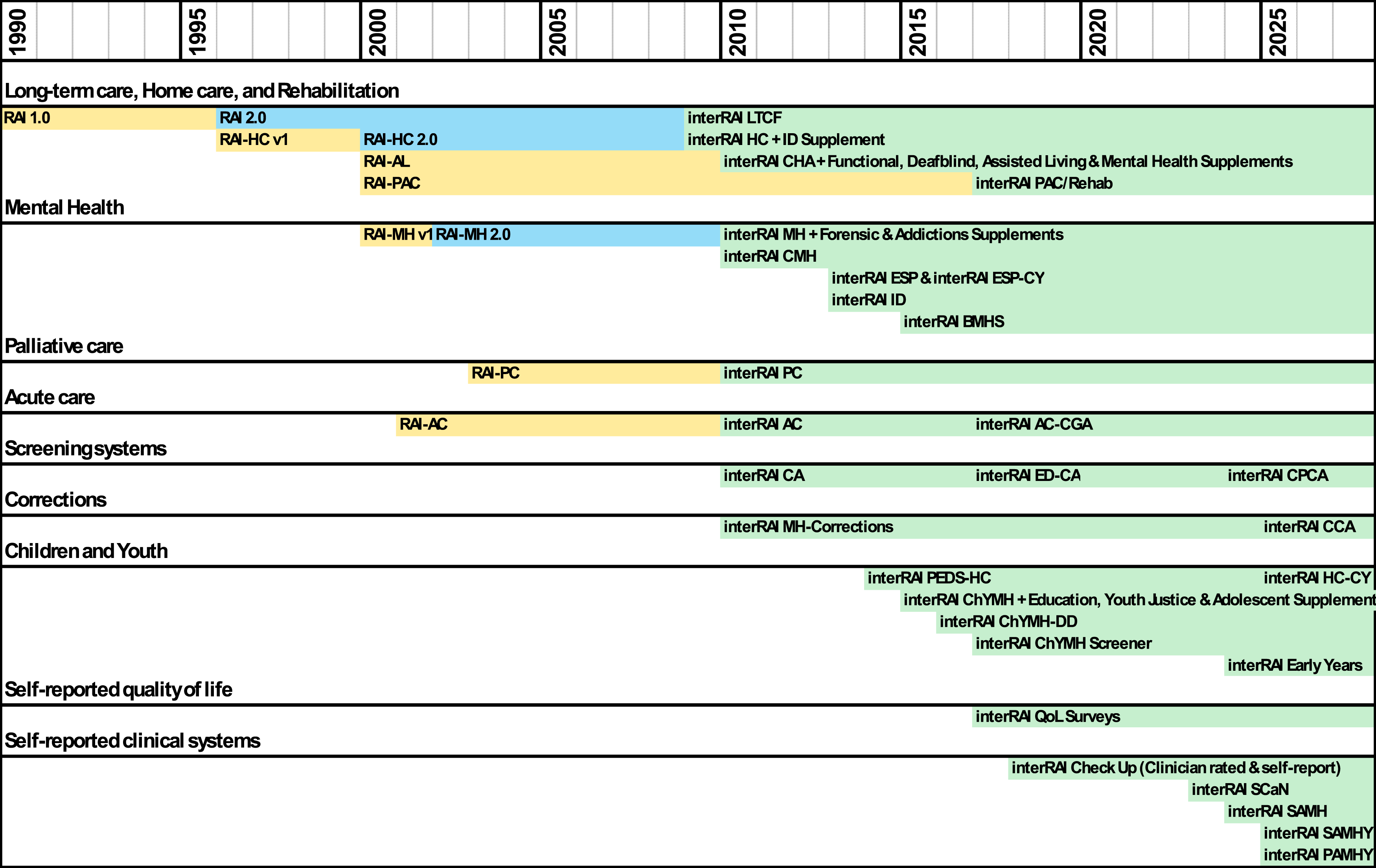
Integrated Clinical Information System Across Sectors
Despite a standard development methodology, differences in item structure between instruments, even within the same population (e.g., older adults) hindered the formation of a fully integrated clinical information system.
