
Abstract
This article describes the development of an organization-wide intervention to address moral distress in healthcare. A multidisciplinary team, including researchers and organizational partners, used intervention mapping and the theoretical domains framework to create the moral empowerment system for healthcare. This system encompasses a suite of strategies designed for integration into organizations’ operations to empower healthcare professionals individually and collectively to address moral events. This suite includes an ethics education program for healthcare professionals, interprofessional teams, and leaders; moral empowerment consultations; reflective debriefings; and mentoring. An implementation and evaluation plan is also presented, highlighting a staged approach that reflects the organizational context. Ultimately, the approach described here offers health leaders a practical and systematic method to design, implement, and evaluate moral distress interventions, tailoring them to their specific environments.
Introduction
Healthcare Professionals (HCPs) face ethically complex situations that can lead to a specific type of stress known as moral distress.1–8 Moral distress affects HCPs' well-being, leading to reduced patient care quality, burnout, job turnover, recruitment costs, decreased productivity, sick leaves, early retirements, and resignations.1,9–11 Consequently, addressing moral distress is crucial for retaining healthcare providers and mitigating the broader factors contributing to the global staffing shortage making it a key concern for health leaders and organizations.12–14
Identifying and implementing strategies to address moral distress remains challenging, with inconclusive evidence for effective interventions despite research advancements in the understanding of this phenomenon.15–17
A key factor impacting intervention effectiveness is whether they are designed and implemented in alignment with the real-world organizational context in which they will be deployed.18–20 Healthcare organizations are dynamic and complex, and successful intervention design and implementation require alignment with existing practices, processes, mindsets, and resources.18–20 These factors highlight the importance of designing interventions using an evidence-based, systematic, and context-sensitive methodology to ensure they are not only theoretically sound but also practically feasible and impactful in specific settings.20–22 To our knowledge, previous moral distress interventions have not been consistently designed using such an approach. 15
There are several methods available to develop organizational interventions.19,22–24 Specifically, the Intervention Mapping (IM) framework23,24 in combination with the theoretical domains framework25–27 provide a systematic and theory-driven approach that enhances the precision and real-world efficacy of interventions through thorough collaboration between researchers and organizational partners.
This article reports in detail the process of applying these frameworks to develop an organization-wide moral distress intervention, the Moral Empowerment System for Healthcare (MESH), offering a guide for researchers and health leaders aiming to tackle moral distress rigorously and collaboratively.
Methods
Setting
MESH was developed for Northern Health, a healthcare organization in British Columbia, Canada, serving approximately 300,000 people with over 10,000 employees across 18 hospitals, 25 long-term care facilities, 9 diagnostic, and treatment facilities, and community health services in 27 communities. 28
Team
MESH was designed collaboratively by a team of researchers, organization’s leaders, and experts in education, organizational development, and ethics. These individuals were project partners; therefore, research ethics approval was not required.
Theoretical frameworks
MESH was developed using the IM framework, a structured approach consisting of iterative steps.23,24 These steps include conducting a needs assessment to develop a thorough understanding of the problem and establish the intervention conceptual basis, setting specific objectives to address the identified needs as well as relevant change determinants or behavioural factors relevant to achieving the objectives, selecting theory-based, practical strategies to address those determinants, and developing an implementation and evaluation plan.23,24
The identification of behavioural change determinants was informed by the theoretical domains framework, 25 which categorizes factors influencing behaviour into essential domains, such as knowledge, beliefs, social influences, and environmental context to facilitate the identification of specific behaviours that need to be promoted to achieve the desired outcome.25–27
Rapid literature review and thematic analysis
To establish the conceptual basis for the intervention, a rapid literature review was conducted. 29 Peer-reviewed manuscripts from PubMed, Web of Science, Cochrane, and Scopus were reviewed and synthesized through a six-step thematic analysis process: data familiarization, coding key points, generating themes, reviewing themes, defining and naming themes, and finalizing the analysis. 30
Results
This section outlines the results of applying the IM steps leading to the development of MESH.
Step 1: Conceptual foundation
The intervention’s conceptual understanding includes three primary components.
