
Abstract
Eight years ago, we were part of a team of authors who wrote about challenges facing public health at that time, indicating threats to public health that also threatened the health of the population and the sustainability of the healthcare system. Eight years later, the issues we discussed remain. In this article, we reflect on what “public health” is, its challenges, and its role both within and beyond the healthcare sector. In particular, we focus on the challenges of downgrading public health within governments and health authorities, of limiting the independence of public health officials, and of limiting public health’s scope by combining it with primary and community care. We conclude with the role of public health in wider society and on what could be gained both within and beyond the health sector from a strong public health system that is oriented around a well-being society.
Introduction
Eight years ago, we were part of a team of authors who wrote about the challenges facing public health at that time, indicating that the weakening of public health threatened both the health of the population and the sustainability of the healthcare system. 1
Eight years later, the issues discussed then remain a concern. In this article, we reflect on what “public health” is, its challenges, and its role both within and beyond the healthcare sector. In particular, we focus on the problems that may result from downgrading public health within governments and health authorities, from limiting the independence of public health officials, and from limiting public health’s scope by combining it with primary and community care. We end by focusing on the role of public health in wider society and on what could be gained both within and beyond the health sector from a strong public health system that is oriented around a well-being society.
So what is public health anyway?
The Canadian Public Health Association (CPHA) defines public health as “the organized effort of society to keep people healthy and prevent injury, illness, and premature death. It is a combination of programs, services, and policies that protect and promote the health of all Canadians.” 2
Public health—not to be confused with “publicly funded healthcare”
1
—can be understood in at least four main ways: 1. At its broadest, “public health” means the health of the public; that is to say, protecting and improving the health of the public. In that sense, public health is synonymous with population health or, at a more local level, with the health of a community,
1
and with all the many factors that determine the health of the community or the society. As the Lalonde report pointed out more than 50 years ago, the major determinants of health lie beyond the healthcare system. Indeed, a recent review suggests that “healthcare accounts for 5% to 15% of the variation in premature mortality, centred on 10%.”
3
2. Public health is a service within the health sector, although not necessarily within the formal healthcare system; for many decades, public health services in some provinces were located in municipalities or independent Boards of Health; this is still the case in Ontario. The core functions the public health service are population health assessment, health protection, health surveillance, disease and injury prevention, health promotion, and emergency preparedness and response.
4
3. Public health is a discipline, a field of professional practice, with a set of defined and certified public health practitioners—public health nurses, public health inspectors/environmental health officers, public health and preventive medicine specialists, medical officers of health, community nutritionists, health promoters, and others—and a set of public health professional organizations, from the World Federation of Public Health Associations to national and provincial public health organizations. There is also a set of core public health competencies for Canada.
5
4. Public health is an academic field of education and research, with schools of public health all over the world. In Canada, a 2017 review noted 31 post-secondary educational programs across 8 provinces (only New Brunswick and Prince Edward Island were not listed) with “sufficient and relevant public health content” to prepare students for a career in public health.
6
Clearly, if public health is about the organized effort of society to keep people healthy, it deals not only with health sector policies, programs, and services, but with the entire range of determinants of health: ecological, social, economic, structural, commercial, cultural, and other upstream factors as well as biological, behavioural, and healthcare determinants. 7 For that reason, the public health field and public health professionals work both within and well beyond the healthcare sector.
Public health within the healthcare system
It helps at the outset to understand that public health is in the same business as the rest of the healthcare system (which we will refer to here as “clinical care”): saving lives, reducing suffering, and improving the health and well-being of people. But they operate in very different ways.
First, as Public Health Physicians of Canada (PHPC) notes: “While other physicians concentrate on diagnosing and treating individual patients, Public Health Physicians see entire communities as their patients.” At the community level, public health works to create healthier communities, while at the provincial, national, and global levels, it seeks to create healthier societies and a healthier world. 8
In doing so, public health identifies and challenges those disparities in health which are based in economic, social, and cultural inequalities, including those rooted in sexism, racism, colonialism, and other forms of discrimination. Public health works to identify and eliminate health inequities, both as a matter of social justice and also because doing so is one of the best ways to improve overall health for a population or community. This also means supporting policies and programs that seek to ensure that all the members of society can enjoy access to the necessities of life.
