
Abstract
Registered Dietitians (RDs) are essential professionals within Canadian Team-Based Primary Care (TBPC). RDs utilize practice competencies to ensure provision of high-quality care while working closely with other TBPC members. To fill in the gaps in the literature, the study’s objective was to explore RDs’ perception of their contributions to TBPC settings and their educational needs. This will help inform health leaders who manage interdisciplinary teams. A survey was distributed to Canadian TBPC RDs. They (n = 73) reported contributing to nutrition care for various populations, managing a large range of nutrition problems, and using competencies from multiple practice domains. Furthermore, they identified their need to enhance their knowledge about cultural safety within TBPC, as well as their interdisciplinary teams’ need to increase their awareness of the dietetic scope of practice. Identifying RDs’ contributions, competencies, and learning needs helps inform Canadian health leaders to improve care.
Introduction
Registered Dietitians (RDs) are essential healthcare providers in Team-Based Primary Care (TBPC). Their unique role as food and nutrition experts includes the provision of nutrition care to manage a wide range of nutrition-related issues for individuals of various ages and cultures, including, but not limited to malnutrition, for which they perform screening and provide treatment, and chronic disease management. In TBPC settings, dietitians work collaboratively alongside other healthcare professionals to optimize the quality and scope of care. If dietetic competencies and skill set are not well known by other TBPC professionals, the quality and effectiveness of care may become compromised.1-4 Further, to provide role clarification, exploring competencies specific to TBPC RDs is needed. By improving interdisciplinary healthcare providers’ understanding of TBPC RDs’ role, they will also be better able to make appropriate and timely patient referrals. In addition, identification of competencies required would assist in highlighting continued education strategies which would not only benefit RDs, but interdisciplinary teams as a whole.
In scientific literature, studies focusing on RDs practicing within TBPC settings, as well as studies surrounding dietetic educators revealed common themes in dietetic care such as interdisciplinary collaboration, 1 nutrition care and counselling,7,8 health promotion, 9 and communication.10-13 Additionally, themes such as equity diversity inclusion and accessibility competencies and advocacy resurfaced from grey literature as learning needs. 14 The literature also highlights professional development as a common strategy used to promote competent care practices, increase knowledge, and confidence for healthcare professionals.15-17 Yet, to date, there are gaps in the literature in identifying the perceptions of healthcare professionals, particularly RDs, towards their contributions in TBPC settings and their needs for further education. These areas are important to explore so that health leaders can be well informed, advocate for dietetic care, and ensure that interdisciplinarity is optimized in their TBPC.
The study’s objectives were to investigate RDs’ perspectives about their contributions in TBPC and their perceptions on areas of continuing education needs in order to guide health leaders to identify effective interdisciplinary education opportunities. This is in line with the aim of the Team Primary Care overarching project focusing on Interprofessional Dietitian Education for Team-Based Primary Healthcare, which was to identify key practice competencies and common nutrition-related health issues facing dietitians in primary care to better prepare dietitians for interprofessional collaborative team-based primary care in Canada.
15
Who classifies as a Registered Dietitian? Education: Bachelor’s or master’s degree in food and nutrition and practicum training
5
Dietetic Care: Registered Dietitians (RDs) are health professionals who use the Nutrition Care Process to provide care, which includes performing nutritional assessments, nutrition diagnosis, planning and implementation of nutrition interventions, and monitoring and evaluating nutritional status indicators. They also mentor dietetic students and interns, as well as provide nutrition education to the public and to interdisciplinary colleagues5,6 Competencies: The Integrated Competencies for Dietetic Education and Practice (ICDEP) identify a set of professional competencies that RDs must be able to continually meet in order to practice in Canada
6
Methods
To gain the perspectives of TBPC RDs across Canada, a bilingual (English and French) on-line national survey accessed via SurveyMonkey was created. Fifty-three multiple-choice and short-answer survey questions were developed based on competencies and contributions of RDs in TBPC, identified using a literature review. The literature search was performed using MeSH keywords and a search strategy in the Medline, Nursing and Allied Health, PsycINFO, and CINAHL databases with the support of a librarian. Articles found were imported in the Covidence software, screened independently by two researchers, and the key findings were summarized. Test re-test reliability was verified. The survey aimed to explore (1) the contributions of RDs including a list of acute and chronic nutrition-related health issues commonly encountered by RDs in TBPC, (2) key competencies needed for RDs to work in TBPC, and (3) perceived knowledge gaps and challenges facing RDs in TBPC settings. Both English and French versions of the survey were piloted for face and content validity with TBPC RDs.
