
Abstract
Canada’s federal structure is the institutional reality informing our system of public health. While there are advantages to this decentralization, it can also lead to fragmentation and inefficiencies. Calls for stronger federal leadership or better collaboration between jurisdictions are common, but they do not directly address the question of why there has been so little progress in moving in either of these directions. Through the lens of six key public health functions, this article describes contextual realities and disparate interests of the jurisdictions. These underpin a dynamic for public health decision-making in which rational decisions can lead to suboptimal outcomes collectively. Understanding the dynamics of federalism underlying public health in Canada can help us to identify and address barriers to a more effective public health system.
Why focus on federalism?
The structure of Canadian federalism is highly relevant to public health service delivery, with both advantages and disadvantages. Better understanding this context can help health leaders achieve goals of improving health and decreasing inequity.
From pathogens to environmental contaminants to social determinants of health, the subjects of key concern for public health are notorious for their disregard of political boundaries. More than any other area of health services, public health addresses issues that transcend jurisdictional and intersectoral borders. Yet federal systems are designed precisely to limit authority within clearly circumscribed regions. Canada, which assigns considerable responsibility for health to the Provinces and Territories (PTs), faces even deeper distinctions between the realities of localized authority and the calls for national public health approaches. A deeper and more nuanced understanding of Canada’s federal structure and how this impacts decision-making in public health is a critical step in moving toward a more coherent and integrated public health system.
