
Abstract
Primary care practitioners are optimally positioned to reduce the Greenhouse Gas (GHG) emissions produced by the healthcare system, which pose great risk to the health of people and the environment. This narrative review discusses 19 initiatives that can be implemented into primary care practices to reduce GHG emissions and financial costs through decreasing highly intensive emergency room visits and hospitalizations. This article also summarizes the time it may take for primary care practitioners to embed each of these initiatives into their care delivery. Lastly, this article demonstrates how best practice initiatives in primary care may show a higher GHG reduction than commonly conducted initiatives aimed at reducing GHGs.
Introduction
There is an inseparable link between health and the environment: diminished outdoor air quality depletes respiratory health, rising temperatures lead to and exacerbate severe and common chronic cardiovascular conditions, and the changing climate yields fatal vector-borne diseases.1-10 In addition, pollution disproportionately affects vulnerable populations; globally 92% of pollution-related deaths occur in minority and marginalized communities. 1 In Canada, family physicians are often the first point of contact for patients seeking care, and physicians face increasing and changing healthcare challenges related to the climate. 11 Primary care providers build lasting relationships with their patients, and act as key informants about their health, placing family physicians in an ideal position to initiate fundamental sustainable change.12,13
On a lifecycle basis, the Canadian healthcare system produced 33 million tons of Carbon Dioxide Equivalent (CO2e) between 2009 and 2015, which is equivalent to 4.6% of Canada’s national emissions, and is only estimated to grow. 14 While often overlooked, primary care and other clinical settings contribute heavily to growing pollution, with physicians and clinical services contributing 14% of the healthcare system’s total Greenhouse Gas (GHG) output. 14 A Swiss study found that an average primary care practice produces 30 tons of CO2e annually, which is equivalent to the annual electricity consumption of 20 average Canadian households.15,16 Through offering chronic disease management and helping patients avoid preventable emergencies and hospital admissions, primary care teams contribute significantly to decreasing the environmental burden of healthcare. 17 With its regular, direct, and frequent contact with patients, a sustainable and well-supported primary care system is fundamental to delivering equitable and low-carbon healthcare and reducing Emergency Room (ER) visits and hospitalizations.
While existing research suggests a multitude of plausible interventions aimed at improving care delivery, to our knowledge, the relative environmental impact of these interventions has not been quantified. In this study, we aim to quantify the reductions in GHGs, costs, and time resulting from implementing certain clinical practices that most physicians conduct daily such as minimizing unnecessary testing, reducing polypharmacy, and switching environmentally intensive medications to low emission alternatives of similar medical efficacy.12,18 We also describe the impact of interventions such as counselling patients on preventive care, social prescribing, dietary changes, and Advanced Care Planning (ACP).12,13,19 Given the link between health and environment, these interventions can achieve a profound impact on patient health and help alleviate some socioeconomic burdens for both attached (patients who have a regular family physician) and unattached patients. This study aims to educate physicians about the most impactful mitigation initiatives in their clinical practice and office. We argue that by strengthening the effort to incorporate the presented solutions into each independent family practice we can significantly decrease the environmental GHG impact in primary care, while providing effective and high-quality care to patients.
Methods
In this study, we conducted a narrative review as this methodology provided us with the flexibility and rigour to critically examine the entire literature available on the topic of sustainable initiatives in primary care. 20 The review identified key interventions that: (1) lead to improved patient health outcomes, (2) decrease hospital admissions, and (3) make the office more efficient. Data collected was supported with expert knowledge. We then calculated reduction of GHGs and cost (time and/or financial) it might take physicians to implement the initiatives. Detailed methods about each component of this approach are described below.
