
Abstract
Paramedics and Palliative Care is an example of a promising practice (“pilot”) that underwent successful spread and scale across Canada. Through the support of two pan-Canadian health organizations and concurrent evolution of the profession of paramedicine, this innovation has become integrated into practice. Evaluation of the innovation sites showed positive impact in all elements of the Quintuple Aim, and data from the expansion sites mirrors this success. Paramedic comfort and confidence is improved. Patient and family satisfaction is high. Quality indicators such as time spent at home, and home deaths, improved after program launch. There are time and cost savings with the program in place. The framework that enabled this spread and scale is presented and elaborated, to support further uptake of this innovation and provide a blueprint for successful expansion of other promising practices to support healthcare improvement across Canada.
Introduction
The spread and scale of healthcare innovations is often limited because great ideas fade away after their local pilot comes to an end. The Paramedics Providing Palliative Care at Home/Assess Treat and Refer program (the Program) provides an example of a local innovation that has become successfully embedded into practice on a pan-Canadian level, through a partnership that leveraged the experience of early innovators and catalyzed concurrent change. Demonstrated positive impact in the innovation and expansion sites through all elements of the Quintuple Aim should spur other Canadian and international jurisdictions to adopt the Program. Breaking down silos between paramedicine and other components of the healthcare system, as well as professional evolution of paramedicine, presents opportunities for other novel collaborations. The roadmap for this change is presented and provides a useful model for the spread and scale of other promising innovations.
The innovation: Embedding a palliative care approach into paramedicine
The Program was developed and implemented initially in Nova Scotia (NS), Prince Edward Island (PEI), and Alberta (AB) between 2010 and 2014, to better align paramedic services with the needs of people receiving palliative care in the community. 1 The Program includes three elements: (1) the development of a clinical practice guideline specific to palliative care that allowed paramedics to provide treatment in the home without automatic transport to the Emergency Department (ED), a major shift in practice; (2) education on a palliative approach, which was novel to paramedic practice; and (3) a database/mechanism to make patient goals of care accessible to paramedics. Communication between paramedic services and palliative care/usual care providers before and after the 9-1-1 call was a key component. Overall, the breaking down of silos between providers all serving the same population underpins this model of care.
Canadian collaboration to support and accelerate spread and scale
Between 2010 and 2017, the Canadian Partnership Against Cancer (the Partnership) supported the implementation of the Program in NS and PEI, and in 2016, NS, PEI, and AB (the “innovation” sites) worked with Healthcare Excellence Canada (HEC) on an economic evaluation which led to recognition of the Program as a promising practice ready for spread and scale. In 2019, the Partnership and HEC came together to support a pan-Canadian collaborative (Paramedics and Palliative Care: Bringing Vital Services to Canadians, “PPC” 2 that supported seven teams from British Columbia, Saskatchewan, Manitoba, Ontario, New Brunswick, and Newfoundland and Labrador to tailor and implement the Program in their local context. As paramedicine evolves, supporting new initiatives within the field can be a force for driving meaningful change and delivering more effective, patient-centred care. 3 While these efforts can be complex, Pan-Canadian Health Organizations (PCHOs) can leverage their expertise, networks, and broad health system perspective and play a key role in facilitating these advancements.
Key elements to support scale and spread: The roadmap
Elements for the successful spread and scale of PPC.
