
Abstract
Mass casualty events can cause patient surges within healthcare facilities. These surges can be limited to hours or continue for days or weeks. As emergency departments are the front doors to the healthcare system, it is critical that they are prepared to accept patient surges. Focusing plans on optimizing space, staff, and supplies is critical to a successful response. Boarded or non-emergent patients must be diverted, discharged, and decanted from the emergency department to expand resuscitation space. If inadequate, non-clinical space may be required for patient care. Staff call-in lists should be maintained, and in-house berthing for staff during prolonged responses may be necessary. Further, identifying the spectrum of care, from conventional to crisis, is necessary to thrive during a disaster response: staff must understand that business as usual will not be compatible with austere disaster response before levels of care begin to decline.
Introduction
A medical disaster has been traditionally defined as a “catastrophic occurrence, a sudden or major misfortune” which “results in multiple casualties that overwhelm local resources.”1, 2 This means that what constitutes a disaster is directly related to the responding health system’s capacity and will vary widely across systems and time. Since 1990, there have been over 110 discrete events across Canada that have been defined as mass casualty events by the Canadian Disaster Database with five or more injured persons or injuries with at least one fatality. 3 While the aetiology of these events are varied, ranging from natural (land slides, wildfires, floods, and heat events) to man-made (traffic accidents, shootings, and terrorist activity), the result is uniform: injuries, fatalities, and a potential pressure on pre-hospital and hospital systems to respond to the injured.
For most hospital-based health systems, the Emergency Department (ED) is the access point for casualties arriving from a mass casualty event. They must be prepared to absorb significant numbers of casualties in the immediate aftermath of a disaster as the entirety of the hospital system ramps up its disaster response. Optimizing the ED’s surge capacity is critical to patient survivability. 4
When discussing surge capacity, we must consider the three “S” model: space, staff, and supplies.5, 6 Following a review of these concepts and how EDs can optimize surge capacity, attention must be drawn to the notion of the spectrum of care from conventional through contingency to crisis levels and how EDs may require unconventional response to dire circumstances.
Space
Space is often one of the most challenging aspects of surge capacity, as in-patient bed availability across North America has been increasingly poor. 7 Indeed, the United States Health Resources and Human Services Administration recommends that 500 hospital beds per million population above the usual daily staffed bed number be available within 12 hours of a disaster. In many, if not all, jurisdictions in Canada this is presently not possible. 8
To optimize space, the ED must be prepared to divert, discharge, and decant patients in a rapid manner.
Diversion requires liaising with local pre-hospital providers. There should be regular communication between bed management, managers, and clinicians representing hospital and pre-hospital health services to coordinate patient movement. All elective transfers to affected hospitals should be cancelled. Low acuity patients should be diverted to unaffected regional centres where possible. High acuity transfers, for example, regional Intensive Care Unit (ICU) to tertiary ICU, should be delayed. In principle, it is better to have some care at a sub-optimal facility than to receive no care at an ideal facility.
Discharging patients safely and quickly is the second step in expanding surge capacity. It is recommended that departments have a prepared discharge classification system to guide clinicians in the safe discharge of low-risk patients. Formulating a comprehensive system well in advance of a disaster is ideal as this allows for clinicians to make discharge decisions more easily. 9 Patients who are determined to have a <4% risk of serious adverse event should be discharged immediately from the ED. In clinical practice, this may include people who are awaiting low pre-test probability diagnostics, or those with non-critical illness who are being offered symptom control. Patients with 5% or greater risk of a severe adverse event should be transferred to the lowest acuity bed they can safely be housed in during the disaster response. The concept of “reverse triage” has proven to be extremely helpful in opening bed capacity rapidly, especially when extended beyond the emergency department and to in-patient units. 10 This latter aspect can facilitate decanting of patients.
Decanting of patients refers to the rapid movement of patients from the ED to in-patient wards so as to open resuscitative capacity within the ED itself. Decanting patients requires a commitment from all in-patient services to respond during a disaster. This should be codified in a policy or memorandum of understanding between the departments and hospital leadership so that, when the time comes, there is no room for debate: when seconds matter, minutes count. A viable but succinct handover pathway must exist for nursing staff, and patient movement from ED to in-patient unit should be facilitated by any able-bodied person who is not required for immediate clinical use. Consider patient care attendants, housekeeping staff, and other non-clinicians for this task.
