
Abstract
Workforce planning ensures that the health workforce is aligned with current and future population needs. Engagement with partners and knowledge users is a leading practice in planning and is essential for planning to be successful. The goal of this study was to explore the considerations and processes involved in integrating engagement into workforce planning. Through a case study of primary care workforce planning in Toronto, we address the role of engagement, how it can be integrated into planning, and how lessons from engagement support spread and scale of effective workforce planning. In the course of engagement with five Ontario Health Teams between September 2023 and February 2024, we learned that there is considerable enthusiasm for planning, but that support is needed, and that engagement guides investment and strengthens relationships. We offer guidance for leaders with respect to actualizing engagement and building capacity for health workforce planning across the health system.
Introduction
As health workforce challenges accumulate, health leaders are turning to planning as a means to anticipate and proactively mitigate the impact of workforce crises on services and communities.
Planning is an essential component of health system management. Health workforce planning is the process of “estimating the number of persons and the kind of knowledge, skills, and attitudes they need to achieve predetermined health targets and ultimately health status objectives.” 1 An iterative process that has political, social, and technical dimensions, 2 health workforce planning is necessary to ensure the health system meets the evolving needs of communities therein. 3
In a health system context, strong relationships between health system partners can enhance planning processes and accelerate innovation. Engaging individuals who influence or use innovations as active partners can help to ensure fit-for-purpose innovation 4 and can enhance the potential for spread and scale of planning innovations.4,5 Considerations for integrating engagement into workforce planning have not been systematically articulated in the literature, and guidance for planners and leaders is needed. 6
Aim and objectives
The aim of this work is to systematically explore the considerations and processes involved in integrating engagement into workforce planning at the local level.
Through a case study of primary care planning in Toronto, we highlight lessons learned from the process of engagement, addressing the following questions: (1) What role does engagement play in planning? (2) How can learnings from engagement be incorporated into planning? (3) How can learnings from engagement facilitate the spread and scale of leading practices in workforce planning?
Methodology
Study design
This work is presented as a qualitative case study with an exploratory design that takes a developmental evaluation approach. 7 Developmental evaluation monitors developments, progress, or advancements during the design or implementation of an innovation. Developments are analyzed for key learnings and adaptations are made to improve the innovation. 8
Case study: Primary care workforce planning in Toronto
Over 2.7 million people live in Toronto, the largest city in Ontario, Canada’s most populous province. 9 The City of Toronto includes one census division with 11 sub-regions and 158 neighbourhoods.
Primary care workforce planning challenges in Toronto include rapid population growth, patient mobility, physician retirement, and a changing primary care landscape, exacerbated by the COVID-19 pandemic. A comprehensive, regional level planning approach supports health workforce decision-making and equitable deployment of primary care resources across the city.
Workforce planning has been a strategic priority in Toronto, and work is underway to build capacity for planning at local levels. Integration of local primary care decision-makers into regional planning processes occurs through Ontario Health Teams (OHTs). OHTs are a collaborative of health service providers with a central leadership structure, accountable for improving the health of the local population, by organizing and delivering care that is connected to patients in their local communities. 10 Eight Toronto-area OHTs were offered formal support for primary care workforce planning.
Engagement
Our engagement with OHTs unfolded in four stages: • June 2023—Initiating OHT engagement and recruitment: Our planning team presented a brief overview of workforce planning to gauge interest from Toronto-area OHTs. Our recruitment of OHTs followed a purposive, homogeneous sampling approach.
7
Following this session, five OHTs self-identified as being interested in further engagement. • September 2023—Workforce Planning 101: In this session, we: (1) provided an overview of the fundamentals of workforce planning, (2) sought feedback through a real-time evaluation survey (Supplemental materials
1
), and (3) identified areas of priority for OHTs. The survey included six Likert scale questions to understand baseline levels of knowledge, confidence, and enthusiasm for planning. Results of the survey were presented back to participants in the moment. The survey (administered through SurveyMonkey) development was guided by the theoretical domains framework,
11
a cross-disciplinary implementation science framework used in behaviour change research to explore capabilities, opportunities, and motivations. • October 2023 to February 2024—OHT engagement sessions: We conducted one-on-one sessions with each of the OHTs. In preparation for these sessions, we sent out a pre-session survey (Supplemental materials
1
) through Microsoft Forms to each OHT asking about: (1) the factors that influence workforce planning and (2) planning activities they would find helpful. Each session included a tailored agenda with flexibility to adapt in the moment. In these sessions we: (1) provided an opportunity for OHTs to present their planning challenges and needs, (2) presented a curated data package tailored to each OHT, and (3) provided an overview of relevant planning tools. The data packages included community characteristics, service requirements, spatial patterns of utilization, workforce profiles and capacity, alignment, and resources. Two OHTs requested a second one-on-one session to cover more material. • February 2024—Final “Network of Planners” engagement session: In this session, we: (1) asked OHTs to share an update on their workforce planning, (2) presented preliminary results from our developmental evaluation to inform OHTs of common challenges and opportunities to move forward, and (3) discussed how our team can continue to provide support for planning.
