
Abstract
This article outlines the key functions and practices of government in addressing a public health crisis. Governments are responsible for planning and coordinating, resourcing and responding, and revising and evaluating. These three core functions are supported by cross-cutting practices in governance, accountability, and communication. Health leaders are advised to ensure that their organizational emergency plans intersect with those of government, and that they have processes to work with public health, government, and other partners to support robust responses to health crises.
Introduction
Responses to public health emergencies are an area of active global scholarship. Researchers and practitioners have highlighted the importance of strong public health institutions, 1 addressing uncertainty, 2 and resilience 3 in responding to public health emergencies. Before COVID-19, there have been policy papers focused on the role of intergovernmental processes in addressing public health, 4 and COVID-19 remains a key event for observations around how emergency plans translate into policy interventions 5 and on the roles of public health officials in health emergencies.6,7
My experience involves work as a public health physician at both regional and provincial/territorial levels in Canada for over a decade, as well as several years prior to this in a training capacity in public health and medicine. During this time, I have participated in and lead public health response activities related to many health emergencies and “crises,” as well as the multi-year COVID-19 pandemic. Canada has a multi-level system of government where health is largely allocated to sub-national jurisdictions. Yet, a nationwide public health emergency requires a national approach for fulsome impact.
Based on my involvement with governments that relied on federal coordination and action, I consider the role of the federal government to be the same whether or not a public health crisis exists—only the scale and the speed should be different between routine operations and emergencies. Most of the problems faced by governments in emergencies are due to delayed action rather than inaction, as well as decision entrenchment. So critical decisions come too late to make a difference, or not at all. And, if the situation has changed by the time the decision is made, it is difficult to reverse or change course.
Another significant challenge is that “crisis” and “emergency” have definitions that are subject to considerable interpretation. The World Health Organization defines emergency as “a situation impacting the lives and well-being of a large number of people or a significant percentage of a population and requiring substantial multi-sectoral assistance.” 8 By this definition, almost all public health issues of today (food and housing insecurity, access to clean water, cancer, adverse childhood experiences, injuries) fit the definition of emergencies just as easily as COVID-19 did. The breadth of this definition is problematic for deciding on the scale and speed of action to address the issue. Rather than being a set of criteria that triggers a unique response, the words “crisis” and “emergency” are increasingly used as advocacy tools to draw attention to an variety of issues that are each different in scale, scope, and cause and require different responses.
Finally, the government has many obligations outside of the country (through international health regulations, for example) and within the country (to Indigenous populations, for example) that must be maintained and fulfilled during an emergency—not being an expert on these I have not written about them but I believe they fall under the umbrella of accountability practices that ensure that existing obligations are upheld.
Key functions
The approach described below is based on government organizations, and it is also relevant to health organizations in their responses to health-related emergencies. I propose that rather than worrying about how to do things differently in an emergency, we should consider how to do the same things bigger, better, and faster. One of the ways in which this can be done is by deciding in advance which decision-making structures (such as emergency operations centres or incident command structures) and protocols will be used for public health emergencies, and resourcing these for scalability. The actions below constitute what I believe are the basic functions of government with respect to the health of the public (see Figure 1). After describing them, I will discuss how they should be adapted in emergencies or crises. The three major areas of government work to support health routinely and during crises are: planning and coordinating, resourcing and responding, and revising and evaluating. Overview of government roles in a public health emergency.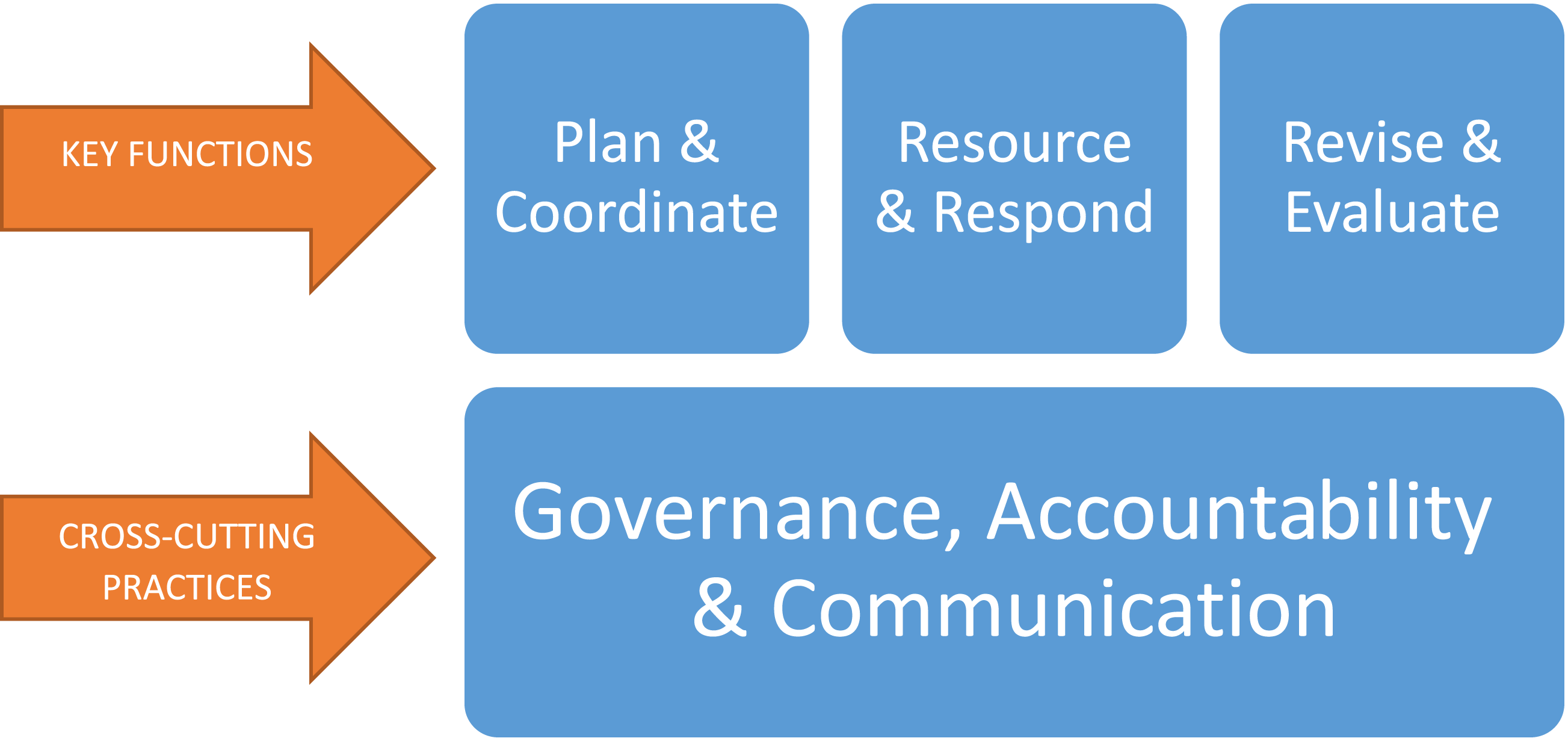
Planning and coordinating
Government is responsible for planning and coordinating responses to all national emergencies, and this ability is similarly important during health crises and emergencies.
9
