
Abstract
Learning health systems are promoted as solutions in Canada to bridge the disconnect between research and care delivery by integrating applied research and evidence supports within healthcare. Patients and clinicians see and experience healthcare system gaps and are therefore uniquely positioned as co-producers and partners in research to advance learning health systems. Practice-based research programs provide point-of-care healthcare professionals with training, mentorship, and nominal seed funding to conduct small research projects in their clinical contexts to address gaps in practice and care. Patient-oriented research engages patients, caregivers, and family with lived experience as partners in the process of identifying gaps, generating knowledge, and applying evidence to inform healthcare delivery. This article describes the benefits gained from unifying patient-oriented research programs in British Columbia, Canada, under a provincial collaboration to standardize practice and advance collective priorities, including the foundation to cultivate and support learning health systems transformation.
Introduction
The concept of the Learning Health System (LHS) has garnered much attention over the past decade. The LHS was first proposed in 2007 to capitalize on the evolving health data landscape, including the expansion of electronic health records and database infrastructures, as a strategy to rapidly generate evidence to inform and improve clinical practice and policy. 1 Advancements in health information technology provided new opportunities to swiftly and systematically gather large amounts of data about clinical practice, so that knowledge about the efficiency, effectiveness, and other aspects of healthcare could be quickly produced and applied. 2 While knowledge and evidence generation were once synonymous with the research enterprise, LHS frameworks now position the data gained from quality improvement, informatics, analytics, evaluation, and patient feedback as additional, crucial sources of knowledge alongside research to drive innovation and improve healthcare.3,4 By leveraging these sources of knowledge for dynamic and continuous learning, LHSs are expected to optimize the balance between health system costs and improved health outcomes, patient and family experience, and healthcare provider satisfaction. 5
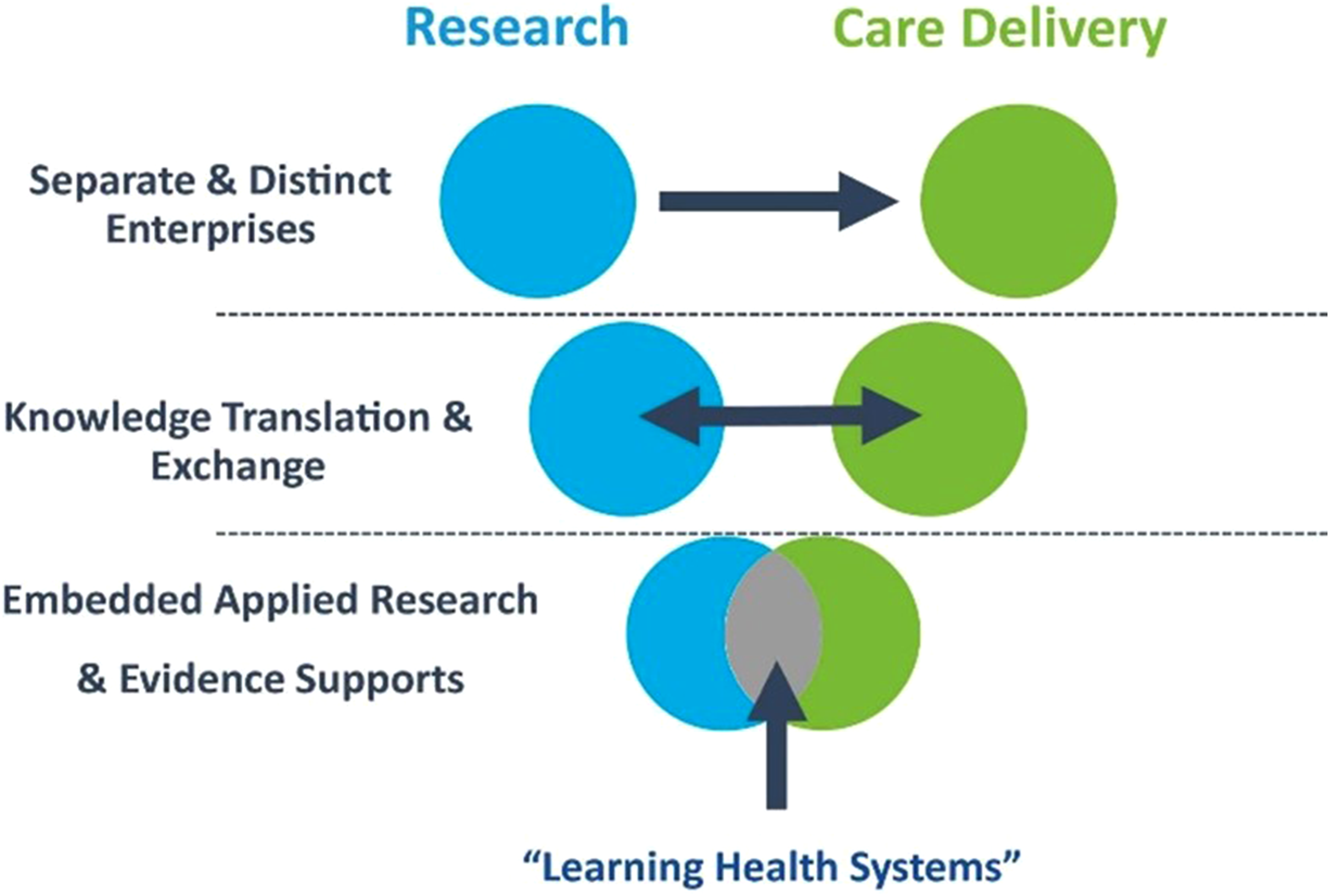
As LHS frameworks continue to expand to include more sources of knowledge and evidence, it is important to recognize the original role of research as a fundamental contributor to LHSs. While health data-derived insights can be more rapidly generated and integrated into healthcare delivery than traditional academic research, embedding applied research processes within the care setting is another important strategy to support LHSs (Figure 1).
3
Menear et al.
5