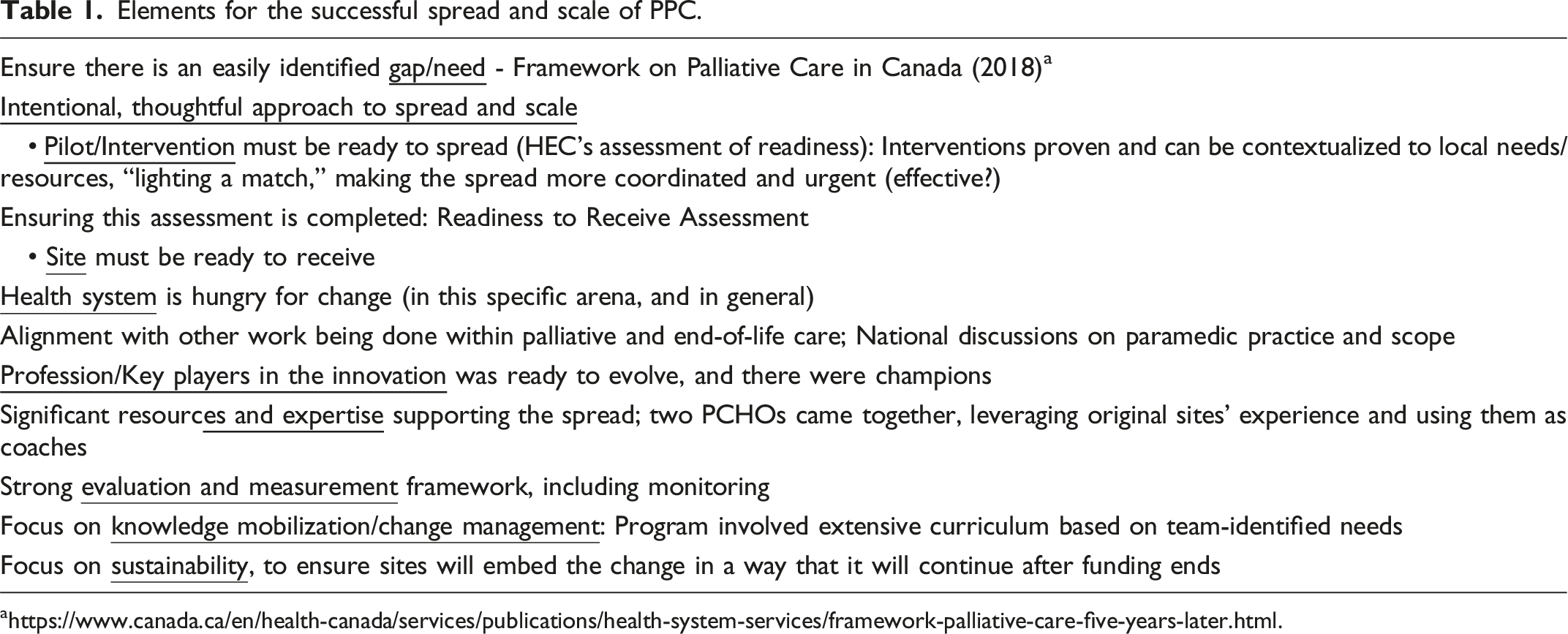
Clearly identified gap
In the last two weeks of life, 40% of patients with palliative goals of care visit the ED 6 and paramedics facilitate more than half of these ED visits. 7 EDs tend to be chaotic and overcrowded, making them less than ideal for a palliative approach.8,9,10 While 70% of Canadians express a desire to die at home, only 20% of people are ultimately able to do so. Past work has demonstrated that paramedics are called by the public for support in this goal, because their usual supports are delayed or unavailable, or because in the moment of crisis the number for help is 9-1-1. 1 Although paramedics are familiar with managing many of the most common palliative symptoms (pain, shortness of breath, and nausea/vomiting), various legislative, policy, and education elements were misaligned with paramedics providing a palliative care approach.
