
Abstract
This article outlines the findings of a study that looked at the self-management needs of Chronic Obstructive Pulmonary Disease (COPD) patients and the feasibility of an eHealth intervention. This study found that patient self-monitoring is sub-optimal. Patients want the technology to include record keeping, feedback, the integration of biomedical and environmental data, exacerbation detection, and the ability to connect with providers. Health leaders could benefit from this information by working with their suppliers to eliminate system and technology barriers, and ensuring that technology is interactive, personalized and easy to use.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) has the highest prevalence in three Canadian Maritime Provinces (MPs). 1 Health authorities across these provinces are focusing on managing COPD in Community-Based Primary Care (CBPC) facilities, such as the Fredericton Downtown Community Health Centre (FDCHC) 2 in New Brunswick (NB). FDCHC follows a collaborative practice model with a multidisciplinary team of Primary Healthcare Providers (PCPs) providing care to vulnerable populations. There are numerous challenges at patient, provider, and system levels that influence the capacity of PCP teams to provide care.3,4 A variety of technological advances in mobile health, sensors/wearables, automated data capturing, and feedback formats5,6 hold promise for optimizing COPD management in CBPC settings such as FDCHC. The long-term goal of this research is to help patients with COPD and providers to optimize the use of technological advancements, specifically to help reduce the gap between onset of COPD exacerbation and triage by PCP. This paper outlines the first step toward achieving this goal and presents the results from a qualitative pilot study performed at the FDCHC with aims to (i) understand the Self-Management (SM) and patient care needs of the COPD patients and their PCP and (ii) ascertain specifications and the feasibility of an eHealth intervention for COPD management. A particular focus of this research was to identify the most optimal pathway for integration of interventions in COPD patients’ daily lives to help predict and treat exacerbations. We expect that early detection of possible exacerbation through technology can potentially allow patients triaged and optimally cared for by the PCP at the FDCHC and might pre-empt emergency department visits and admissions to acute care.
Methods
A qualitative descriptive design encompassing two separate Focus Group (FG) sessions for patients and providers was used. Three Theoretical Frameworks (TFs) were used to develop the two moderator guides: (i) Chronic Care Model 7 to include aspects related to chronic disease management; (ii) Bandura’s Social Cognitive Theory 8 to include personal, behavioural, and environmental factors related to health behaviour; and (iii) Nielson Usability Heuristics 9 to help understand end-users’ usability needs for COPD software. The TFs guided data collection and analysis and provided broader understanding of the most common and critical personal, behavioural, and technology-related issues needing to be addressed for optimal technology development. Content validity of the guides was established by reviewing relevant literature and through critique, modification, and consensus by the experts on the team. Purposive sampling was used to identify two FG cohorts: (i) patients with COPD (n = 8) and COPD care providers (n = 4). The target patient population included all English-speaking FDCHC COPD patients enrolled in UPSTREAM 10 and INSPIRED 11 programs and their providers. Focus group sessions were held at the FDCHC, where a co-moderator and a research assistant were physically present, while the other moderator, because of COVID-19 restrictions, was in Halifax, and conducted the FG remotely through Zoom. Each participant was asked to complete a demographic questionnaire. During the patient session, a brief (5 minute) demonstration of a commercial mobile app “COPD manager” 12 was played on the projector. The app includes limited functionalities such as daily journals, feedback in the form of charts, and reminders. The demonstration was included to encourage meaningful discussion about the potential use and features of a COPD technology.
Data analysis
Audio files and field notes from the two focus group sessions were uploaded to ATLAS.Ti software. Thematic analysis 13 was used to analyze the data. Open codes assigned to the quotations were further classified into axial codes based on commonalities. Validation of the codes was performed by continual referral back to the original data. The data was analyzed by two researchers. Any discrepancies in the results were resolved through discussion and consensus before codes were finalized. Descriptive analysis was performed on the quantitative data.