Second, public health is concerned with interventions before the onset of disease, injury, or death. In terms of the widely recognized four levels of prevention (see Figure 1), public health is concerned almost entirely with primordial and primary prevention. “Upstream” primordial prevention addresses “underlying economic, social, and environmental conditions leading to causation” and primary prevention—prevention of onset of a disease or injury—focuses on “specific causal factors” such as immunization, preventing tobacco use, or wearing a seat belt. Levels of prevention.
9
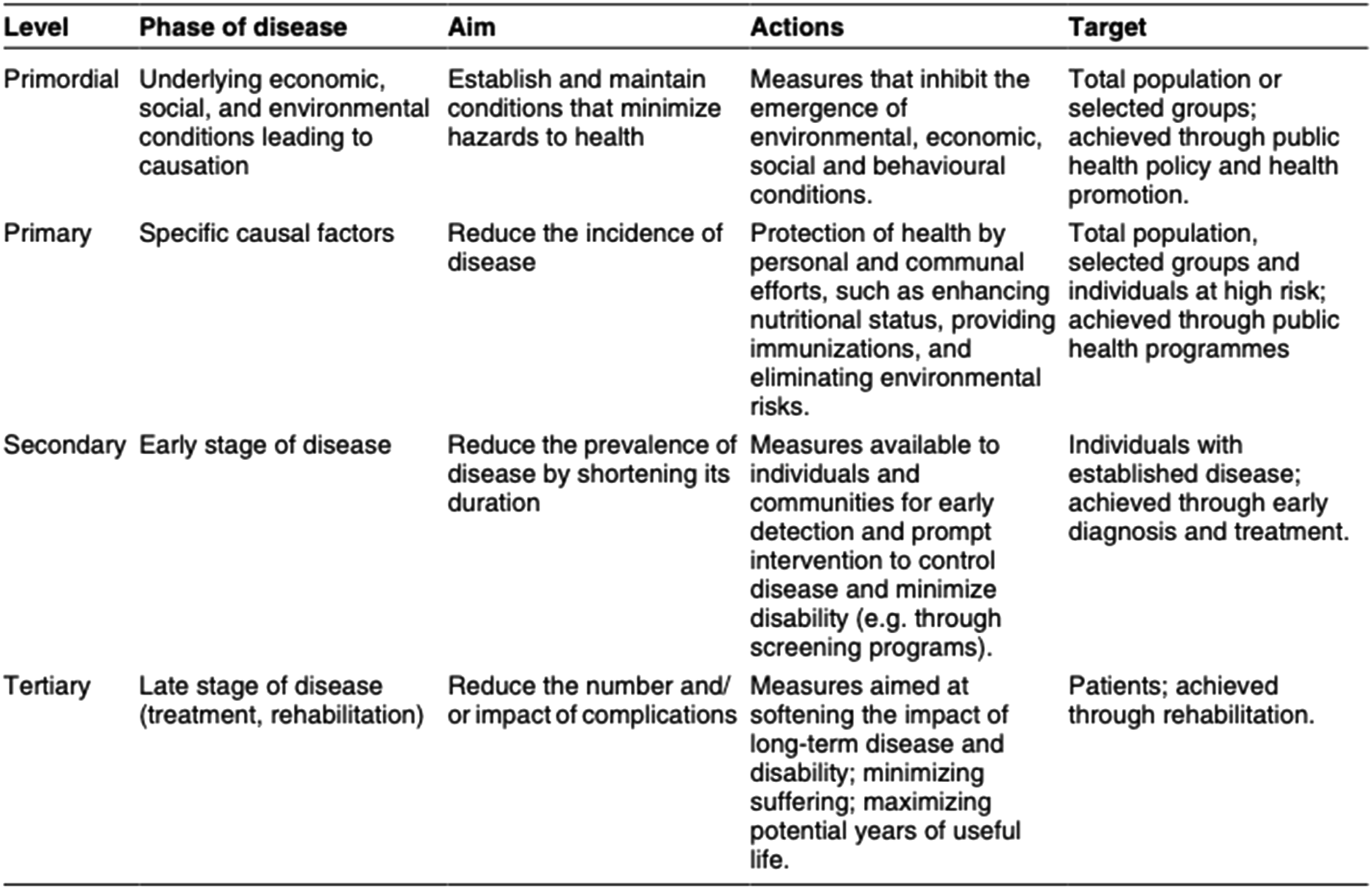
These are distinct from secondary and tertiary prevention, practiced by clinical care. Secondary prevention includes screening for early signs of disease (e.g., cancer screening), and treatment to cure or shorten the duration of the disease or injury and return people to health. Tertiary prevention seeks to limit the extent and duration of complications. (There is also quaternary prevention, which aims to protect patients from medical harm, which can extend to preventing an unhealthy death.) 10
Importantly, “primordial and primary prevention contribute most to the health of the whole population, while secondary and tertiary prevention are generally focused on people who already have signs of disease.” 9 That is why public health and its focus on primordial and primary prevention is important for the sustainability of the healthcare system; it can reduce the overall burden of disease in the population and thus reduce demand on the system.