Component A: Defining moral distress
Following Morley, 2019 31 moral distress was defined as the combination of three core elements: (1) the experience of a moral event, (2) the experience of “psychological distress,” and (3) a direct causal relation between (1) and (2). 31
This definition captures the essential characteristics of moral distress and, therefore, remains broad enough to encompass a wide range of moral events that HCPs encounter in organizational settings.31–37 These events include moral constraint, where individuals know the appropriate action but face external barriers, such as institutional policies or lack of support, or internal barriers like self-doubt and perceived powerlessness.31–37 Moral tension involves recognizing moral issues without addressing them, leading to internal struggles and unease.31–37 Moral conflict is characterized by disagreements over the right course of action, often influenced by power dynamics within a team or organization.31–37 Moral dilemmas arise when conflicting moral obligations cause significant distress, as fulfilling one obligation means violating another.31–37 Lastly, moral uncertainty occurs when the correct course of action is unclear, causing individuals to feel conflicted.31–37
Psychological distress, defined as discomfort from confronting challenging moral events, may manifest as frustration, anger, anxiety, guilt, decreased self-worth, depression, nightmares, and physical reactions like sweating, shaking, headaches, diarrhoea, and crying.38,39
Component B: Interventions to address moral distress
Various strategies have been proposed to address moral distress.15–17 Educational interventions offer instruction on recognizing and managing moral distress by developing coping strategies or applying ethical analysis and reasoning.40–47 Education based on ethics theory and professional standards has shown particularly promising results in addressing the symptoms and underlying causes of moral distress.16,46,47
Group reflective debriefings, often guided by medical leadership, 48 ethicists or trained team members,36,37,49–52 provide a space for HCPs to reflect on challenging cases, seek emotional support, and receive ethical guidance. Consultation services facilitate case discussions, clarify values, and support the development of action plans. 53
Personal reflective exercises and resiliency training support HCPs to process experiences and enhance coping strategies 54 while mindfulness-based stress reduction programs target HCPs emotional and physical well-being. 55
Although these interventions show potential, conclusions on their effectiveness remain limited because of methodological aspects such as small sample sizes, lack of control groups, and inconsistent use of validated measurement tools.15–17 Furthermore, often the rationale for how the specific strategy chosen relates to the context in which it will be implemented is not given except in the most general terms. 15
The current state of the literature then suggests that a universal solution to moral distress is difficult to identify. It is more likely that several types of strategies are required to address this complex phenomenon. 16 Furthermore, it is critical to align those strategies with organizational realities to ensure their relevance and, therefore, enhance their impact and sustainability.15,22
Component C: Moral empowerment
Some interventions have focused on empowering HCPs to address the causal relationship between moral events and psychological discomfort, instead of mitigating their psychological symptoms.41,43,53,56–61 Those interventions suggest that individuals who feel empowered to engage with moral events effectively experience less intense and less frequent episodes of moral distress.56–61 Thus, the effect of empowerment appears to counteract moral distress.56–61
Empowerment is a participatory process through which individuals and organizations gain efficacy and control over their environment.60,62–65 It involves two dimensions: psychological and structural. Psychological empowerment focuses on individuals and includes the cognitive, attitudinal, and behavioural processes that make them feel capable of carrying out tasks.62,64–68 Structural empowerment focuses on the organization’s systems, processes, social interactions, and hierarchies.64–68 Structural empowerment results in increased perceptions of psychological empowerment, which subsequently supports further development of structurally empowering conditions.63–69
The cognitive, attitudinal, and behavioural processes that psychologically empower HCPs to engage with moral events are referred to as ethical competence. 70 These include recognizing the moral dimensions of a situation; regulating associated emotions; and utilizing ethics knowledge to critically evaluate courses of action; making a value-based decision; acting on that decision71–73; and actively incorporating ethical values into their professional identities. 74 A lack of ethical competence can lead to moral distress,12,74–76 while its presence has been identified as a crucial factor in preventing and alleviating it.36,37,74–82
Structural empowerment refers to the conditions that enable employees to perform their roles effectively.62–65 Elements of structural empowerment that have been linked to moral distress include staffing patterns, resource availability, organizational policies, and institutional support.14,36,79,83,84 The organizational partners indicated that these elements were being addressed through workforce sustainability initiatives, which are part of the organization’s strategic planning and beyond this manuscript’s scope. Therefore, the team focused the intervention on interprofessional collaboration and leadership, which are crucial for creating the structural conditions necessary to effectively engage with moral events.60,62–65 By doing so, MESH was positioned as a significant complement to the organization’s overall strategic plan.