The promising practice was ready to spread (and sites were assessed as ready to receive)
The innovation site teams recognized the gap and built strong programs through significant consultation and support. The initial evaluation of the innovation sites looked at all aspects of the Quintuple Aim. The concept is based on leveraging the strengths of an existing resource; paramedics are trained to treat the most common symptoms at the end of life, and unlike other palliative home care providers, paramedics are positioned for widespread availability and rapid unscheduled responses, carry controlled substances, and do not travel in personal vehicles. Through the Quintuple Aim lens: (1) Provider: The NS/PEI program demonstrated improved paramedic comfort and confidence. (2) Patient/Family: High patient satisfaction with patients/families noting the professionalism and compassion of paramedics (“I can’t speak highly enough about the care they gave her. They explained what they were doing and why, so I knew what to expect and what was going to happen”); 24/7 availability (“This was my only comfort, knowing I could call paramedics. They made it very clear to us that if we weren’t comfortable, we could call them, doesn’t matter if it was once or five times. They said ‘we will be here”); relief of symptoms. (“When he can stay home, it helps a lot. We made the initial call, thinking he would have to go to the hospital, but they relieved his symptoms to the point that he could stay home”). (3) Clinical outcomes: In this early stage of implementation, 40% of calls to 9-1-1 resulted in treatment at home, and a time savings of a median of 20 minutes on 9-1-1 calls. Controlled for age and sex, there is a 23 % increased hazard of dying at the hospital (P < 0.001) in the pre-program period as compared to after the program launched. (4) Financial: Analysis in NS showed a four-fold return on investment in the first year of operation. (5) Equity for rural populations is increased because of the positioning of paramedic resources to ensure population coverage, and current work is examining the influence of sociodemographic factors.5,11,12
The profession, key players, and the health system were ready to evolve
A Canadian study found over three quarters of patients with advanced chronic diseases present to the ED in the last 6 months of life, with 68% resulting in hospital admission. 13 Patients receiving palliative care frequent EDs as other options for at-home care may be limited, particularly in certain situations (e.g., rural areas and outside business hours). EDs, which tend to be loud, crowded, and have increasingly long wait times, are not optimal and are often stressful for patients who are simply seeking symptom control. 14 Health systems around the world are looking at innovative ways to support more care in the community, align the “right care” with the “right place,” integrate previously siloed health and social services, support interprofessional working and optimize scopes of practice, and develop services that put the patient, their family, caregivers, and community at the centre.
Paramedics traditionally work to resuscitate severely ill and injured patients; getting “a save” is so often seen as the goal. Incorporating a palliative approach, where the “save” is focused on quality of life not quantity, introduces a new thought process. Incorporating a role as a palliative healthcare provider into what it means to be a paramedic, in concert with other expanded or novel roles, forms a picture of an evolving professional identity in Anglo-American Emergency Medical Services systems such as those in Canada, the United Kingdom, Australia, and others.
Paramedics and palliative care teams see this as a good fit with paramedic professional identity. Paramedics strongly agreed that “all paramedics should be able to provide basic palliative care” median score 7 (IQR 6-7) on a 7-point scale. 15
Paramedics are taking on more independent roles, with clinical practice guidelines instead of linear protocols, work in primary care and public health settings, and non-transport configurations, all of which is novel. This is supported by the growth of degree programs in paramedicine, professional colleges of paramedicine, and paramedics with graduate degrees who are advancing the science of their own practice. The newly updated and released National Competency Framework for Paramedics now emphasizes the roles that paramedics play in primary and urgent care, and includes broadened competencies for supporting those with palliative care needs.16,17
The call for sites to join the spread collaborative catalyzed efforts already underway or under consideration in many jurisdictions; it sparked the effort to “do it together” and “do it now,” ultimately leveraging resources of the innovation sites, the PCHOs, and the other spread and scale teams.
Diverse resources and expertise supported the spread and scale through a pan-Canadian interprofessional collaborative effort
Together, the two PCHOs working with the Program innovation sites brought significant skills, resources, and expertise, as well as the mandate to spread and scale promising programs in healthcare. The Program was evaluated for readiness to spread and scale and was deemed appropriate. Individuals who developed and implemented the Program in the innovation sites filled “coaching” roles to provide guidance and support to the expansion sites. The Innovation Sites and PCHO leads worked to create a jurisdiction-agnostic model and launch a pan-Canadian collaborative.
An evaluation of this collaboration highlighted key learnings that support the use of partnerships and collaboration in similar work. While partnering organizations can be of any size, it was found that relevant PCHOs may add the most value in three areas. First, pan-Canadian organizations often have more specialized staff and expertise available. For example, HEC provided expertise in quality improvement, evaluation, and engagement practices, and the Canadian Partnership Against Cancer provided leadership in financial, performance measurement, impact assessment, resource, and project management. Second, initial seed funding and resources are often more available and secure for a set period of time to ensure the promising practice can be spread, instead of having to continuously apply for funding. Third, the perception of branding, trust, and credibility of the initiative can be bolstered by partnering with pan-Canadian organizations. Smaller scale programs may benefit from this especially in terms of expanded reach and promotion, including through the creation of a Change package, multiple manuscripts, and participation in several in-person events.18,19,20,21
Compared to launching a pan-Canadian spread as a research project, or a quality initiative led by one person or team, the breadth and depth of resources brought to bear would otherwise be unobtainable. Participating teams had the added benefit of learning from each other, accessing diverse perspectives, and developing new networks and connections.