Results
Quantitative results
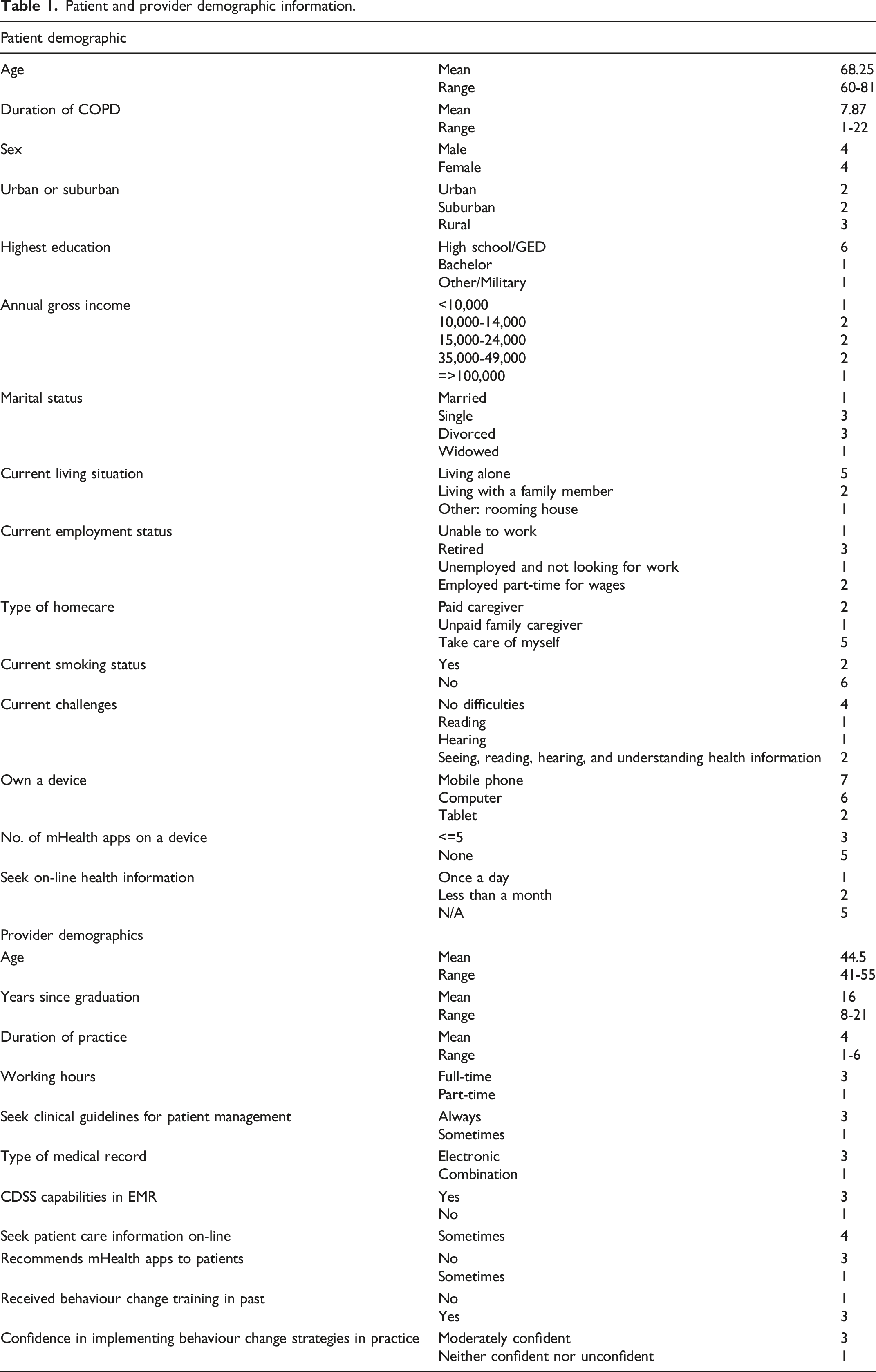
The patient sample is predominately White, elderly with a mean age of 68.25 years, balanced in terms of sex and a good mix of urban, suburban, and rural. Most patients have access to computers and mobile phones and are generally comfortable using technology (Figure 1). The provider sample included four female PCPs: two Respiratory Therapists and two Registered Nurses, with three PCPs working full-time, with mean duration of practice of 4 years. The sample, largely moderately confident in implementing Behaviour Change (BC) strategies, received BC training in the past. Demographics are displayed in Table 1. Patients’ comfort level with use of computer, mobile phone, and tablet. Patient and provider demographic information.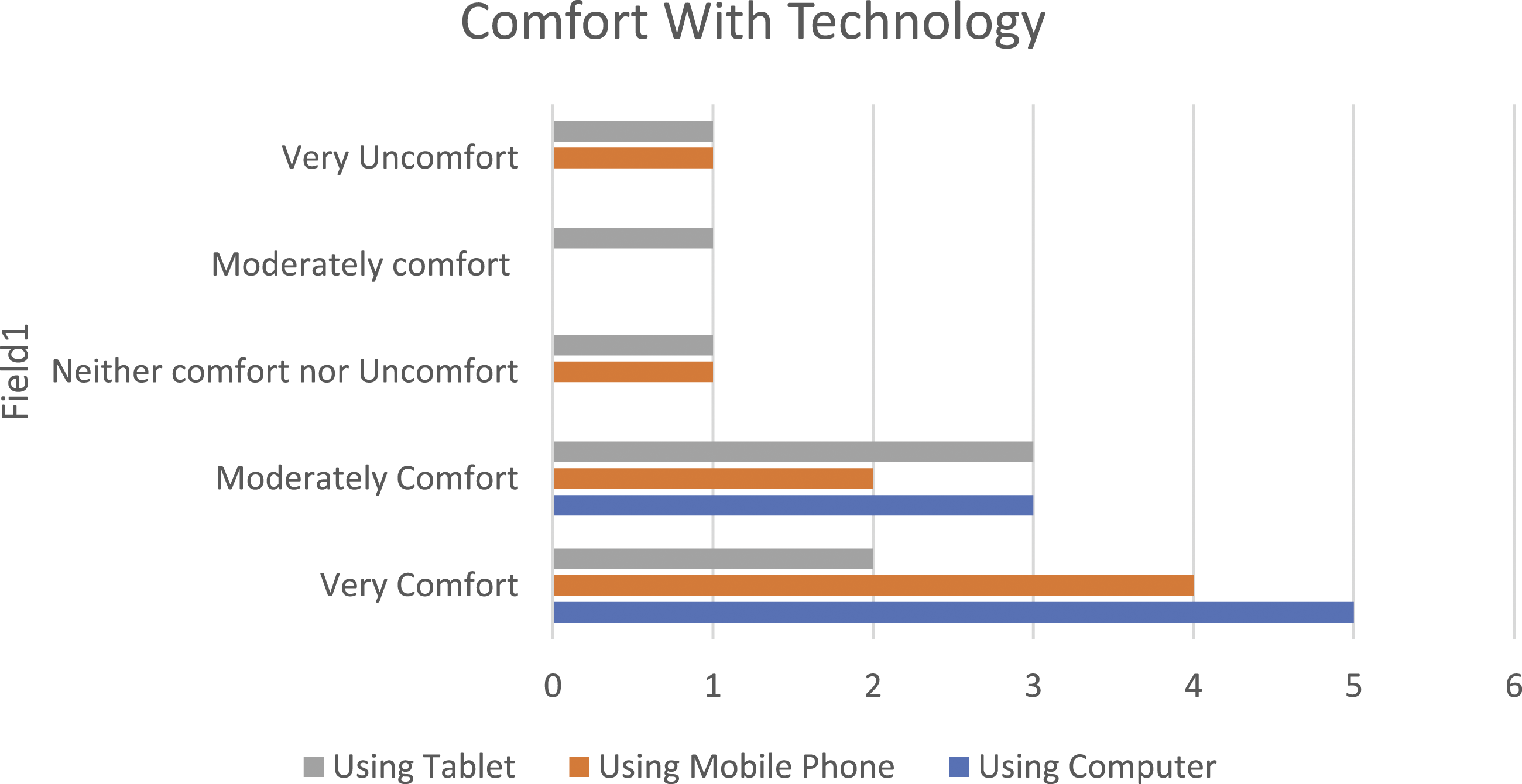
