
Abstract
Indigenous people in Canada continue to experience barriers accessing healthcare services including systemic racism and disproportionate healthcare disparities. Indigenous Patient Navigators (IPNs) and programs may mitigate these barriers by providing culturally safe care and support for Indigenous patients and their families navigating healthcare systems. Unfortunately, few IPNs and IPN programs exist in Ontario. We conducted an environmental scan of IPN resources and programs in Canada. Our aim was to determine evaluation frameworks, training, responsibilities of IPNs, and current IPN programs in Canada. We found 97 web sites or documents that were gathered between January and March 2021. We offer gaps in knowledge uncovered during the environmental scan. We conclude with recommendations for the implementation of IPN programs. Indigenous patient navigators have the potential to improve Indigenous healthcare experiences. Specific and sustained action is required to improve and create an equitable health system for Indigenous people across Canada.
Background
Indigenous people continue to experience barriers accessing healthcare services including pervasive anti-Indigenous racism and disproportionate healthcare disparities as a result of systemic inequality.1-3 Indigenous Patient Navigators (IPNs) have been introduced to hospitals and healthcare settings as one means of reducing these structural and interpersonal barriers.4,5 IPN programs support Indigenous patients and their families through the provision of culturally appropriate and specific care.4-6 Specifically, IPNs can improve access to culturally safe care, coordinate translation services, improve service coordination between multiple jurisdictions, and in some circumstances, act as an educational resource to healthcare providers and staff within the hospital.5,6 The inclusion of IPNs in various health provision services could assist with reducing institutional and interpersonal racism experienced by Indigenous people as seen in the high-profile cases of Brian Sinclair and Joyce Eschaquan.7,8 Furthermore, IPNs could uphold principles such as Jordan’s Principle, which was designed to ensure accessible services to all First Nations children.9,10 Jordan’s Principle is a child-first and needs-based principle that stipulates First Nations children living on and off reserve will not be denied health services as a result of jurisdictional disputes.9,10
