
Abstract
Investment in capacity for implementation of leading practices in regional-level health workforce planning is essential to support equitable distribution of resources and deployment of a health workforce that can meet local needs. Ontario Health Toronto and the Canadian Health Workforce Network (CHWN) co-developed and operationalized an integrated workforce planning process to support evidence-based primary care workforce decision-making for the Toronto region. The resultant planning toolkit incorporates planning processes centred around engagement with stakeholders, including environmental scanning tools and a quantitative planning model. The outputs of the planning process include estimates of population need and workforce capacity and address challenges specific to Toronto, such as patient mobility, anticipated rapid population growth, and physician retirement. We highlight important challenges and key considerations in the development and operationalization of workforce planning processes, particularly at the regional level.
The planning imperative
Ontario Health Toronto (Toronto Region) 1 plans, funds, implements, and evaluates local health services and is tasked with optimizing access to integrated services across the Toronto Region. To respond to this mandate, and to support evidence-based decision-making regarding the deployment of the workforce and other health system resources, a robust approach to primary care workforce planning is needed.
The planning landscape in Toronto is complex given the cultural and socio-economic diversity of the population, population mobility, and variations in health service use, health outcomes, and distribution of service providers across the 140 neighbourhoods in the city. A tailored workforce planning approach that addresses the core needs and key challenges present within the Toronto Region’s primary care landscape is, therefore, required. The planning toolkit needs to: (1) enable population needs-based and evidence-informed planning; (2) be integrated and multi-professional, including all the providers and services involved in the delivery of primary care; (3) facilitate an assessment of alignment between population needs and workforce capacity at the neighbourhood, sub-region, and whole city levels; (4) accommodate short planning horizons, in line with regional decision-making timelines; and (5) address certain challenges specific to Toronto, such as patient mobility, population growth, and anticipated physician retirement.
Process
In 2017, the Health Analytics team at Ontario Health Toronto partnered with experts from the Canadian Health Workforce Network to co-develop and operationalize a fit-for-purpose toolkit to support integrated primary care workforce planning in the Toronto Region. For this project, which has spanned two phases of work to date, we adopted an approach informed by a participatory action research framework 2 involving continuous collaboration between Ontario Health Toronto and the Canadian Health Workforce Network, and extensive consultations with community, health system, and data stakeholders. This approach builds capacity for and commitment to primary care workforce planning within the Toronto Region, while simultaneously enhancing the acceptability and validity of the toolkit and its outputs.
Phase 1: 2017-2018
In Phase 1, we conducted a targeted review and assessment of existing planning models. 3 Models were assessed for suitability based on guiding principles related to the unique planning needs of the Toronto Region (identified a priori). Since no single model fully met these needs, the final approach combined key features from existing models (including England’s Robust Workforce Planning Framework, 4 Australia’s Health Workforce Planning Tool 5 and several tools from New Zealand’s Workforce Intelligence and Planning Framework). 6
The final health workforce planning toolkit,
7
summarized in Figure 1, includes a cyclical process for primary care workforce planning, as well as a fit-for-purpose quantitative workforce planning model. The development of the quantitative model was informed by an environmental scan and assessment of available data sources.