Qualitative results
A total of 318 quotations were included in the final analysis, with 225 patient quotations and 93 provider quotations. Overall, 104 open codes were assigned to the patient quotations and 57 to the provider quotations. The open codes were then classified into 31 axial categories based on commonalities. Patient data included 24 axial categories and provider data included 7 axial categories. The 31 axial categories were constantly compared against the categories based on the unstructured questionnaire in the protocol. Categorization based on patient data is depicted in Figure 2 and discussed as follows. Patient focus group data analysis and categorization. The figure 2 depicts 24 axial categories in the patient data being assigned to 9 high-level categories based on the patient focus group questionnaire.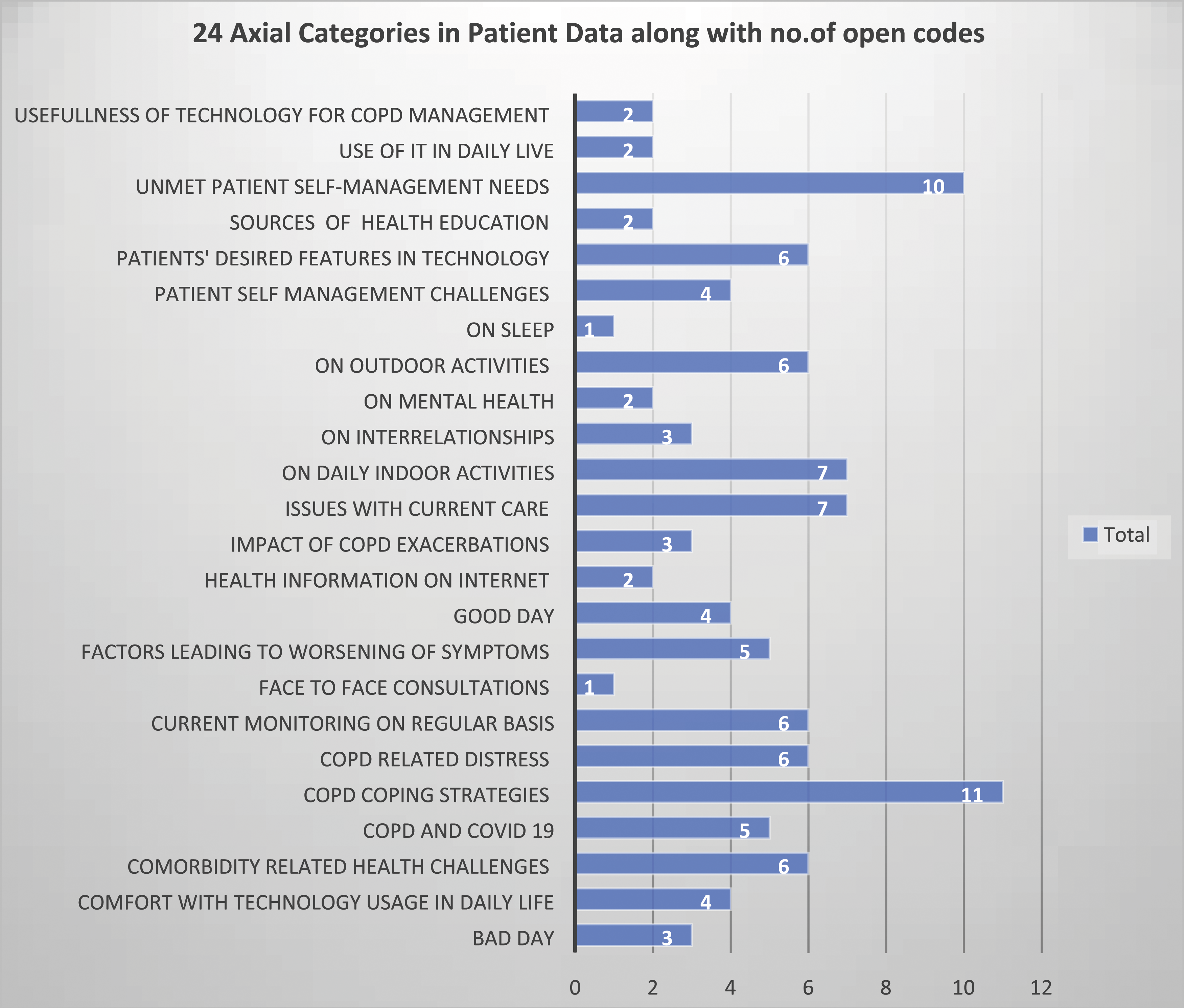
Patients’ perspectives
Effects of chronic obstructive pulmonary disease on daily living
A good day for most of patients is described as the ability to perform preferred daily indoor and outdoor activities, have a good night’s sleep, and to control one’s symptoms, including anxiety. A bad day constituted prolonged breathlessness and wheezing, being listless, sleepless, helpless, and wanting to isolate. This distress is articulated as fear of being drowned, trapped indoors, losing control, and resigning to one’s inability to perform daily activities: “it is like, my lungs are always soaked. Yeah, I feel like I'm drowning all the time.”