The target audience for the survey was RDs working in a TBPC setting. Therefore, the survey was distributed in French and English via e-mail through Dietitians of Canada networks, TBPC centres, conferences, and social media platforms. In terms of distribution methods, multiple avenues were used, such as a promotional poster including a QR code which was distributed through social media platforms such as Facebook, dietitian support groups, Dietitians of Canada, Primary Care Dietitian Association, Association of Family Health Teams of Ontario, Dietetic Educator Leadership Forum of Ontario, Canadian Association of Professional Programs in Human Nutrition, and the Eastern Network of Dietetic Educators. The survey took 20-30 minutes to complete. Quantitative data were analyzed using descriptive statistics including frequencies, means, medians, and standard deviations. Although the exact number of TBPC RDs in Canada is not known, the response rate was estimated to be about 10.0% in Ontario, and less in other provinces. Using the text of the participants’ answers to open-ended survey questions compiled into an Excel document, a thematic content analysis approach was utilized to deductively and inductively discover themes. An initial code book was determined based on findings from the literature to guide the beginning of the analysis using a deductive approach, then new emerging themes discovered inductively while analyzing the data were added into the code book. Two researchers analyzed the data independently. They then met to discuss their coding, and discrepancies were solved to reach consensus. A third researcher was involved in the discussion to help reach an agreement when consensus could not be reached between the two researchers. The code book was updated. The percentage of agreement between the coding of the two researchers was over 95%. This was a multistep process including line-by-line analysis to understand context, applying codes meaningful segments, and then grouping codes into themes. Thematic saturation was reached during the coding. Supporting citations from study participants were selected to illustrate themes.
Participants’ inclusion criteria included either dietitians currently registered under their provincial college who were currently or had previous experience, working in a TBPC setting in Canada. All participants included were able to read and write in English or French. Registered dietitians with no work experience in a TBPC setting were excluded from the study.
Results
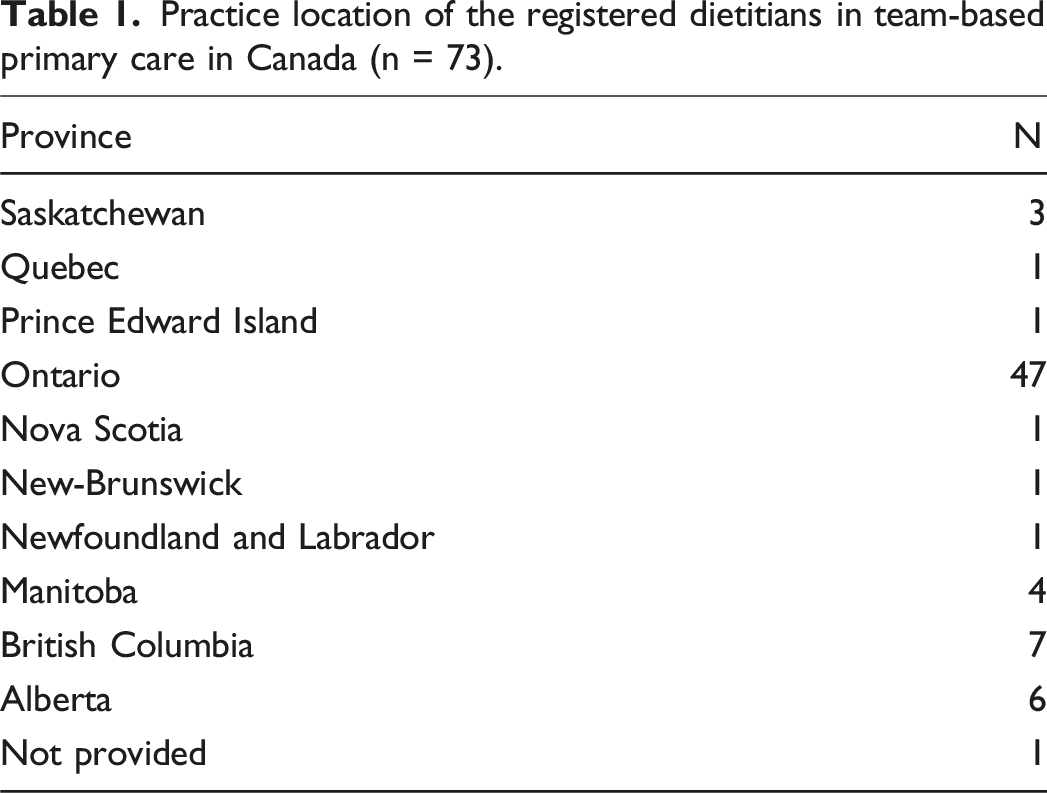
Demographic profile of participants
Practice location of the registered dietitians in team-based primary care in Canada (n = 73).
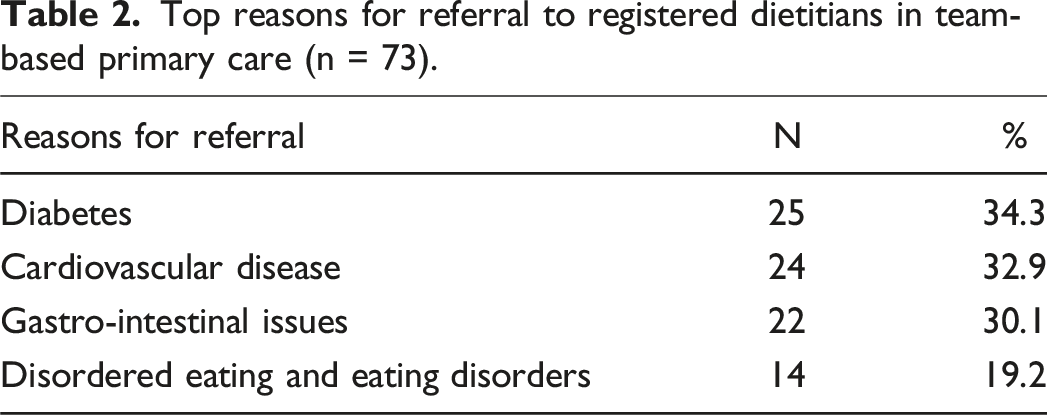
Contributions of registered dietitians in team-based primary care
Top reasons for referral to registered dietitians in team-based primary care (n = 73).
Interprofessional collaboration
Perspectives of registered dietitians on the importance of communication and the dietetic scope of practice (n = 73).