Communication with OHTs was mediated by Ontario Health Toronto’s Health System Strategy, Planning, Design, and Implementation team.
Analysis
The real-time evaluation survey from the “Workforce Planning 101” session and the pre-session surveys for the one-on-one sessions were analyzed in Microsoft Excel using descriptive statistics.
All engagement sessions were recorded on Zoom or Microsoft Teams and the audio was transcribed and de-identified using the software, Condens. There was a dual layer of analysis for each transcript from the “Workforce Planning 101” and the one-on-one sessions. The first layer of analysis was an inductive content analysis 7 which develops genuine themes from the data. The second analysis was a deductive framework analysis 7 which develops themes using a framework as a guide. We used the Institute of Health Information’s Framework for Going to Full Scale (FGFS) to identify themes related to spread (the breadth of planning across the health system) and scale (the depth of planning within organizations) of workforce planning. 12 We adapted the use of this framework for this project; for example, we did not apply the codes for phases of scale-up for this case study as each OHT was at a different phase of workforce planning.
Our codebook along with definitions for deductive codes is available in the supplemental materials. 1
Findings
The OHTs we engaged with span five Toronto sub-regions, 93 neighbourhoods, and over 1.5 million residents. Across all OHTs, we engaged with 53 health system leaders from a range of backgrounds, both non-clinical and clinical (including medicine, nursing, and physiotherapy). There is considerable variation, both between OHTs and within each OHT, in community sociodemographic characteristics, workforce characteristics, and access to primary care.
Workforce Planning 101: Introducing OHTs to the fundamentals of workforce planning