Third, while preventive services are a part of public health, public health also does more. As noted earlier, the core functions of public health include health protection (e.g., the work of public health inspectors, ensuring safe food, water, and air and healthy environments) and health promotion, which includes advocating for healthy public policies (note that advocacy is a core public health competency), creating supportive environments for health, strengthening communities, and helping people develop health skills. 11
Many of these activities, it should be noted, take public health well beyond the confines of the health sector, as we discuss later.
Updates: The status of public health within the healthcare system today
Downgrading the status of public health within governments and health authorities
Lawmakers and decision-makers in Canada have generally acknowledged the strong professional expertise and ethical training of public health officials’ actions. Nevertheless, New Brunswick introduced Bill 104 in 2022, which created changes to public health powers, forwarding more of them to (untrained) elected officials. 12 Specifically, the Act limits the powers of the Chief Medical Officer of Health (CMOH) to interventions in a single region of the province and removes responsibilities for the CMOH in province-wide emergencies, placing them instead with the Minister of Health. Consultation with the CMOH or other public health officials during such emergencies is not explicitly required in the revised legislation.
Eroding the independence of medical officers of health and their ability to speak out on matters of public health concern
Fafard et al. have described that the right of medical officers of health in Canada to speak to the public at large has not often been explicitly protected through public health legislation in Canadian provinces and territories. 13 They further note that without the protection afforded by legislation that speaks to the scientific independence of the CMOH, there is an ever-present risk of conflict between the CMOH and provincial/territorial governments if they hold different views—regardless of the scientific integrity that the CMOH might bring—on a matter of public health interest. Alberta provides several recent examples where the independence of successive medical officers of health seems to have been explicitly curtailed. The current vacancy in the office of the CMOH has been commented on over many months by several senior public health leaders in that province, with agreement that concerns with provincial government interference in the work of that office are hampering efforts to fill the position.14,15 While Alberta provides the most current examples, examples in recent memory also include New Brunswick and also Ontario, where the SARS Commission report in 2006 highlighted the need for the CMOH there to retain independence from government with respect to communications with the public. 16 Of note, these examples are in contrast to jurisdictions such as British Columbia and Newfoundland, where the public health acts carefully outline expected independence of the CMOH and thereby demonstrate ways in which such expectations can be created in the Canadian context.17,18 The Newfoundland example is particularly compelling, given that this legislation was only newly created in 2020 indicating recent favourable (political) attitudes towards public health officials there.
Limiting public health scope by combining it with primary and community care
In Alberta, the recently introduced Bill 55 has moved core public health functions, including health protection functions related to communicable disease, to a new primary care agency, Primary Care Alberta. 19 Similar to New Brunswick, these changes seem to have been designed without widespread consultation with public health experts in Alberta or elsewhere. 20 Analogous changes are underway in Saskatchewan. These developments signal a lack of knowledge in legislative and political decision-makers regarding the profound differences between necessary primary healthcare and public health actions and structures, as outlined above. The primordial prevention work previously mentioned requires public health to be engaged with actors well outside of healthcare systems, and in that way is markedly distinct from delivery of primary healthcare. A key enabling structure for primordial prevention is one that allows access specifically to intersectoral policy tables for the purposes of intervening in systems and communities to prevent risk factors for disease for ever occurring.