40
The interRAI Instrument and System Development Committee was established in 2000 to reconfigure all interRAI systems into a fully interoperable “suite” of instruments spanning all sectors of health and social services.
41
A multi-year effort to review and refine over 2,500 variants of interRAI items was undertaken resulting in additional design parameters: 1. Core domains applicable to all populations (e.g., pain, cognition, and mood) were included in each instrument unless there was a strong rational otherwise; 2. Standard wording described items used in multiple instruments, though illustrative examples could be adapted to the clinical context; a) iCODE variable names were assigned to unique items, scales, and algorithms to provide standards for interoperable software across instruments.
Having established the first set of integrated instruments in this suite, a 12-country study was undertaken to ensure inter-rater reliability internationally and across care settings. 42 Legacy instruments were updated to match the new standards, and new instruments were developed for emergency psychiatric services, community mental health, developmental services for adults, and children and youth, including high-risk infants, toddlers, and preschoolers. Supplements to existing instruments expanded their applicability to specialized sub-populations, including those with dual sensory loss and forensic psychiatry.9,43-48
The initial focus on relatively lengthy instruments for populations with complex and multidimensional needs left a gap in the assessment of lighter care populations. Then interRAI developed an interoperable set of simplified, briefer, screening level instruments for intake into home care, emergency departments, paramedicine, and mental health services.49-53 These developments allowed a more efficient stepped approach to assessment, better aligning with the heterogeneous complexity of populations in different care settings.49,54 The suite was further expanded to non-formal healthcare contexts such as police interactions with persons with mental health needs, correctional services, educational settings, and informal caregivers.55-61
The Person’s Voice
Many quality initiatives emphasize the patient experience as integral to improving health system performance; 62 interRAI developed a suite of self-reported quality-of-life surveys to explore care experiences and subjective dimensions of quality of life in multiple care settings.63-66 The quality-of-life surveys were the first interRAI systems used in low- and mid-resource settings (e.g., Rwanda and Brazil).67-70 The most recent interRAI instruments are self-reported assessments that can be completed without a regulated health professional (e.g., community health workers). Developed in response to demands for instruments to describe the needs of persons in nations with limited resources, these have also been shown to be relevant high-resource settings. The interRAI Check-Up, useful in primary and community care settings for older adults, has been validated in South Africa, South Korea, and North America.67,69,70 The PAULAS project is underway to test the Check-Up in 15 African nations. 71 The Self-reported Carer Needs (SCaN) assessment has been pilot tested in 17 nations on 4 continents.72,73 A self-report mental health instrument for adults and youth is currently being evaluated in pilot studies involving over 30 countries on 5 continents. 71 Multiple assessment systems have been translated into numerous languages and carefully checked, allowing valid international comparisons.71-74
Multiple Applications for Multiple Audiences
The interRAI instruments are considered “second and third generation” systems because the clinical information within a single instrument is deliberately designed for multiple uses, by multiple stakeholders, and across care sectors (see Figure 2).