8
Data related to population health need and profession-specific health workforce supply were identified and assessed for quality, availability and comprehensiveness, as well as overall suitability for use in modelling. Given Toronto’s cultural diversity, variables that could help apply an equity lens to workforce planning, such as gender, language, race, Indigenous identity, and disability were specifically sought and considered. Overview of primary care workforce planning toolkit.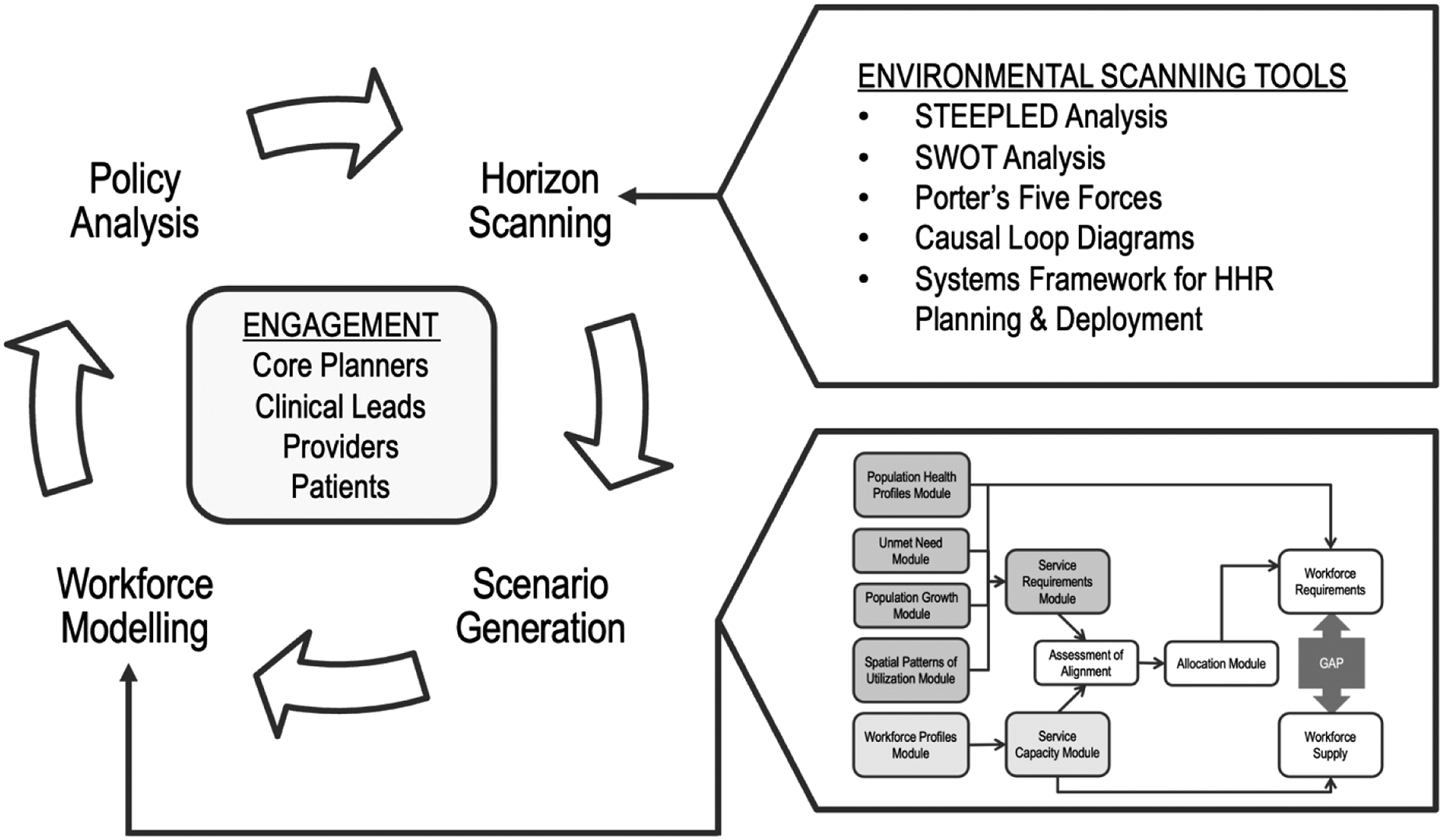
Inspired by the process prescribed by the UK’s Centre for Workforce Intelligence,
9
the toolkit’s cyclical workforce planning process includes horizon scanning (systematic exploration of the likely future developments, driving forces, and potential issues that could influence workforce requirements), scenario generation (development and elaboration of a range of plausible futures), and a quantitative workforce planning model, all of which are intended to inform policy analysis and decision-making. Environmental scanning tools and the modular quantitative model (described in Textbox 1) enable planners to engage with primary care providers, community stakeholders, and Ontario Health Toronto’s network of partners on an ongoing basis. Both planning and engagement are iterative and dynamic processes that allow planning to respond to emerging issues and challenges. Textbox 1: Modules of the quantitative workforce planning model The The The The The The