Public health in the wider society
As we have demonstrated above, as a discipline committed to keeping people healthy and preventing injury, illness, and premature death, public health necessarily has to move beyond the health sector and engage directly with the broader determinants of the health of the population.
This has always been contentious work. Cipolla has described the conflicts between public health officers and merchants in the Renaissance city states in Italy, while 19th century public health had to struggle against the health harming impacts of industrialization and urbanization and the powerful commercial and political forces driving those changes. 21
Two centuries later, public health remains concerned, at the community level, with the impact of built environments on people, related to transportation and air pollution, traffic safety, availability of natural environments, existence of “food deserts,”22,23 availability of social connection, and the myriad other factors that contribute to or detract from a healthy community. These public health concerns in turn require interrogation of oppressive capitalist and consumerist constructs, and so public health’s work remains contentious, but necessary.
More broadly, we are faced with what United Nations (UN) Secretary General Antonio Guterres has called “a confluence of challenges unlike any other in our lifetimes.” 24 The combination of these and other crises has been called a “polycrisis”: “the causal entanglement of crises in multiple global systems in ways that significantly degrade humanity’s prospects.” 25
These massive and rapid global and national changes (war, ecological destruction, widening inequalities, and the pernicious impacts of social media) threaten the health of the population as a whole, and particularly the health of the most disadvantaged and vulnerable.
It is on this basis that public health professionals are required to advocate for all of the things that promote good health; far from being a “dirty word,” advocacy is a duty, as well as a core competency. 26 While such advocacy may be reasonably well accepted when it addresses such obvious issues as tobacco use or drunk driving, it is less well accepted when it challenges powerful social, political, or economic actors, and this can lead to pushback—itself proof of the importance of such advocacy.
Public health in the 21st century: Towards a well-being society
In the face of the polycrisis, a new approach to organizing our whole society is needed: putting the well-being of people and the planet—not the performance of the economy—at the heart of governance. As the World Wide Fund for Nature (WWF) has noted, “Ecosystems sustain societies that create economies. It does not work the other way around.” 27 The economy, in other words, must be re-designed to be in service to the well‐being of people and the planet.
In its Geneva Charter for Well-being, the World Health Organization (WHO) proposes the creation of well-being societies “committed to achieving equitable health now and for future generations without breaching ecological limits.”
28
This involves five key action areas: • Value, respect, and nurture planet Earth and its ecosystems. • Design an equitable economy that serves human development within planetary and local ecological boundaries. • Develop healthy public policy for the common good. • Achieve universal health coverage. • Address the impacts of digital transformation.
We suggest that the practical strategies needed for effective action in these areas must result from renewed deep reflections of public health and health system leaders. As such reflections are not commonly undertaken, we invite leaders to consider the following questions to prompt reflection and further action: • How are we valuing, respecting, and nurturing planet Earth and its ecosystems? Are we being environmentally responsible in all aspects of our operations and are we working with others in the community to create healthy natural environments? If not, why not? What stands in our way? • How are we helping to design an equitable economy that serves human development through responsible labour practices, responsible purchasing, combatting commercial practices that harm health, and calling for the creation of well-being economies locally, provincially, and nationally? • How are we working locally, provincially, and/or nationally to encourage governments at all levels to examine the health impacts of their policies and to ensure that public policy in all sectors reduces inequalities in health?
A renewed dialogue within the health system co-led by a strong public health system and focused on collective well-being as an outcome could shed some light on these important questions and suggest health system contributions to a sustainable future for us and for the planet. We conclude, then, by suggesting that strengthening public health is an important antecedent to effective actions towards improving societal outcomes such as well-being.
Footnotes
Ethical approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.