There was a strong, co-designed evaluation framework
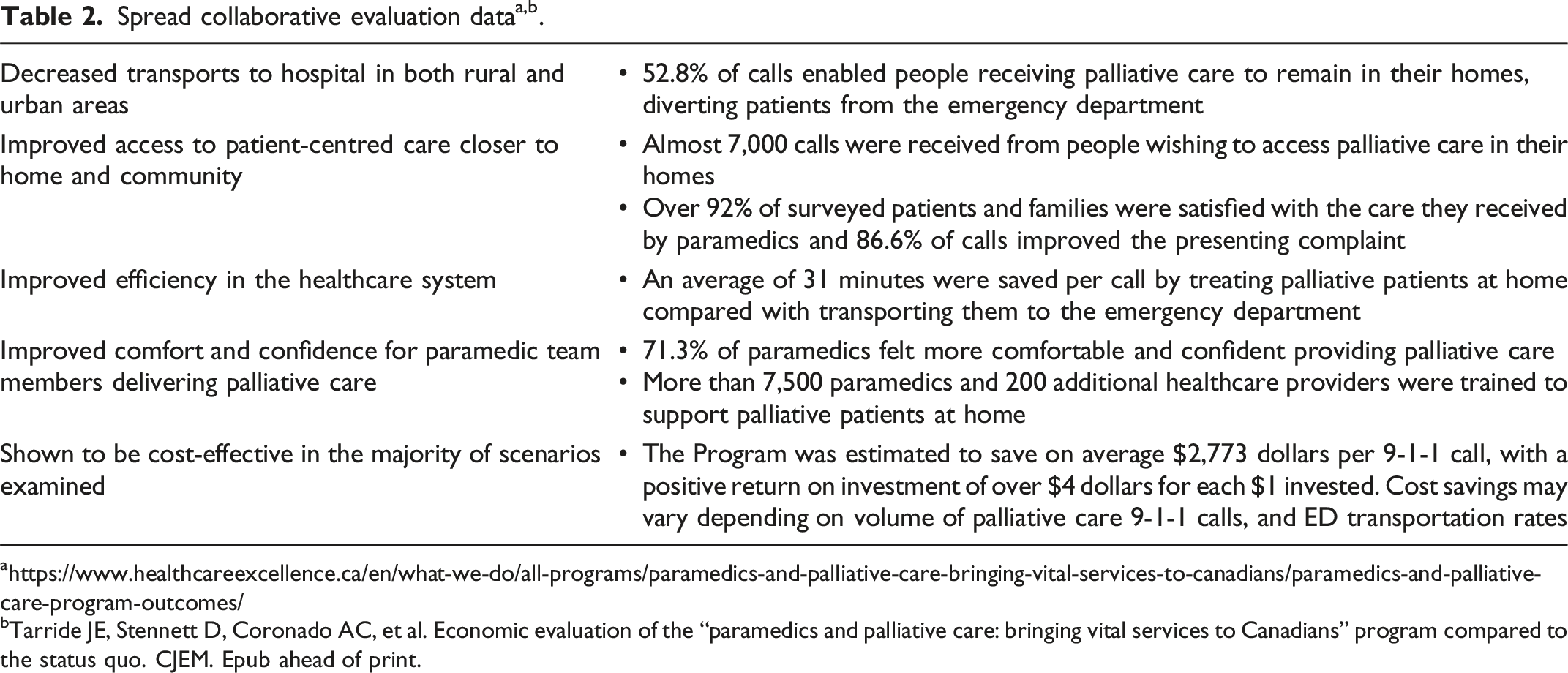
bTarride JE, Stennett D, Coronado AC, et al. Economic evaluation of the “paramedics and palliative care: bringing vital services to Canadians” program compared to the status quo. CJEM. Epub ahead of print.