Interprofessional collaboration involves HCPs from various disciplines working together to achieve a shared goal,85–88 such as addressing a moral event.89–96 Achieving this goal requires interprofessional ethics competence, which builds on individual ethics competence and encompasses interpersonal skills (e.g., communication, integrating differing values and perspectives, engaging in collaborative decision-making, and managing power differentials).97,98
Leadership is the ability to inspire, influence, and guide others towards a common goal. 99 Leaders play a crucial role in creating and maintaining broader systemic structures that impact HCPs’ ability to engage with moral events. 100 Studies suggest that HCPs’ experiences of moral distress tend to increase when leaders lack transparency in decision-making, reactively instead of proactively address challenges, and fail to prioritize support, resources, and open dialogue opportunities.79,83,101–104 Conversely, enhancing leaders’ ethics competence fosters structural and psychological empowerment.101–104
Based on this conceptual understanding of moral distress informed by the practical realities of the organization, the intervention goal was to disrupt the relationship between moral events and psychological discomfort by empowering HCPs to engage with moral events through enhancement of ethics competence and the sustained provision of organizational support systems.
Step 2: Determinants of change, objectives and strategies
Determinants of change, objectives, and interventions.
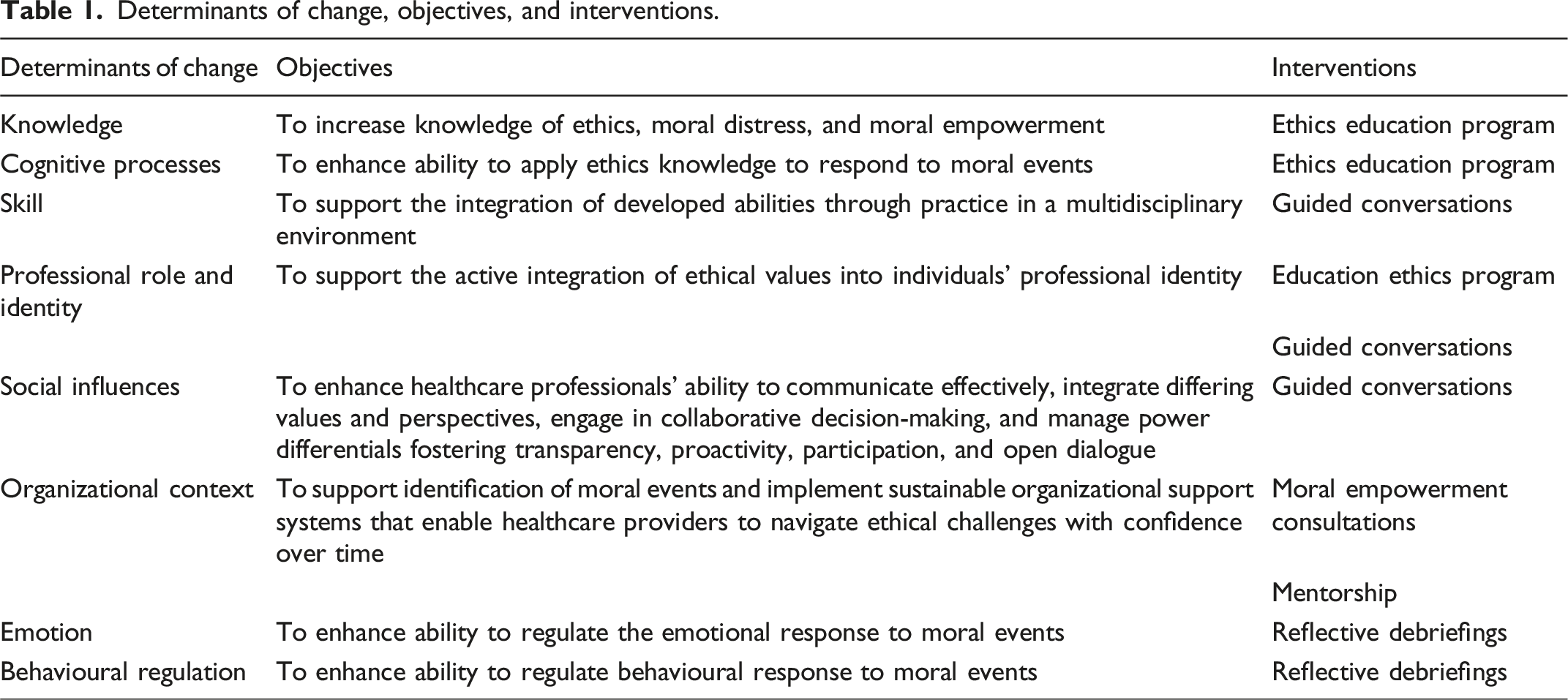
Specifically, the strategies identified were moral empowerment consultations, ethics education program, mentoring, and reflective debriefings, which together formed the intervention Moral Empowerment System for Healthcare or MESH.