75
Schematic of a Fully Realized and Deployed interRAI System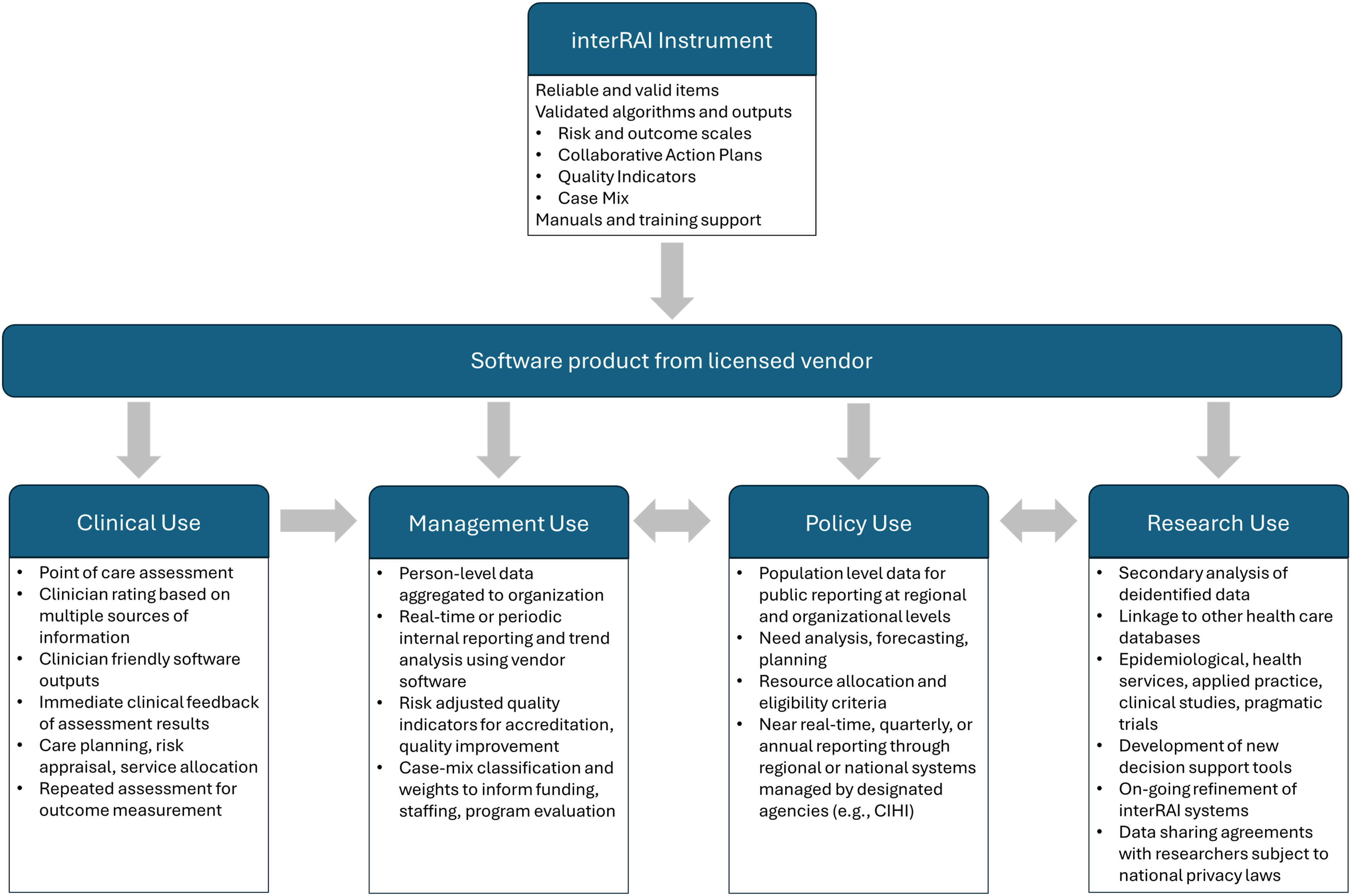
The approach of measure once, use multiple times confers several benefits. First, to achieve the primary objective of improving care, clinicians are invested in ensuring that an assessment accurately reflects the person for whom they are caring. Second, non-clinical stakeholders, such as those charged with quality improvement and equitable funding, have a keen interest in data accuracy. Finally, multiple applications provide countervailing incentives for accuracy (e.g., upcoding functional measures to attain higher case-mix values for funding would yield poorer performance on the associated quality indicator). All these are made possible when interRAI systems are computerized, so information can be derived from the basic data.
