
Abstract
Background
Palliative care (PC) optimizes quality of life for individuals and their families by providing care that promotes dignity, respect, and comfort. Some groups experience inequities related to PC, including persons with mental illness, those living with dementia, linguistic minority groups, and living in rural, remote, or northern areas. There is little data on palliative needs among underserved groups in Canada.
Methods
We analyzed anonymized pan-Canadian population-level data on 1,451,135 home care clients. Palliative needs were defined as having a prognosis of six or fewer months to live, having palliative goals of care, or being offered or receiving hospice/palliative services. We examined the prevalence of palliative needs overall and among underserved groups, as well as whether membership in an underserved group was associated with recognition of palliative needs after controlling for other personal, social, functional, and clinical characteristics.
Results
Overall, 5.0% (n = 72,161) of home care clients had recognized palliative needs. Controlling for age, sex, social characteristics, functional, and clinical characteristics, persons aged 85 + years (0.85 OR), living with dementia (0.57 OR), mental illness (0.91 OR), and linguistic minorities (0.88 OR) had decreased odds of recognized palliative needs, while those living in rural areas had slightly increased odds (1.01 OR).
Conclusion
These findings highlight that the palliative needs of certain groups may not be recognized, and therefore they may not be receiving the care that they need. Future work on promoting earlier identification and awareness of palliative needs is needed.
Keywords
Background
The goal of palliative care (PC) is to holistically support the needs of individuals with serious and life-limiting conditions and their families across the physical, psychological, social, and spiritual domains of health, promoting dignity, respect, and comfort.1–3 High-quality PC aims to minimize pain and other issues through early identification, correct assessment, and timely treatment and intervention. 4
Global evidence demonstrates that many groups experience persistent equity gaps related to PC. Across several countries, persons with non-cancer illness, ethnic minority groups, persons aged 85 + years, and those living in rural or socioeconomically deprived areas remain underserved.5–7 In Canada, the need to improve access and understand PC needs and experiences of underserved populations has been highlighted.3,8 Recently, a Canadian report identified several underserved groups in terms of palliative care, including older adults (ie, 85 + years), linguistic minorities, persons living with dementia, and persons living in rural/remote settings 9 ; persons with mental illness are also known to experience inequitable access to PC.10,11 The continued cancer-centred focus of PC has contributed to the under recognition of palliative needs among persons with conditions that have long-term decline and uncertain trajectories, such as dementia. 12 Additionally, a recent scoping review showed that language discordance negatively affected both the quality and accessibility of PC 13 and only two of the studies reviewed were conducted in Canada.
In spite of recognizing that some groups experience inequitable access to PC in Canada, there are relatively few Canadian studies. This study aimed to examine the association between membership in an underserved group and recognition of palliative needs in Canada.
Methods
Data Source and Study Population
This cross-sectional study utilized secondary data collected using the RAI Home Care (RAI-HC) assessment across six Canadian provinces (British Columbia, Alberta, Manitoba, Ontario, Nova Scotia, and Newfoundland and Labrador) and one territory (Yukon). 14
The RAI-HC was developed for use in various populations including home care, long-term care, and palliative care settings. 15 The RAI-HC is a standardized assessment that is used routinely for all persons eligible for long-stay home care in Canada. 14 The assessment contains roughly 300 items covering key domain areas such as cognitive and physical functioning, communication abilities, disease diagnoses, and informal support and has established reliability and validity. 16 Assessments are completed by trained care coordinators (typically registered nurses) through discussion with the person, their informal care providers, other health care professionals (eg, primary care physician), and review of available medical records, as needed. Reassessments are typically completed every 6–12 months or following a change in health status. 15
Since this study involved secondary analysis of anonymized data, ethics approval was not required according to the Tri-Council Policy Statement 2022 Article 2.4B. 17 An exemption from ethics review was obtained from the Lakehead University Research Ethics Board.
This study is based on the most recent RAI-HC assessment of 1,415,975 home care clients, aged ≥18 years, completed between 2001 and 2024.