This includes internal coordination within the government, as well as broader multi-sectoral and intergovernmental coordination. (a) Preparing: The federal government should work with provinces and territories to have health emergency plans that clearly outline the thresholds for declaring the emergency, the process by which the emergency is declared, as well as the general responsibilities of managing the emergency and how these are shared. This document should be clear enough to allow flexibility while also delineating who is accountable for what part of the response. (b) Surveillance and situational awareness: The government should either have or coordinate surveillance activities for public health purposes. It should also have processes for maintaining situational awareness within and outside of the country, and for integrating scientific evidence into its decision-making cycles. (c) Issue assessment and prioritization: The above processes will result in issues being identified. These issues need to be assessed and prioritized based on actual, potential, real, and perceived risks and benefits. There should be a framework of information gathering and evaluating that enables a relative comparison of issues in an emergency, to ensure a high quality triage of issues for resolution. (d) Scoping: Determine the scale and importance of the crisis relative to other health priorities and relative to other societal priorities. Identify the jurisdictions affected, and the role of each level of government (federal, sub-national, and regional/local) in addressing the issues presented by the situation. Develop mechanisms to keep situational awareness at different levels of government—global, multinational, national, sub-national, and local. Assess the likely duration of the crisis. (e) Convening: Since health is the constitutional responsibility of provinces and territories, without overriding their decision-making autonomy, it can be challenging to have a federally coordinated response to a crisis. There may be a need to predetermine when or if provincial/territorial autonomy needs to be superseded, how that would work, and for what decisions and duration. Yet, the federal government has a convening power that should be exercised to ensure provinces and territories can share information and strategies for managing health emergencies together.
Resourcing and responding
The government is responsible for resourcing and responding to the emergency. Certainly, COVID-19 vaccines could not have been obtained effectively if each jurisdiction were trying to negotiate with vaccine manufacturers. Similarly, government support for human resources and physical goods to address the pandemic was crucial, especially in smaller jurisdictions. The response of government to a health emergency involves the following areas: policies, programs, people (and money and things), and partners. (a) Policies: Federal policy responses to health emergencies are crucial, especially in the areas where only the government can enact such responses. During COVID-19, for example, federal policies were used to financially support business operations in key industrial sectors, to govern federally regulated industries such as air transport, and to adapt entry requirements to Canada based on emerging information about infections. Pre-assessment of the kinds of policy tools that are available should also be considered in developing emergency response plans. (b) Programs: One of the main intervention targets for the federal government should be the programs that it runs and funds. Adjusting program parameters, funding, eligibility, and reach is a critical segment of the federal government’s response to emergencies. So, for example, expanding the eligibility for financial aid and tax relief to individuals impacted by COVID-19 was a key programmatic intervention to address pandemic impacts on individuals. Such program changes should be considered in advance of a pandemic or emergency such that they can be rolled out efficiently. (c) People (and money and things): Emergencies require the ability to bring on additional human resources to address the multitude of issues that can arise. It is infeasible to quickly scale up human resources for such operations without pre-existing procedures to reallocate and onboard existing staff (based on the need of the emergency as well as continuity of operations plans for essential services). In addition, there should be a mechanism to speed up recruitment practices for temporary periods as needed during the emergency. Of course, the government will also need to invest in procuring goods and in directly financing many elements of the response operations. This can only be done effectively with enough human resources to manage the procurement, financing, and other processes that must occur. (d) Partners: Partners are an overlooked resource that should be utilized in an emergency. The federal government has the ability to partner with other public and private sectors for all of the above. The challenge in an emergency is that the process of partnership development could take longer than the emergency itself, and governments and partners will have differing expectations around risk tolerance, budgeting, and other implementation pieces. You can’t do the work of building these relationships in the middle of managing an emergency and are more likely to rely on networks and connections that you have already built. So, my advice is that the government should intentionally build a wide network of relationships for emergency management and consider MOUs to retain and harness partnerships through non-emergency times that can be leveraged in emergencies.