Care Planning
All interRAI assessments include Collaborative Action Plans (CAPs, replacing RAPs) comprised of triggering algorithms and best practice guidelines from international research to inform development of person-centred care plans to prevent adverse events, enhance clinical improvement, or slow decline.76-82
Outcome Measures
All instruments support scales summarizing multiple clinical domains to support comprehensive care planning. The homogeneity of items across instruments makes many scales available in multiple instruments (e.g., the Cognitive Performance Scale is found in the LTCF, home care, acute care, and mental health instruments), facilitating tracking patient trajectories across sectors.32,83 Other scales are specific to certain sectors only, such as the Forensic Problem Behaviour Scale in the mental health instrument or the Internalizing Subscale in children’s instruments.48,84
Need Analysis
With over 300 items in most assessor-driven instruments, summary measures and quality software are needed to harness the full functionality of an instrument. 76 Algorithms derived from assessments reflect risks of specific adverse events, drawing clinician’s attention to important clinical issues at the person level. These measures can also be employed by providers or governments to conduct regional or national population need analyses to inform policy and program evaluation.
Quality Improvement
Most interRAI instruments provide Quality Indicators (QIs) to assess healthcare performance in a particular sector and indicate potential problem areas that require investigation.85-92 QIs are most frequently summarized across all assessments for an organization or governmental district. Prevalence and incidence QIs are available, the latter being most powerful as they represent the strongest outcome measures of care. The comprehensiveness of an interRAI instrument allows for sophisticated risk adjustment to level the playing field for differences in populations that are not within the control of an organization. Thus, QIs permit communities of practice in which providers or governments compare quality outcomes for specific domains, identify high performing organizations, and share best practices. This approach has been successfully deployed in the LTC sector to reduce inappropriate antipsychotic prescribing in Canada, and by the Seniors Quality Leap Initiative, a consortium of providers from Canada, the United States, and South Africa.89-93 The Canadian Institute for Health Information reports interRAI quality indicators nationally for home care and long-term care through a publicly available dashboard. 94
Case-Mix
Case mix is the relationship between characteristics of the person and the need for services, to support human resource and financial planning. The first RUGs were developed to predict institutionalization into an LTC home. Case-mix systems exist for interRAI systems in home care, adults and children with intellectual disability, children and youth mental health, and inpatient psychiatry.9,95-101
Disaster Management
The interRAI systems can be used to inform disaster management including planning, prevention, emergency response, and recovery phases. Available decision support algorithms can identify vulnerable persons at risk from natural disasters and potentially requiring evacuation, including pandemics, home fires, heat waves, and air quality events.102-106
Policy
With reliable information regarding populations served, governments can understand unmet needs, geographic inequities, and alternative health system designs, allowing improved decision-making and refinements to the configuration and allocation of resources in health systems. For example, governments can use interRAI decision support systems to specify eligibility criteria and prioritization algorithms to shape resource allocation across community and facility-based care settings.107-109 The adoption of multiple instruments within and across jurisdictions makes possible a system-level perspective and allows cross-sector comparisons. 110
Conclusion
With over three decades of international research, collaboration with health system and government stakeholders, and implementation, interRAI systems can provide an integrated suite of clinical information systems for people of all ages and across the continuum of care. This suite continues to be refined as new insights are gained from ongoing cross-national research and health information needs evolve.
Unlike administrative databases, interRAI systems are first and foremost clinical instruments that person-centred, collaborative approaches to shared decision-making, and that can promote care continuity and coordination as defined by the World Health Organization.111-113 The “measure once, use multiple times” design principles allow interRAI data arising from the point of care to serve the numerous information needs of diverse stakeholders at all levels of the healthcare system. These systems offer an integrated solution to improve care, understand cross-sectoral health and well-being trajectories over the life course, and learn from others through scientifically rigorous international comparisons, thus providing clinicians and health system leaders with the information they need to allocate resources and configure health systems to care for people with complex needs.
Footnotes
Acknowledgements
This manuscript is dedicated to all interRAI fellows and collaborators that have brought the organization to what it is today. The authors wish to thank Karli Chalmers for assistance in preparing this manuscript for submission.
Ethical Approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.