
Abstract
This article investigates whether, in the context of rising nationalism, drawing attention to national innovation strategies influences public health behaviours, particularly vaccine uptake. It draws on an original two-wave panel study of United Kingdom (UK) respondents during the COVID pandemic. The survey included an experimental design, which primed respondents with a nationalist framing of COVID-19 vaccines, drawing attention to the UK’s role in developing the AstraZeneca vaccine and in rapid approval and roll out of other vaccines. Our results show no significant impact of nationalist framing on vaccine willingness, even among those with nationalist or science-skeptical views. These findings suggest public health authorities should be cautious with nationalist framing, as it may be ineffective or counterproductive.
Introduction
Do national innovation strategies shape citizens’ public health behaviours? In an era of rising nationalism, public authorities face the temptation to lean into national sentiment to encourage citizens to engage with public health policies—from taking vaccines to promoting healthy lifestyles. Those citizens most reluctant to participate in public health programs tend to be those both least trusting of government and science, and most attracted to populist framings. This constellation of preferences makes branding policies with “nationalist” imagery superficially attractive. But do such interventions work, both with their target audience and more generally?
In this article, we examine the case of “nationalist” framing of vaccines during the COVID epidemic in the United Kingdom (UK). In the race to develop COVID vaccines, both democratic and non-democratic governments branded vaccine projects to their domestic publics as “national” success stories. In the United Kingdom, the government promoted the AstraZeneca vaccine as “Britain’s gift to the world,” even toying with the idea of placing a Union Jack on vaccine packets. 1 UK politicians further trumpeted that the UK regulatory system meant the first person to be given a fully approved vaccine (the Pfizer/BionTech vaccine), in December 2020, was British. Some critics pointed to the dangers of nationalist discourse in limiting foreign acceptance and adoption of the AstraZeneca vaccine. 2 But the question remains, did these nationalist frames help with vaccine takeup in the United Kingdom?
We ran a two-wave panel survey of a cross-section of the UK population in 2021 and 2022 to test whether intended vaccine takeup was higher when vaccines were framed as (a) a UK regulatory success (rapid approval of Pfizer/BionTech) or (b) an innovation success (rapid approval and development of the AstraZeneca vaccine) relative to a control group that received no informational prompts. We find no evidence of either framing effect on reported willingness to use any vaccine, either among the full sample or those with more nationalist or science sceptical predispositions.
Our findings thus have important implications for public health strategies in Canada going forward. The British strategy of rapidly and competitively pursuing early vaccination, at the cost of collaborative arrangements, led to backlash from global partners with few public health gains. Canada did not pursue a nationalist framing in its public communication strategy around COVID. However, in its aftermath, there has been substantial federal and provincial investment in new vaccine manufacturing capacity, including a new Sanofi backed plant in the greater Toronto area. While political leaders have promoted this plant as an engine of innovation and “made-in-Ontario vaccinations,” 1 our results suggest that they should be cautious in using nationalist frames around Canadian innovations as a public health strategy. We argue that Canadian health leaders should continue to seek a collaborative approach to public health, not a nationalistic one, as the gains to nationalism are limited and the costs potentially high.
Motivation
In the race to develop and administer the COVID vaccines, concerns about “vaccine nationalism” emerged. Vaccine nationalism refers to the competitive actions of nations in securing vaccines for their own populations ahead of other countries. While scholars and ethicists debate the consequences of vaccine nationalism for equitable access to vaccines, we ask a different question. Did nationalist messaging affect how citizens reacted to vaccines?
The United Kingdom offers a valuable case study with which to consider these questions, as despite initially high uptake rates, concerns about vaccine hesitancy led policy makers to employ a variety of public health communications, some of which relied on nationalist messages. 2 The United Kingdom was hardly alone in this approach, since other countries, including China, relied on nationalist frames in public health communication. 3
The large body of work on COVID-19 vaccine hesitancy points to several common concerns among vaccine hesitant respondents: safety concerns, lower levels of trust in the state/market, and a belief that vaccines are unnecessary. 4 More general work on vaccines shows that distrust of institutions is a more important predictor of vaccine hesitancy than scientific ignorance. 5 These studies further suggest that the national origin of vaccine development and regulatory approval may be an important mediator between individual correlates and vaccine behaviours for two reasons.