Phase 2: 2019-2022
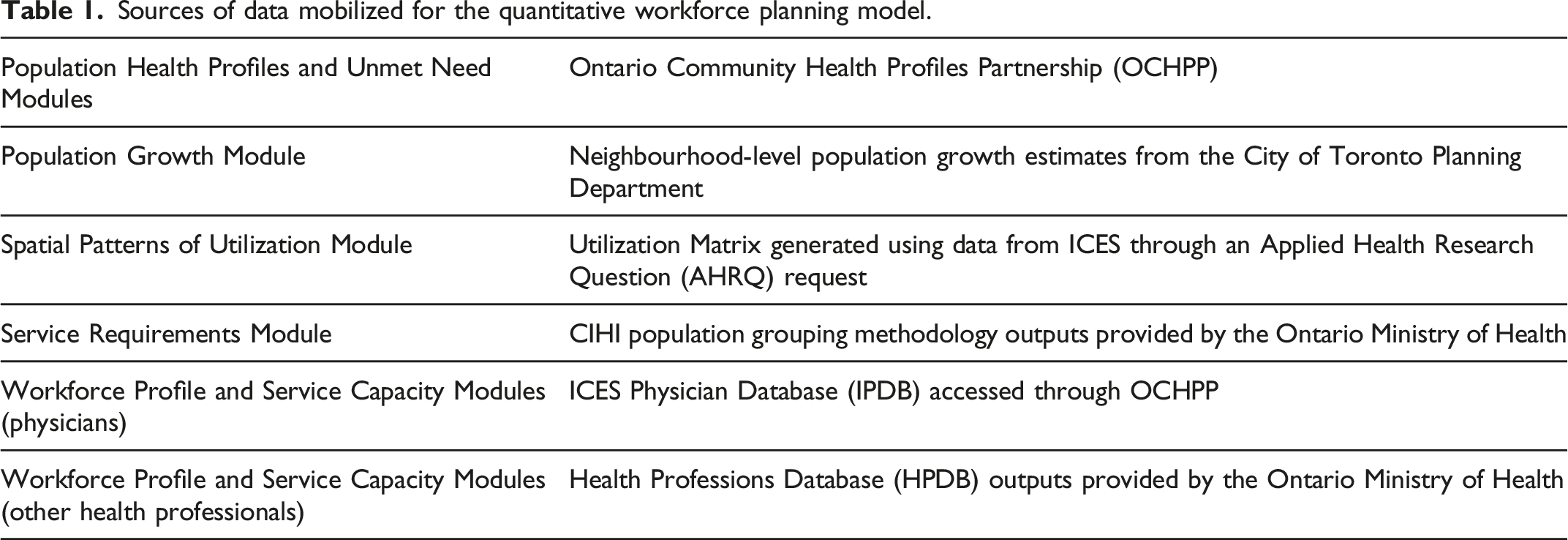
Sources of data mobilized for the quantitative workforce planning model.
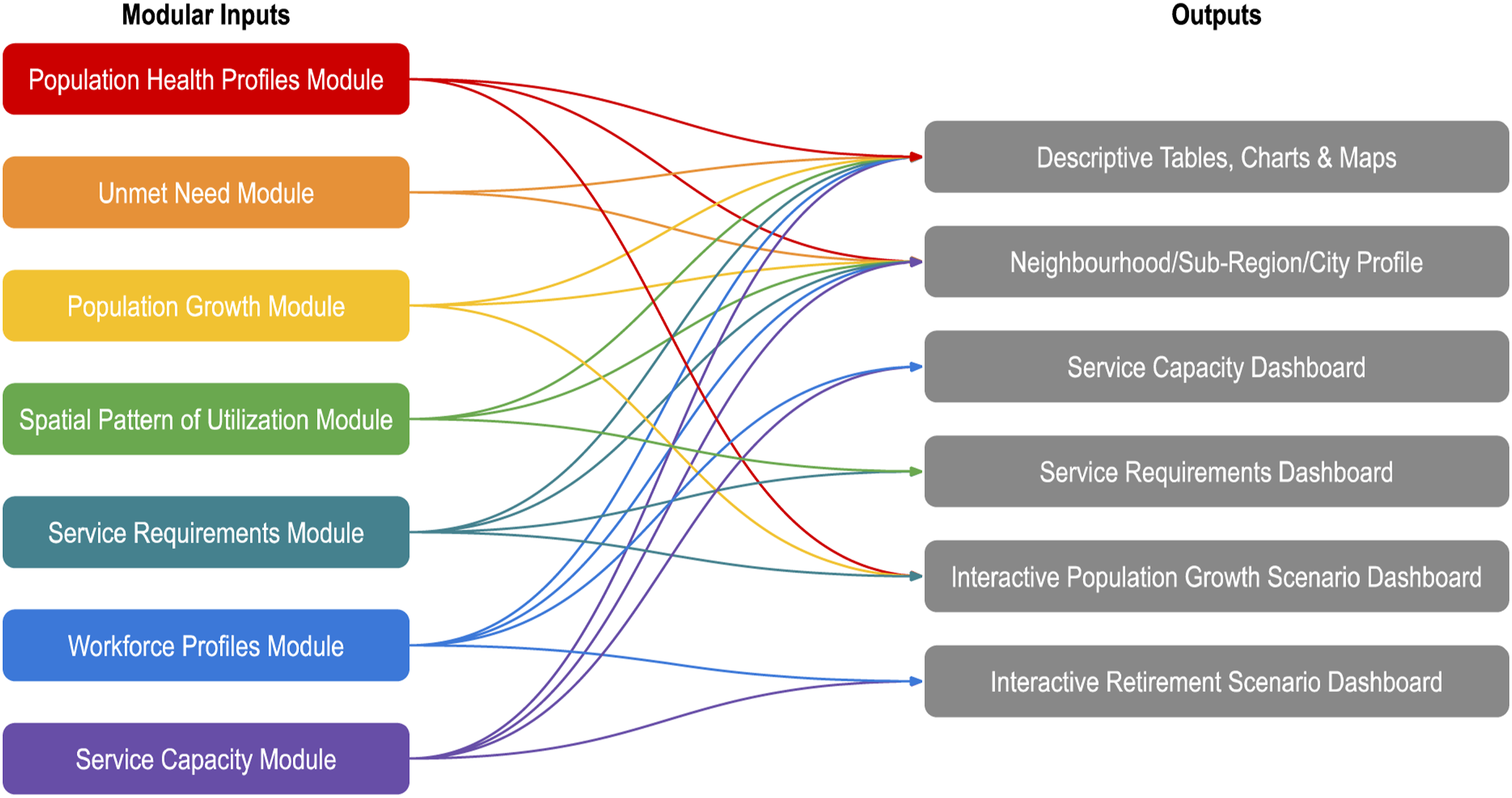
Data flow between modules and outputs.
Phase 3
The third phase of work, which initiated in September 2022, will involve updating the data in all the modules, building capacity for primary care workforce planning within and beyond the Toronto Region, developing and implementing additional modules that respond to the planning needs of local stakeholders (Textbox 2), and evaluating the impact of the toolkit. Textbox 2: Modules targeted for operationalization in Phase 3 The After an initial assessment of alignment between population service requirements and workforce service capacity, an optional After consideration of Unmet Need and various Allocation scenarios, gaps in alignment between population need and workforce service capacity may remain. The
Key outputs
Through the first cycle of workforce planning, we produced a variety of outputs designed to support evidence-informed decision-making at the neighbourhood, sub-region, and city levels.
A neighbourhood package available for each neighbourhood across Toronto includes a series of three static dashboards that bring together information about the population, the workforce, and the alignment of the two. Sub-region packages, which collate the static dashboard outputs for all neighbourhoods in a given sub-region, are also available for the ease of reference of users. Finally, a city package is available, including a static city-level profile and a series of descriptive maps. Interactive dashboards and more detailed information about specific communities are available upon request through Ontario Health Toronto.
In line with our commitment to ensuring that the toolkit, and its outputs are open-access and readily available for use by health system stakeholders within and beyond the Toronto Region, the tools we have developed are available on the Canadian Health Workforce Network website 10 and all of our static outputs are posted on the Ontario Community Health Profiles Partnership (OCHPP) web site. 11
Our integrated knowledge translation 12 activities have also involved a series of tailored presentations to health system stakeholders who contributed to toolkit development and operationalization, or who are interested in making use of the toolkit and/or, its outputs. Ontario Health Toronto will support ongoing engagement with interested users and provide assistance in the development and interpretation of targeted scenarios.
