
Abstract
Wait times for elective surgical procedures in publicly funded healthcare systems impede patient well-being and resource efficiency. Patients with gallstone disease requiring semi-urgent intervention are often treated via inpatient emergency pathways due to limited elective surgery access. This study aimed to evaluate the rationale and cost-effectiveness of providing timely outpatient semi-urgent cholecystectomy. We retrospectively reviewed 512 patients with urgent biliary disease (excluding cholecystitis) who underwent surgery between July 2019 and December 2022. The primary outcome was time from booking to operating room; the secondary was the estimated cost of prolonged hospital stays. Patients waited an average of 26.45 hours; 19.1% waited 48 hours or longer, and 6.2% waited 72 hours or more. The associated cost was $405,785 over 40 months. Implementing semi-urgent surgical resources could reduce costs, improve efficiency, and enhance patient quality of life. Future work should involve stakeholders to address barriers and facilitators in Canada.
Background
Patients awaiting elective surgical procedures remain a growing challenge in settings with fixed resources. Canada spends more on healthcare than most high-income countries with universal healthcare systems, and ranks highest for expenditure on healthcare as a percentage of Gross Domestic Product (GDP).1,2 Despite this, Canada ranks last for wait times, with 38% of patients reporting waiting 4 months or more for elective surgery.1,2 These lengthy wait times occur when the demand for elective surgery exceeds the accessible supply of surgical-related resources. Clinicians and health leaders within these systems must make decisions on how to allocate available resources, and who to prioritize for surgery. 3 Health leaders often encounter operational inefficiencies when delivering medical and surgical care, which leads to wasted resources.3-5 Recognizing the urgency of this issue, provincial governments have begun to allocate significant funding towards a surgical recovery strategy aimed at reducing wait times and enhancing system efficiency. 6
Canada’s healthcare system has historically faced significant challenges in delivering timely and efficient emergency surgical care. General surgeons were responsible for both elective and emergency cases, which led to delays and competition for operating room access. Recognizing the need for a more effective approach, Canadian medical leaders endorsed the Acute Care Surgery (ACS) model in 2009. 7 Under this new framework, many Canadian hospitals implemented dedicated emergency general surgery teams, protected blocks of operating room time, and streamlined pathways of care to ensure timely interventions for patients presenting with urgent surgical issues. With the advent of the ACS model, resources and personnel were dedicated to emergency general surgery aiming to provide prompt and specialized care for patients with urgent surgical needs. 7 Studies have since demonstrated that the ACS model has reduced time to surgery for emergency general surgery cases, improved resource utilization, and enhanced patient outcomes. 8 The ACS model in Canada represents a significant shift towards organized, efficient, and patient-centred emergency surgical care.
As surgeons become increasingly constrained by limited access to elective surgical resources, they adopt mitigating strategies of managing semi-urgent outpatient indications through inpatient emergency pathways. 9 Notably, patients admitted from the emergency department with gallstone-related disease generally fall into two categories: those requiring cholecystectomy to treat the current presentation (e.g., acute cholecystitis) and those in whom cholecystectomy is performed to prevent future episodes (e.g., biliary colic or cholangitis). The impact of prolonged admissions for semi-urgent indications to access emergent surgical resources has not been well studied. Understanding the effects of this practice on individual patients and the healthcare system is crucial in the eventual development of solutions for semi-urgent patients.
While the Canadian ACS model provides dedicated resources for emergent general surgery, and elective resources are in place for scheduled, non-urgent surgeries, semi-urgent general surgeries represent a neglected gap. Although semi-urgent cases are non-life threatening, timely intervention is critical in order to avoid re-presentation (i.e., recurrent choledocholithiasis or recurrent pancreatitis). 10 These cases therefore frequently compete with both elective and emergency surgeries for Operating Room (OR) time. The current model of prolonged admission to facilitate cholecystectomy through urgent ACS operating room time often results in semi-urgent cases being postponed when true emergencies arise, resulting in a cascade of delays, evidenced by our results. Semi-urgent cases may alternatively displace elective surgeries when prioritized using elective resources, exacerbating already lengthy wait times for elective procedures. Adapting the ACS model to better accommodate semi-urgent cases could help address these challenges. By designating a dedicated semi-urgent surgical pathway—complete with allocated resources and scheduled OR blocks—semi-urgent patients can receive timely care without competing directly with emergent or elective cases. Such an approach can also decrease unnecessary inpatient days.