First, national origin can provide cues about the efficacy or safety of vaccines. Vaccines that have been developed by an untrusted source are likely to accentuate respondents’ concerns, and vice versa. Bullock, Lane, and Shultz, for instance, find more reported willingness in a UK-based survey to take fictitious vaccines (including those associated with discredited pharmaceutical company Theranos, which most respondents had not heard of) than the Russian Sputnik or Chinese Sinovac vaccine. 6 Kreps and Kriner, using a conjoint design that included attributes related to vaccine efficacy and national origin, also find origin effects on reported vaccine usage intentions. 7 Among their sample in the United States, they find respondents are more likely to accept vaccines from the United States and United Kingdom—and less likely to accept the Russian or Chinese vaccines. These results suggest that vaccine sources may exert some influence on behavioural intentions, via a mechanism of public trust.
Second, a range of studies, including our own, show that populist sentiments can predict vaccine hesitancy. In the United Kingdom, Brexit voters were slightly more vaccine hesitant. Nationalist frames that resonate with populist concerns about global health organizations, and prime attention to national success, could potentially reduce hesitancy.
Scholarly work examining the public health components of “vaccine nationalism” is less developed than more generic studies of origin effects. However, in a major fourteen-country study of vaccine preferences, Barceló et al. show a substantial increase in the likelihood of preferring a home produced or home developed vaccines, as well as generalized support for “American” and “German” vaccines (and negative support for “Chinese” vaccines) across a wide variety of contexts. 8 They further find that this home preference holds across all groups, but that it is elevated among a subset of respondents who report high levels of nationalism.
This work suggests that nationalist frames may increase support for vaccines, both by providing cues about safety and appealing to pro-social nationalist attitudes. However, while Barceló et al. draw a link between vaccine preference and vaccine use, questions remain as to whether the preference for home-country vaccines translates into intended usage. 9 The results from other studies suggest little difference in how respondents distinguish among vaccines from similar nations (e.g., Western democracies) in determining use intentions. 10 Thus, questions remain as to whether nationalist frames regarding innovation and regulation affect take up rates. This question is critical for public health leaders, both in government and on the ground, as they communicate to diverse populations about the nature of vaccine risks.
Research design and methods
To investigate these questions in the UK context, we conducted a two-wave panel study on a representative sample of residents (excluding Northern Ireland) using the polling company YouGov. The first wave took place on September 30, 2020 and October 1, 2020 and had 1,642 respondents. The second wave surveyed the same group of respondents, receiving 1,219 responses from the original 1,642 participants (a retention rate of 74%), over the week commencing February 1, 2021. The purpose of the study was to investigate a range of attitudes towards COVID policies, trust in government, and the political and social correlates of health behaviours.
In both waves, we asked a similar question exploring how likely people would be to take a vaccine against COVID-19. Our initial question involved a four-point item ranging from “very unlikely,” to “unlikely,” to “likely” to “very likely,” with respondents allowed to answer “don’t know.” We further dichotomised this variable by combining the first two and the last two categories. In between the first and the second wave, the UK government began its vaccine roll out program, with the first vaccines administered on December 8, 2020. By the first week of February, around 20% of the population, mostly older or high-risk individuals, had been vaccinated. As such, in the second wave, our approach to measuring vaccine hesitancy was slightly more complex. We added an option “already taken the vaccine” to the response choices. In analyzing the data, we both include respondents who have taken the vaccine in the “very likely” group and run all models excluding the already vaccinated as a robustness test.
To investigate the effects of nationalist framing, in our second wave, we added a survey experiment that provided respondents with alternative frames about vaccine origin. We randomly assigned respondents to either a control group or one of two treatment groups (each with 1/3 of the sample). Both treatment groups received prompts aimed at emphasizing “vaccine nationalism,” allowing us to assess whether priming respondents about the successes of the UK’s vaccine program affected their willingness to take the vaccines.
The first treatment had the following question: “On December 2 of last year, Britain became the first country in the world to approve a vaccine against COVID-19—the BionTech/Pfizer vaccine developed by German scientists and a pharmaceutical company in the United States. How likely would you be to take a vaccine against COVID-19 if you were offered one?”