Impact
The outputs from this integrated primary care health workforce planning approach benefit Toronto region providers, planners, and stakeholders broadly. The toolkit helps characterize primary care patients (where they come from and their primary care needs) and uses leading practices (such as the CIHI Population Grouping Methodology 13 ) to generate an estimate of the primary care resources needed in communities across Toronto. Adjustment for patient mobility and consideration of future population growth respond to planning challenges that are specific to Toronto and further enhance the utility of the outputs.
Decision-makers in Toronto and elsewhere are in urgent need of support to identify high-needs areas and future emerging primary care needs, taking into account population growth, demographic shifts, provider retirement, and changing practice patterns. Our outputs respond to a need for evidence to support decisions such as where new physician positions would best be placed, which community would benefit most from new or expanded integrated primary care teams, where best to allocate additional funding, and where other allied health resources should be deployed. Planning processes such as ours provide this evidence, along with the foundation and scaffolding to support the development of essential local and regional primary care planning capacity.
Challenges and limitations
Neighbourhood-level planning is driven by the aspiration to provide comprehensive primary care close to home for all patients. And yet, mobility of patients and service providers continues to be a challenge for decision-makers. Incorporating adjustments for spatial patterns of utilization has helped to explain observed utilization patterns and made neighbourhood-level planning meaningful. But care-seeking patterns are dynamic, and they influence—and are influenced by—the primary care landscape, so the importance of iterative planning with regular timely data and methodological updates cannot be overstated.
Health workforce data are critical, not only to inform deployment of resources, but also to assist with evaluation of workforce-related health system interventions. And yet, availability and accessibility of workforce data to regional-level planners is a major barrier to evidence-informed decision-making. Record-level data for physicians and the allied health professions that are high quality, granular, comprehensive, and timely are often difficult to access. Our team invested significant time and effort to identify high quality datasets that captured the data elements required to populate our quantitative model, and to design robust and reliable methodologies and automated analyses that could be run by third parties and output in aggregate at the neighbourhood-level. Delays in access to data significantly extended the timelines for the project, and data lags and limited longitudinal information constrain extrapolation, and in some cases undermine the accuracy of our projections. Engagement with local stakeholders will help us to estimate the degree of uncertainty that is associated with our results.
We have had to adapt to an evolving landscape of health system transformation, although most of the workforce planning issues facing decision-makers in Toronto have remained pertinent or become more urgent. Regular engagement with stakeholders and decision-makers confirmed that the planning priorities and project outputs remain relevant. The iterative nature of the planning process and the modular model allowed us to easily consider the impact of additional scenarios (such as early retirements) and we are confident that future emerging issues (such as virtual care and the changing roles of pharmacies) can be addressed in a similar manner.
Key success factors
Throughout the project, we committed to adopting and championing leading practices in planning (identified in Phase 1), including the use of high quality and comprehensive data. The Ontario Health Professions Database 14 (HPDB), a rich dataset that brings together standardized, consistent, and comparable demographic, geographic, educational, and employment information on all regulated health professionals in Ontario, was an important facilitator of integrated planning for this project. Likewise, the Canadian Institute for Health Information Population Grouping Methodology 8 was an enabler of regional-level needs-based planning.