Intervention selection
We have used a modified PRISMA checklist to report on the key items in this narrative review. We conducted a search in the following databases to identify relevant studies: PubMed, Google Scholar, and grey literature sources including Google searches and professional organization websites. In areas where the published literature was scarce, we gathered data directly from consultations with family physicians from our working group to determine the decrease in GHGs, cost, or the effort it takes to implement the initiative. Included studies were limited to those conducted in Canada and countries with similar primary healthcare contexts. We searched the literature using the following terms: “GHG emissions,” “life cycle analysis,” and “carbon mitigation efforts” in primary healthcare settings. The study literature was collected between January 2024 and March 2025. There were no restrictions placed on the year of publication; however, among the included studies, the most recently available data was used for calculation purposes (e.g., the most updated version of a government report was used, even though previous versions were available and included in the selection process). We also did not limit the search based on study methodology used or type of publication. We hand-searched reference lists of included studies and supplemented this with expert consultations to help maximize the discovery of relevant papers and reports.
Papers were allocated into distinct thematic categories and used to calculate GHG emissions, time it takes to implement the initiative or cost associate with this action. The categories included in the final paper were grouped within the following a priori categories: (1) lead to improved patient health outcomes, (2) decrease hospital admissions, and (3) make the office more efficient. We selected the top items within each of the categories to be represented in the final graphical abstract. Expert review was used to maximize content validity. To do this, we developed a working group consisting of six family physicians from Ontario and Alberta and environmental sustainability researchers. All clinicians were from urban centres in Ontario, and we acknowledge that practices in other geographical regions may have other important contextual considerations. This may be considered a limitation of the study. Over the course of a year, we gathered data and met