Federalism can be advantageous in geographically large or culturally diverse countries: for example, to increase citizen participation or to minimize over-concentration of power in a particular geographic/cultural group. 1 But federalism also has notable limitations, and public health is no exception. The phrase “Why don’t they just…?” occurs often, and usually with a certain level of frustration. But this misses an opportunity to learn from and work with the tensions that exist, improving health systems and health outcomes.
This is particularly relevant to health leadership in Canada. All leadership styles require thoughtful adaptation to context. Federalism is an important contextual layer in Canada, particularly when efforts are being made towards interjurisdictional collaboration or legislative/regulatory change.
The structure of federalism
This section outlines existing structures, previous calls for changes, and suggests that a deeper analysis of policy tensions can help with next steps.
Federal distribution of powers set out in the Constitution Act. a
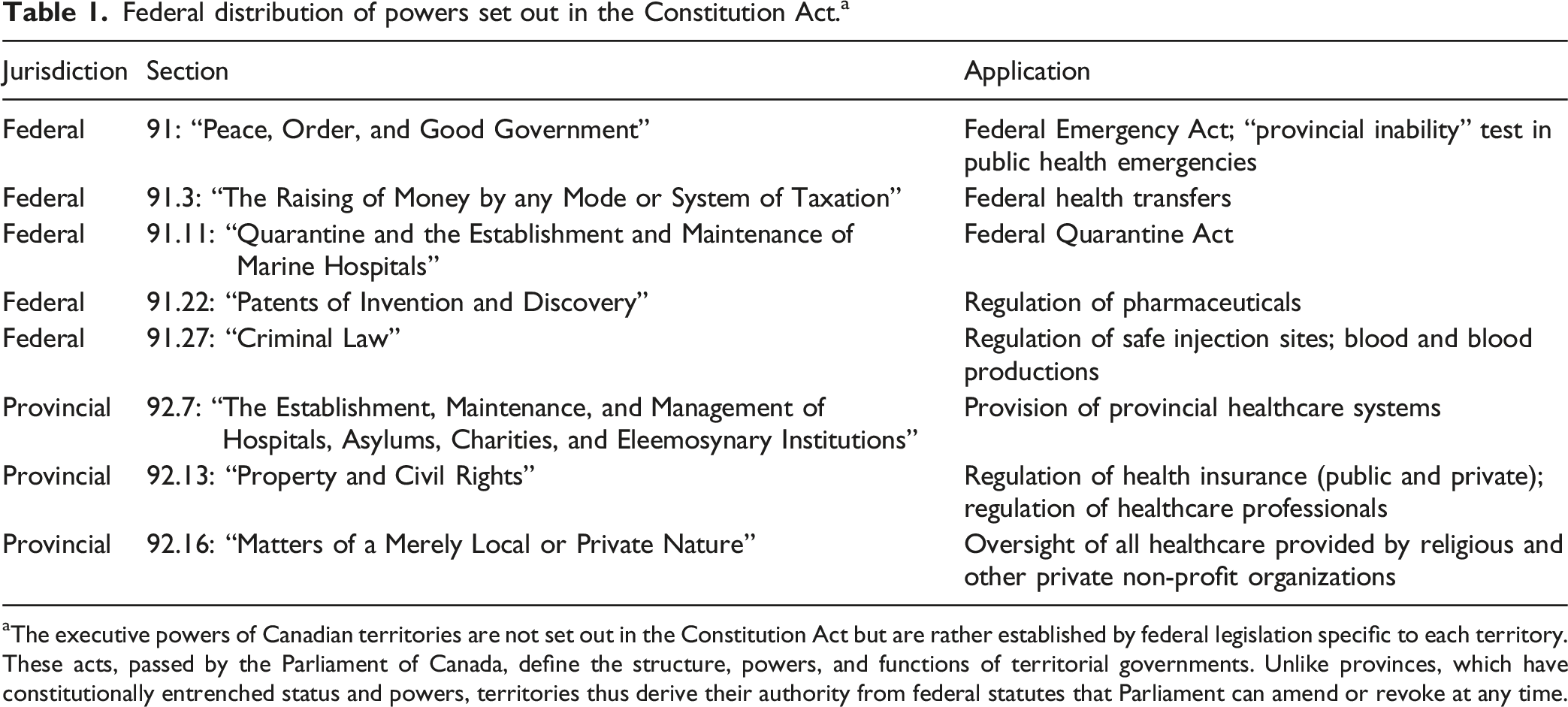
aThe executive powers of Canadian territories are not set out in the Constitution Act but are rather established by federal legislation specific to each territory. These acts, passed by the Parliament of Canada, define the structure, powers, and functions of territorial governments. Unlike provinces, which have constitutionally entrenched status and powers, territories thus derive their authority from federal statutes that Parliament can amend or revoke at any time.
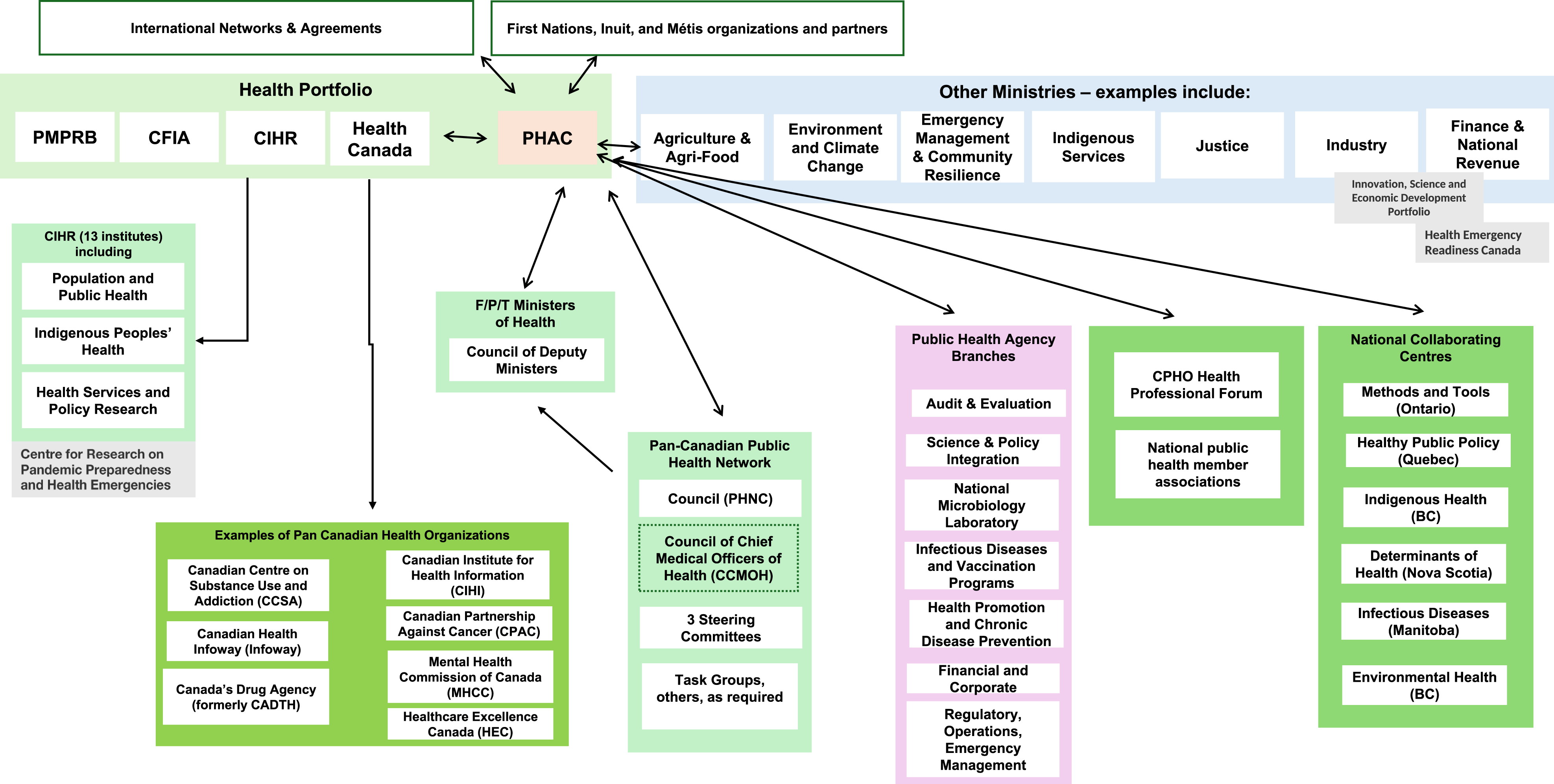
Network of administrative links maintained by the Public Health Agency of Canada. (Adapted from Fierlbeck, 2011). Note that this figure provides examples and is not exhaustive, and there are others (e.g., universities).
Despite the recognition that FPT jurisdictions must work more closely together, there has been less focus on the question of why, if a more integrated national system of public health is so compelling, there has been so little progress in this direction(2). 6