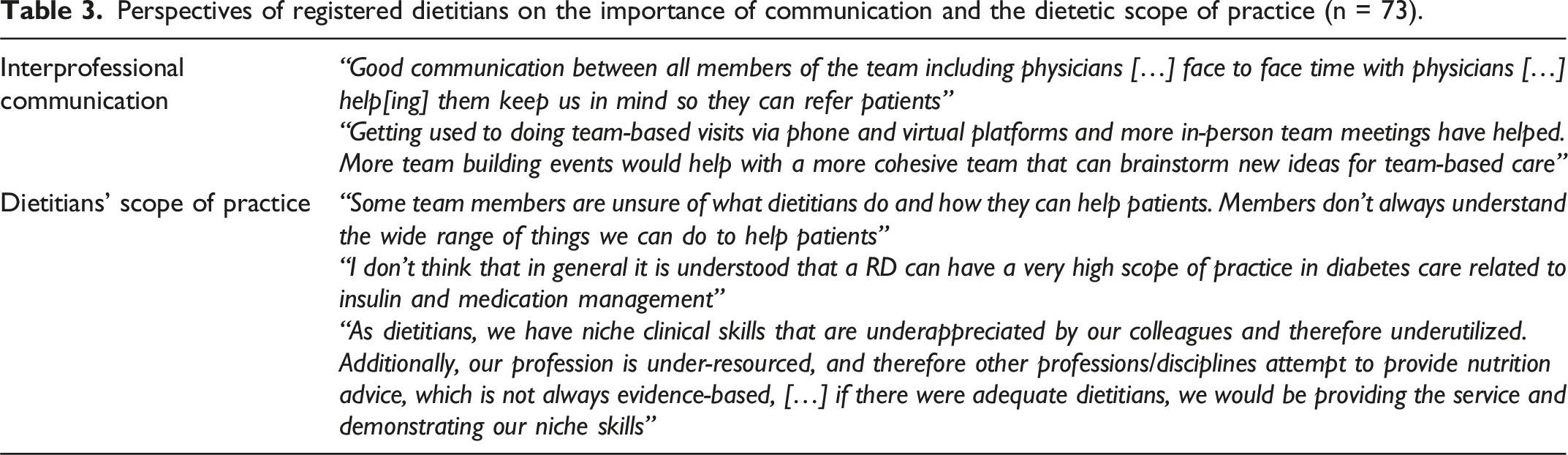
Moreover, most respondents (95.9%) agreed that team meetings facilitated communication among different disciplines when working in TBPC settings. Respondents identified the nutrition cases where they were more likely to work with other team members as being disordered eating and eating disorders (71.2%), mental health concerns (e.g., depression, substance use, and nutrition support) (68.5%), diabetes (64.4%), and cardiovascular disease (39.7%). Interprofessional competencies identified as being most challenging to implement within TBPC setting included: role clarification and negotiation (45.2%) and team disagreement processing (39.7%). In addition, only 50.7% of respondents felt that other professionals understand RDs’ scope of practice, and 58.9% felt that RDs’ role is well understood within TBPC settings. This reflects participants’ comments found in Table 3 regarding this issue. Yet, 83.6% of respondents agreed that they understood other interdisciplinary team-member roles and they felt effective as a team member.
Team-based primary care learning needs identified by participants
Regarding participants’ perception of learning needs in TBPC, results were wide ranging. Topics requiring further education that impact other members of the TBPC team included those related to interdisciplinary collaboration, including team disagreement processing (68.5%), role clarification and negotiation (38.4%), and collaborative relationship-focused care and services (34.3%). Practice competencies for which they would need more education included practicing in a manner that promotes cultural safety (50.7%), fostering development of food literacy in others (50.7%), and using risk management approaches (46.6%). All these issues are possibly true for many of the TBPC team members.
Participants also reported the need to enhance their practical competencies in specific dietetic areas, such as disordered eating and eating disorders (58.9%), mental health concerns (43.8%), and bariatric nutrition support (42.5%). In addition, they identified continuing education needs related to topics such as cultural safety (61.6%), nutrition care process and medical nutrition therapy (46.6%) and navigating the primary healthcare system (46.6%). Interestingly, 75.3% of respondents sought out their own learning opportunities after completion of their formal education to achieve competency levels that support their primary patient demographic.