The second treatment had the following question: “On December 30 of last year, Britain became the first country in the world to approve the Oxford/AstraZeneca vaccine against COVID-19—developed by British scientists at the University of Oxford and the British company AstraZeneca. How likely would you be to take a vaccine against COVID-19 if you were offered one?”
The first treatment provides a weaker form of vaccine nationalism—priming the speed of the UK regulatory process—and the second, a stronger form—priming both Britain’s regulatory response and national development of the AstraZeneca vaccine. The control group received no informational treatment and was asked about vaccine intentions (or usage). We thus can compare the effects of our informational treatments across the sample as whole.
We then look at the effects of the treatment across groups of respondents based on their reported Brexit vote. Voting to “leave” in the 2016 Brexit referendum is a significant predictor of vaccine hesitancy. Brexit voters tend to have stronger levels of nationalism, but lower levels of trust in politicians and the state, meaning that the nationalist prime might be particularly effective for this group.
Results
We first compare reported vaccine intentions across the three groups: control, Pfizer treatment, and AstraZeneca treatment. We use survey weights to adjust the sample to reflect the UK population (the unweighted results are substantively and statistically similar). Figure 1 shows the proportion of respondents who said they were likely or very likely to take the vaccine, with 95% confidence intervals. Average support varies only between 0.86 and 0.89—in line with the aggregate vaccine take up rates—but there is no statistically significant variation across the treatment groups. Proportion likely or very likely to take vaccine.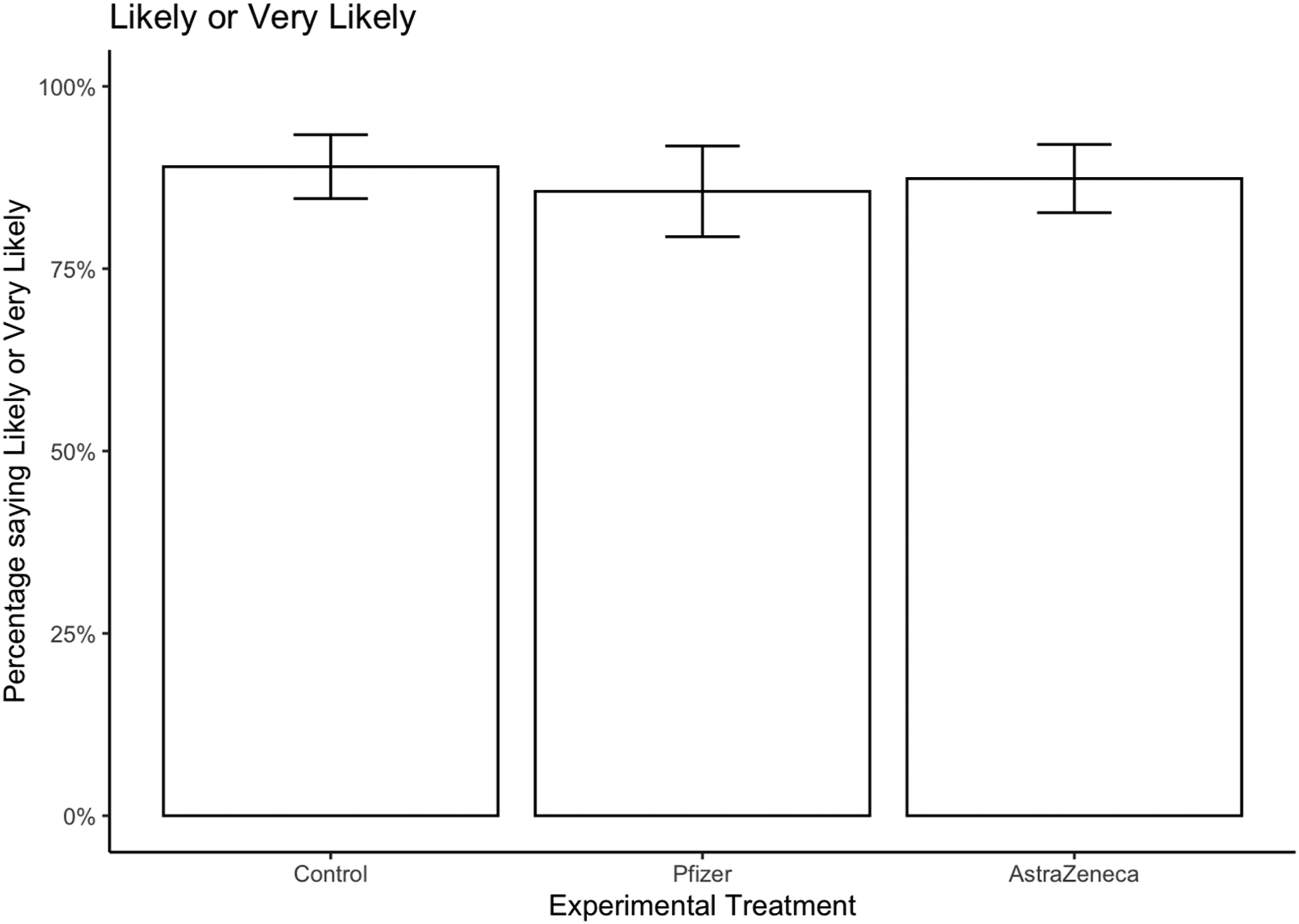
Overall, there is no evidence supporting the conjecture that “vaccine nationalism” framing affects willingness to take the vaccine.