Path dependency can lead to outcomes PTs and federal teams have not have intentionally chosen. Unlike most of Canada’s comparator states, for example, Canada does not have a single national immunization schedule. Rather, each of the PTs has its own schedule, while the federal government has one as well. This can impact the spread of and response to outbreaks across jurisdictions. 7 Moreover, a patchwork of immunization guidelines can cause considerable confusion, especially given the mobility of Canadians across PT jurisdictions. The same holds true with reportable disease lists, which differ slightly across FPT jurisdictions, as well as cancer screening guidelines. While different infrastructure, funding processes, and geography can explain some difference, does this much divergence make sense within a single country?
Given the institutional constraints imposed by Canada’s federal system, the obvious strategic pathways to achieve a more robust public health system have focused on either greater centralization or more FPT collaboration. The former approach endorses greater “federal leadership” within the parameters of Canadian federalism; a recent manifestation was the 2022 report by the Canadian Public Health Association. 8 The second approach, seeking greater collaboration between all jurisdictions, is evident in the creation of the PHAC with recommended regional connections in the wake of the 2003 SARS pandemic(3). 9 Both aspirational approaches, in theory, make perfect sense; yet both face ongoing impediments that constrain progress in either direction and limit the ability of Canada to provide a coherent and efficient public health framework. This article examines these dynamics in greater detail in order to show why generalized exhortations to “just get along” fail to appreciate why the desired level of collaboration so often fails to materialize.