From the “Workforce Planning 101” session, we learned that the majority of OHT participants were enthusiastic about planning (Figure 1A) and felt that it was important (Figure 1B) but had limited knowledge (Figure 1C) and confidence (Figure 1F) in relation to planning. The engagement session was well received by OHTs and enthusiasm for planning across the OHTs was evident during conversation: “If there’s anything we can do to help you liberate more data because we’re all about data, let us know” and “we’re hot on the heels of conversations with our executive leadership team about our primary care strategy, so this is very important and very timely.” Participants also discussed strategies to leverage interprofessional team-based care to enhance comprehensive practice in their regions, including shifting physician services to nurses and other providers and exploring alternate compensation and payment models. Much of the conversation focused on uncertainties with respect to using data to predict workforce trends and challenges inherent in planning, which were noted as barriers to planning in the survey (Figure 1D). There was appreciation for the guidance and resources provided by our planning team as enablers in the planning process (Figure 1E). “[The toolkit] raised our capability to do planning in primary care.” Participants expressed in discussion and in the real-time survey (Figure 1F) feeling a sense of confidence, agency, and enhanced capability to plan using these resources moving forward. Workforce Planning 101 real-time survey results. The percentage of OHT representatives (n = 12) reflecting on workforce planning in terms of (A) enthusiasm, (B) importance, (C) knowledge, (D) barriers they foresee, (E) enablers they foresee, and (F) confidence to undertake workforce planning.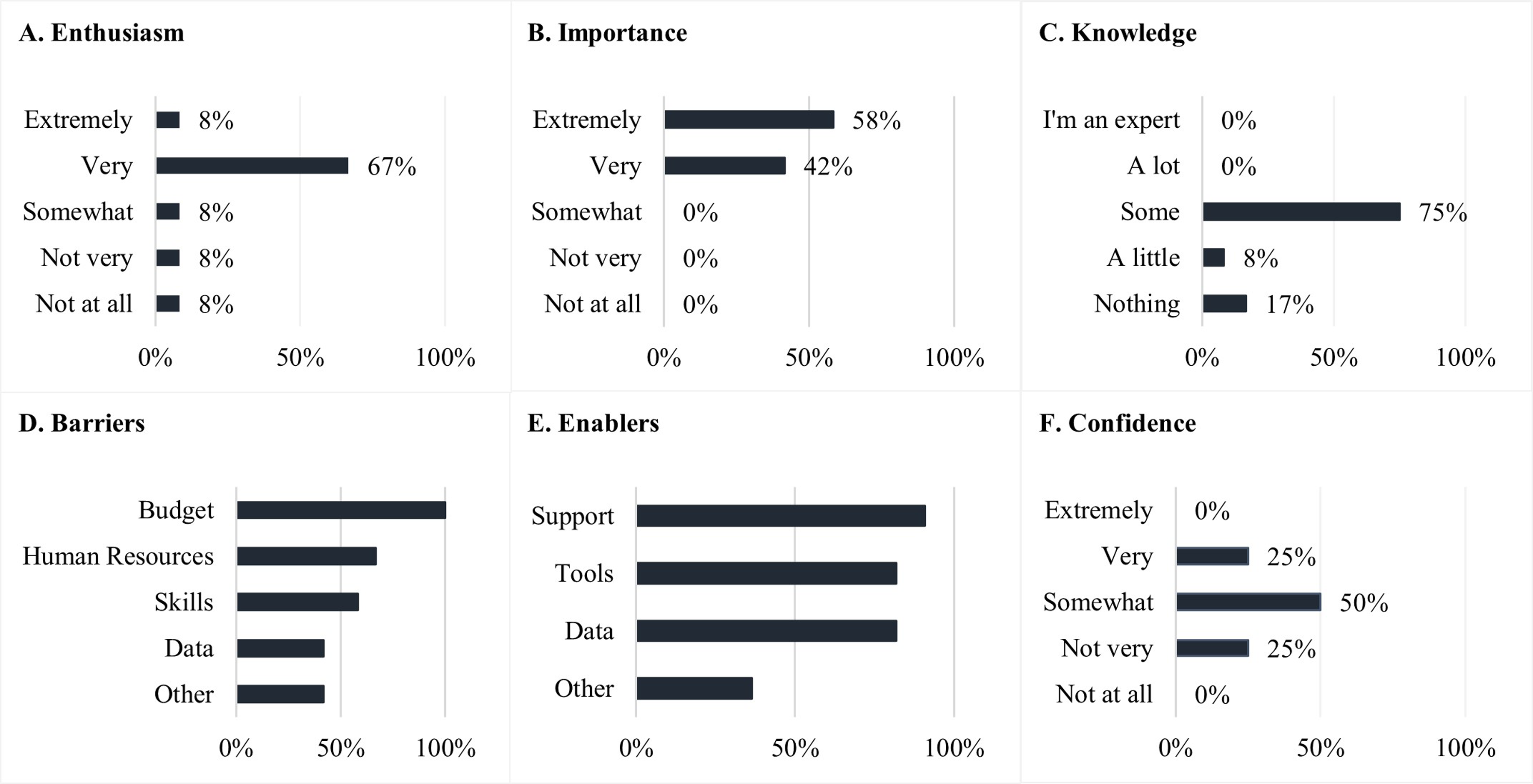
OHT engagement sessions (one-on-one): Workforce planning at the community level
The pre-session surveys helped us to tailor the agendas for each session to individual OHT priorities, although we retained some flexibility to address specific questions and respond to specific concerns during the session. Reviewing the data packages was a priority for most OHTs and represented the largest time commitment in most sessions.