It is likely that discharge, diversion, and decanting will not open enough beds rapidly enough or in enough numbers to fully accommodate a mass casualty disaster. In this case, expansion of clinical space will be required. For the walking wounded, areas with ample seating can be used as aid stations: consider internal waiting rooms for larger departments such as radiology or cardiology. Often, orthopaedic or minor procedure clinics can offer ample space for non-ambulatory patients and provide access to limited surgical lighting and medical air/oxygen. In dire scenarios, any open spaces—theatres, cafeterias—can be transformed into care areas. All these expanded areas, however, are nothing without the clinical expertise to staff them.
Staff
Staffing during disasters presents a problem unto itself. Evidence of employee absenteeism rates is sparse. Theoretical surveys suggest that between 8-15% and 22-30% of clinical staff may not respond to work during disaster events.11, 12 In events where hospitals and staffs’ homes are directly affected, as in the 1995 Hanshin-Awaji earthquake, only 58.4% of the doctors, 44.2% of the nurses, and 31.0% of the clerical employees were able to reach the hospital. 13 Similarly, following the Fukushima tsunami in 2011, upwards of 52% of physician and nursing staff were unable to work, and these shortages persisted to a lesser degree for more than 12 months following the initial disaster. 14 A systematic review of willingness-to-respond studies found that both perceived risk to self and care of family (elder care, child care, and pet care) played large roles in overall willingness-to-respond. 15 Addressing these issues prior to a disaster will be critical in ensuring adequate staffing.
Mechanisms for optimizing available staff include call-in lists, automated call-in software, dedicated staff berthing, and emergency child care facilities. Call-in lists, ideally automated and redundant (phone, SMS, and e-mail) should be a key component of your ED’s disaster plan. Being able to offload the role of calling in staff to automated software is important, as it can take considerable time to make phone calls during a disaster. Ensuring there is berthing available to staff can allow for staff to stay on site during prolonged disasters, augmenting staff levels and reducing staff injury by reducing commuting in disaster zones. Similarly, having emergency child care available to staff on-site would mitigate the most common concern held by clinical staff during disasters. 16
Mobilized staff should have a known location to report to, rather than haphazardly arriving in the department. Incident commanders and operational section chiefs must be aware of the human resources they have at any given time. Schedules should be shifted from 8 hour to 12-hour shifts, with an operational period being every 12 to 24 hours. As the surge reaches its natural rise and fall, and the situation becomes more controllable, it is important to demobilize staff as soon as possible. Rest is necessary to allow fresh staff to return to work when the disaster is over.
Supplies
Since the 1990s, many hospitals have come to rely on “Just In Time” (JIT) supply chain systems, and do not maintain large stockpiles of medication, intravenous fluids, consumable wound dressings, or antidotes on site.17, 18 While this is financially ideal during normal operations, during disasters it can be problematic. 19 It is important that healthcare facilities have adequate tracking of their supplies, so that bottleneck losses can be predicted during a crisis.
Based on an estimated patient surge, a hospital system should be able to calculate how many hours supplies will last and which supplies will run out first, effectively creating a care bottleneck. 20 Consider involving your blood bank in these discussions as well as this will assist in predicting how many units may be realistically available in the immediate aftermath of a disaster. Once your bottlenecks have been identified, action can be taken to mitigate this through alternate supply chain processes.
Suturing trays and dressing material can be the first supplies overwhelmed when dealing with mass traumatic casualty events. It is wise to consider even a meager stockpile of sterile trays and dressings that can rotate into general supply near expiry cycles. This stockpile can, at least, alleviate up front bottlenecks. Considerations should be made to sterilization of surgical equipment in the case of casualty need outpacing sterile-processing capacity. Evidence has shown that simple chlorhexidine cleaning is non-inferior, and contingency plans should be discussed with your infection prevention and control groups 21 ; ensure you have an agreed upon contingency so that your ED can recycle surgical trays in austere environments.
Drug stockpiles are more challenging, and loss can be costly for health systems due to supply expiry. 22 For toxicological or CRBNE (chemical/radiological/biological/nuclear/explosive) disasters, regional stockpiles can offer a more economic and efficient option.23, 24 Ensure that your pharmacy representatives are involved in disaster planning to determine where bottlenecks may occur during response.
Conventional, contingency, and crisis care
During large patient surges associated with disasters, it may become impossible to provide a conventional standard of care to all patients.