At a large tertiary care centre with more than 1,000 inpatient beds across multiple campuses, patients diagnosed with cholangitis, choledocholithiasis, or gallstone pancreatitis follow a protocol of same-admission laparoscopic cholecystectomy unless otherwise prohibited by patient-related factors. The structure of the current system fails to account for the potential benefits of semi-urgent surgical intervention for this patient population that can be managed as an outpatient once the acute presentation is resolved. This study aims to evaluate the impact of prolonged admission for patients with semi-urgent indications to utilize emergency surgery resources in an academic institution on patient length of stay and associated costs within a publicly funded, universal healthcare system.
While there is substantial literature on the efficiency and cost-effectiveness of emergent and elective surgical pathways, there is a notable lack of Canadian data specifically addressing cost-effectiveness and wait times for semi-urgent cholecystectomy. Our study fills this gap by quantifying the financial and operational impact of prolonged admissions for semi-urgent indications and highlighting the need for more efficient surgical pathways. By doing so, we build on existing knowledge of the ACS model and demonstrate how a targeted semi-urgent program may yield significant cost and efficiency benefits—an area not well explored within the Canadian context.
Methods
Study design
This is a retrospective chart review conducted at a large academic health institution. The local Research Ethics Board reviewed the proposal and approved the project as a quality improvement and program evaluation initiative. The Knowledge to Action – Implementation Roadmap (KTA) framework was followed, which frames three phases for implementation of a program or change. 11 The KTA framework is a widely used model in implementation science that facilitates the translation of evidence into practice. It emphasizes the dynamic and iterative processes required to move knowledge into healthcare systems effectively. 12 The KTA consists of two main components: knowledge creation and the action cycle. This study is focused on Phase 1 of the action cycle, which involves identifying the knowledge-to-practice gap, assessing local context, and determining barriers to optimal surgical care delivery for semi-urgent cholecystectomy. The KTA framework positions this study within a larger theoretical tradition of health services research and implementation science, reinforcing the rigour and relevance of our approach to healthcare system improvement.
Study population
Patients who underwent laparoscopic cholecystectomy at the inpatient campuses of a large academic institution between January 1, 2019 and December 31, 2023 were included for review. Inclusion criteria were patients 18 years and older, with a diagnosis code that did not include acute cholecystitis and were booked for laparoscopic cholecystectomy as either a priority D (surgery to be done within 8 hours of case request) or priority E (surgery to be done within 24 hours of case request) priority. Exclusion criteria were patients without recorded diagnosis codes, or patients with diagnosis code that included acute cholecystitis.
Data collection
Data were extracted from the Electronic Medical Records (EMRs). The following variables were collected: medical record number, patient age at time of surgery, patient ASA (American Society of Anesthesiologists) score, patient admission diagnosis, time of surgical case request, time of surgical procedure, case priority, patient admission date and time, patient discharge date and time, and length of stay. Manual chart review was performed of all D priority cases to capture cases booked as an E that were then upgraded to D. As the patients analyzed excluded cholecystitis as a diagnosis, the upgrading of priority is driven by a pressure to facilitate surgical access as opposed to a changing clinical priority. All cost data are reported in Canadian dollars. These costs reflect both direct expenses (e.g., nursing staff, medications, and meals) and indirect expenses (e.g., laboratory tests, imaging, allied health services, housekeeping, finance, and record-keeping), as collected through the hospital’s financial department and submitted to the Ontario Ministry of Health via Ontario’s case costing data. All data was anonymized and entered into a secure database. The primary outcome of interest was waiting time between time of surgical case request and time of surgical procedure. Secondary outcomes included cost associated with length of stay.
Statistical analysis
Descriptive statistics were used to analyze the data. Continuous variables were summarized as means and Standard Deviations (SD) or medians and Interquartile Ranges (IQRs) as appropriate, and categorical variables as frequencies and percentages.
Ethical considerations
This study adhered to the principles of the Declaration of Helsinki. Patient confidentiality was maintained throughout the study by anonymizing data before analysis.
Results
Demographics
Demographic and clinical characteristics of patients undergoing laparoscopic cholecystectomy.