Revising and evaluating
Health emergencies are characterized by dynamically changing states of knowledge, context, values, and behaviours. Accordingly, there must be a way to review and revisit these changes during an emergency response. Just as in routine situations, it can be challenging to prioritize reflection and revision, and there are institutional inertias and biases that prevent governments from reversing decisions previously made, even if they no longer fulfil the purpose of response. A good example of this inertia during the pandemic is the implementation of any population-wide restrictions on movement, gatherings and so forth—even if these were deemed to be necessary, they were almost invariably implemented and removed later than would have been optimal because of institutional change processes that are not able to accommodate the necessary speed to respond. Ongoing questions (at least every decision-making cycle) to ask during an emergency response are: (1) What is the overall goal of the response? (a) Has it changed, or does it seem like it will change soon? (2) What are the current sets of interventions being used in the response? (a) How well is each intervention working to achieve its portion of the stated goal, and how would we know? (b) What information do we need from the interventions and from our resources above (people, programs, policies, and partners) to better understand how well our efforts are working? (3) What interventions need to be changed or discarded? (4) What interventions need to be added (and why?) (5) What is the best available time estimate for return to routine operations?
Cross-cutting practices
The domains above address the “What” of health emergency responses by the government. I have outlined what the government should do in its response. I will now address parts of the “How”—the mechanisms by which such actions should take place. I believe these are cross-cutting practices that are foundational to an effective response, and these are three general areas: communication, accountability, and governance.
Governance
The response to a health emergency must have a pre-determined governance structure that allows for real-time decision-making and implementation. This structure must include where authorities and responsibilities lie for different kinds of decisions. Although health is a provincial responsibility in Canada, many true health emergencies require resources and coordination at the federal level, so it may be that an alteration of traditional roles is needed in order to properly manage the emergency—if we do not have the ability to centralize decision-making in an emergency, the response will always be scattered, haphazard and uncoordinated. At the same time, regional flexibility may be needed in terms of implementation and these conversations should be had in advance of a true emergency so that differences in implementation based on contextual need are not seen as disorganized or preferential. A good example during the COVID-19 pandemic was the prioritization of Northern Territories for COVID-19 vaccine distribution—these communities lack healthcare infrastructure, require long distance travel to access ICUs, and are already restricted by structural barriers to health and healthcare, and the numbers in communities are so small that it makes sense to immunize as many as possible at once rather than consider population tranches. These real contextual factors necessitate an altered implementation of vaccine delivery, but they should be understood and planned in advance so as not to be perceived as preferential.
Accountability
Health emergency response frameworks must clearly establish what the government is accountable for, to whom, and when. Accountability is supported by efficient documentation systems, and I am hopeful that AI and other such technologies might revolutionize this space to allow for timely and accurate documentation of events and decisions. Accountability in the response involves information and data management, financial and budgetary management, and meeting legal obligations and commitments that the government has to other nations as well as within Canada.
Communication
The deliberative decision-making process within government can result in excessive layers of approval required for any government communication. Communications plans should be developed by the government for emergencies, and these should include “short-cut” communications pathways for time-sensitive information to be publicly communicated. There are too many media platforms and channels to describe here, but each platform has a value that should be understood and utilized to promote effective communication of government processes, decisions, and actions. Notwithstanding the need to communicate in many languages (not just the official ones), as well as the need to communicate at many levels of literacy, the types and depth of information to be provided need to be thought out well before an emergency. In general, the public should be provided with at least three types of communication: quick bursts of information to update on a situation, longer segments of information that outline decisions and how they are being made, and synthesized versions of high-volume information flows such as policy options, evidence of interventions, and evaluations of actions.
Conclusion
No emergency response is perfect. We can anticipate many perspectives and values engaging in the “rights and wrongs” of decisions made in a public health emergency, and these play out simultaneously with the response itself. It is important to have mechanisms to take in these perspectives while not paralysing decision-making by trying to meet everyone’s needs. What is critical is the iterative speed, the processes which support those iterations, and how well they document the reflection on the diversity of perspectives before, during, and after an emergency response. Although this framework addresses government functions, it can be applied and adapted to health organizations in their emergency response as well.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no external financial support for this project, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required.