
Abstract
The Senior Friendly Hospital Accelerating Change Together in Ontario program linked the Collaborative Network Model and the Senior Friendly Hospital Framework in a unique multi-hospital knowledge-to-practice initiative to improve care for hospitalized older adults. The design enabled teams from 78 Ontario hospitals to close a shared skills and knowledge gap while meeting the varied needs of their diverse contexts. Results suggest that this design meant to reduce unnecessary redundancy, while preserving requisite diversity, was successful in achieving its specific objectives: to build a collaborative network and increase the confidence, knowledge, and skills of its members sufficient to lead sustainable improvements in their unique hospital settings. Findings with special relevance to process improvement specialists, health system leaders, and hospital administrators and managers are discussed.
Introduction
Hospitals can be “unfriendly” to older adults. Contributing factors include inappropriate environmental design,1-3 ageist attitudes,4-7 clinical processes compromised by lack of knowledge,8,9 and overestimations of competence.10,11 As a result, hospitalized older adults, especially those with frailty, have longer lengths of stay and are at heightened risk of hospital-acquired complications12-14 including delirium, 15 functional decline,16,17 adverse drug events, 18 injuries from falls, pressure ulcers, 19 post-operative complications,20,21 and malnutrition. 22
The Senior Friendly Hospital (SFH) Framework developed by the network of Regional Geriatric Programs in Ontario provides a blueprint to help hospital managers and staff optimize health outcomes for seniors. The framework guides users to consider 5 domains when implementing improvement processes: processes of care, organizational support, emotional & behavioural environment, ethics in clinical care and research, and the physical environment. The framework served as the foundation for a system-wide survey of senior friendly care practices in all of Ontario Canada’s publicly funded, non-paediatric hospitals. 23
Survey responses suggested a readiness to improve senior friendly care that was tempered by a recognized obstacle to practice improvement24-26—a gap between the clinical skills of staff and those skills needed to lead Quality Improvement (QI). The survey also revealed that needs varied across the respondents diverse environments which ranged from small rural hospitals to large urban science centres. To build on this readiness, an intervention was needed that would reduce unnecessary redundancy in closing a skills and knowledge gap while preserving the contextual diversity of each hospital’s needs to minimize reactance to change.27-29
From among the range of theories, models, and strategies29-33 that have emerged to guide practice improvement in healthcare settings, the Collaborative Network Model (CNM) has been frequently used.33,34 The model’s fundamental features include: convening teams across multiple organizations to implement a specific intervention with common metrics; learning from experts and each other; and receiving support from organizational leaders and coaches. Systematic reviews of CNM interventions across many clinical settings have reported encouraging results 35 including its use in improving care for seniors.36-38 The CNM promised a solution to avoiding redundancy—teams could learn about the SFH Framework, QI, and leadership skills while implementing improvements together.
The SFH Framework promised a solution to the challenge of satisfying each hospital’s diverse needs. The framework was designed to guide improvements in the care of older adults across a hospital’s varied clinical environments and the “processes of care” domain, encompasses the variety of guidelines to meet their clinical needs. Using the SFH Framework, participants could select a practice improvement to suit their specific need.
Could a system-wide intervention guided by the CNM and the SFH Framework help build the skills and knowledge of teams to implement more senior friendly care despite each team’s specific needs? This was an overarching question for the Senior Friendly Hospital Accelerating Change Together in Ontario (SFH ACTION) program, a complex multi-hospital knowledge-to-practice initiative including specific objectives: 1) build an interorganizational collaborative network; 2) increase team confidence in using the SFH Framework and leading practice change; 3) implement practice improvements; and 4) sustain interventions.
Methods
The Standards for Quality Improvement Reporting Excellence (SQUIRE) 2.0 39 were used to prepare this article. SQUIRE guidelines provide a standardized but adaptable framework for reporting knowledge about how to improve healthcare.
Intervention
The SFH ACTION program engaged teams from two cohorts of hospitals in a process comprising preparation, a 3-day knowledge transfer and exchange workshop, 9 months of coached implementation, and a second 1-day workshop. Cohort 1 teams were invited to continue their participation during cohort 2’s timeframe.
CEOs of Ontario’s 145 non-paediatric publicly funded hospitals received a letter inviting their hospital’s participation. Interested hospitals nominated clinical, support or administrative staff, patients, and caregivers to form their implementation team and identified an executive sponsor and an improvement goal. Cohort assignment was based on order of acceptance.