Discussion
This study highlights the significant contributions of RDs within TBPC teams. Among their contributions to patient care within TBPC include the ability to manage the nutritional components of a very wide range of health issues. Since they deal with such a variety of health and nutrition issues, it emphasizes the need for continuing education for RDs to maintain their level of expertise. Since RDs work with many health professionals in a variety of settings, it is significant that they identified interprofessional collaboration as an important contribution as well. This enhances the exchange of knowledge between professionals, particularly in terms of understanding the roles of team members. 15 Applying theoretical frameworks like interprofessional collaboration and cultural safety in TBPC highlights practical challenges, such as the limited understanding of RDs’ roles by other professionals, which necessitate refining and expanding theoretical models to address real-world complexities. Currently, mechanisms that ensure theoretical advancements are translated into practice include continuing education, awareness of the RD role through interdisciplinary training, and knowledge-sharing platforms, all which play a critical role in bridging the gap between theoretical understanding and practical implementation.
Continuing education
RDs expressed the need for ongoing education related to the functioning of the TBPC team, including team disagreement processing and collaborative relationship-focused care and services. They also highlighted. Among the diversity of insightful results obtained, two issues arose which should be prioritized and addressed in the continuing education of the team.
Awareness of the RD role
Interprofessional training and collaboration are key elements in quality patient-centred care delivery. Interestingly, only 50.7% of respondents agreed that other professionals understand RDs’ scope of practice in TBPC setting. This demonstrates a significant barrier which prevents RDs from serving as an integral part in the healthcare team. This can result in reduced rates of referrals and hinder collaborative approaches to patient care.
The literature underscores that the RDs’ role in interdisciplinary TBPC settings can improve patient-centred care and increase skills and knowledge on nutrition of TBPC colleagues as well as contribute to more efficient teamwork.17-19 Considering that 83.6% of respondents reported that they have an understanding of other interdisciplinary team-member’s roles, health leaders should work to ensure that the same level of awareness is reciprocated towards dietetic care. Engaging in interprofessional education enhances collaborative skills and communication with other healthcare professionals, leading to improved patient outcomes. 20 It is considered a vital pedagogical approach in healthcare education, equipping healthcare professionals, including RDs, to deliver safe, high-quality patient care. 21 Therefore, healthcare managers should advocate for dietetic care through continued interdisciplinary education in TBPC.
Cultural safety
Health leaders and educators play a significant role in integrating theory into practice by fostering environments where principles like cultural humility and equity are consistently applied and where practical insights are used to inform academic and professional discourse. This approach encourages a deeper understanding of how the integration of theory and practice shapes not only immediate outcomes but also the broader trajectory of professional growth and system-level improvements. When asked about continued education needs, in this study, 61.6% of participants identified cultural safety as an emerging topic of interest. This concept has been explored on an international level 22 in dietetics and other health professions. Of note, this is one of the very few Canadian studies targeting TBPC dietitians that have explored this topic.
Cultural safety is a crucial concept in healthcare education. It involves creating an environment where practitioners can recognize power imbalances, systemic racism, and biases that may impact their practice with clients from diverse cultural backgrounds. 23 Cultural safety education can prepare caregivers to deliver care that respects and responds to the cultural needs of individuals, promoting inclusivity and equity in healthcare settings, and is also an important part of all staff’s responsibility to practice ethically, safely, and competently.24,25
When providing individualized, equitable care, RDs should feel competent giving nutrition recommendations that take into consideration various cultural practices, norms and beliefs. A high percentage (75.3%) of respondents reported seeking out their own learning opportunities after completion of their formal education. This shows the willingness for RDs to improve their quality of care, as well as their ability to self-identify gaps in knowledge and be self-directed to address those areas of need. This emphasizes the importance for health leaders and managers to identify and address barriers and knowledge gaps in cultural safety strategies, particularly for TBPC. It highlights the importance of creating opportunities not only for RDs, but healthcare professionals as a whole to engage in continuing education opportunities based on identified learning needs.