with group members individually to solidify our approach to data collection and analysis. After multiple rounds of review, we chose to focus on 19 distinct categories listed in Figure 1, which are supported by literature and practice. Initiatives include: adding a net new family physician, discussing advanced care planning with 10 patients annually, reducing prescription medications by 4%, promoting plant-rich eating, implementing social prescribing to address frailty in older adults, transitioning 10% of MDI users to DPIs, countering mis/disinformation through promotion of pneumovax, influenza, and COVID-19 vaccines, conducting up to 30% of visits virtually, encouraging active transport for patients, reducing OTC medications by 4%, switching to low-carbon banking, attending conferences virtually, using green energy providers such as Bullfrog, adopting LED lighting, using AI scribes to save 3 hours of administrative time per week, refusing products from carbon intensive suppliers, improving office efficiency to save 20 minutes per week, reducing 2% of unnecessary tests, reducing waste, reusing sharps containers, and recycling cardboard. This tree is adapted from an earlier illustration published in Healthcare Quarterly 25(3).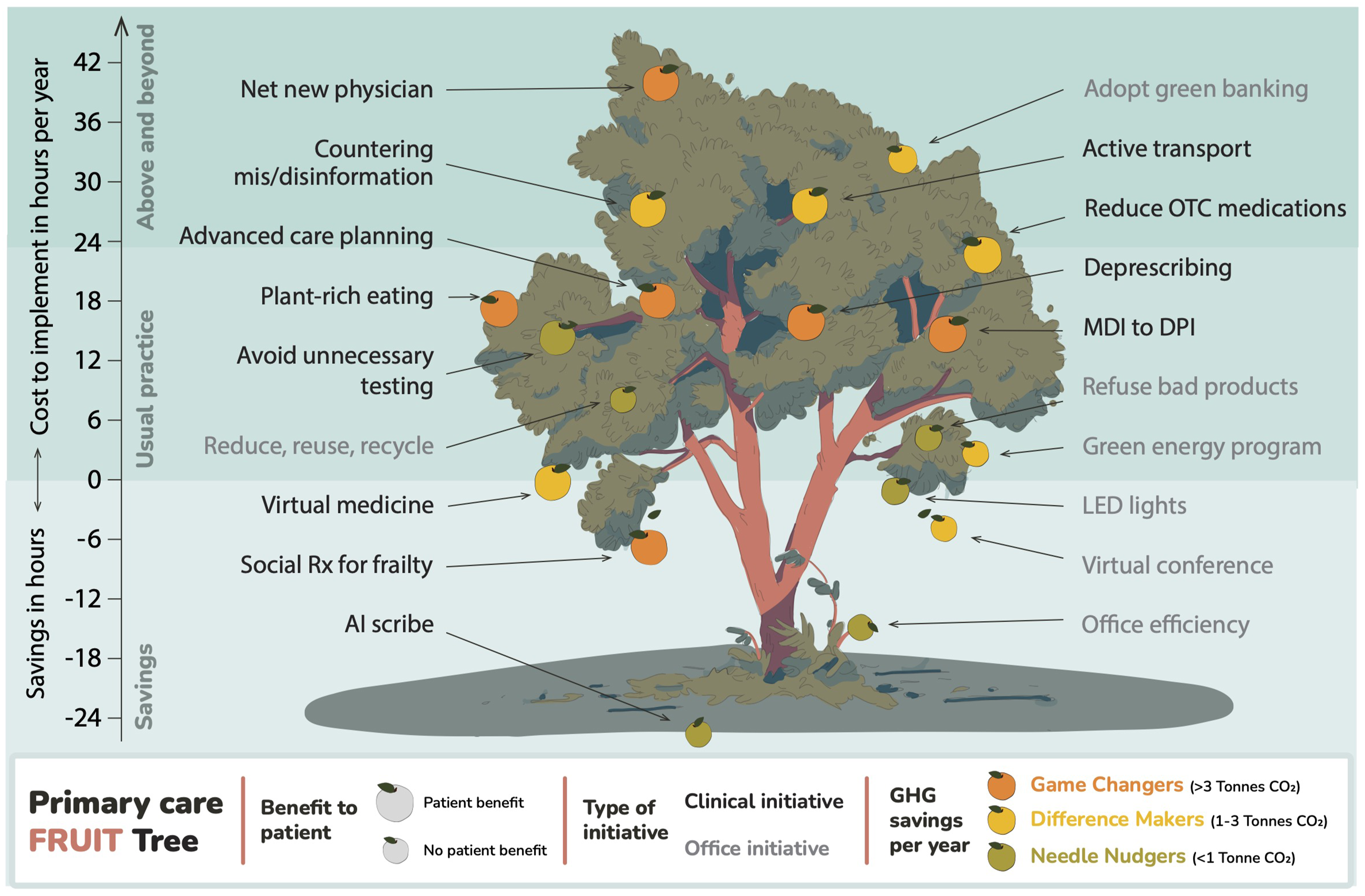
Calculations
We used a similar calculation method to the one used in the hospital iteration of the Peach Tree. 21 Values used in the analysis were extracted from the literature. When completing the GHG calculations, we broadly collected statistical information related to each of the chosen items from peer reviewed and grey literature. We applied our findings to a standardized format of a 3,600-patient primary care practice with three doctors taking on 1,200 patients each (which is considered a medium sized urban practice in Canada). To acknowledge uncertainties regarding the exact reduction of GHGs, cost, and amount of effort it may take to implement the initiatives, we present ranges along with establishing a set of assumptions based on literature, clinical experience from team members, and feedback surveyed from several family doctors across the country.
Results
In this article, we present a variety of “low-hanging fruits” which are quickly implementable, attainable initiatives that are specific to primary care and greatly support advancing environmental sustainability goals, while also providing high-quality healthcare.