Intergovernmental tensions in public health functions
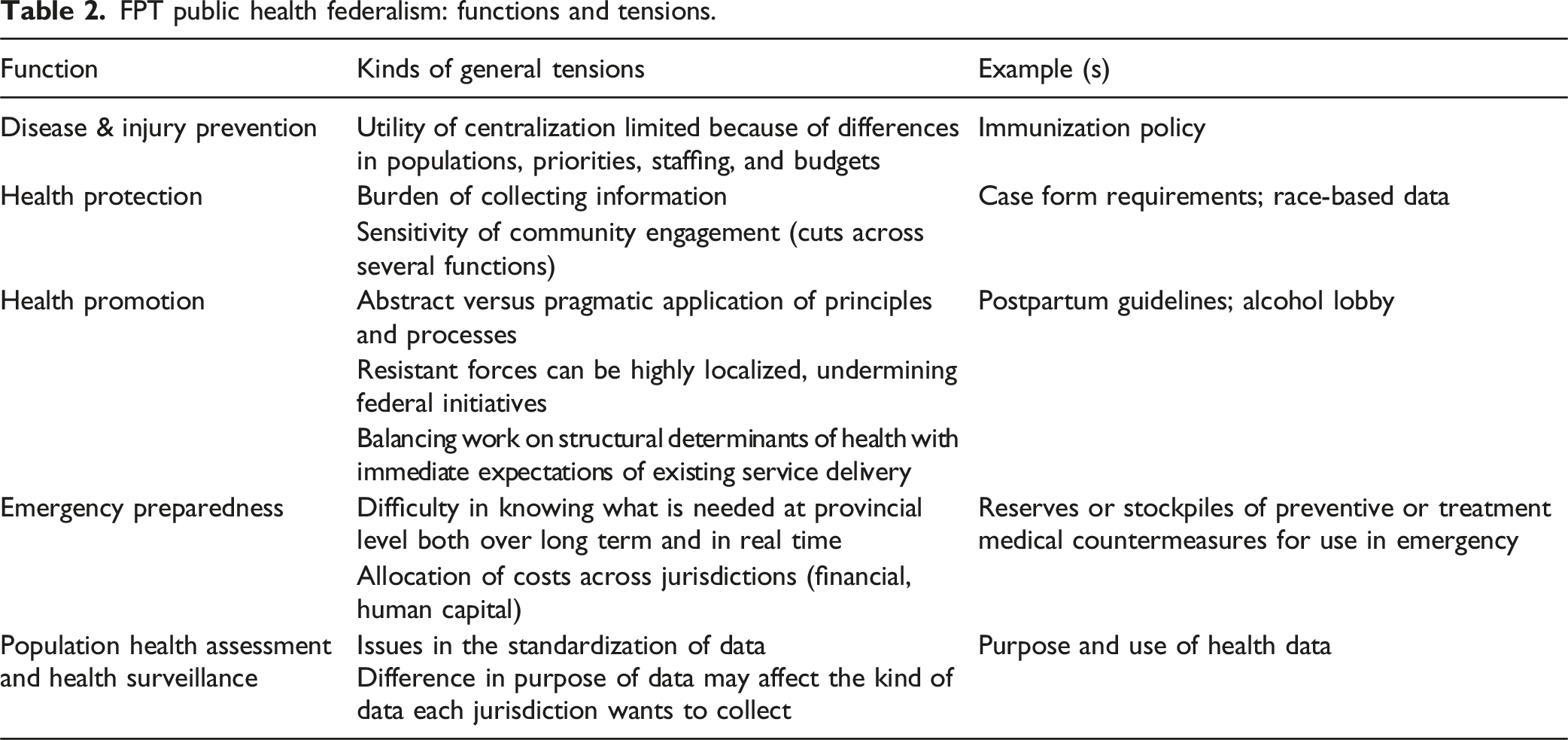
FPT public health federalism: functions and tensions.
Health protection
While there are examples across more than fifty reportable communicable diseases and numerous air/water/soil/other environmental health hazards, COVID-19 highlighted many issues of interjurisdictional public health governance. One early concern was the risk of transmission within large congregate work settings, especially in remote settings (such as mining sites) where workers frequently moved across PTs. As McGill et al. point out, Early detection and notification of an outbreak with the potential for interjurisdictional spread is essential to an effective multijurisdictional outbreak response … there are numerous examples of rotational workers returning from industrial worksites with active outbreaks spreading SARS-CoV-2 to household members and starting community outbreaks in their home jurisdiction.
14
To better address these multijurisdictional outbreaks, PHAC’s Outbreak Response Unit (ORU) created “enhanced setting-specific” questionnaires to supplement information collected in the national COVID-19 case report form.