Originating in the American healthcare system, patient navigation was first introduced by Dr. H.P. Freeman as a volunteer and peer support program designed to reduce health disparities experienced by African-American and Latino women accessing breast cancer treatments in Harlem, New York. 11 Since then, the model has grown and expanded across jurisdictions with some programs utilizing the peer support model developed by Freeman to employ allied and trained health professionals such as registered nurses and social workers.
We conducted an environmental scan of Indigenous patient navigator resources and programs in Ontario and Canada. Our aim was to determine evaluation frameworks, training, definitions of the IPNs with their responsibilities, and IPN programs in place in various healthcare contexts. As there was a wide variation in information, we have provided diffuse information about Indigenous patient navigators.
Methods
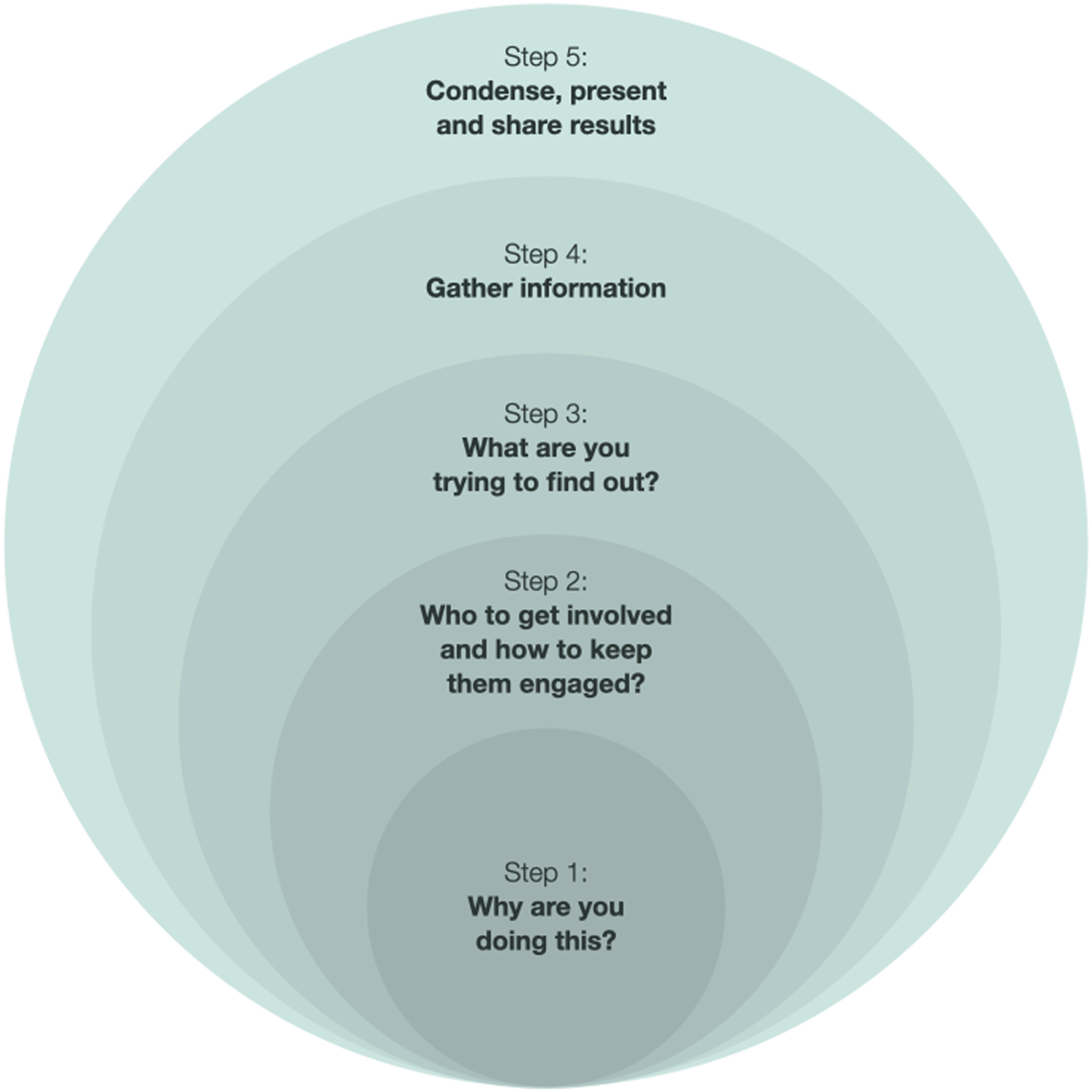
This research utilized a rapid Environmental Scan (ES) method modifying the five-step protocol developed by Shahid and Turin
12
(Figure 1). An environmental scan method was selected as it is a useful tool in health research for the collection of diverse types of knowledge and for supporting evidence-informed policy and program development.
13
As our scan also included the meaningful integration of Indigenous community knowledge and perspectives, it was important to implement a protocol that integrated diverse sets of knowledge and reflexivity thus we adapted Shahid and Turin’s model to suit this purpose. Figure 1 depicts our vision of Shahid and Turin’s
12
five steps represented in an iterative and relational way. Iterative approach to the five steps of environmental scanning. Adapted from Shahid and Turin.
12
Inclusion and exclusion criteria

Findings
We found 97 web sites or documents that were gathered between January and March 2021. We report our findings by location in Canada and conclude this section with gaps in knowledge uncovered during the environmental scan. Given the nature of environmental scanning, it is likely some organizations with IPNs did not appear in our search. As such, our findings intend to provide a high-level landscape but are not necessarily comprehensive.