21
Low-hanging fruits are simple but impactful actions that correspond to meaningful reductions in GHGs, financials, and time (Figure 1). Carbon emissions saved per initiative, per year.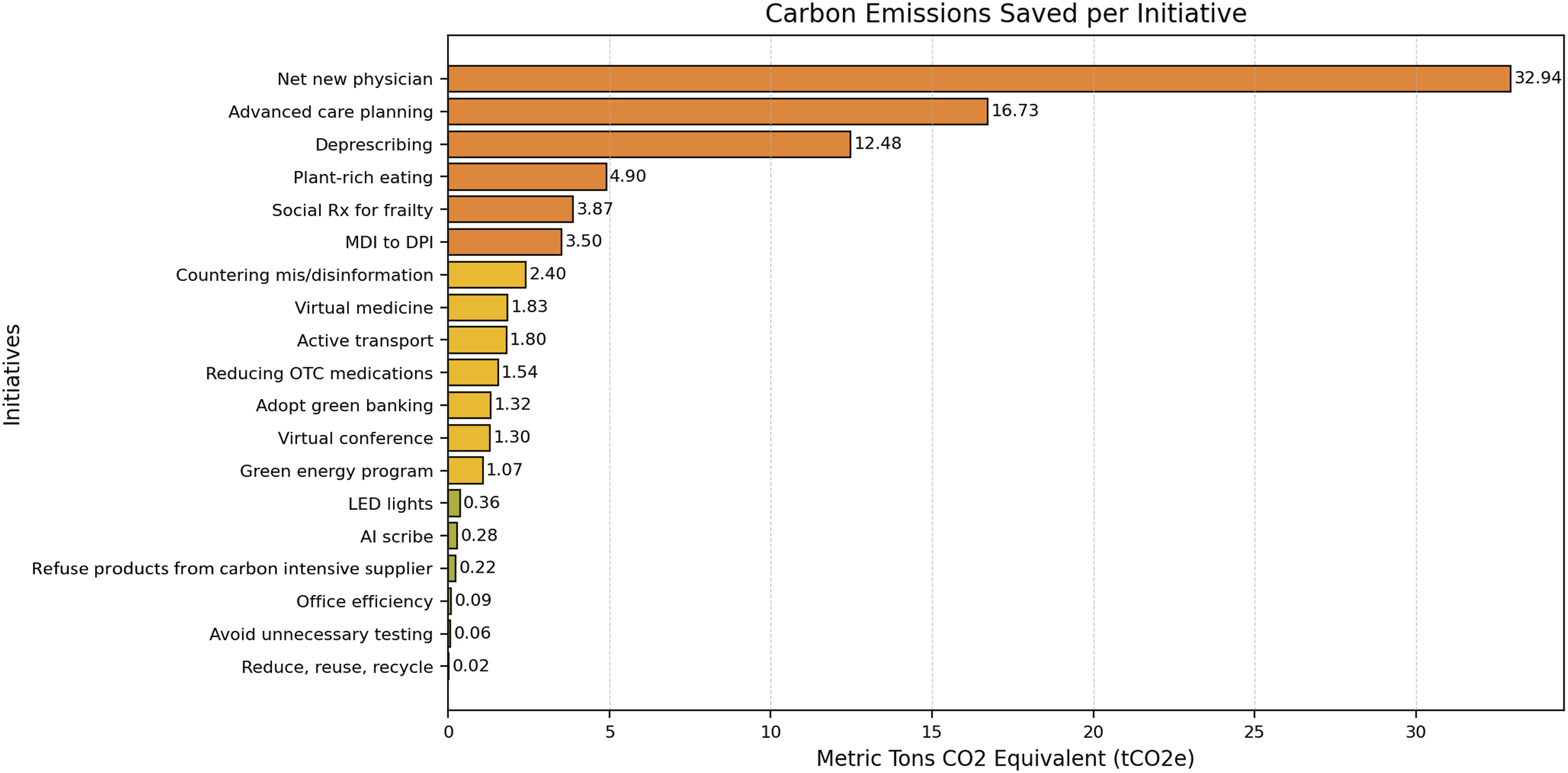
The advice we give
As family doctors well know, excellent patient care involves caring for the whole patient in their context. 22 This is also important for the environmental impact of care. Connecting patients with social services through social prescriptions can support better quality of life and mitigate demands on the healthcare system.23,24 For example, recent literature has found that loneliness is a very notable social determinant of health. 25 Alleviating loneliness in patients can significantly decrease repeat visits to doctors, and overuse of ERs and hospitals. We recommend using social prescriptions to help your patients, especially when working with vulnerable people such as elderly people.26,27
Primary care physicians are a key figure in delivering scientifically proven, valid health-related information to patients. Physicians have the power to inform their patients by countering mis/disinformation related to recommended vaccinations.28,29 Although the production of vaccinations has an environmental impact, the benefit of preventing serious and potentially life-long care far exceeds the cost of making the vaccines.29,30 Similarly, physicians can educate their patients on the value of balanced plant-rich eating using the “Canada Food Guide,” and where available, provide patients with monetary or social program support to help access fresh foods.31-34 Switching from a meat-heavy diet to a plant-rich/low-meat diet can lead to a significant decrease in personal GHGs and carries significant health benefits. Advocating for healthy eating is impactful.33,35-38
Finally, we suggest that physicians discuss the benefits of active transportation during the travel time your patients use to get to work or school. Active transportation can improve health and significantly decrease GHGs.39-41 When discussing transportation, it is important to consider the infrastructural context of the municipality where your practice is located. If the city supports active transport by providing bike lanes and pedestrian walkways, this may facilitate persuading your patients to choose active transport. We also encourage physicians to advocate locally for better active transportation infrastructure and protections.