But, while more robust data can sometimes assist in understanding and addressing public health events, attention must also be given to the burden of collecting information. This is especially important where time and staffing are severely constrained. Over-collecting information that is underused or misused can also badly impact trust. In the case noted above, the “enhanced questionnaire” (to be given in addition to the standard COVID-19 case report form) was 21 pages long. Each questionnaire may have to have been completed for hundreds or possibly thousands of individuals. Unsurprisingly, national-level initiatives that include labour-intensive “outbreak response protocols” and “outbreak investigation tools” may be viewed by PTs with wariness if they are perceived to impose burdensome costs on local resources or require significant legal acts such as blanket indemnification. This is particularly true when initiatives lack direct evidence of impact—either of improved health outcomes or decreased health inequities.
From a federal perspective, it can be difficult to find the best ways to be supportive when legislative and regulatory authority is less clear. Provinces and territories have relatively clearly defined scope, ownership, and responsibilities in both public health and healthcare service delivery. There are often expectations of national-level organizations to contribute but a lack of clarity on how to do best to so. Further complicating this, provinces and territories may often ask for slightly different ways of doing things. This can further hamper harmonization and standardization.
Effective health protection at the local level may also require the careful and gradual establishment of relationships between local public health officials and marginalized communities. 15 In some cases, such as the COVID-19 pandemic, this involved the collection of race-based data. Unsurprisingly, PTs were concerned at the way in which this data could be used or represented and were often resistant to sharing this information more widely given the sensitivity of the data and the significant efforts made in establishing the trust of community leaders. 16
Disease and injury prevention
Immunization schedules provide useful insights into federal dynamics. As a country, we tend to end up with broadly similar coverage but often with slightly different timing and formulations. This can lead to additional complexity both for administration and also attempts to buy in bulk as a country. For example, while PTs begin administering measles-containing vaccine to children at the same age, there are differences in adoption of MMR-V as opposed to MMR as well as the timing of the second dose. There is even more variability with the specific tetanus, diphtheria, and pertussis vaccines. Some of this variation can be explained by an increase in the number of available vaccines. 17 More specifically, factors such as cost effectiveness, public acceptance, feasibility (including staffing), and the burden of disease (ibid) contribute(5). 18
Provinces with older populations may choose to focus on enhanced influenza vaccines; those with a large congregate university population may prefer to cover meningococcal B vaccines. Yet it is not simply a matter of choosing which vaccines to prioritize, but also the best way to administer and also pay for them. There is nuance to some trade-offs. For example, better seroprotection is achieved with Hepatitis B vaccination between the ages of 5 and 15 (99%) but this means not having protection before the age of 5. In communities where Hepatitis B is more common, especially where young children are susceptible, it may make more sense to vaccinate children before they are 2 years old, which still provides 95% protection. 19 Differences in vaccination schedules between provinces and territories reflect these nuances.
Health promotion
Of all the public health functions, the understanding of “health promotion” is perhaps the one most debated by public health specialists. Once focused directly on the elimination of disease and illness, the “failure to translate good intentions behind health promotion” into better health, especially for more vulnerable populations, has led to a rethinking of how to conceptualize health promotion. 20 Rather than simply focusing on clinical indicators of health, these approaches suggest that more subjective measures of quality of life or perceptions of meaningfulness have a strong impact on health indicators (or even that they ought to be measures of “good health” in and of themselves). But if this is the case, then localism becomes much more important in pursing health promotion goals. 21 There are also considerations of balancing underlying structural determinants of health and the distribution of power, money, and other resources, as well as how worldviews and ways of being are prioritized.
A different kind of barrier can also impact national attempts at building a comprehensive health promotion strategy. Many countries have introduced policies focusing on smoking cessation, limiting advertising of unhealthy foods to children, or limiting alcohol consumption; it would seem logical that Canada too should attempt to establish these kinds of strategies at a national level. But powerful industries can be affected by such proposed policies, and provinces/territories can be unwilling to support health promotion policies that may jeopardize the economic well-being of local food and beverage industries(6). 22
Emergency preparedness
Much has been written about the FPT relationship in pandemic preparedness including role clarity and coordination. 23 But even when such apparently clear divisions of responsibility exist, more nuanced issues still surface regarding both the way in which emergency preparedness should be operationalized during periods where emergencies are not evident and, conversely, when scarce resources are needed in real time. This became evident during the COVID-19 pandemic, when critical resources were in short supply. In theory, PTs can have their own supply stockpiles, while the federal government’s National Emergency Strategic Stockpile (NESS) provides surge capacity. Yet when the pandemic began, Ottawa had little idea what PTs had in their respective stockpiles, while the PTs were equally uncertain about the composition of the federal stockpile. 24 Processes were also unclear about how to flow supplies to areas of greatest need.