conceptualized LHSs at different system levels, with the smallest microsystem LHS centring on clinical units that deliver health and social services, and the individual patients and practitioners involved in that care. Healthcare organizations benefit when they leverage research to better understand the care experience at the individual patient level.
6
Thus, patient-oriented research and practice-based research are two embedded research processes occurring at that microsystem level that are integral to LHSs and are of recent focus in British Columbia (BC). Learning Health Systems sit at the intersection between research and healthcare delivery.
3
Patient-Oriented Research (POR) is health research that engages patients, caregivers, and family members as partners in the research process alongside clinicians and health system decision-makers, ensuring that inquiry focuses on patient-identified priorities, and ultimately leading to better patient outcomes. 7 Patients, as well as their caregivers and family members, through navigating and receiving care, experience and examine the healthcare system in a different way from health researchers or practitioners; they have firsthand knowledge of living with an illness or condition and accessing health services. Incorporating these insights and perspectives enhances the relevance of research, providing significant benefits to both the healthcare system and its patients. 8 For example, patients may identify important considerations for participant recruitment and retention, or check that qualitative interview guides are reflective of, and sensitive to, lived experience. As emphasized in theoretical LHS models grounded in POR, support for patient engagement is a key enabler of LHS capacity development. 9
Practice-Based Research (PBR) in healthcare is research that investigates clinical questions, in real-world settings, to inform clinical practice. 10 PBR is a systematic and scholarly endeavour 11 ; however, it is primarily initiated and led by healthcare professionals, those who hold an active role in patient care and service delivery, rather than academic or industry researchers. The power of PBR, in comparison to academic or industry research, is that its proximity to the clinical context facilitates its implementation to enhance evidence-based practice, patient care, and the healthcare system. In addition to identifying potential service or policy changes, PBR also supports the development of research literacy and leadership amongst clinicians, which are individual competencies that support LHSs. 12 Furthermore, a well-executed PBR project gathers together a learning community, which is a group of people with shared interests and appropriate experience to meaningfully collaborate to solve health and health system problems. 13 Learning communities are foundational structures for LHSs, 14 and so both PBR and POR can be important precursors to the creation of an LHS environment in and across health system organizations.