Measures
The main outcome of interest was having recognized palliative needs, which was operationalized based on three items in the RAI-HC: prognosis, palliative goals of care, and offer or receipt of hospice or palliative services. Prognosis was defined using a single binary variable on whether the patient had been identified as having a prognosis <6 months. A binary variable on whether the person has palliative goals of care (yes/no) was also used. There is a set of items focused on services, including hospice care. This item is coded as “yes” if the hospice care was scheduled or received in the last seven days. If an individual met any one of the three above criteria (ie, had a prognosis OR had palliative goals of care OR hospice care was scheduled or received), then they were considered as having recognized palliative care needs.
The main predictor was membership in an underserved group. Specific underserved groups included: (1) persons ≥85 years of age, (2) persons with any psychiatric diagnosis (eg, mood disorder, schizophrenia or other psychotic disorder), (3) persons living with dementia (ie, diagnosis of Alzheimer or other dementia), (4) linguistic minority (ie, language other than English listed as primary language), and (5) persons living in a rural or remote area (ie, based on Statistic Canada's Statistical Area Classification type 18 ). These groups are not mutually exclusive, therefore, an individual could belong to multiple underserved groups.
Personal, social, functional, and clinical characteristics were considered as covariates.
Analysis
The population was described and the characteristics of non-underserved persons and underserved groups were compared. Given the large sample size and potential for type I error, we used an absolute standardized difference of 0.2 or higher to identify statistically significant differences between those in an underserved and not underserved group. 21 Logistic regression analyses explored the unadjusted and adjusted relationship between underserved groups and recognition of palliative needs. All analyses were conducted using SAS version 9.4. 22
Results
Population Characteristics
The total study population included 1,451,135 individuals. Overall, 40.7% of home care clients were aged ≥85 years, 32.2% had a dementia diagnosis, 20.2% had a diagnosed mental illness, 14.1% were part of a linguistic minority, and 14.4% lived in a rural area; the remaining 24.0% were not in any underserved group (Table 1).