Study limitations
This study is not without limitations. Forty-seven out of 73 respondents were from the province of Ontario. Although Ontario is the most populated province in the country, 26 it would have been valuable to collect more data from a larger sample size, across all Canadian provinces and territories. This would allow for a broader and more comprehensive understanding of the RDs role in divers TBPC settings (e.g., rural areas and northern regions).
Nonetheless, this study is one of the few addressing the perspectives of RDs within TBPC setting in Canada. The fact that the survey was distributed in both French and English allowed the researchers to target RDs from both official Canadian languages. Additionally, the survey was created in collaboration with a group of RDs working in various TBPC settings as well as dietetic educators, allowing for expertise and relevant perspectives. The survey was able to target RDs with a variety of patient populations and a wide range of referral reasons.
Furthermore, by being part of the Team Primary Care overarching project, this project gained from being supported by primary care principles, interprofessional collaboration with multiple other disciplines’ national networking and projects, the insights from TBPC settings, and the equity, diversity, inclusion, and accessibility cross-cutting project part of Team Primary Care. 15
Conclusion
The survey results underscore the impactful role RDs play in TBPCs in managing the nutritional aspects of diverse health issues and contribute to interprofessional collaborations that support quality patient care. The findings identify a strong desire among RDs for continued professional development, particularly in areas such as cultural safety, team dynamics, and advanced dietetic competencies. This willingness to seek out learning opportunities demonstrates their commitment to providing equitable, high-quality care and addressing the diverse needs of Canada’s population. To address these challenges, health leaders should prioritize targeted interdisciplinary education, focusing on role clarification, team collaboration, and culturally safe practices. By doing so, they can support RDs in overcoming systemic barriers and empower them to further enhance their contributions to TBPC.
However, the study also highlighted critical challenges, including limited understanding of RDs’ scope of practice by other professionals and the need for enhanced cultural safety education, which serve as barriers for RDs to maximizing their impact within TBPC settings. Additional concerns include optimizing opportunities for dietetic input and interdisciplinary team collaboration. RDs provide care for a wide range of clients with various health and nutrition issues and work in diverse environments alongside other TBPC team members. These conclusions could also generally apply to other TBPC team structures and care situations, particularly in the areas of interprofessional role clarification and scope of practice understanding.
RDs expressed confidence in their ability to meet essential competencies for their profession based on the competency frameworks which guide their practice. To further support full use of the practice competencies, interprofessional education will raise awareness of RDs contributions within interprofessional teams but also enhance team functioning and patient care. Therefore, health leaders should focus on continued interdisciplinary education, as it is essential for bridging knowledge-practice gaps, and fostering collaborative care.
Ultimately, this study not only identified the education and practice needs of RDs but also highlighted the importance of fostering an environment that supports collaborative and culturally competent care. Advice for health leaders includes supporting TBPC RDs’ through role clarification and integration of their nutritional expertise. Understanding their unique contributions to healthcare teams will improve interprofessional collaboration, patient health outcomes, timely access to quality care, and improve disease management. Researchers, educators, health leaders and leaders should continue working alongside RDs in TBPC settings to implement and test educational interventions designed to address these identified needs, along with developing and utilizing knowledge and performance measurement tools to evaluate their effectiveness. Addressing these gaps will strengthen interdisciplinary teamwork, improve patient outcomes, and ensure that the role of RDs is fully integrated and recognized within TBPC settings. These efforts are essential for advancing the quality and effectiveness of primary care across Canada.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: Team Primary Care was supported by Employment and Social Development Canada through a grant to the Foundation for Advancing Family Medicine, co-lead by the College of Family Physicians of Canada and the Canadian Health Workforce Network (Workplace Integrated Demonstration Project Grant).
Ethical approval
The research study was approved by the University of Ottawa’s Research Ethics Board, certificate number H-07-23-9472.
Consent to participate
All participants provided written informed consent to participate.
Consent for publication
Written informed consent for publication was provided by participants.