The issue of stockpiles can be quite politically and logistically complex. Where they are not needed for long periods of time, they can be expensive to run, with a high degree of waste incurred due to the disposal of large amounts of expired goods. One means of addressing this is to rotate supplies into current health service delivery, thereby continually updating supplies and keeping supply “fresh” without wastage. 25 If applied to federal stockpiles, however, this would entail coordinating federal supply and delivery with separate hospital governance structures within each PT: not impossible, but not a simple exercise either.
Even more problematic is the question of precisely what resources Ottawa should supply during emergencies, especially with emergent technologies. During COVID-19, for example, Ottawa bought large quantities of rapid tests and distributed them to the PTs. But there were also concerns about the effectiveness and opportunity costs of using the tests as part of the overall response within PTs. This caused a public outcry in some PTs where governments were asked why they were not releasing rapid tests when other jurisdictions were distributing them freely. This, in turn, led to some PT resentment, as federal activity indirectly forced provincial and territorial policy-making into directions they had not wanted to go. 26
Population health assessment and health surveillance
Both assessment and surveillance require a robust and workable data framework. There has been considerable analysis of why Canadian health data is suboptimal (see, e.g., Goel, 2021). 27 Because Canada is such a decentralized federal system, this problem is exacerbated because of the considerable “path dependency” each jurisdiction has experienced in the collation and development of their health data systems. Data standardization is therefore a significant undertaking. Moreover, the way that data is used does not always consider specific PT context. For example, physician billing and shadow billing data is used for CIHI databases, but this doesn’t work in provinces or territories where the physicians are not paid fee-for-service and also do not shadow bill.
The purpose for which data is collected can also influence the way in which jurisdictions choose to collect information. Federal bodies want to be able to compare data across jurisdictions; this need for harmonization may require local particularities to be ignored or smoothed over. And federal data objectives generally have longer time horizons, so idiosyncrasies become less relevant. But PT public health service delivery is often required to respond to active issues in real time, from outbreaks of hepatitis or measles to water contamination to rabies exposure. In these cases, more granular information can be quite valuable, and general data collection templates can be an impediment. Finally, as noted above, in cases where public health information can be perceived as politically sensitive (e.g., for vulnerable groups), PTs may be reluctant to share this information if they do not know how it will be used (e.g., if information that may provoke tensions between communities will be made public). 1
We are not the only country or region of the world that struggles with these dynamics. The European Commission for example has used a collaborating and convening approach for evidence-informed policy that we can look to for learnings.
We also write this article recognizing that much of our approach in health systems across the country is rooted in the biomedical worldview that is dominant in Western medicine that has its own strengths and limitations. There is a richness and strength in other worldviews, in particular those of First Nations, Inuit, and Métis, that include opportunities to learn from connection to the natural world and intergenerational thinking and learning. There have also been related summaries for FPT health systems policies. 28 Other articles in this edition explore these questions in greater depth.
Conclusion
The principal aspect of public health federalism is the institutional structure on which it rests. As there is no regular direct federal funding for public health per se, this relative financial autonomy creates a dynamic giving PTs considerable power through simple inertia. Another important dynamic is perspective: the immediate interests of federal and PT governments often simply don’t align. Each jurisdiction may be acting rationally in seeking different routes towards shared outcomes, given their constraints and context. Health leaders, especially when working interjurisdictionally or on legislation/regulation, can be alerted for “why don’t they just?” statements. This provides an opportunity to identify the tension(s) at play and find ways to mitigate them and move forward. It can also provide a flag for outcomes to monitor, evaluate, and learn from. Understanding the nuances and tensions that produce the dynamics we have now can help us shape the steps towards the system we want.
Footnotes
Acknowledgements
With thanks to Nadine Purdy, Asantewa Quansah, and Menaka Shanmuganantha for support with formatting.
Ethical approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jasmine Pawa works as a public health physician.