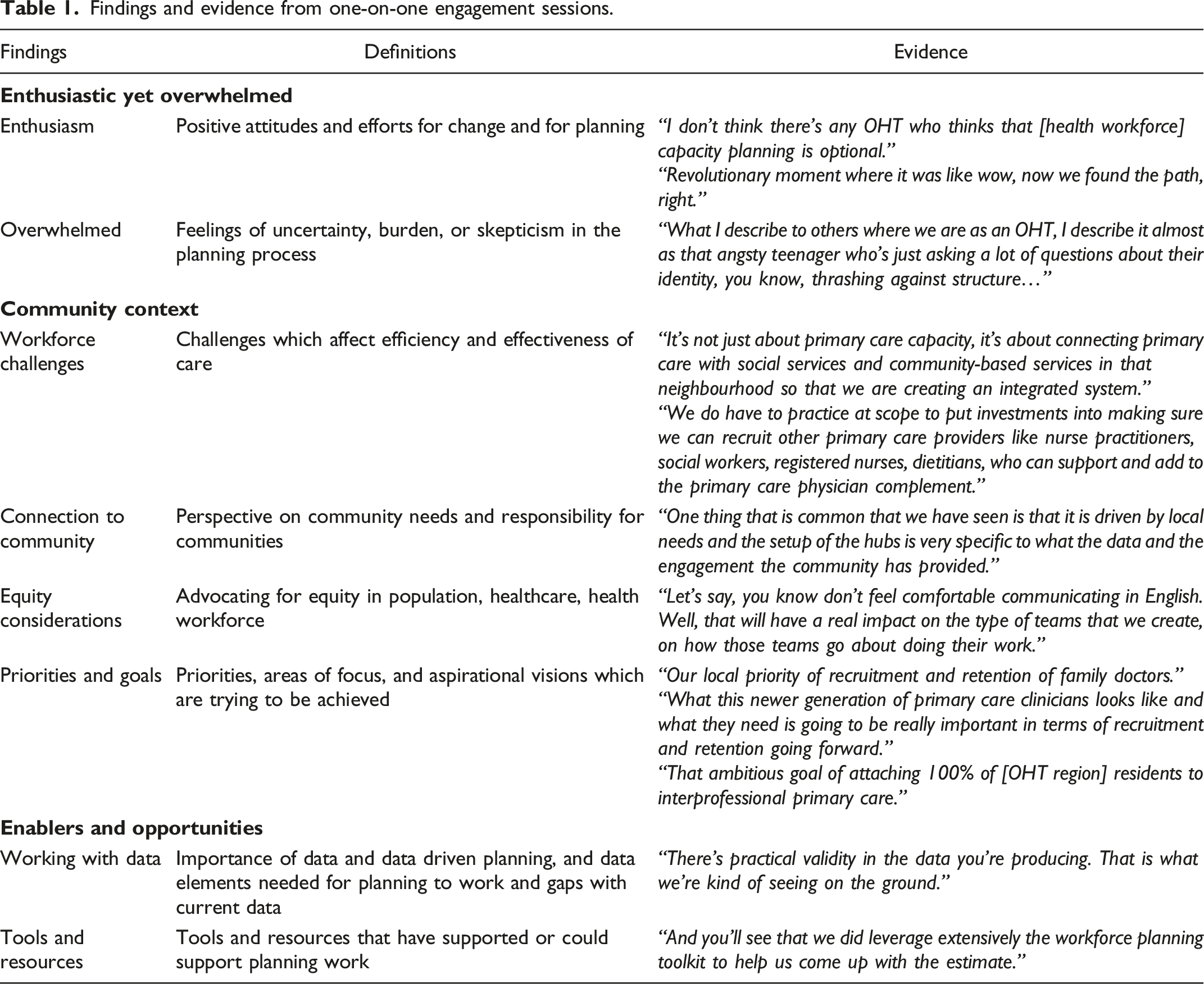
Findings and evidence from one-on-one engagement sessions.
Final “Network of Planners” engagement session: Building capacity for planning
The final session generated spontaneous and relevant conversations between the OHTs and provided an opportunity for OHTs to share innovations as well as barriers, challenges, and plans. Innovations being trialed include community hubs to attract physicians and improve patient access, more resources for unattached patients, social prescribing models for comprehensive care, supporting existing practices to build interprofessional teams, and a focus on proactive support for closing practices. Challenges and barriers cited include funding, lack of resources for planning, physician payment models, and the need to align local community priorities with the regional system.
The evolution of planning at a local level became apparent as participants shared their lessons learned during the engagement process and their plans for moving forward. In addition to expressing appreciation for the engagement and resources shared by our team, they reiterated the usefulness of data and how it has helped them to identify gaps in their communities. Collective advocacy for data and planning was a key focus and there was a shared sense of responsibility and enthusiasm for collaboration with one another and Ontario Health Toronto to ensure a coordinated health system strategy.
Spread and scale of health workforce planning
Findings and evidence from engaging with OHTs for spread and scale of workforce planning.