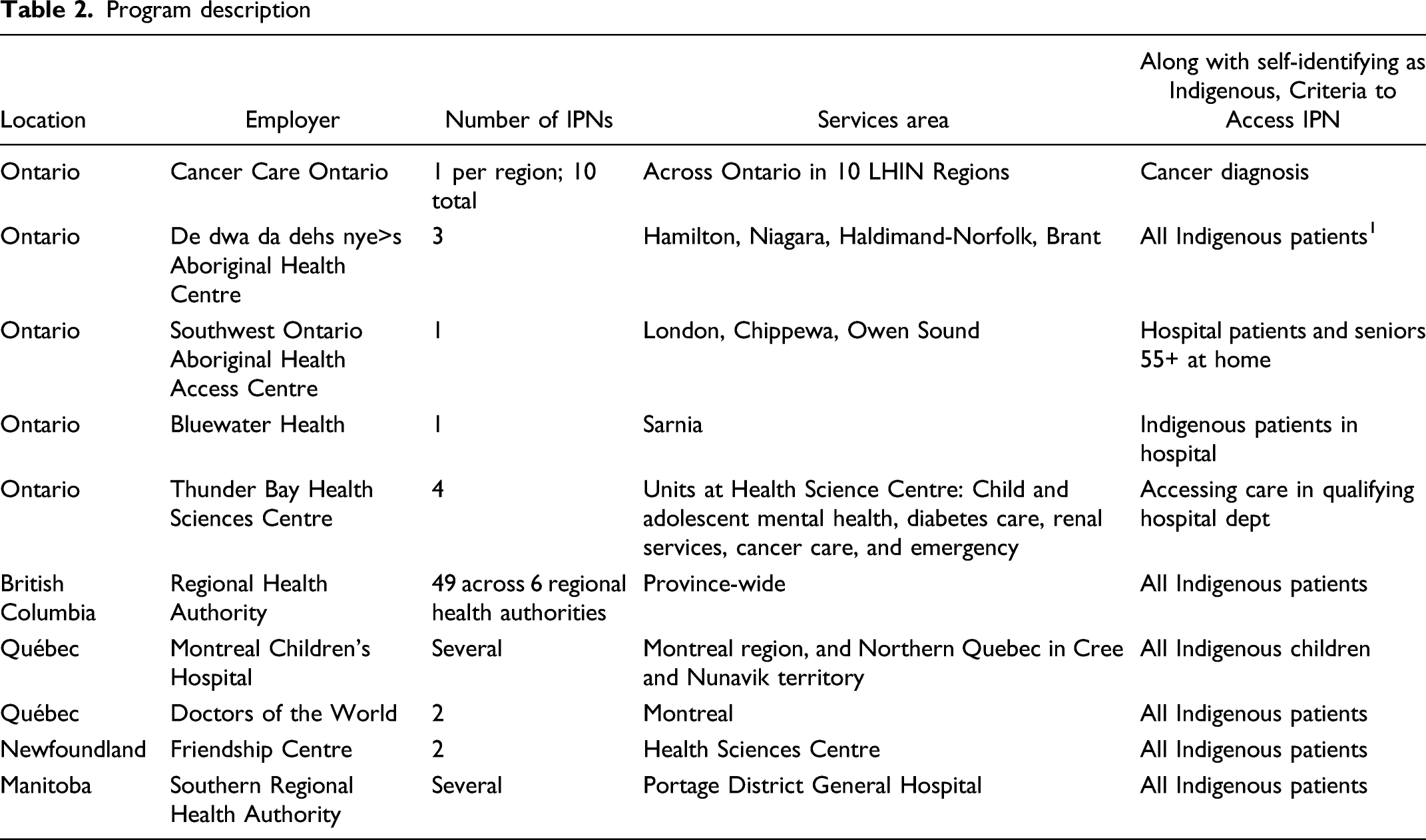
Across the Canadian healthcare landscape, we identified several IPN program structures. Specifically, there is wide variability on the role of an Indigenous patient navigator, the types of healthcare facilities they operate within, and the number of IPNs available in a given healthcare setting. For example, Ontario has a very small number of IPNs and they work within very narrow medical criteria (ie, cancer care or diabetes care) with only 10 IPNs staffed by Cancer Care Ontario serving all Indigenous people accessing cancer treatment in the province. 16
Ontario
Program description
British Columbia
British Columbia has one IPN program throughout the province (Table 2); each of the four regional health authorities and one provincial health authority coordinate a subset of the IPN program. Based on all of the programs identified in this environmental scan, British Columbia offers the leading example of an Indigenous patient navigator program for several reasons. 17 First, there are a high number of IPNs employed in the province with upwards of 40 IPNs. Second, there are no medical criteria (diabetes treatment, cancer care) to access the IPN service, so all Indigenous people can access IPN services. Third, although there is one overarching program, the IPNs are hired by a wide variety of organizations, including hospitals, community organizations, and regional public health authorities, which results in the wide geographic distribution of IPNs. Their IPN program was established in 1986, decades before many of the other mentioned IPN programs. 17 Furthermore, the IPN program in BC has immense support from Healthcare Practitioners (HCPs) who said the program improves communication within the healthcare team, brings culturally safe care to patients, and offers learning opportunities for HCPs about Indigenous history. This support from HCPs results in the uptake of IPNs by Indigenous patients because IPNs are brought into the care plan and made accessible to the patient. 17
Additional provinces and territories
There are several IPN programs throughout the rest of Canada (Table 2). The environmental scan did not reveal any IPN programs in Nunavut, the Northwest Territory, or the Yukon.