To address the determinant of organizational context, a strategy involving moral empowerment consultations was selected. These consultations, led by healthcare ethicists, followed a structured process that included identifying the moral event causing psychological discomfort, uncovering underlying root causes, and brainstorming possible strategies to overcome these barriers. 52 The focus was on enhancing HCPs' moral agency and ethical decision-making skills, using the moral event as a catalyst for promoting systemic transformation.
On-line learning module topics.
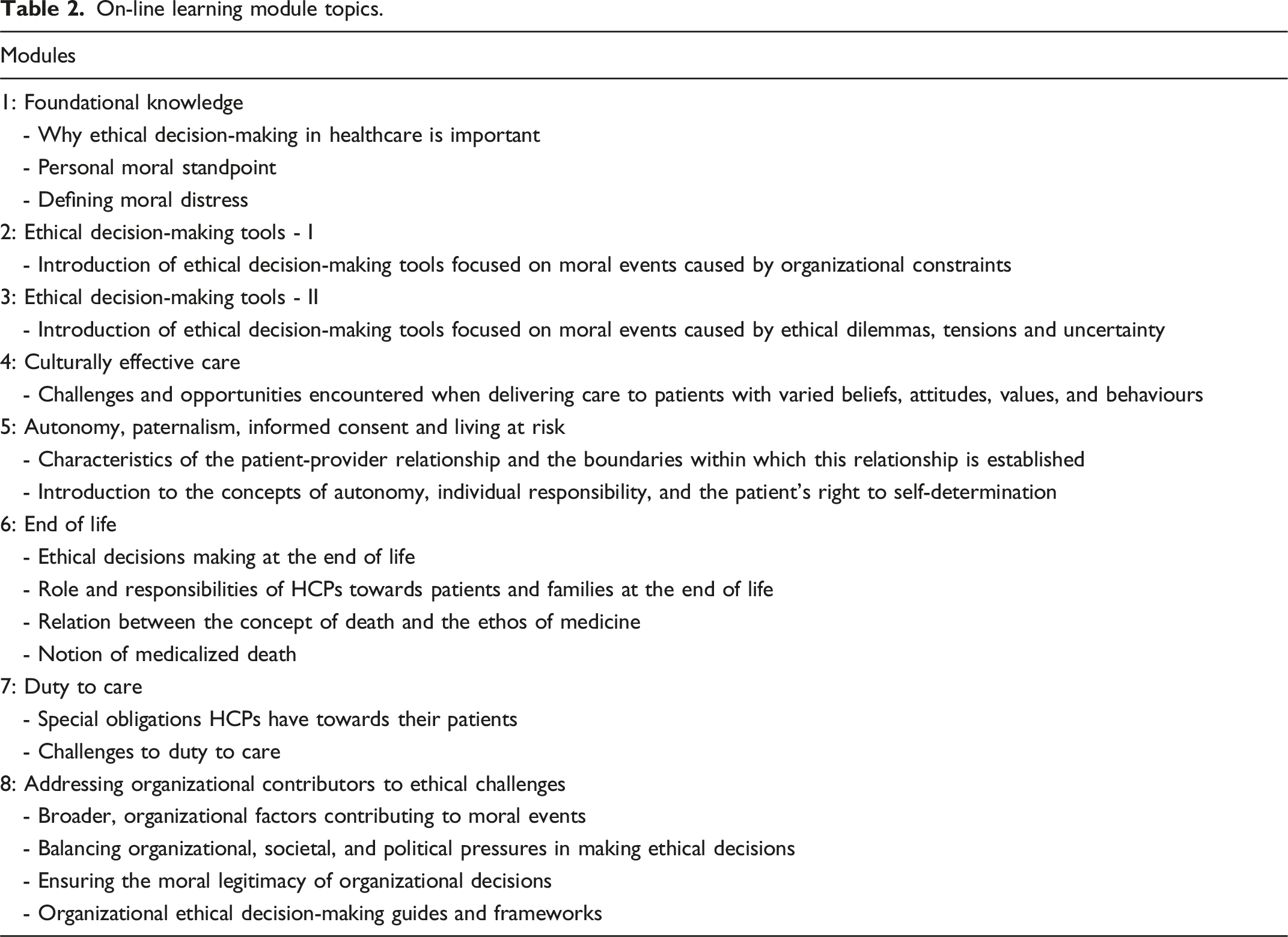
Guided conversations were the strategy chosen to address the determinants of skill, professional role and identity, and social influences. These conversations were organized as group-based training sessions in which participants, either interdisciplinary teams or leaders, applied the content of the modules in a collegial environment. These conversations, led by ethicists and organizational development consultants, integrated knowledge in ethics, change management, team dynamics, leadership, and conflict resolution. The conversations began with an overview of the module and proceed to apply it to the analysis of a moral event. Facilitators employed coaching techniques such as active listening, open-ended questioning, and reflective feedback to support engagement, promote self-reflection, and deepen understanding of ethical principles in practical contexts.
To address the determinant of organizational context, the strategy of mentorship was selected. This intervention provided support to HCPs who, after completing the education program, wished to serve as a resource for their colleagues. As such, this strategy created a sustainable support system to engage with moral events in daily practice. The mentorship program was led by an ethicist and included regular sessions to discuss mentors’ progress, challenges encountered, and best practices.
Reflective debriefings were selected to address the determinants of emotion and behavioural regulation. These debriefings focus on the emotional impact of moral events to prevent increased psychological distress and promote the ability to regulate emotions and behaviours in response to future events.36,37 Unlike consultations, they do not delve into the root causes of moral events but instead prioritize emotional processing. These debriefings were loosely structured, starting with broad questions followed by probing questions to encourage discussion and reflection.36,37 They were facilitated by an ethicist and a spiritual health practitioner.
Step 3: Developing an implementation and evaluation plan
The MESH implementation plan involved three stages. In stage 1, moral empowerment consultations were employed to address organizational causes of moral events in order to build trust, promote employees’ engagement and establish a foundation for the implementation of subsequent stages. These consultations were integrated as part of the continuous, organization-wide support resources available to staff.
Stage 2 included deploying the ethics education and mentorship programs to promote sustainable practices. They were made available gradually to interprofessional teams and leaders balancing organizational needs and resource availability. The education program lasted between 5 and 8 months while the mentorship program is provided on an ongoing basis.
Finally, stage three comprised reflective debriefings, which were also available to all staff members on an ongoing basis.