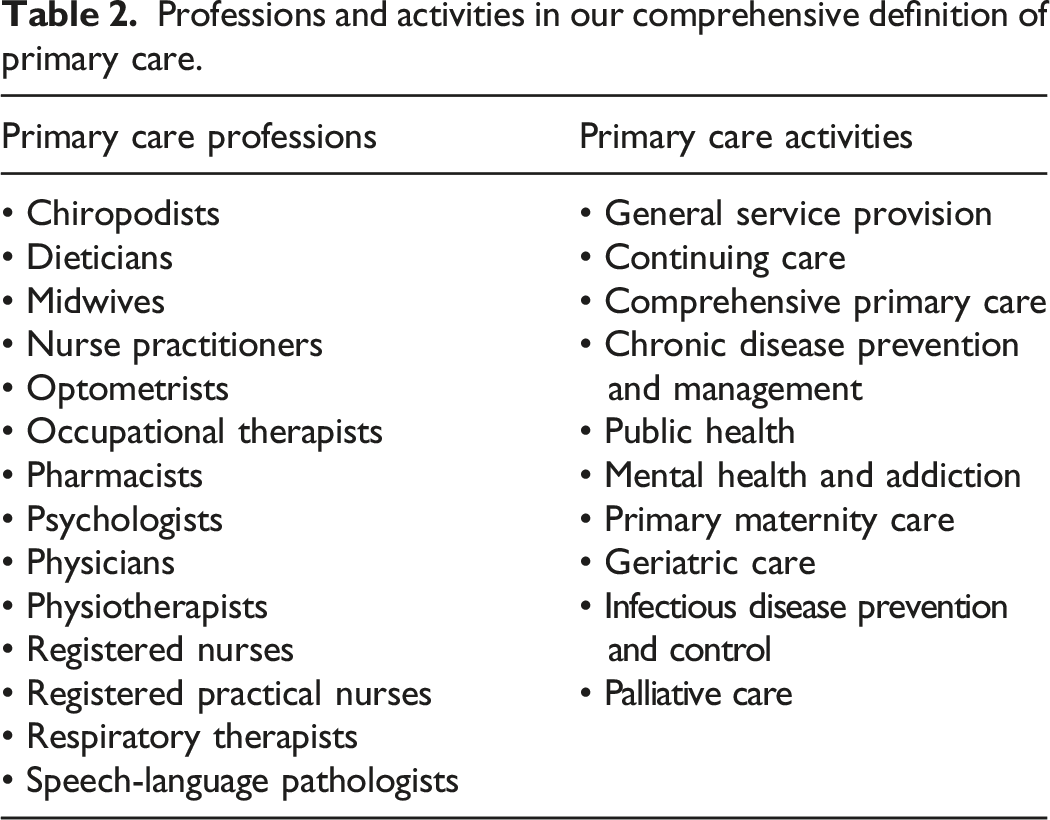
Professions and activities in our comprehensive definition of primary care.
What we have learned and want to share
This project is a case study in leading practice health workforce planning. It responds to an urgent need for intelligence to support evidence-informed health system decision-making in Toronto. The process emphasizes collaboration with stakeholders and incorporation of local knowledge to supplement the toolkit outputs, validate the results, and build a fulsome picture of local primary care needs. Having a holistic view of the various factors at play can help local decision makers to exercise flexibility and ingenuity in developing innovative solutions to address primary care service gaps.
We have built a strong foundation for comprehensive primary care workforce planning. The toolkit and model will be shared with others doing primary care workforce planning to spread and scale this type of leading practice and to promote use of a common methodology. But more needs to be done: in keeping with the iterative nature of planning, the model will be refined on an ongoing basis, to incorporate updated population data and more current primary care utilization patterns and workforce information. Over time, through continuous cycles of iterative methodological refinement, the accuracy of estimates produced by the model will be evaluated and enhanced.
At the policy level, our experience indicates that there is a need for decision-makers to recognize the importance of planning and support the development of planning capacity, literacy, and engagement. Targeted investments in data and data infrastructure, tools to support planning, and supported networks of leaders, clinicians, analysts, and other stakeholders committed to the principles and promise of health workforce planning will be essential to the success of future planning endeavours. We encourage aspiring planners to adopt leading practices, to anticipate challenges and advocate for their resolution, and to prioritize engagement and collaboration in their health workforce planning endeavours.
Footnotes
Acknowledgements
The authors would like to acknowledge and specially thank the following for providing their guidance, feedback, and data and mapping support: Ontario Health Toronto Health System Strategy, Planning & Implementation and Communications teams; Ontario Community Health Profiles Partnership (OCHPP); The Toronto Region Primary Care Regional Council (PCRC); Unity Health Toronto; City of Toronto Planning Research and Analytics, City Planning Division; ICES; Ontario Ministry of Health (MOH) Health Analytics & Insight Branch; MOH Health Workforce Planning Branch, Capacity Planning & Capital; Canadian Institute for Health Information; Statistics Canada; East Toronto Family Practice Network and East Toronto Health Partners; along with other Ontario Health Teams.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Unity Health Toronto.
Ethical approval
Institutional Review Board approval was not required.