The participants reported extreme sensitivity to household cleaning products and cosmetic sprays like perfumes and hairspray, even entering a pharmacy through the cosmetic section could trigger an exacerbation, as well as prolonged physical activity, humidity, extreme temperatures, and poor air quality. COPD and exacerbations have adverse impact on (i) daily activities, for example, cooking, cleaning, grocery shopping, and putting garbage bin out; (ii) interrelationships especially with family caregivers, leaving them feeling guilty and burdensome; (iii) mental health, for example, anxiety and depression; (iv) sleep quality; (v) ability to hold conversation; and (vi) cognitive issues. One patient remarked: “Sometimes with COPD, you get a flare up and then you get lightheaded…So, you're not thinking clearly and might even snap at the wife or one of the kids when they come in for a visit…”
Participants feel greater vulnerability during the COVID-19 pandemic. Unable to go out as much, they feel stuck at home, and unable to interact with others. They find it difficult to breathe through a mask and having to stand in a queue to enter a store.
Current self-management of chronic obstructive pulmonary disease
Participants have developed various coping strategies, for example, healthy eating, indoor/outdoor physical activity, cannabis usage, yoga, mindfulness, breathing through nose, use of mouth covering, and planning their activities ahead of time. While data indicates some self-monitoring of blood pressure, exercise, oxygen level, and heart rate, fewer quotations associated with these open codes indicate relatively weak evidence of self-monitoring. The devices used for monitoring ranges from electronic devices, for example, oximeter and blood pressure device, to exercise monitoring via paper calendar: “Measuring of oxygen concentration, for example, I have a unit that I put on my finger when I work out, and so forth… as a measurement of where I am in terms of exercise, and how quickly am I recovering.”
Self-management support
Some participants find health education useful in improving their SM practices, for example, monitoring and recognizing symptoms, and breathing exercises. Main information source includes courses at FDCHC. Few participants actively sought information from health magazines or web sites. Most participants have reservations about the accuracy of health information on Internet and believe it should be validated by PCP.
Current care of chronic obstructive pulmonary disease
Most participants are frustrated about not being able to gauge if they are getting better or worse between clinical visits and believe that medication management and symptom monitoring are suboptimal. Some even feel invalidated by their providers. They suggest having a record of what transpired on a regular basis, tracking their symptoms, and communicating that record with providers during visits will help improve communicating challenges. They find it difficult to navigate the healthcare system and multiple providers, especially patients with comorbidities.
Patient self-management challenges
Most participants struggle to understand their symptoms or their origins and find medication adherence challenging, with major SM gaps being inability to effectively communicate daily struggles with providers: “Because when you got 1,000 questions, when you go to the doctor, and when you get there, you ask one question. And then you forget everything else you're going to ask. And then once you're in the car halfway home, you go, I was going to tell her whatever ...” Many participants have comorbidities, for example, sleep apnoea, stroke, multiple sclerosis, and Crohn’s disease that further complicate COPD-related challenges.
Current use of technology
More participants use mobile phones rather than tablets and computers. They use technology for simple recreational activities, for example to play games, read books, or web surfing. Few participants use health apps or seek on‐line health information. Some participants indicated use of Digital Assistants (DAs) for setting alarms, calendars, reminders, agendas, and switching lights on and off. One patient noted: “I've invested in Google Home, and I rely on that for everything. I can set timers alarms, everything like that…and if I don't remember what it's for, I can say okay what's that alarm for?” Most participants believe they are not particularly technically savvy.
Perspectives on self-management technology
Generally, patients appreciate the pervasive and portable nature of mobile and sensor technology and believe that features such as library, record keeping, feedback, guidance, integration of biomedical and environmental data, detection of triggers for exacerbation, and ability to communicate these with PCP during visits can be very useful in helping overcome many of the SM challenges. One patient noted: “It would be very interesting to see a technology that had a combination of library and record keeping. So, for example, that if I were looking for something like for diet, are there items that I should probably be staying away from, because it affects my breathing …..” Participants believe that a technology should not replace in-person consultations with providers.
Providers’ perspectives
Current management of patients with chronic obstructive pulmonary disease
Most providers have extremely busy days and the most challenging aspect of COPD management is dealing with socioeconomic issues that compound health problems, for example, lack of drug coverage, resources at home, or patient without a PCP and in need of medications without a prescription: “When you get the complicated patients who don't have drug coverage who don't have the resources at home, or don't have a, you know, a provider … that makes for a busy day.”