There are several BC healthcare organizations offering low-barrier internal funding programs to engage clinicians in PBR. These PBR programs have been evaluated and found to be important for improving clinicians’ research confidence and abilities, as well as enhancing their familiarity with evidence-based practice.15,16 Research projects supported by these programs encompass both quantitative and qualitative paradigms, as well as quality improvement and evaluation. Some projects have provided sufficient standalone evidence for changing clinical practice, while other projects have yielded foundational data to secure external grant funding for further research. Despite the similarities between these PBR programs, including the goal of improving the healthcare system through clinician and patient engagement in research, until recently, the work was conducted largely in isolation from other programs and with inconsistent integration of POR principles.
The BC Patient-Oriented Practice-based Research Collaboration (BC POPRC)
In June 2020, the British Columbia Support for People and Patient-Oriented Research and Trials Unit (BC SUPPORT Unit) brought together representatives from PBR programs and a patient partner advocate to form the BC Patient-Oriented Practice-based Research Collaboration period after collaboration. The BC POPRC was established as a community of practice for PBR programs to share knowledge, resources, and best practices for administering a research capacity-building initiative. 17 For example, BC POPRC members co-developed peer and patient approaches for reviewing PBR proposals and co-designed surveys for evaluating patient engagement, among other shared resources and tools. Consequently, it has afforded individual programs the opportunity to optimize their own structures and processes, and a pipeline for new member organizations to establish PBR programs. A quote from the lead for the most recent program to join the BC POPRC captures this: “We have launched our first Practice-based Research Challenge and hope to announce our funded teams in September! Thank you to everyone for your generosity in sharing your experience and resources to support us in getting to this point.” Representatives from each healthcare organization continue to meet regularly to discuss their PBR programs, collaborate on shared endeavours, and plan future directions for the BC POPRC.
The BC POPRC was also established to ensure POR principles and practices were consistently integrated into all PBR programs. To do so, the BC SUPPORT Unit formed the Patient Engagement in Research Collaborative (PERC) with Patient and Family Partner (PFP) representatives from each of the healthcare organizations, to ensure a robust patient-oriented lens is applied to all PBR activities undertaken by BC POPRC member organizations. PERC members contribute to ongoing POR support for PBR programs, including the development and implementation of a POR training curriculum, review of PBR proposals, as well as supporting clinicians to engage with PFPs on their PBR project teams. The PERC also serves as a parallel forum to the BC POPRC for PFPs to come together to share their experiences and best practices of supporting programs to achieve meaningful patient engagement in health research.
Positive outcomes of the BC POPRC
There are five member organizations of the BC POPRC that offer PBR programs within their own healthcare organization. Some member organizations have long been offering PBR programs (up to 14 years), while others began offering programs following creation of the provincial collaboration. Prior to 2020, POR practices at each member organization were not well established or tracked, if carried out at all. Since the BC POPRC was formed, each organization now offers POR training within their PBR programs, whether as workshops, direct one-on-one mentorship, or other modes of delivery, and strongly encourages teams to embed POR principles within their projects. Furthermore, all organizations now include a PFP on their PBR advisory committee and ensure all project proposals are reviewed by a trained PFP. Of the 88 PBR projects that have been funded across participating organizations since the creation of the BC POPRC, 77 (87.5%) have included a PFP on the project team itself.
In October 2024, a program survey was sent to all team leaders (n = 25) who have initiated and completed their PBR projects since the BC POPRC began offering POR training, to evaluate the experience of engaging PFPs. Team leaders across the member organizations are generally required to be point-of-care nursing and allied health professionals with majority or full-time clinical caseloads. Questions explored team leaders’ preparation to engage with PFPs, as well as PFP roles, contributions, and value for the PBR projects. Nineteen responses were received, though some surveys were incomplete (76% response rate). Notably, 84% of respondents felt that engagement with a PFP was valuable for their project. Many respondents (79%) felt their team was well prepared to engage with a PFP on their project, and 84% felt comfortable leading engagement with PFPs for future projects.