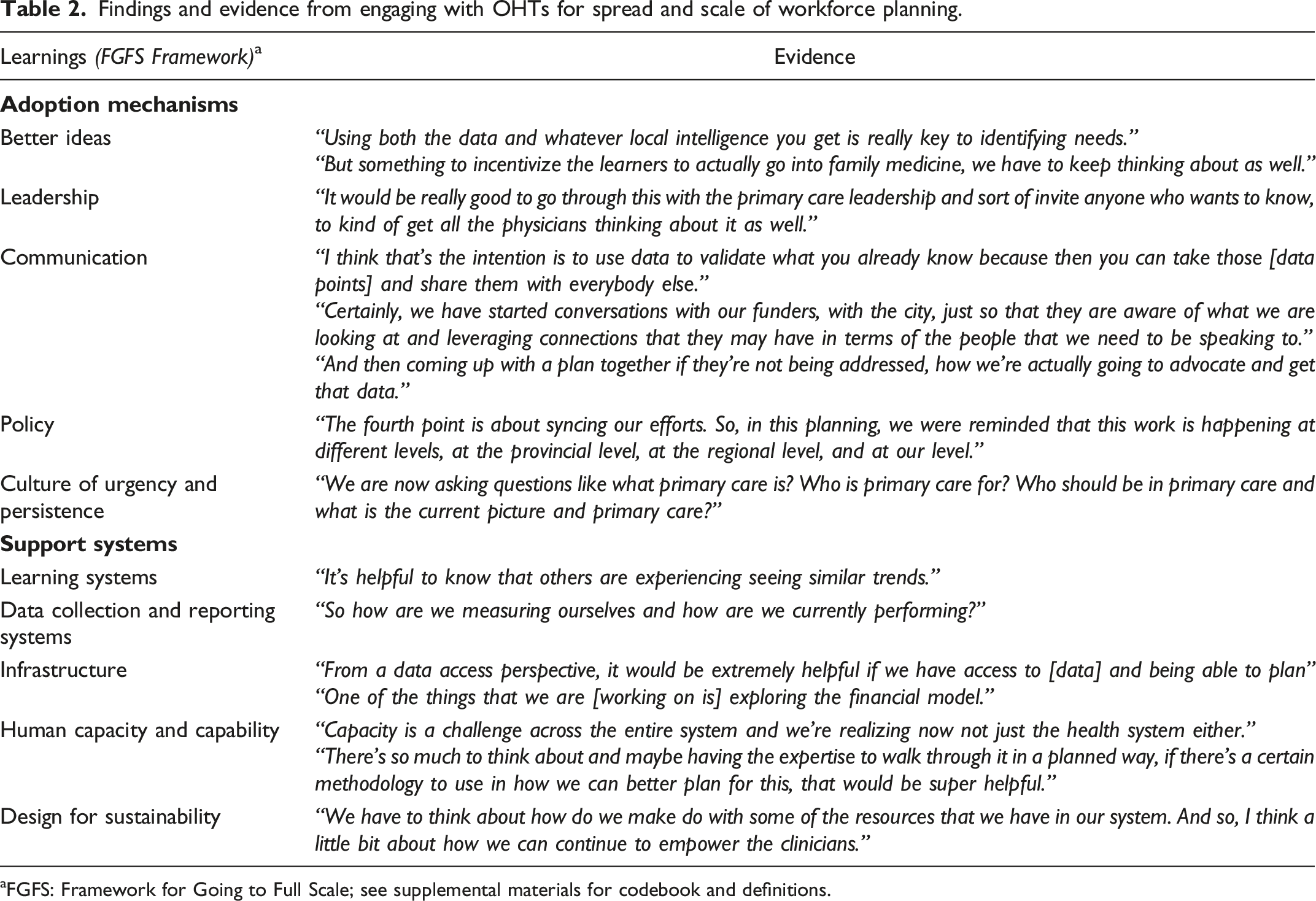
aFGFS: Framework for Going to Full Scale; see supplemental materials for codebook and definitions.
Key lessons learned
Support is needed for planning
Engagement is enthusiastically welcomed by knowledge users—“I’m interested to learn more.” Health leaders are eager for more information to support decision-making and are keen to use data and tools for planning—“we can’t do it without the data, the reports and the toolkit that you have shared with us.” They recognize the benefits of planning to their communities and are willing to invest considerable time (collectively, nearly 200 hours were devoted to primary care planning engagement activities in Toronto during this phase of planning) and energy to learn more. At the regional level, engagement plays an important role in planning by clarifying local planning challenges and providing a foundation for the development and refinement of data supports and other fit-for-purpose resources.