Subgroup analysis
We now turn to subgroup analysis. We use data from the YouGov panellists about their vote in the 2016 EU Referendum, and group respondents into those who voted to Remain, those who voted to Leave, and those who did not vote.
We begin by showing that in aggregate, those who voted Leave or did not vote were less supportive of taking the vaccine in both the first and second waves. Figure 2 shows that across both waves, people who voted Remain in the 2016 EU Referendum were around 7% points more willing to take the vaccine than those who voted Leave or who did not vote in the referendum (here using the binary vaccine variable). Support for taking the vaccine conditional on Brexit vote.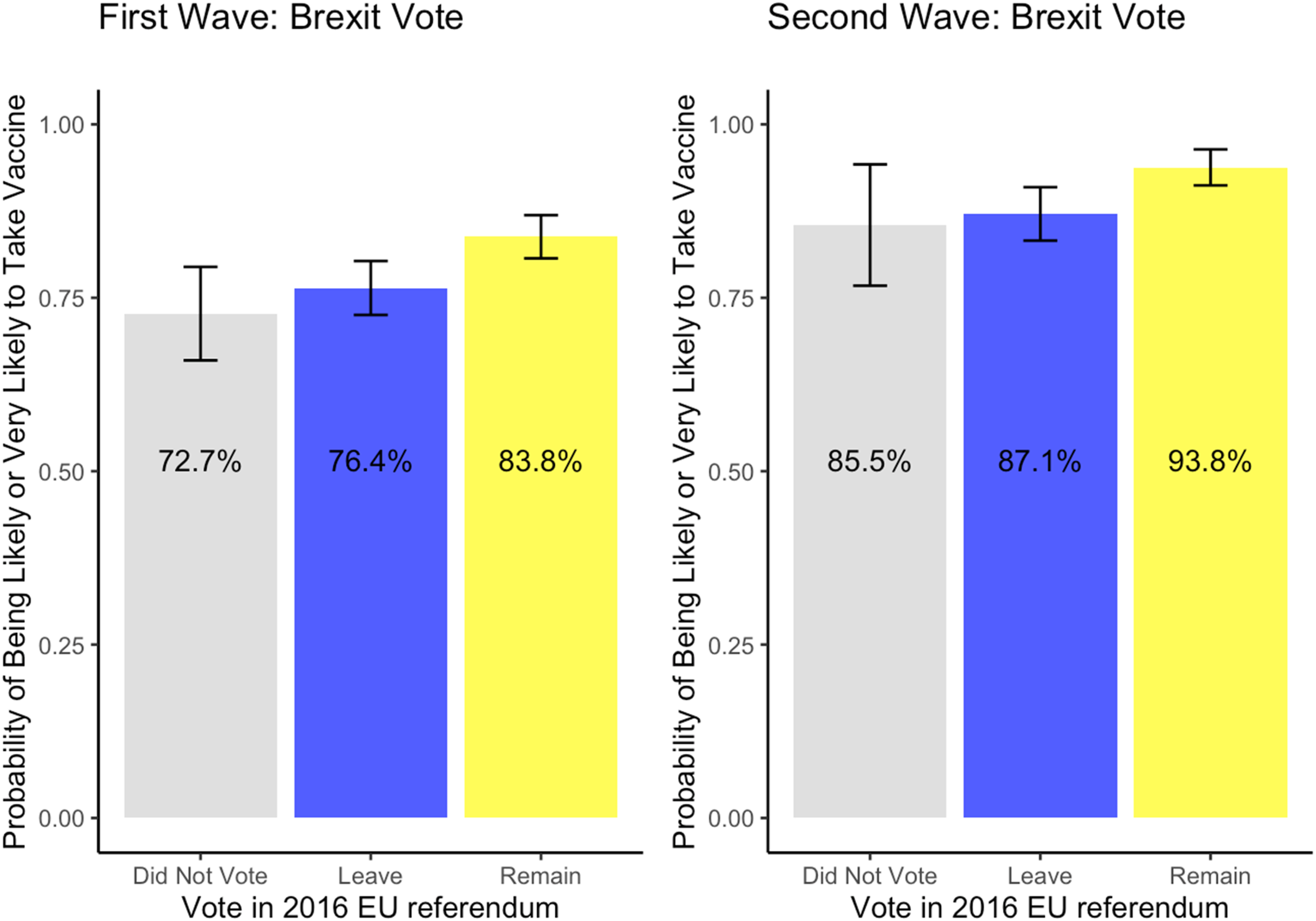
Support for taking the vaccine: treatment and demographics.
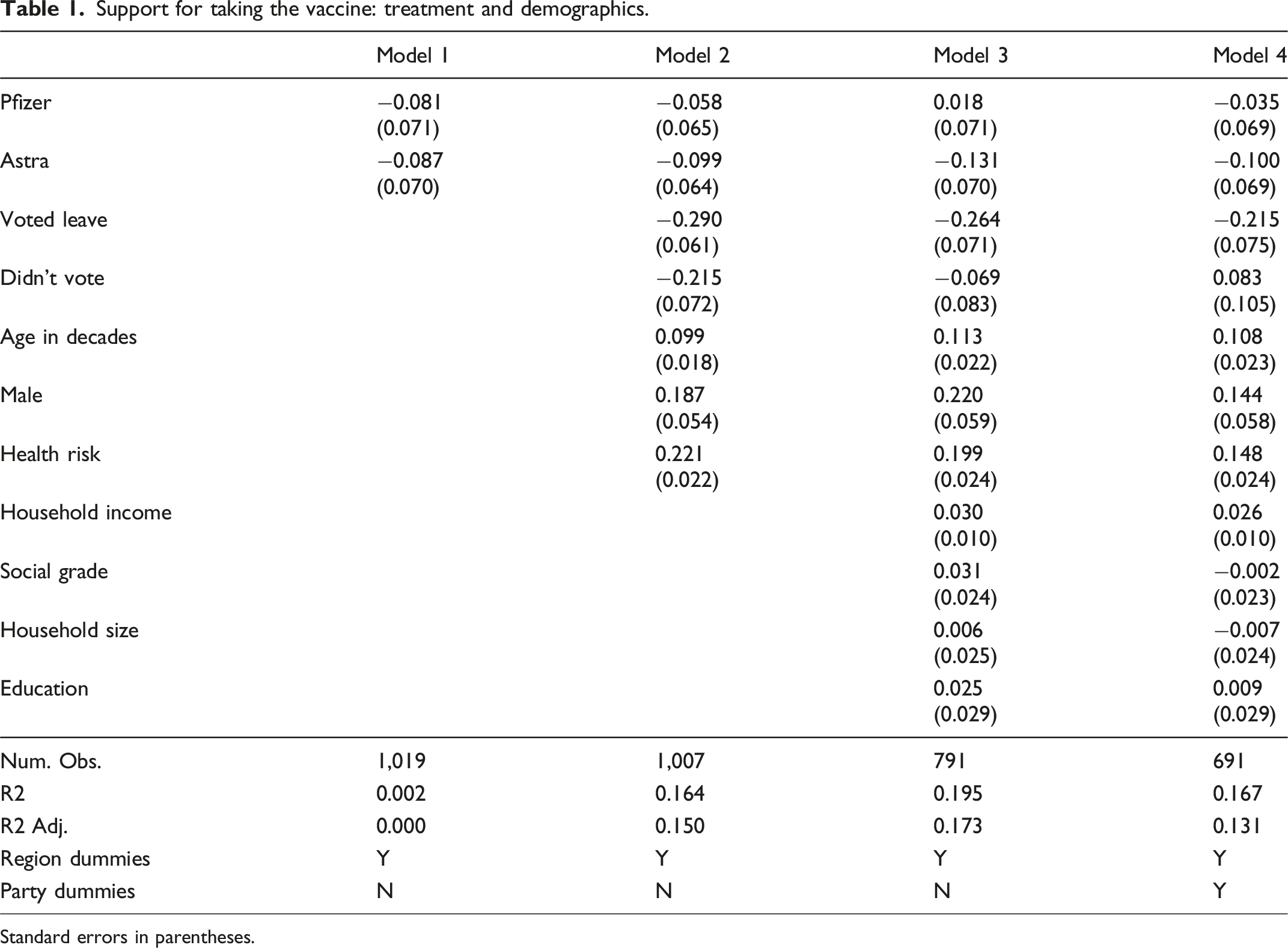
Standard errors in parentheses.