Focus on sharing and knowledge mobilization strategies
During the collaborative, knowledge exchange between coaches and teams, and amongst teams themselves, was given specific attention. In addition to the essential ongoing support provided from the PCHOs, valuable and meaningful relationships were established amongst the teams of expansion and initial innovation sites. Coaches and support came from a very diverse range of sources; PCHOs, paramedic services, researchers, clinical champions, and cancer and palliative care agencies, which has been key to success. These partnerships were of exceptional value for teams that were smaller and did not have access to the diverse resources available to larger teams (project managers, researchers), and during COVID, many teams lost/reallocated resources as priorities shifted from the project to support pandemic response.
One partnership of particular significance was the coaching support provided by members of initial innovation sites. The ability to leverage the expertise and experiences of those individuals was instrumental, especially at the onset of the project when teams needed guidance on where to start, and how to merge very different specialities that historically had little to do with each other. This included support with identifying who to engage, changes from a regulatory and legislative perspective, and change management methods to successfully demonstrate how palliative care fits into paramedic practice.
Informal partnerships were founded amongst the project teams/sites themselves. There were scheduled meetings and annual events hosted by the PCHOs, but many teams worked collaboratively offline and found solace in recognizing that many teams faced the same challenges.
End-of-project knowledge mobilization included, but went well beyond, traditional conference presentations and publications. Formal partnerships were developed to support the initiative, and many have organically continued past the project dates and resulted in inter-provincial professional relationships. These relationships are helping to guide ongoing and future initiatives, and influence the direction of paramedicine in Canada.15,16
A broad knowledge translation strategy brought this new Program to the attention of professional practice groups throughout emergency medicine, palliative care, nursing, home care, and paramedicine. This concept of paramedics having a role in palliative care has been embedded, in the update to the national occupational competency standards for paramedicine. Sites not part of the spread collaborative are reaching out to existing Program sites to bring this into their local practice. It is being incorporated into provincial paramedic practice standards (Ontario). There are two pan-Canadian communities of practice. Paramedics and Palliative Care is now woven into the fabric of paramedic practice and palliative care in Canada but also in multiple countries internationally.
Emphasis on sustainability
Although the Program represented a big shift in practice, significance emphasis was placed on planning for sustainability, embedding the change in a way that ensured it would continue after the project funding and spread collaborative ended. For example, the program was strategically embedded in all major partners’ business plans (ministry, paramedic service provider, health authority), and system-wide complex change approaches were employed. Rather than being designed as an “add on” service or care provided by a new or specialized team, the approach changed how paramedics served patients and families they were already supporting in their routine 9-1-1 caseload. Palliative care education for paramedics has now been embedded into recruit orientation and adopted by educational institutions who train paramedics. Program specific clinical practice guidelines, protocols, policies, and procedures were integrated into larger organizational frameworks and aligned with established ongoing review cycles. Electronic charting software was updated to include palliative care data fields, and regular audit process and monitoring mechanisms were added to existing quality assurance programs. The ability of this promising practice to spread and scale across Canada represents significant adaptability and highlights the potential application in national and international settings. The 10 different regulatory frameworks for paramedicine and varying practice environments across the spread collaborative required significant jurisdictional tailoring, all while preserving the core vision and elements of the program. The stories and experiences of patients, families, caregivers, paramedics and other healthcare providers continue to be collected and told to reinforce that the new way is not only the better way, but the easier way.
Conclusion
The Paramedics and Palliative Care program has successfully launched from a promising practice to part of the national framework for palliative care, and the professional identity of paramedics. The Program has strong evidence through all elements of the quintuple framework. Breaking down silos between providers serving the same population is essential to patient, provider, and healthcare system success. Taking this beyond the specific example of the PPC program, or even these two specific PCHOs, this showcases the elements upon which a successful pan-Canadian spread and scale program are dependent, and highlights the strength of bringing together multiple players with diverse contributions.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors 1, 2, 4 and 7 have received a stipend from HEC as a coach on the national spread collaborative and Author 1 received travel support from the European Association for Palliative Care. Author 3 is employed by HEC and authors 5 and 6 by CPAC.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.