The knowledge transfer and exchange workshops employed multiple methods including expert lectures, practice-based experiential learning, team-building exercises, small group problem solving, just-in-time surveying and prioritizing, peer-to-peer storytelling, poster presentations, and celebrations of achievement. Expert lectures were delivered by topic-based local and international leaders including patients, caregivers, clinicians, academics, and politicians. Topics included the SFH Framework, team development, change leadership, and QI methodologies including writing aim statements, cause and effect analysis, process mapping, plan-do-study-act cycles, data collection and analysis, and stakeholder engagement.
During implementation, coaches skilled in the use of the SFH Framework, QI, continuing health professional education, knowledge-to-practice processes, and clinical geriatrics, were available to the teams. Coaches provided support during workshops, responded to requests for assistance with emergent needs, monitored team progress, provided feedback on monthly reports, and facilitated regular educational webinars.
The program also provided a web-based portal comprising an array of shared resources including: project management and QI tools and templates, SFH Framework materials, and resources developed or used by the teams.
Measures
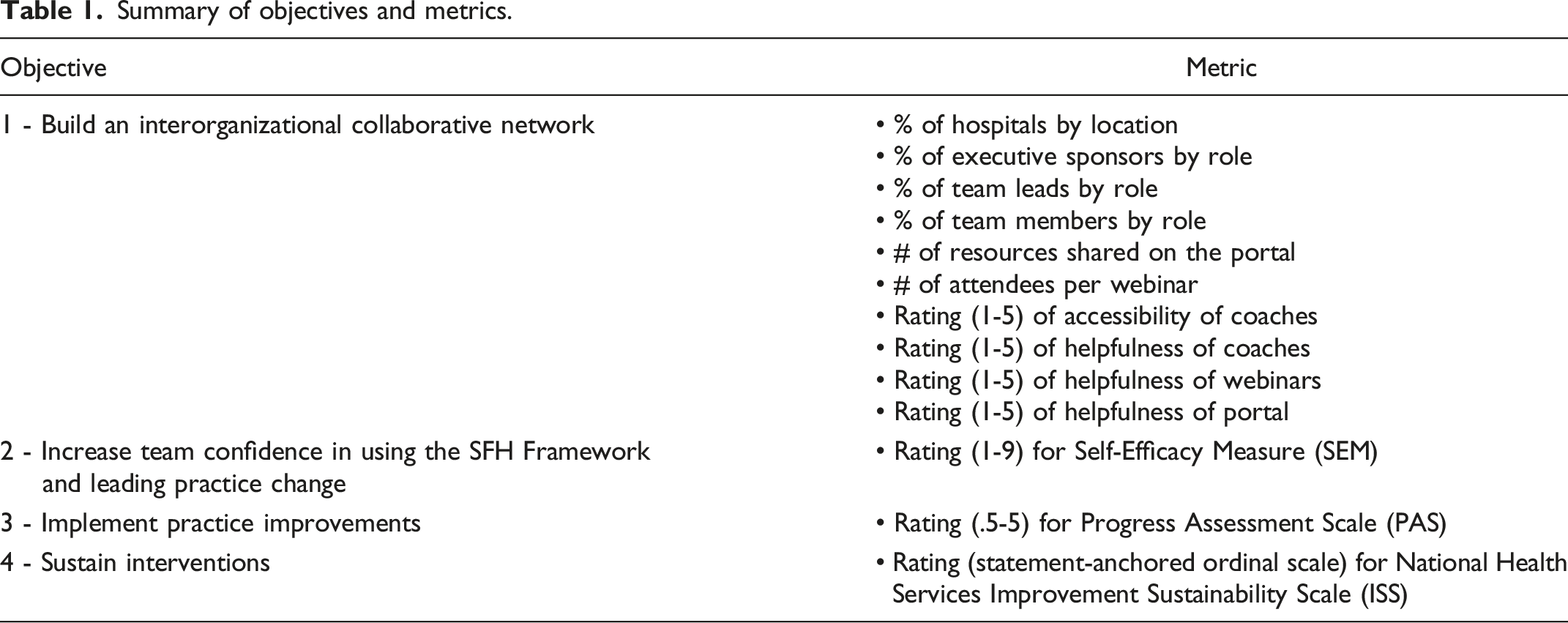
The program evaluated metrics for four objectives (Table 1).