Population Characteristics (n = 1,415,975).
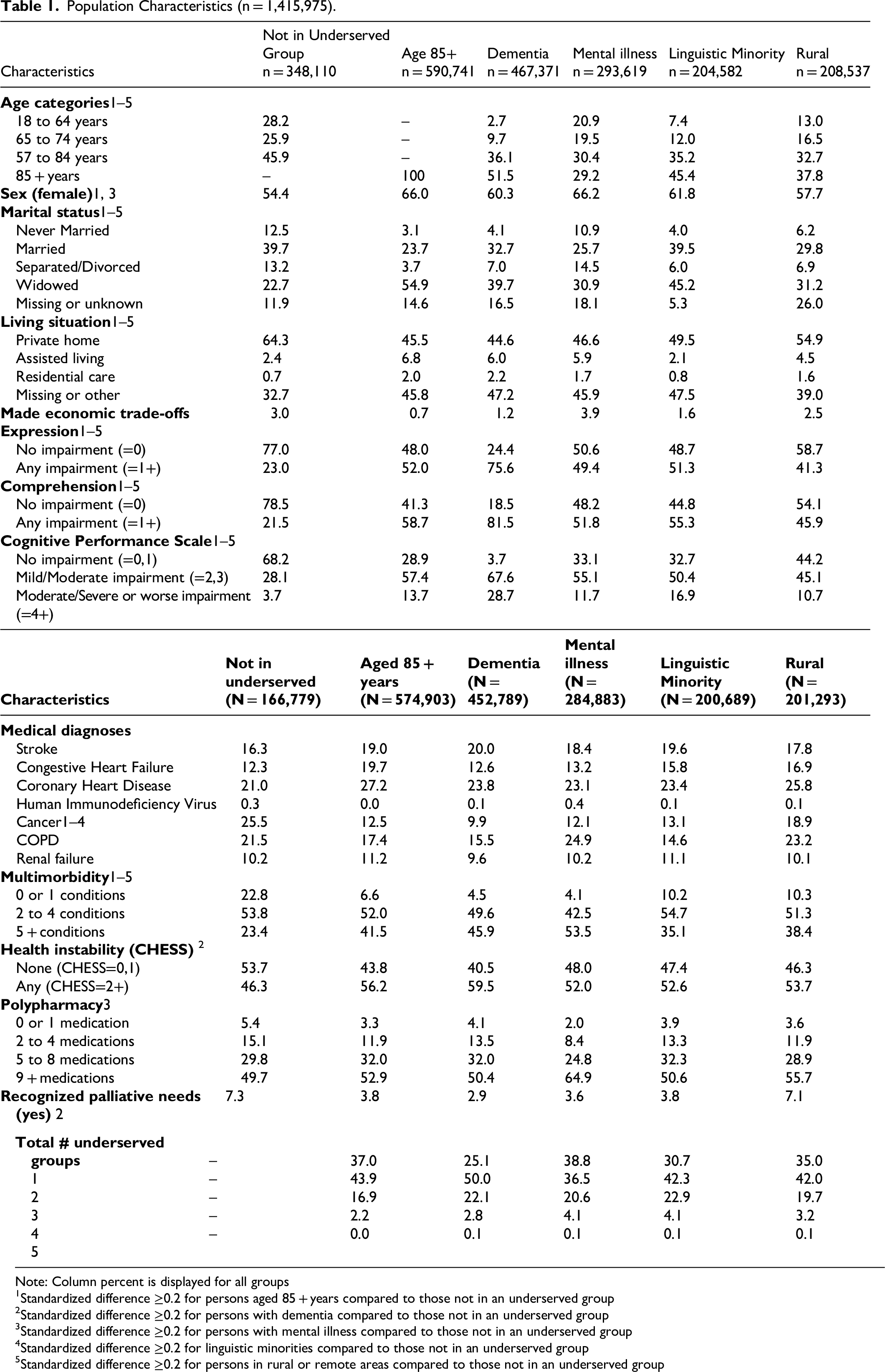
Note: Column percent is displayed for all groups
Standardized difference ≥0.2 for persons aged 85 + years compared to those not in an underserved group
Standardized difference ≥0.2 for persons with dementia compared to those not in an underserved group
Standardized difference ≥0.2 for persons with mental illness compared to those not in an underserved group
Standardized difference ≥0.2 for linguistic minorities compared to those not in an underserved group
Standardized difference ≥0.2 for persons in rural or remote areas compared to those not in an underserved group
As noted in Table 1, statistically significant differences existed between underserved groups and those not in any underserved group for most of the considered characteristics. Most notably, compared to those not in an underserved group, all groups had higher prevalence of communication impairment, impairment in cognitive functioning, multimorbidity, and being widowed; and lower prevalence of living in a private home and (with the exception of persons living in a rural or remote area) having a cancer diagnosis. Health instability was also higher among persons living with dementia.
Recognition of Palliative Needs Among Underserved Groups
Overall, 5.0% of home care clients had recognized PC needs (Table 1). Analyses (not shown) revealed that approximately 3.2% of home care clients had a prognosis of six or fewer months to live, 4.3% had palliative goals of care, and hospice care had been scheduled or received by 0.2%.
Recognition of palliative needs was higher among those not in any underserved group (7.3%) compared to persons aged ≥85 years (3.8%), living with dementia (2.9%), mental illness (3.6%), in a linguistic minority (3.8%), and living in a rural area (7.1%).
In both the bivariate and multivariate models, membership in each underserved group was significantly associated with the recognition of palliative needs (Table 2). After controlling for covariates, living in a rural or remote area remained associated with higher odds (OR = 1.01; CI: 1.01–1.02), whereas odds remained significantly lower for persons aged 85 + years (OR = 0.85; CI: 0.83–0.87), persons living with dementia (OR = 0.57; CI: 0.56–0.59), persons with mental illness (OR = 0.91; CI: 0.89–0.93), and persons in a linguistic minority (OR = 0.88; CI: 0.86–0.91).
Logistic Regression Models Predicting Recognition of PC Needs.