The MESH evaluation plan included surveys to assess HCPs’ perceptions of the quality and effectiveness of moral empowerment consultations, debriefings, and mentoring. It also included a pilot study specifically focused on evaluating the education program. This pilot study, which lasted 8 months, involved two frontline interdisciplinary teams and was evaluated using pre/post quantitative measures such as the Moral Distress for Healthcare Professionals (MMD-HP) 27-item questionnaire, 106 the Psychological Empowerment Scale, 107 and a self-report questionnaire developed by the researchers to assess perceived ethical competence levels. A midterm evaluation after five months showed increased confidence in addressing interpersonal and organizational causes of moral events, a stronger professional purpose, and better alignment with personal values. Teams also felt more confident handling moral issues together and experienced greater cohesion. Participants found ethical decision-making tools useful for explaining decisions, understanding others' perspectives, and managing emotional situations. 108 A full evaluation of all strategies will be published in future publications.
Discussion
This article presented the process of developing an evidence-informed, comprehensive, and organizationally integrated intervention, MESH, which includes a suite of strategies that work synergistically to enhance individual and collective ability to address moral events in healthcare organizations.
Two critical characteristics set MESH apart from other moral distress interventions. First, it was developed using the IM method in a collaborative approach between organizational leaders and researchers. This resulted in a contextually relevant prioritization of intervention objectives and change determinants that aligned with and complemented the organization’s strategic plan. Moreover, it led to the formulation of an adoption plan tailored to the organization’s needs and resource availability. Consequently, MESH’s potential to serve as a sustainable support system with enduring effects was enhanced.
Secondly, MESH focuses on moral empowerment rather than merely mitigating symptoms of moral distress. Consequently, MESH capitalizes on HCPs' agency to establish the structural conditions required for effective engagement with moral events and to foster systemic transformation.
Finally, MESH does not rely on one strategy but on several strategies ensuring that multiple aspects of moral distress and empowerment are addressed. These strategies are implemented through stages to ensure alignment with the unique needs, and resources of the organization, thereby enhancing MESH overall effectiveness and sustainability. However, it is important to recognize that other organizations aiming to implement a similar intervention to address moral distress may need to adopt a different approach based on their own specific circumstances and realities.
One potentially limiting aspect of MESH is its reliance on the organization’s willingness and ability to allocate the necessary resources. Allocating resources in any organization involves navigating a landscape of complex and potentially competing priorities. In the case of MESH and moral distress interventions more generally, leaders must carefully weigh the potential benefits of implementing innovative solutions that address urgent needs, against the risks of failure. This involves not only assessing the immediate costs and potential disruptions but also considering the long-term gains in staff well-being, retention, and quality of care. Ultimately, effective resource allocation for programs like MESH requires a forward-thinking approach, a willingness to take calculated risks, and a commitment to continuous evaluation and adjustment based on outcomes.
Conclusions
This article contributes to the moral distress research literature in two ways. It provides a detailed description of the process involved in developing an organization-wide moral distress intervention. This process relied on the IM approach supported by the Theoretical Domains Framework, ensuring a structured and evidence-informed method grounded in collaboration between researchers and organizations. By detailing this process, the article provides a replicable model for future similar interventions.
Additionally, the article presents the outcome of this development process: the MESH intervention. MESH’s comprehensive design, centred on moral empowerment and grounded in organizational realities, has the potential to maximize long-term benefits. Future research is needed to evaluate MESH’s broader impact and scalability across different healthcare environments.
Footnotes
Acknowledgements
The authors would like to acknowledge with respect and gratitude that this work was developed on the traditional, ancestral, and unceded territories of the diverse and vibrant First Nations of British Columbia, Canada. This includes, but is not limited to, the territories of the Coast Salish, Nlaka’pamux, Syilx, Secwepemc, Ktunaxa, Haida, Tsimshian, Nisga’a, Haisla, Gitxsan, Wet’suwet’en, Tahltan, Tlingit, Dakelh Carrier, Tse’khene Sekani, Dane-zaa, Nihew Cree, Saulteau, and Dene Peoples.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Collaboration for Health Research in Northern BC Seed Grant Funding supported by a tri-partite MOU with the Provincial Health Services Authority, Northern Health and the University of Northern BC.
Ethical approval
Ethical approval was not required.