Primary care physicians can greatly improve patient care through implementing Advanced Care Planning conversations, and this also significantly reduces the environmental impact of healthcare.42-44 At the End-of-Life (EOL), healthcare utilization significantly increases, and patients are often placed in hospitals rather than at home.45-47 Physicians should begin conversations regarding EOL decisions and goals of care when a patient experiences a hospitalization or receives a serious diagnosis. The physician can ask if the patient has an allocated decision maker who understands and respects their EOL goals to help avoid unnecessary hospitalizations, or medication use which can be contrary to the wishes of the patient. 48
Clinical practice
Family physicians take actions daily to make healthcare delivery more efficient, decrease costs, and serendipitously decrease GHGs. For example, arranging and managing home care services for patients and providing longitudinal comprehensive care that, in turn, reduces ER visits and hospital admissions, both reduce the environmental and financial strain on the healthcare system. We have included all of these under the category of finding a net new physician for your community. Our findings suggest that recruiting an additional family doctor into your community is the most impactful initiative. An additional family doctor within the system has the capacity to take on 1,200 patients and provide support in implementing all sustainable solutions listed on the tree into practice showing the fundamental role primary care physicians play in our society.
The appropriate use of clinical and diagnostic testing also requires consideration in terms of both value-based patient care and GHG emissions. Undertesting may delay diagnosis, ultimately increasing GHG associated with subsequent treatments, but over testing unnecessarily uses resources and may lead to false diagnoses. Best practice clinical decision making is grounded in scientific evidence, however it is not always possible, or wise, to strictly adhere to guidelines. For the past 11 years, CWC has helped family physicians learn how to safely reduce testing.49-51 The doctors in our working group already practice choosing wisely and did not feel that they could reduce testing much further without falling into a zone of undertesting.52,53 For our modelling, we chose not to look at each specific CWC primary care recommendation; rather, we looked at general MRIs, CT scans, and ultrasounds). Our working group concluded that a further reduction of testing by 4% was too aggressive and therefore used a reduction of 2%.