Objective 1: Build an interorganizational collaborative network measures included the characteristics of participating hospitals and team members, number of resources shared on the portal, number of webinar attendees, rating of accessibility of coaches, and ratings of helpfulness for webinars, coaches, and portal.
Summary of objectives and metrics.
Mean team confidence.
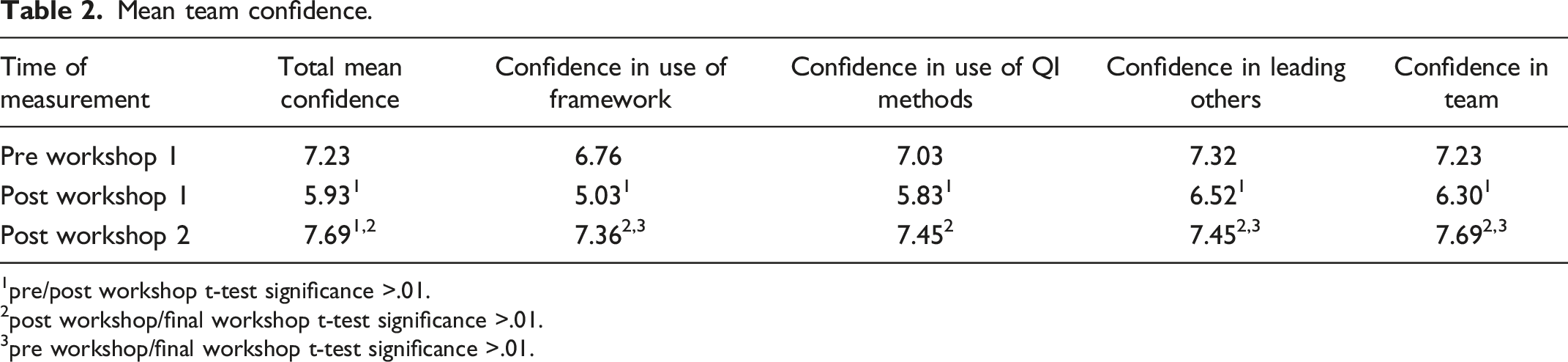
1pre/post workshop t-test significance >.01.
2post workshop/final workshop t-test significance >.01.
3pre workshop/final workshop t-test significance >.01.
Mean quarterly progress assessment scores (PAS).
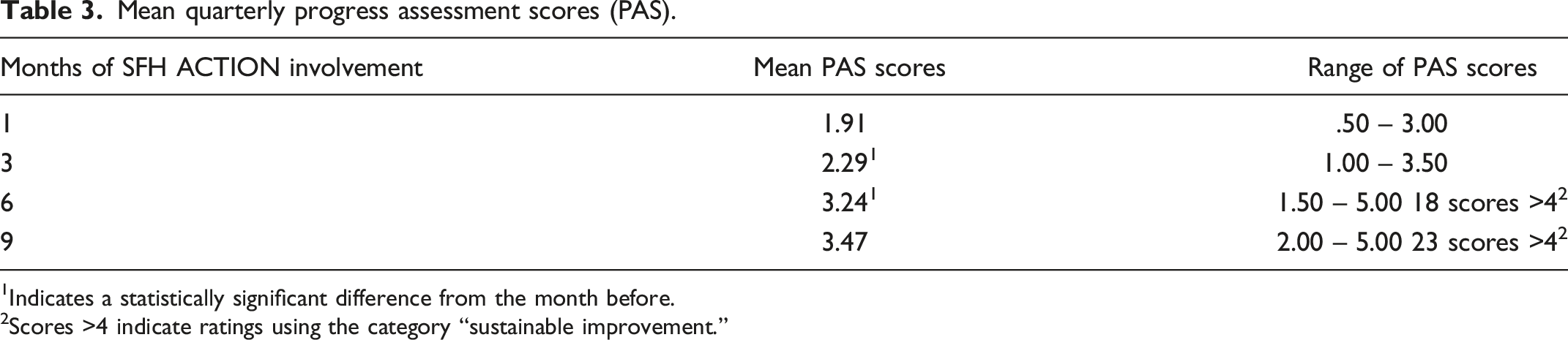
1Indicates a statistically significant difference from the month before.