Engagement guides investment
Engagement helps to tailor the support to the context. By giving local knowledge users an opportunity to consider and convey their needs, engagement can inform the tools that are available to support planning and decision-making—“Sometimes, we want to know what we don’t know… if you’ve got a list of potential conditions that you can access the data for, that would be useful.” For example, our customized data packages included information that validated some community and workforce trends while raising questions about others, triggering additional iterative consultation, enhancements to subsequent data offerings, and advocacy for additional and more granular data. An iterative approach to engagement ensures that local needs have been recognized and that learnings have been incorporated into the supports offered.
Engagement strengthens relationships
Iterative engagement strengthens relationships between health system partners—“We’re trying to reframe our thinking, look at all these amazing opportunities for us to work together.” The participants we engaged with were very tuned in to the needs of their communities and our engagement activities created a cascade of additional connections at multiple levels: within individual OHTs, between different OHTs, between OHTs and their partners, as well at a regional level. In our “Network of Planners” session, we witnessed spontaneous collaboration in real time and the sharing of ideas and solutions between previously unconnected parties with common experiences—“your voices all together will be louder than just you on its own.” Stronger relationships foster trust, confidence, and optimism and are essential to the spread and scale of a culture of planning.
Discussion
Health leaders want to use leading practices in planning to improve their local health systems. Engagement provides tailored support for local decision-makers and helps to ensure that they have the resources they need to undertake planning. Feedback from engagement clarifies local priorities and needs and helps to identify gaps in data and tools, which in turn guides investment into remediation of those gaps and efforts to advance broader system change. And finally, engagement strengthens existing relationships and creates new relationships, connecting leaders with planners, analysts, data stewards, and other supports, and ultimately facilitating the spread and scale of a culture of planning.
Engagement can take many forms and should be tailored to the purpose, setting, and the needs of the participants. The modality chosen for engagement should accommodate the intent, whether it is dialogue, priority-setting, knowledge translation, or request for feedback. Having dedicated administrative and coordinating support is an important enabler. The approach to engagement can include email, formal or informal surveys, in-person or virtual sessions, and the provision of individualized support. Ultimately, the results of careful listening should be reflected in the supports, resources, and data that are returned to participants. Building local capacity for planning requires flexibility and responsiveness to local needs and a commitment to iterative engagement.
Health leaders are often asked to do a lot with limited resources, and planning can help to extend the reach and impact of available resources. Providing both conceptual and technical support for workforce planning deepens local commitment to planning and improves confidence and capacity. Engagement leads to the creation of relationships, connections, and networks within local health systems and beyond, and by highlighting challenges that are often representative of needs across the system can have an important impact at scale.
Conclusion
Through our analysis of this case study of primary care planning in Toronto, we have confirmed that partner engagement plays an important role in health workforce planning. Having demonstrated how engagement can be effectively integrated into the work of planning, we expect to continue to leverage our learnings with respect to engagement in subsequent cycles of planning. Building local capacity through engagement with partners represents an important intervention to enhance the impact of health workforce planning within communities and across the health system.
Footnotes
Acknowledgements
We would like to acknowledge the support of Ontario Health Toronto for this work. We also acknowledge the participation of North York Toronto Health Partners, North Toronto Ontario Health Team, East Toronto Health Partners, Mid-West Toronto Ontario Health Team, Bridgepoint Family Health Team, and West Toronto Ontario Health Team. Within these OHTs, the following individuals actively engaged in this project: Edward Aust, Subo Awan, Ryan Banach, Lori Brady, Karen Chu, Jennifer Winter DiCola, Karen Fleming, Kashtin Fitzsimons, Kimberley Hill, Justine Humphries, Susan Joyce, Samantha Kearney, Margery Konan, Kitty Liu, Danielle Manis, Maria Muraca, Tach Murray, Michelle Naimer, Nicole Nitti, Holly Opara, Pauline Pariser, Jeff Powis, Rishma Pradhan, Steve Scott, Neil Shah, Jagger Smith, Anne Wojtak, Ivy Wong, and James Yuan. We would also like to acknowledge the opportunity to be a part of the Team Primary Care initiative; beyond the benefits of funding from this opportunity, we have built long-lasting relationships with individuals and organizations within and outside of primary care.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded under the Team Primary Care: Training for Transformation initiative. Team Primary Care was supported by Employment and Social Development Canada through a grant to the Foundation for Advancing Family Medicine, co-led by the College of Family Physicians of Canada and the Canadian Health Workforce Network.
Ethical approval
This study was approved by the University of Alberta Research Ethics Board (Pro00128443).