Self-management resources for patients
Providers sometimes recommend credible web sites and YouTube videos related to COPD self-care, physical activity, and mental health issues.
Usefulness of technology for chronic obstructive pulmonary disease self-management
While providers see the benefits of SM technology, they also identified numerous patient-, information technology-, provider-, and system-related barriers to its usage. The patient-related barriers include sociodemographic factors including low literacy, poverty, old age, cognitive decline, patients’ low efficacy, and motivation. Technology-related barriers include access to Internet and smart devices; setting up technology at patients’ homes; low digital literacy; and technology acceptance. One patient suggested: “Every time I look at those web sites with any of my patients, and usually it's when we've been in person, and I just say, well, you know, you go home and do this, I realize that 95% of the time, they probably aren't.”
Provider-related barriers include the onerous addition of new technology to an already busy day, causing potentially burdensome and constant communication with patients. System-related barriers include needing constant information technology, support for patients and providers, possible patient perception about replacement of in-person care by the new technology, and compromising care quality. Nevertheless, providers believe that good design and proper training might be useful for some patients, for example, in rural communities, with accessibility issues due to weather or transport, at the time of diagnosis, or to debunk misinformation.
Desired features in chronic obstructive pulmonary disease self-management technology
Providers recommend that technology should be interactive, non-intimidating, and easy to use, for example, simple language and navigation and even use of humour. Other desirable features include gaming and rewards, graphics, voice activated record keeping, and feedback and reminders. The action plans should be personalized based on sociodemographics, disease stage, comorbidities, and patient readiness.
Discussion
Our data indicate relatively weak evidence of regular and consistent self-monitoring. One of the major gaps is the inability of patients to effectively communicate daily struggles with providers. Most patients use mobile phones for communication and recreational activities and voice activated DA for daily routines but are not necessarily technically adept. Providers believe the addition of new technology to already busy days might cause burdensome, constant communication with patients. COPD eHealth interventions of various types and intensity, for example, medication adherence, symptom trackers, educational, and counselling have been developed with mixed results in effectiveness. 14 This research is in line with national self-care strategy 15 that calls for delivery of innovative, personalized, and easy to use self-care programs to build health promotion and disease prevention into practice. Our study highlights a need for a comprehensive easy to use framework that combine interventions that (i) predict/detect an exacerbation episode via monitoring of physiological parameter and contextualizing them with various environmental and personal triggers; (ii) provide feedback in the form of easy-to-understand visualizations that patient can communicate with the PCP during visits; and (iii) use voice activation, graphics, gaming, and information personalization for delivering COPD action plans. The advances in mobile technology, wearables/sensors, data analytics, and visualization have made it possible to capture and analyze data in real time to monitor symptoms, detect a possible exacerbation, and track behaviours. Involvement of patients and providers is necessary to build trust in an intervention. The theoretical frameworks used for data collection ensured that the important predictors of SM and technology adoption are accounted for. This is an exploratory study with a small, English-speaking, White sample. All participating patients and providers are from FDCHC. It is possible individuals interested in technology were more likely to participate compared with the wider population of patients and providers. Consequently, the study may have self-selection bias. Inter-rater reliability between two researchers during data analysis and interpretation ensured the scientific rigour. During the short visits, critical decisions are made based on reconstruction of events from patients’ memory and pieces of incomplete data about patients’ concerns. Policy-makers and researchers should place emphasis on systematic investigation of use of pervasive data collection and tailored self-management technologies. However, not all patients will have cognitive or emotional abilities to self-manage to the same degree and flexible plans with or without technology might be needed. In future, the results of this study will be used to design and test an intelligent, adaptable, and easy to use self-management intervention for patients with COPD.
Conclusions
Patients’ desired features in technology include library, record keeping, feedback, guidance, integration of biomedical and environmental data, exacerbation detection, and improving PCP communication. Providers identified patient-, provider-, system-, and IT-related barriers to the technology usage, recommending technology to be interactive, user-friendly, and individualized.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UNB University Research Fund Competition 2020 (RF Explore).
Ethical approval
Ethics approval was obtained from Horizon Health REB (NB) and Dalhousie REB (NS).