2Scores >4 indicate ratings using the category “sustainable improvement.”
Mean improvement sustainability scale (ISS) scores.

Analysis
Data analytics used the GNU PSPP program release 1.4.1; a software program for statistical analysis of sampled data, which included descriptive statistics of data for objective 1 along with internal consistencies, correlational analysis and pre-post t-tests for data from the SEM, PAS, and ISS measures.
Results
Objective 1: Build an interorganizational collaborative network
Seventy-eight of the 88 enrolled community, teaching and rehabilitation hospitals completed program participation by submitting the required data. The 78 participating hospitals represent 54% (78/145) of Ontario’s 145 non-paediatric public hospitals and 62% of its in-patient beds. The number of beds in participating hospitals ranged from 13 to 1,337. Forty-eight (62%) identified as rural and 30 (38%) as urban. Executive sponsors for the initiative comprised CEOs (17%), CNOs (45%), VPs (20%), and program directors (18%). Team leads comprised managers (36%), nurses (42%), and allied health professionals (22%).
Across the two cohorts, 238 team members participated. On average, teams comprised 3 members and included managers (21%), nurses (51%), allied health, support staff, and patients (28%). The 12 webinars were attended by an average of 75 participants, and 203 resources were shared on the portal including charters, initiative summaries, project templates, and audit, communication, and point-of-care tools. Ratings of webinar and portal helpfulness were 4.1 and 4.2, respectively, on scales in which 1 = “poor” and 5 = “excellent.”
Coaches provided 1,107 unique facilitations on themes including the development of aim statements and measures, communications, the use of run charts, data templates and graphs to demonstrate small tests of change, inter-team linkages on similar aims or challenges, linkages to clinical resources, and reporting support. Mean ratings of the helpfulness and accessibility of coaches were each 4.5 on scales in which 1 = “poor” and 5 = “excellent.”
Unexpectedly, 75% of the hospitals in the first cohort voluntarily continued their involvement in the network after its formal period of engagement, which suggests that the initiative’s collaborative network aspirations were achieved with organizational retention rates (89%) exceeding those reported in systematic reviews. 35
Objective 2: Increase team confidence in using the SFH Framework and leading practice change
Table 2 portrays mean SEM ratings. The SEM’s internal consistency reliability is high (Cronbach’s alpha = .96) suggesting one overriding confidence element. Results for each confidence dimension show a pattern of high confidence before workshop 1 that decreased following it and was at its highest at initiative’s end. There were no confidence differences associated with team leaders’ organizational role.
Objective 3: Implement practice improvements
SFH ACTION supported a diverse array of improvements across the 78 teams. Twenty-eight (36%) were focused on delirium and 24 (31%) on mobilization and the prevention of functional decline. Other improvements included falls (4), responsive behaviours (4), continence (4), nutrition (3), sleep (3), transitions/readmissions (3), service satisfaction (3), medications (1), and physical environment (1). Even within categories, diverse applications were evident. Consider delirium interventions. While 86% focused on Confusion Assessment Method screenings, variations included location and timing of screening, screening triggers, anticipated screening rates, screener roles, physician engagement, and volunteer/family knowledge transfer.
Table 3 portrays mean PAS scores. Scores increased at each interval and with one exception these improvements were statistically significant. Seventy-one (91%) of the teams reported progress toward their QI aim, 33 (47%) of these were rated as “significant improvement,” and 23 (32%) were rated as “sustainable.” It is of interest that 33 (75%) cohort 1 teams voluntarily submitted PAS scores during cohort 2’s timeframe and of these, 14 reported achieving “sustainable improvement.”
Objective 4: Sustain interventions
Table 4 portrays mean ISS. Internal consistency reliability for the ISS scale was “borderline” (Cronbach’s alpha = .68) but was optimized by using all scale items. Forty-nine (63%) of the teams completed the ISS at both points in time (time 1 = pre-workshop 1 and time 2 = 6 months later).
Significant improvement is evident for all domains of sustainability. At both points in time, the domain of sustainability due to staff and leadership was rated highest. In an analysis of T1-T2 ISS difference scores, this domain improved significantly more than either the process (t = 5.22, P > .000) or organizational fit domains (t = 4.27, P > .001).
The organizational role of team leader was unrelated to implementation progress and sustainability ratings.