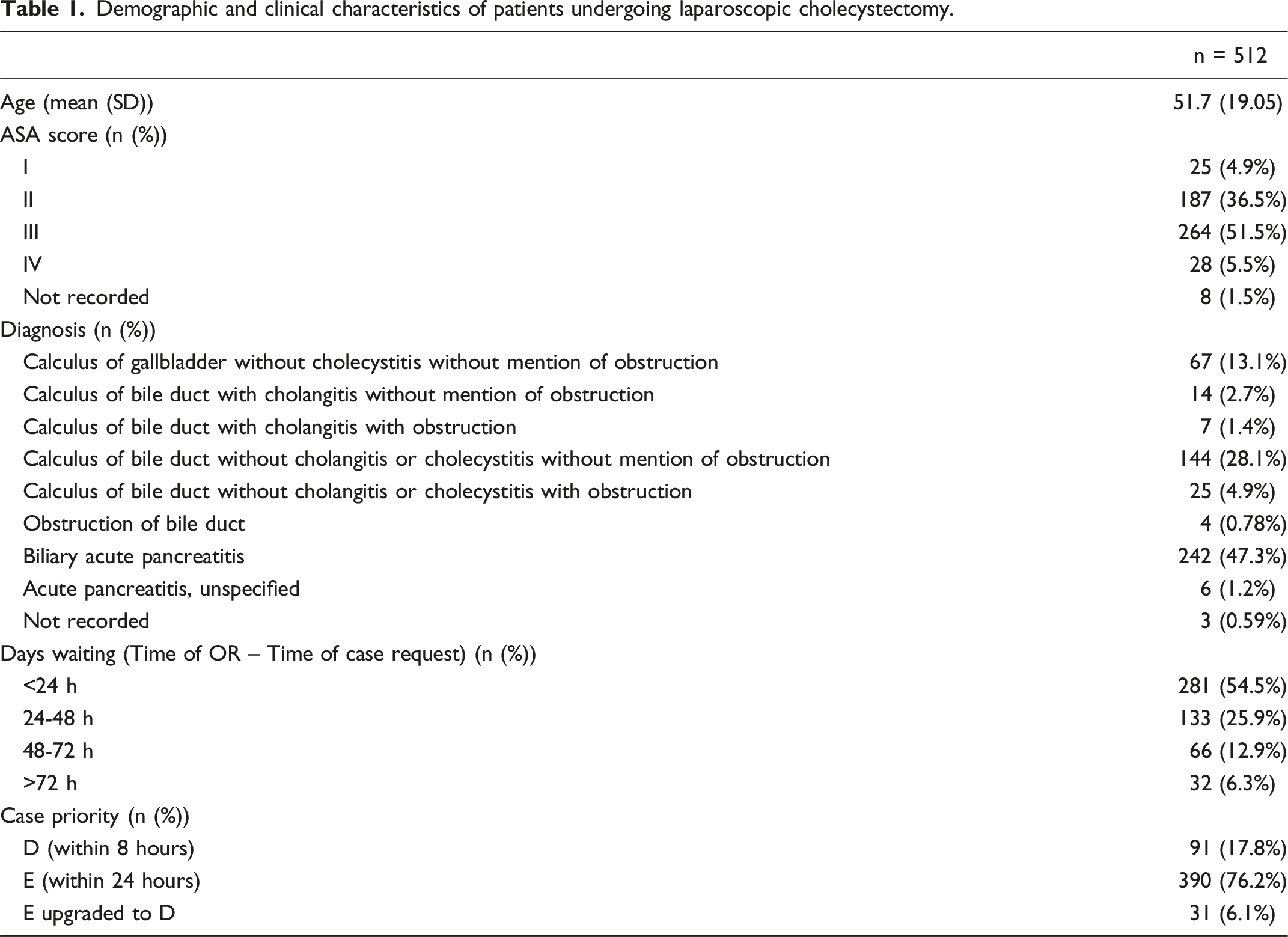
During the study period, 512 cases of laparoscopic cholecystectomy were analyzed, divided into three priority categories: E upgraded to D (5.8% of cases), Urgent D (15.6%), and Urgent E (78.6%). The distribution of cases across these categories highlights the reliance on Urgent E scheduling.
Wait times
Distribution of laparoscopic cholecystectomies by time of day and day of week.

Cost
Waiting times and associated costs for laparoscopic cholecystectomy by case priority.

Discussion
Our results provide valuable insights into the wait times and associated resources for semi-urgent cholecystectomies at a single academic care centre. Forty-five percent of patients admitted to hospital with a semi-urgent indication for cholecystectomy waited more than 24 hours for their procedure. The associated cost with this unnecessary wait time for the cases included in our study is approximately $400,000. These costs are incurred from the time the surgeon makes a case request for surgery, to the time of surgical procedure. When scaled to a larger provincial or national context, these figures highlight the broader implications of resource inefficiency; addressing it through targeted interventions and semi-urgent scheduling models has the potential to significantly reduce both direct costs and the indirect burdens on patients and hospitals alike.
Our findings build on existing literature demonstrating how health system design can impact surgical wait times and costs. More importantly, this study adds new information by focussing explicitly on the cost-effectiveness and resource utilization of semi-urgent surgical cases within a Canadian context, where such data remain sparse. By quantifying the economic burden associated with prolonged admissions, we highlight the potential for significant system-wide savings if semi-urgent cases are managed through a dedicated resource and workflow. This directly addresses the lack of Canadian data on semi-urgent cholecystectomy cost-effectiveness and highlights the need for further research in this area.