Training
The environmental scan did not reveal any organizational training available to hospital staff for implementing IPN programs or training for IPNs. There are certificate-level training programs for patient navigators at Fleming College, York University, and Mohawk College, although there are no programs specific to serving Indigenous students wishing to become IPNs.18-20 Each of the programs focuses on the fundamentals of patient navigation, healthcare navigation, patient-centred care, health promotion, and interpersonal collaboration and communication. However, none of the navigator programs require cultural safety training and do not specialize in Indigenous-specific health and navigation services.
Evaluations
The environmental scan identified only one evaluation of an IPN program. This evaluation was conducted by the Northern Health Authority in British Columbia 6 which utilized several methods including colleague surveys, patient interviews, and Aboriginal Patient Liaison (APL) surveys. The results from both the colleague surveys and patient interviews showed overwhelming support for the program and positive experience in healthcare as a result of the program.
Job descriptions
To further understand the role and responsibilities of an Indigenous patient navigator in Canada, we attempted to find job descriptions. We were unable to find publicly available job descriptions; however, we found some job postings. Of the IPN job postings available to review, we found a lack of consistency pertaining to the educational background and requirements for the positions as well as a lack of clarity of the specific responsibilities for the role. Similar to the lack of consistency across job postings, there is a lack of consistency in required qualifications for the IPN. This range in qualifications varies from professional designation (ie, RN, SW, midwife, and MD) required to have professional designation optional.
Accountability
The environmental scan did not identify any accountability mechanisms for implementing Indigenous patient navigator programs. The specific mechanisms and functions of accountability will vary and we recommend that organizations work with Indigenous communities to decide on clear accountability mechanisms.
Recommendations
The Truth and Reconciliation Commission 21 and the Murdered and Missing Indigenous Women and Girls Final Report, 3 as well as the In Plain Sight 2 report, have all recommended more culturally safe healthcare, which IPNs would be central in this provision by providing health literacy, advocacy, and connecting to other services. As IPNs are situated within healthcare settings, they can act as knowledge brokers (ie, translate medical terminology and advocating for Indigenous ceremonies), as well as connect patients and families to Indigenous programs and services in the area that may assist with the long-term treatment of the medical issue, and voice concerns within the healthcare teams and management. We offer recommendations in five sections: organization training, evaluations, job descriptions, accountability, and availability of IPN service.
Training
For IPNs to have the support of their colleagues and other health professionals, the hospital or health setting should become a learning health system where there is an iterative process of making changes brought about learning.22,23 Cultural safety training within healthcare has been an ongoing discussion with accreditation bodies offering the suggestion that all healthcare professionals take it (see CPSO, Royal College of Physicians and Surgeons). To ensure the success of the IPN program, senior leadership should implement cultural safety training for healthcare professionals and staff working with IPNs and Indigenous patients and families. IPNs need to have access to training that will help them as navigators and advocates for their patients, which could be negotiating, assertiveness, and cultural brokering.
Evaluations
Evaluations are an essential component of implementing programs such as an IPN program in healthcare settings. We were unable to identify any evaluations, so they will need to be developed by the implementing organization. All evaluation frameworks should be based on Indigenous research methods and data sovereignty. 24 Using Indigenous research principles, such as OCAP and Inuit Qaujimajatuqangit, can ensure that an evaluation is culturally safe, that the analysis includes an Indigenous lens, and that recommendations and program changes are reflective of the Indigenous patients and their family’s needs. Evaluations can also provide a voice to Indigenous people who have used the IPN program(s) to determine success, challenges, and wise practices.