Similar to reducing tests, we acknowledge that physicians have also put significant effort into reducing the number of unnecessary prescriptions.54-56 One key example of this is switching patients, where appropriate, from metred dose inhalers to dry powder inhalers. 57 Deprescribing is an important climate mitigation strategy, as is counselling patients on the appropriate use of Over-the-Counter medications (OTCs). 58 Globally, OTCs, vitamins, and supplements are a multimillion-dollar industry and are openly available for consumption. 59 The journey of a pill from the extraction of resources, to the certification of ingredients in a lab, to the creation of the pill and shipment to distribution centres, results in a massive environmental impact. 60 Physicians have the power and expertise to educate patients on the negative effects of over-using OTCs and other unnecessary supplements. We acknowledge that completing a full review of non-prescribed medications takes significant time and effort. However, deprescribing OTCs is one of the simplest opportunities to improve long-term patient care through reducing harmful and/or unnecessary pharmaceuticals and significantly improving their environmental impact.61,62
Office management
Improved office efficiency can reduce the burden of organizational administration, including paperwork and Electronic Medical Record (EMR) inbox management, saving time.63-65 There are multiple organizational tools that can be used to run an efficient office. Data around Artificial Intelligence (AI) notetaking (such as AI scribes) suggests physicians can save 3 hours per week. 66 Saving valuable hours in the clinic can be used for providing additional care to patients or taking time off to improve physician wellness. We also examined the impact and challenges of implementing AI tools in clinical practice. 67 While concerns exist about the GHGs generated by AI use, the net time and energy savings for physicians using AI tools can lead to lower overall carbon emissions.68,69
Additionally, virtual medicine can overcome barriers to accessing care, reaching patients who may otherwise have foregone medical attention such as those who are home-bound, have mobility limitations, have social anxiety or who must travel long distances to the office.70-73 It also mitigates environmental costs associated with accessing care such as transportation. Embedding a half day of virtual medicine into your clinical flow leads to a reduction in GHGs and a reduction in the use of gasoline for patients.74-76 Hosting any building produces GHG emissions, so we recommend sharing your spaces with other clinicians and relocating your offices to blend with other practices. Attending conferences virtually rather than in person can also cut your GHG emissions.
Finally, each primary care clinic requires banking services to perform routine financial operations such as paying staff and bills within the clinic. We found that the choice of financial system has a significant environmental impact. We understand that making the decision to adopt green banking is difficult; however, big Canadian banks have a high carbon footprint, and supporting smaller, more sustainable banks, or credit unions can reduce your office’s GHG impact. 77
Office resources
There are multiple initiatives within your office space that you can adapt to improve its efficiency and reduce its carbon footprint. Primary care teams can make the choice to switch to green energy programs which guarantee the replacement of energy used to power the healthcare facility and services with more sustainable sources of energy. These programs vary by province, and one example is the Bullfrog Power program. 78 The subscription fees for green energy programs vary, but they lead to a shift towards using more sustainable energy sources.
The procurement of goods, office equipment, and other items can have a significant environmental impact. Consider local sustainable producers and vendors within your geographic area. In Hamilton, we have created a procurement guide listing some of the local sustainable suppliers within the area who are rated highly by sustainability evaluation programs such as the Science-based Targets Initiative.79,80 The commonly referred to “3 Rs”—reduce, reuse, recycle, are also on the tree. In our analysis, we quantify these items through three different case study examples from local clinics. For example, we looked at the impact of reducing the use of examination table paper and reusable sharps containers.81-89 While reusable gowns were discussed with our working group, they were not included in our final calculations as post-COVID gown usage in most family practice settings was felt to be minimal and unlikely to substantially impact emissions. Individual clinics should consider their own context when reusing equipment. We demonstrate the impact of recycling through the example of recycled cardboard. 90 Within your office, you can also embed systems that can program your screens, and lights to automatically shut off when not in use, and these systems can greatly reduce your bills and energy use. Although it may seem that the impact from reducing, reusing, and recycling is miniscule, our goal is to completely reduce unnecessary carbon use, meaning that every action counts.
Finally, utilizing light emitting diodes for lighting needs are an easy and implementable step towards greening your practice.91,92 This small change can lead to significant financial and energy savings over time, along with a significant reduction in GHGs.