Discussion
Hospital administrators and managers had acknowledged a readiness to improve their organizations’ care of older adults but a gap in staff skills and knowledge was considered an obstacle to progress. SFH ACTION was designed to close this gap and build hospital teams with the skills and knowledge needed to confidently lead sustainable improvements in senior friendly care within their organizations.
Consistent with implementation science research on the use of evidence-informed theory and frameworks in intervention design,29,45-47 SFH ACTION was guided by the CNM and the SFH Framework. The former serving to reduce redundancy in the training of skill sets (QI, leadership, and SFH Framework) while providing a psychological environment encouraging collective action. The latter enabling teams to select and adapt improvements to best fit their hospital’s context, reduce reactance to top-down control and maximize opportunity for innovation that may be particularly important in multi-hospital/unit initiatives.26,29 In linking these two features SFH ACTION may be unique amongst applications of CNM and multi-hospital interventions in the care of seniors.46,47
Despite methodological limitations including non-random cohort assignment, reliance on subjective measures, and the absence of control groups, clinical outcome measures, or cost effectiveness data, results suggest that SFH ACTION achieved its objectives and can inform process improvement specialists, health system leaders, hospital administrators, and unit managers who are building more senior friendly hospitals.
Process improvement specialists should consider the dynamics of contextual variation. Hospitals are complex adaptive systems, 29 each comprising a unique context where an organizational goal such as “improving delirium care” may have diverse meanings. We think that the SFH Framework allowed us to limit attrition in this complex intervention by being respectful of the need for contextual variation. Participants did not want to leave the network and when competing priorities are no longer a distraction 26 to healthcare systems, a re-energized network can support more senior friendly improvements informed by the rich diversity of the collaborative’s innovations. In this regard, alternatives to the SFH Framework that have emerged internationally48,49 might serve the value of contextual adaptation in their settings.
For health leaders our findings suggest that declaring senior friendly care as a system priority and encouraging collective action in a manner that reduces redundancy while preserving diversity can accelerate system-wide practice improvement. We encourage hospital administrators to consider that regardless of their organization’s size or complexity, small teams can achieve sustainable change when they are focused on improvements that fit within the organization’s context and when they have multifaceted supports. Our findings suggest that supports that help teams achieve success include: designating an organizational leader as an executive sponsor, support by knowledge-to-practice facilitators within a collaborative network, and guidance by an explicit framework such as the SFH Framework. We encourage unit managers to consider that while their participation on implementation teams is advantageous, they do not need to lead the intervention. Interprofessional leadership can be effective allowing managers to support their team’s psychological dynamics such as overconfidence, confidence loss, and its recovery.
“…the initial kick-off meeting was exciting… but in the back of your mind, you’re feeling a little bit overwhelmed with, how can we make this work? What does this mean to me? How am I going to get my team to buy in? What is a goal and how am I going to do all of this? By the end, though, it was exciting to see because the room now had an entirely different feeling. It was charged. It was positive. People were sharing their successes. It was a glory moment…you could see the pride amongst all of the teams.” - Manager
Conclusions
By linking the CNM and the SFH Framework, the SFH ACTION program was able to close a gap in the skill and knowledge needed to lead improvements in the care of older adults, and accelerate change in 78 hospitals.
Study findings help build our understanding of knowledge-to-practice processes in healthcare and provide practical insights for others who are looking to accelerate change. In future work using similar designs, researchers are encouraged to consider the integration of more clinical health system metrics in their shared measurement model. Metrics amenable to such an undertaking might include health system priorities such as length of stay, or alternative care designations whose causal pathways are as diverse as the improvement strategies that are implemented.
The actions taken by 78 hospitals contributed to the development of an integrated, intersectoral vision of senior friendly care; a vision that now has its own framework—the sfCare Framework 50 to guide all healthcare organizations in their pursuit of more senior friendly care.
Footnotes
Acknowledgements
The authors would like to thank Ummu Almaawiy for conducting end-of-program interviews and Ata Miyar for research assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by funding from the Toronto Central Local Health Integration Network and through a 3-year Capacity Award of the 2014 Health System Research Fund from the Ontario Ministry of Health and Long-Term Care (grant number 06689). The funders played no role in the design, execution, analysis and interpretation of data, or writing of the study.
Ethical approval
The study received research ethics board approval from Sunnybrook Health Sciences Centre.