PFPs played a contributing role at all stages of the research cycle (Figure 2). More often, PFPs were involved as informants on research teams, participating in team meetings and supporting research decisions. Team leaders reported that PFPs were less often involved in research conduct activities, such as data collection. Most team leaders felt that adequate time was allocated for the PFPs to be fully engaged on the project, and that the PFP positively influenced the project activities. Team leaders also reported consistent sharing of project goals with PFPs, and that their teams were receptive to input from the PFPs. Expected patient and family partner roles on practice-based research projects (n = 19, respondents could select multiple options).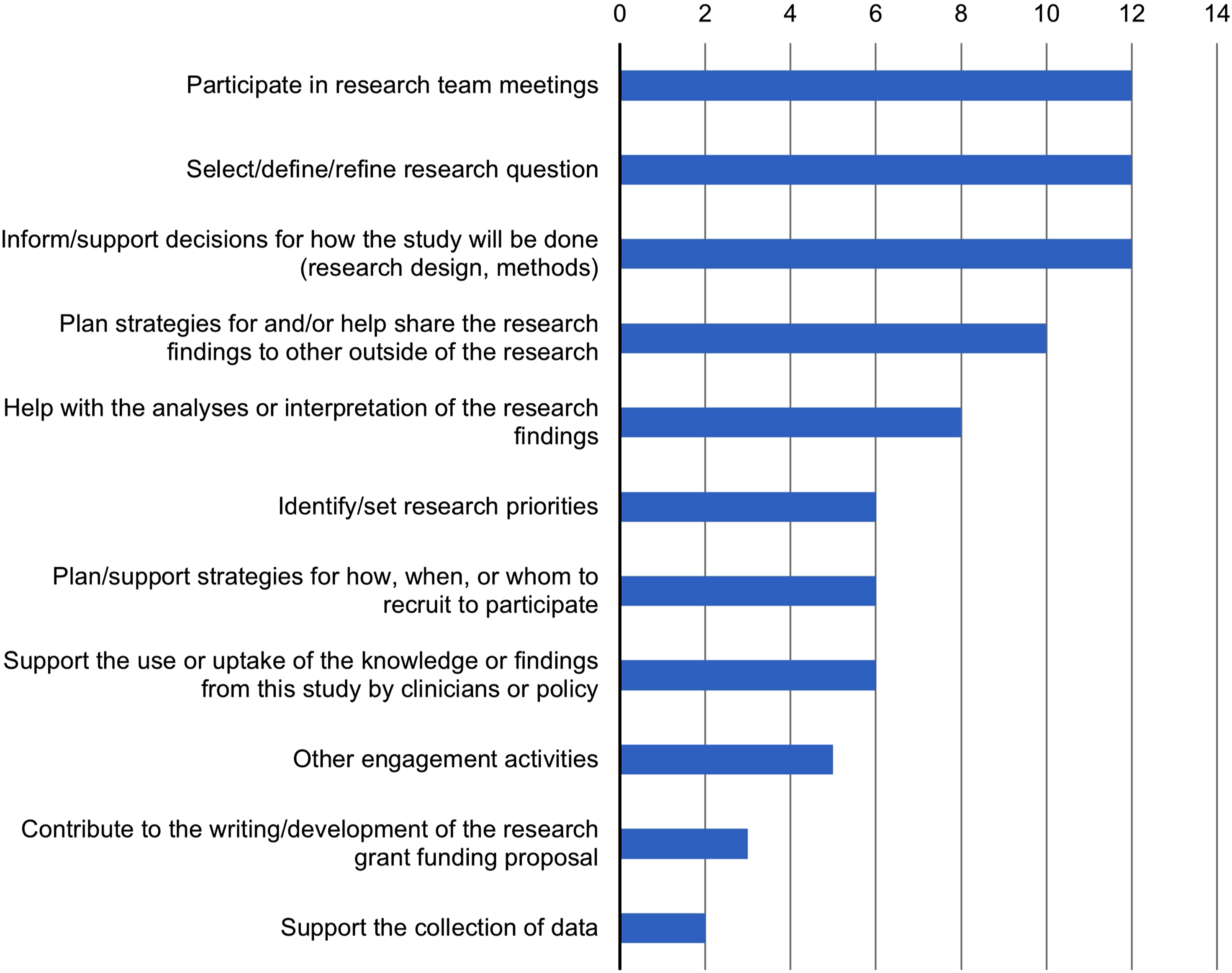
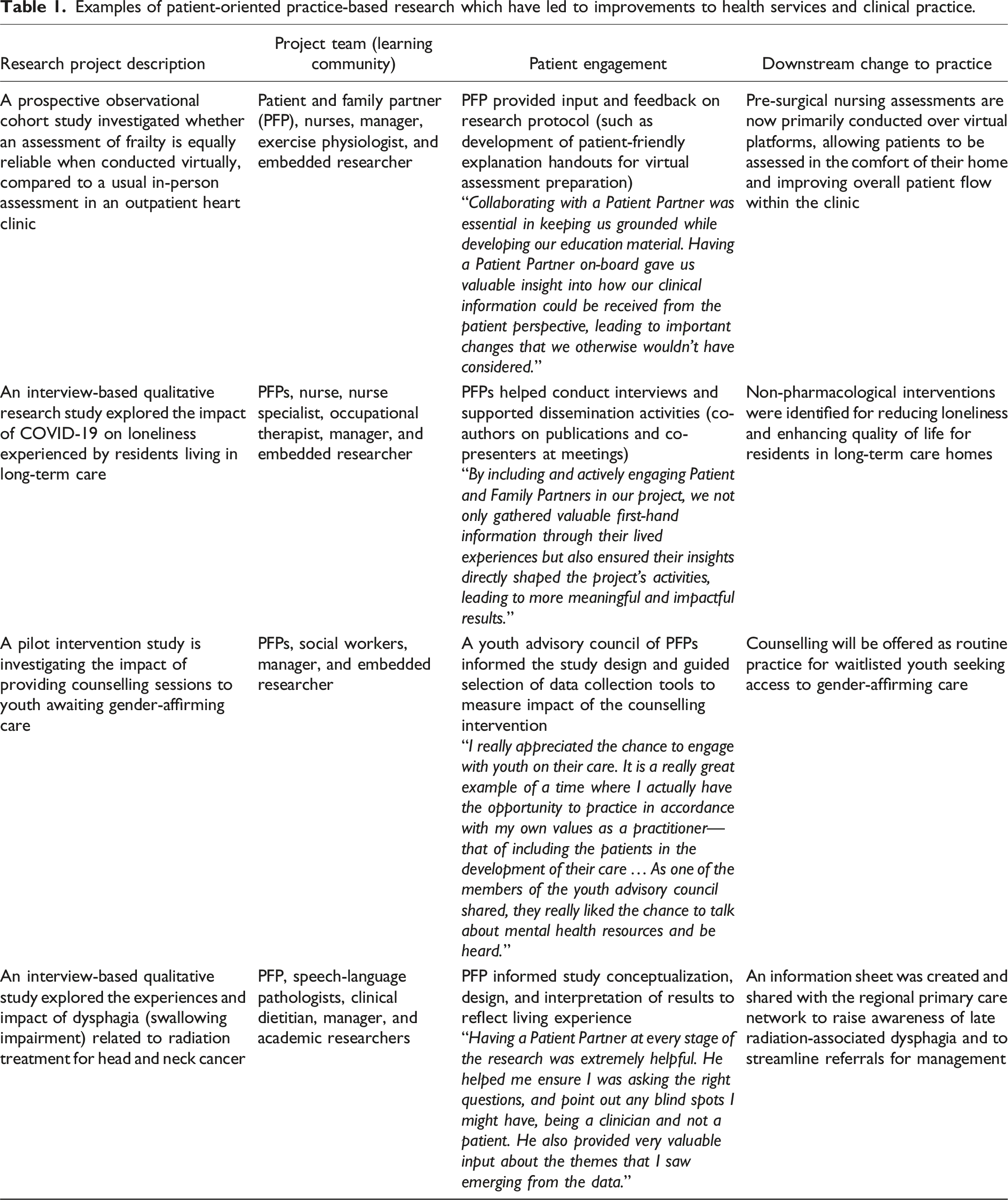
Examples of patient-oriented practice-based research which have led to improvements to health services and clinical practice.