25
Figure 1 outlines the commonly understood definitions of this spectrum of care. The spectrum of care.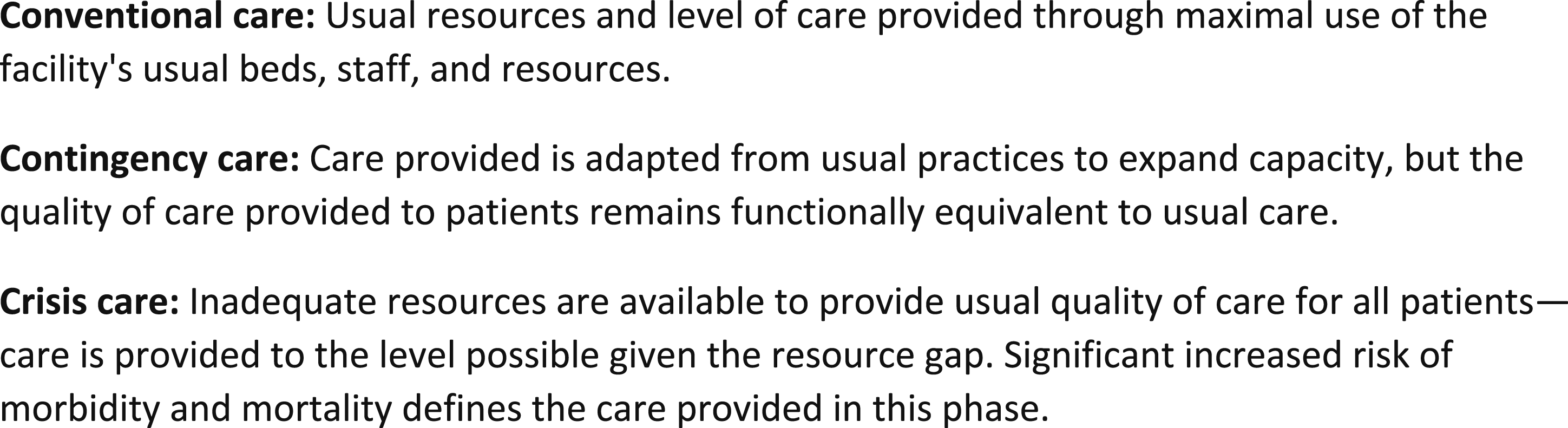
It is important to ensure that ED staff, clinical and non-clinical, understand the gravity of disasters and mass casualty medicine. There may be deaths that occur in volumes generally unacceptable in conventional medicine; patients may suffer without appropriate medications in inappropriate parts of the hospital, cared for by underqualified staff.
Following initial triage, victims in mass casualty events undergo SAVE triage. SAVE, or Secondary Assessment of Victim Endpoint, asks clinicians to decide if the patient will survive regardless of intervention, die regardless of intervention, or require intervention to be saved. As resources become increasingly sparse during prolonged patient surges and catastrophic disasters, decisions must be made over who is, effectively, worth the treatment that you have given a rationed supply. 26
The experience during the COVID pandemic has forced many health systems worldwide to negotiate these issues; to date there is no consensus on exactly how patients should be triaged in extreme circumstances, and that triage sieves may differ depending on the care resource required and the specifics of the disaster.27, 28 It is important that your hospital ethicists be involved in the planning for mass casualty disasters and patient surges, so that all care providers from the ED to the Operating Room (OR) to the ICU are on the same page. Preparing your staff for these decisions is also important as discussing it in advance will make doing it in the moment much easier psychologically.
Having a plan to respond to surges of patients is the most important first step in mitigating the potentially catastrophic consequences of disaster. Ensuring optimal space, staff, and supplies should allow your department to provide the best care possible from conventional to crisis levels.
First steps for your health system
The challenges of adequate staffing, supplies, and clinical space in an already pressured system are rapidly exacerbated by patient surge and the limitations of contingency and crisis care; being at the helm of emergency preparedness within healthcare is often an unenviable position. Priorities will be addressing the “S” factors as efficiently as possible so that some contingency exists in the event of a disaster.
First and foremost, you will need a reliable ability to call-in additional staff. Whether your organization is small enough for a simple call-out list to work or your health system requires a third-party automated application, having access to surge staff is the critical substrate to any disaster response.
Your second priority is securing clinical space. Agreements regarding other clinical and non-clinical spaces must be established so that access is seamless during a disaster. For example, if you plan to expand into an out-patient clinic, ensure there is a rapid process to clear patient appointments or offload those out-patients to a secondary site. Attempting to negotiate access during a disaster wastes time and goodwill between care providers.
Finally, address the bottlenecks in your supply chain and ensure that you have rotating surge supplies in your circulation cycle. This additional redundancy will mitigate any slowdown in care during contingency and crisis situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.