Conclusion
The fruit tree for primary care highlights several high-value innovations that can be implemented in a primary care setting. Using this novel approach to evaluating sustainability initiatives in primary care, we consider the ability to reduce greenhouse gas emissions from emergency department visits and hospital admissions, which are known to have a significant carbon footprint. It is of critical importance that primary care clinicians and interprofessional primary care team members understand that the greatest opportunities to reduce greenhouse gas emissions from medical care require continuous and explicit attention to be paid to medication prescribing, vaccination, scientific vs. dis- information, advanced care planning, and healthy eating. Collectively, optimization in these realms can achieve a massive downstream reduction in carbon emissions from the health system. Although counselling patients about transitioning from MDIs to DPIs, or about safe over-the -counter medication use, are considered time consuming, they are also very impactful in terms of reducing greenhouse gases.
Strategic actions for leaders to promote environmental sustainability in primary care.
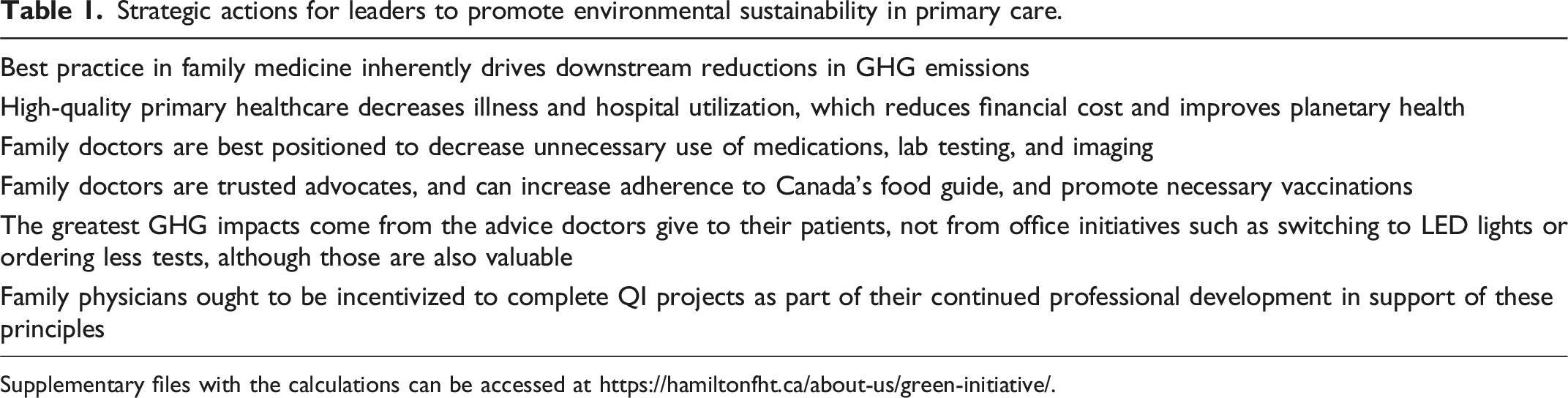
Supplementary files with the calculations can be accessed at https://hamiltonfht.ca/about-us/green-initiative/.
Footnotes
Acknowledgements
The original knowledge translation tree design concept was conceived by Myles Sergeant, original illustration by Aidan Lucas and editing by Sujane Kandasamy and Eric Cook for Longwoods. The design was re-adapted for primary care by Myles Sergeant, Elizaveta Zvereva, Danish Zahid and co-authors. We would like to extend our heartfelt acknowledgements to Evan Ferrari, Dr. Kathleen Ross, Dr. Grace Park, Dr. Caroline Laberge, Sonia Hsiung, and Karen Leiva for their feedback throughout the process of data collection. Thanks to Bhavna Samtani for designing the adapted fruit tree for primary care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study did not require ethical approval as it did not involve work with human or animal participants. The study involved the analysis of publicly available data and consultations with the working group.
Data availability statement
Assumptions and calculations for each initiative outlined in this study can be obtained from the corresponding author upon request.