The principles of Value-Based Care (VBC) focus on delivering high-quality healthcare that optimizes patient outcomes while emphasizing patient-centredness, efficiency, and equity. This approach shifts the focus from volume-based models to value-driven care.13-15 VBC is an international framework that can help to achieve improved patient care and outcomes, cost transparency, and capacity to meet current needs. 13
One of the core principles of VBC is the emphasis on patient-centred care that considers the impact of management plans on patient quality of life. It has been previously demonstrated that extended waiting periods for general surgery procedures were associated with poorer general health perceptions, increased anxiety levels, and more negative emotional reactions.9,16,17 Additionally, many patients reported disruptions to their social activities and work life during the wait. 18 Our results highlight the number of days patients with semi-urgent biliary pathology spend admitted to hospital for unnecessary waiting, creating a disruption in their work and social lives during the wait. These patients are often fasting for multiple consecutive days in preparation for an OR that may continue to be postponed accommodating incoming surgical emergencies.
The unnecessary and prolonged patient hospitalization occupies beds that may serve patients in need of acute care. This effect contributes to hospital overcrowding, delays in care, longer wait times, and potentially worse patient outcomes. 19 This disruption in patient flow and increased burden on healthcare professionals is inefficient from the perspective of the healthcare system and contradicts the principles of VBC.
Extended hospital stays also inflate healthcare costs due to increased use of resources such as staffing, medical supplies, and facility operations. Canadian hospitals have been reported to frequently operate beyond capacity, and unnecessary admissions contribute to this problem. 20 Our results highlight the cost of semi-urgent patients, who are otherwise safe for discharge home, during their unnecessary hospital stay for access to ACS resources. Surgical cases that were initially booked as an E priority (within 24 hours) and upgraded to D (within 8 hours) due to expiry had an associated cost of $1,206.90 per case. In an alternate model, such patients can be discharged home once ready (i.e., the date of the initial surgical request), and return for a semi-urgent outpatient procedure, where the cost more similarly reflects that of the D priority, $387.70. Minimizing unnecessary inpatient days is crucial for enhancing healthcare efficiency and reducing cost within Canada’s healthcare system.
There are several limitations to this study. Our data were collected from a single academic institution in Ontario. These results may not be generalizable across Canada or in community settings, where resources or resource allocation may be different. The retrospective nature of this study limits the ability to control for all potential confounders. To mitigate selection bias, all eligible patients during the study period were included. Given this is a retrospective study, the data collected were limited to what was available in the electronic medical record. We were unable to collect additional details of the demographics of the study population to compare between populations, and assess outcomes across different social and economic strata. Missing data were addressed by complete case analysis, and patients with missing data were excluded from analysis. Finally, we relied on diagnosis codes entered into Epic EMR to identify eligible patients; some eligible patients may have been excluded if incorrect diagnosis codes were entered.
Our study highlights a need for increased outpatient semi-urgent surgical programs. Such programs could be developed as an extension of acute care surgery models that traditionally focus on inpatient surgery. The allocation of specific resources for semi-urgent surgeries could reduce competition between emergent and elective cases, while ensuring timely care for semi-urgent patients decreasing the risk of complications from prolonged delays. Integrated semi-urgent care pathways can enhance value-based care by improving the efficiency of care delivery by the system and impact on quality of life for patients, while preserving good clinical outcomes. Reducing the unnecessary length of stay for semi-urgent patients also reduces the associated unnecessary costs and harms of prolonged admissions. These findings provide a compelling basis for policy-makers and healthcare administrators to invest in dedicated semi-urgent pathways, aligning with broader efforts in Canadian healthcare to optimize resource utilization and minimize surgical wait times.
Future directions of this work include phases two and three of the Knowledge to Action – Implementation Roadmap. Stakeholder engagement among policy-makers, healthcare professionals involved in the provision of semi-urgent care, and patients are necessary to develop a proposal for a semi-urgent model. Patient reported outcome measures should be explored to capture the direct measure of patient impact.
Footnotes
Author contributions
Conception and Study design: MC, VI, PG, MM, and FB
Literature Review: DC and SM
Data acquisition: MC and VI
Data Analysis and Interpretation: MC and VI
Drafting of the manuscript: MC, VI, DC, and SM
Critical revision: PG, MM, and FB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no external financial support for this project, authorship, and/or publication of this article.
Authors’ note
Research was conducted at The Ottawa Hospital and Ottawa Hospital Research Institute.
Ethical approval
Not applicable (retrospective chart review with anonymized data; no direct patient contact).