Discussion
The BC POPRC is an example of a high-functioning and provincial capacity-building network, leveraging the synergies of individual members to support the creation of LHS environments. Establishing the BC POPRC has facilitated the initiation and completion of numerous clinician-led, patient-engaged projects within each member organizations. Provincial collaboration has also been instrumental in spreading this work at a much broader (meso-)level, functioning as a community of practice for reflection on best practices, advancing collective priorities like POR, and streamlining the development and launch of PBR programs for new member organizations. Furthermore, unifying the programs under the BC POPRC achieves several of the enablers identified by Strosher and colleagues 9 for LHS capacity development. By advancing POR training and ensuring patient engagement is paramount for PBR projects, the activities and mandate of the BC POPRC very clearly align with embedded research and patient engagement supports, accountability, and shared goals and priorities. Other accelerants offer guideposts for the collaboration’s efforts, such as health workforce engagement, securing adequate resourcing, and multi-level leadership support.3,9 For example, clinicians report a lack of time to engage in PBR, 15 and so promotional activities of the BC POPRC, such as research showcases, have advocated strongly for greater organizational and provincial support for patient-oriented PBR programs.
The collaboration will continue to work collectively to advance patient-oriented practice-based research—both in practice and in theory. Existing research has explored competencies of both POR and PBR,19,20 which can be leveraged for future development and refinement of standardized education pathways for clinicians and PFPs. Much like the difficulty in assessing the impact of LHSs, 21 a similar challenge was noted in summarizing the impact of PBR projects on a broader scale. The collaboration has recently obtained competitive funding to convene PFPs, researchers, decision-makers, and other interested informants from all regional health authorities in the province to co-design an equitable PBR impact evaluation framework, to be able to demonstrate value in achieving the Quintuple Aims 22 of improved health equity, patient experience and outcomes, clinician well-being, and health service efficiency. This work will include potential impacts on health human resource job satisfaction, retention, and recruitment, given that professional development activities like PBR programs align with recommended retention strategies in Canada. 23
Patient-oriented PBR programs offer health leaders a strategic opportunity to address several of the barriers to LHS operationalization, which include low buy-in, limited time and resources, and a lack of infrastructure to capture data. 24 In Harrison and Shortell’s multi-level framework to inform LHS research and practice, 6 middle manager and senior leaders are highlighted for the critical role they play in organizational learning, given that they are responsible for establishing and mediating strategic priorities, as well as providing the opportunities and resources for training. By empowering their point-of-care clinicians to lead embedded research through PBR programs, managers reduce their own burden as sole drivers of innovation, while also building LHS-supporting competencies amongst their team, such as evidence-based practice, teamwork, and analytical skills. 12 Furthermore, forming a learning community with patient partners and developing a culture of inquiry amongst staff are additional mechanisms of co-creation that support a continuous learning cycle of knowledge generation and practice change. 25
Conclusion
The BC POPRC is firmly established with five member organizations, which has created a provincial foundation to support learning across the health system. As a community of practice, it has co-developed, shared, and provided training, resources, and support among its members, as well as to prospective organizations seeking to develop their own PBR initiatives. The BC POPRC also embraces the concept of meaningful engagement with patient, family, and caregiver partners, ensuring that the embedded research it facilitates is driven by shared decision-making. Several priorities have been identified for future work, including creation of POR training resources and development of a framework for evaluating PBR impact. Leadership plays a pivotal role in developing and promoting a culture and climate supportive of learning. Health leaders in British Columbia are therefore called on to advocate for, develop, and sustain patient-oriented PBR programs within their organizations to help advance LHSs and their positive effects and are invited to collaborate with the BC POPRC to leverage its community and resources.
Footnotes
Acknowledgements
The authors wish to thank Rhonda Ellwyn, Sara Lima Branco, and the many other members of the BC Patient-Oriented Practice-based Research Collaboration (BC POPRC) and Patient Engagement in Research Collaborative (PERC), not only for supporting this article but also for the important work they do to enable meaningful practice-based research across the province.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The BC SUPPORT Unit is funded through the Canadian Institutes of Health Research (CIHR) – Strategy for Patient-Oriented Research (SPOR).
Ethical approval
Institutional review board approval was not required.
Data Availability Statement
Data from survey are available from corresponding author by request.