Leave voters and to a lesser extent those who did not vote score lower on the four-point vaccine scale by somewhere between 0.2 and 0.3 points. Older voters are more likely to want to take the vaccine, as are men, and those with higher perceived health risks. The size of the Leave-Remain difference is fifty percent larger than gender, and equivalent to two to three decades in age. It remains robust to controls for household income, education, household size, and education in Model 3, and vote choice in the 2019 General Election (Model 4).
Other analysis shows that Brexit vote choice does not condition the effects of the experimental treatment. There is no clear evidence that voters more supportive of British independence from the EU are more impacted by the nationalist frame. In no case, do either of the treatments differ from the control group. The Pfizer treatment does seem to make non-voters less supportive of the vaccine than it does for Remain voters (though we note there is no evidence of direct effects of either treatment on non-voters). Overall, there is no systematic evidence of heterogeneous treatment effects (results available on request).
Conclusion
In contrast to Barceló et al., we find little evidence of the efficacy of priming nationalist innovation frames affects respondents’ willingness to take vaccines—either for the full sample or among Brexit voters. 11 There are several possible interpretations of these results, with implications for the Canadian context.
The first is that the treatment may be too weak. Particularly in the period around February 2021, public health messaging was strong and pervasive. Providing additional framing in this environment may have had a limited effect. Here, a lesson for public health leaders is that messaging is always occurring in a specific informational context, which can affect its efficacy.
However, a second possible interpretation is that a nationalist frame might have countervailing effects, both priming national pride and negative evaluations of the current government performance. There is evidence that national identity is a predictor of certain positive public non-pharmaceutical health behaviours. Van Bavel et al. find that those who identify with their nation are more willing to engage in physical distancing. 12 Here, priming nationalism may have some positive effects in terms of drawing attention to pro-social behaviors.
However, priming nationalism around pharmaceutical interventions can work differently. While we should be cautious about extrapolating from a single study, these null results do have potentially important implications. Our study provides no support for the conjecture that “wrapping public health policy in the flag” can motivate desirable public health behaviours among the public, including among those who might be less trusting of science or government. Indeed, authorities should be cautious about further unexpected side-effects of promoting “nationalist” framings. If nationalist frames are harmful for the export of vaccines and have limited domestic effects on public health, it suggests a negative net effect.
In short, linking public health strategies to national forms of innovation is a risky strategy. This finding is of importance for health leaders and policy makers as they consider future communications strategies. As Canadian health leaders think about future public health challenges, including building on new life sciences innovations and pharmaceuticals in the Canadian context, they should reflect on how to build support for Canadian and provincial public health institutions without undermining support for global public health messaging and collaborative health institutions.
Footnotes
Acknowledgements
We thank the University of Oxford John Fell Fund (0009190) for financial support. We also acknowledge the support of the Canadian Institute for Advanced Research (CIFAR) Program on Innovation, Equity & the Future of Prosperity (IEP), especially for the comments, suggestions, and support during the health innovation subgroup meetings in Washington DC, and Turin, Italy, in November and May 2023.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institute for Advanced Research (General), John Fell Fund, University of Oxford (0009190).
Ethical approval
This project received ethical approval from the University of Oxford IDREC: reference R71718/RE001.