Job descriptions
Due to the unavailability of job descriptions, our recommendations also focus on job postings. We recognize that the differences in job postings between organizations may be a strength thereby allowing organizations to structure the roles according to their unique requirements, organizational structure, and internal protocols. However, the lack of clear responsibilities could create an opportunity for IPNs to be overburdened with tasks that may be beyond the scope, skills, and knowledge of the IPN. There is a variety of educational backgrounds listed on the job posters, which can create discrepancies in how IPNs are regarded in the healthcare setting. There should be some key parts of the job postings and descriptions that are standardized like the level of education, key duties, and skills that can be expanded upon by the individual healthcare settings. This standardization of job postings and descriptions will assist in bringing clarity to the role and responsibilities of IPNs and ensure that Indigenous patients accessing IPN services experience a standard of care irrespective of which hospital an individual accesses. Therefore, it is recommended that (as stated in training) other healthcare professionals and staff are trained about what IPNs are and do. Without this training for those staff working with IPNs, there is the possibility that IPNs will be pulled into tasks unrelated to their work, which will overburden the very few IPNs in the field and cause burnout.
Healthcare systems prioritize the knowledge of healthcare workers and allied health professionals. In light of this, we suggest that IPN programs will be most successful if IPN staff hired have knowledge and experience in the healthcare system which likely will include holding a professional designation (personal communication with Elders, February 7, 2021). IPNs who possess knowledge of both the western biomedical system and Indigenous worldviews may be best suited to assist Indigenous patients to better navigate the healthcare system. Examples of accreditation for IPNs are registered nurse, registered social worker, personal support worker, and midwife.
Accountability
In order to adhere to the TRC calls to action 22 and 23, 21 organizations need to develop policies to hire and retain Indigenous patient navigators. These policies would support hiring Indigenous people in an effort to reduce job turnover due to burnout. It is critical that IPNs hired self-identify as Indigenous; more specifically, it would be important to hire Indigenous IPNs connected to an Indigenous community the hospital serves. It would be necessary to implement wider anti-racism and cultural safety policies and initiatives in concurrence with an IPN program to reduce the anti-Indigenous racism and microaggressions that Indigenous staff may face in the institutions. 25
Availability of IPN service
Based on the size of the Indigenous population in Ontario (n = 374,395), it is necessary to increase the number of IPNs who are working in the Ontario healthcare system to address the anti-Indigenous racism experienced by Indigenous people. 1 Moreover, the simultaneous overburdening of one IPN while undeserving Indigenous communities is a continuation of systemic oppression and racism against Indigenous people which needs to be addressed immediately if Canada is to uphold the calls to action of the TRC, 21 calls to justice of the NIMMIWG, 3 and the articles of UNDRIP. 26
Limitations
This work was conducted as part of a larger environmental scan project. As such, we were unable to conduct interviews with IPNs and people who access the IPN programs. The rapid environmental scan was conducted using information about IPN roles and programs available on organizational web sites, reports, press releases, news sources, and journal articles. There were no interviews or consultation processes conducted to inform the development of the report. Meaningful collaboration with community members and leaders is essential when working with Indigenous people, so their voices and experiences need to be heard when designing an IPN program.
Conclusion
Indigenous patient navigators have the potential to improve Indigenous healthcare experiences by advocating for negotiating the healthcare system on behalf of and referring Indigenous people to the most appropriate and effective care and resources needed for them and their families. Ontario requires more IPNs in hospital settings to appropriately serve the needs of Indigenous patients and families. Amidst ongoing fatal harms due to anti-Indigenous racism, it is imperative that hospitals take immediate action to provide advocates for this made-vulnerable population. Our review of the IPN literature has raised concerns about the lack of policies, programs, and staff assigned to assist Indigenous people as they navigate a system of multiple paths and resources that they may be unfamiliar with and unaware of. As we noted, IPNs can assist with providing culturally safe and welcoming environments for Indigenous patients and their families, especially when coupled with systemic change. The findings from this environmental scan highlight the need for further work to be done. Our recommendations offer a starting point for organizations to implement an IPN program based on community involvement. Specific and sustained action is required to improve and create an equitable health system for Indigenous people across Canada. We hope this environmental scan inspires healthcare institutions and healthcare professionals to challenge anti-Indigenous racism in healthcare.
Footnotes
Acknowledgements
The TC LHIN Regional Anti-Racism Strategy funded two specific streams of inquiry: Indigenous health and black health. One section of the Indigenous health stream was to locate and describe existing programs, evaluations, and other available tools for Indigenous patient navigation programs in hospitals and healthcare settings. This publication is a summary of the research utilized to provide the TC LHIN Anti-Racism Steering Committee with a review and recommendations regarding the implementation of IPN programs in Canadian jurisdictions.
Funding
This work was supported by a contract with the Toronto Central Local Health Integration Network.