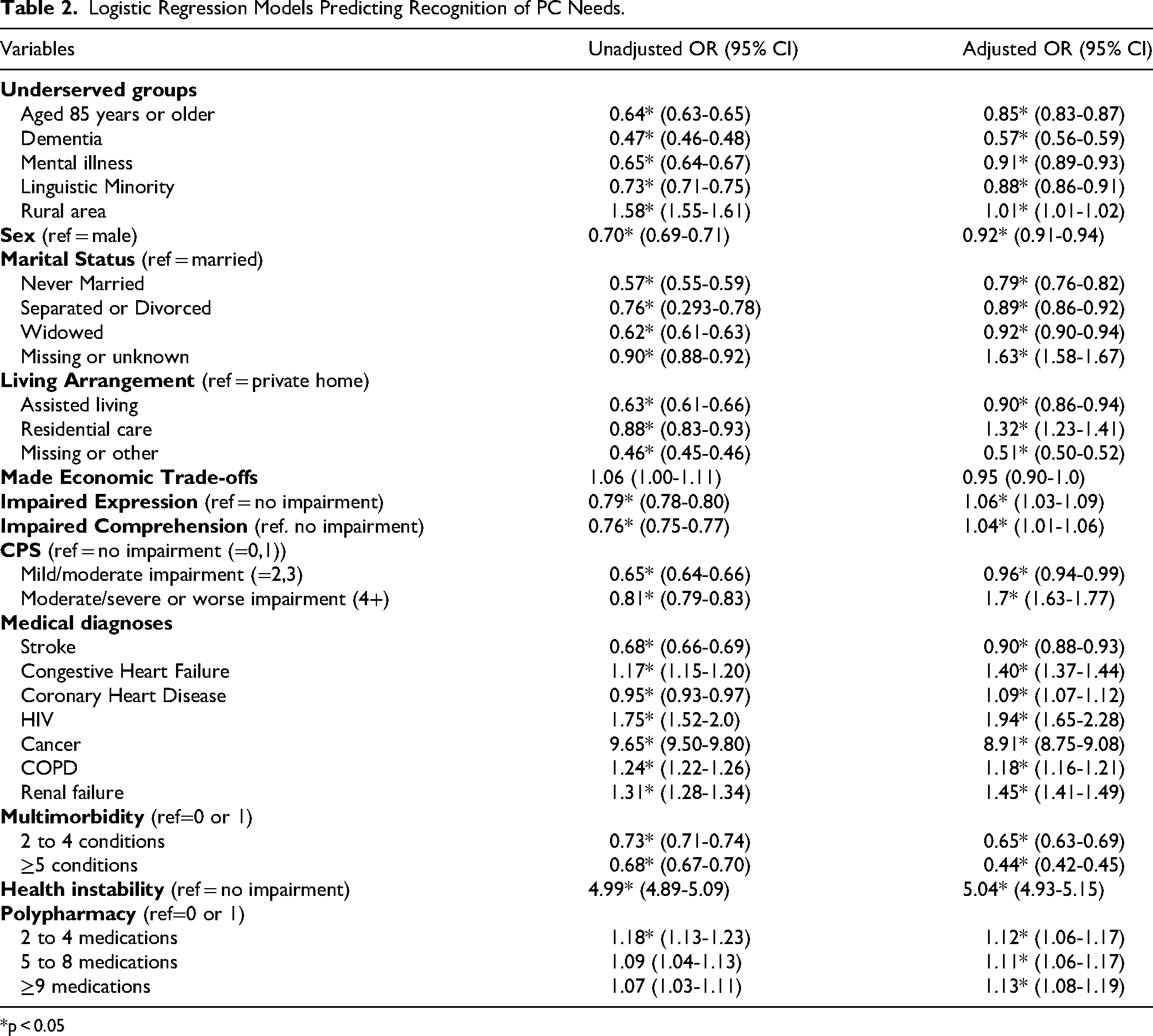
*p < 0.05
Many of the covariates were also significantly associated with the outcome in the bivariate and adjusted models. In the adjusted model, characteristics associated with decreased odds of having recognized palliative needs included: female (OR = 0.92; CI: 0.91–0.94); unmarried (ie, never married OR = 0.79; CI: 0.76–0.82; separated/divorced OR = 0.89, CI: 0.86–0.92); widowed OR = 0.92; CI: 0.90–0.94); assisted living settings (OR = 0.90; CI: 0.86–0.94); mild-moderate cognitive impairment OR = 0.96; CI: 0.94–0.99; stroke (OR = 0.90; CI: 0.88–0.93); and increasing levels of multimorbidity (ie, 2 to 4 conditions OR = 0.65; CI: 0.63-0.69; 5 + conditions OR = 0.44; CI: 0.42–0.45).
Conversely, factors associated with increased odds of recognition of palliative needs included: living in a residential care setting (OR = 1.32; CI: 1.23–1.41); impaired expression (OR = 1.06; CI: 1.03–1.09); impaired comprehension (OR = 1.04; CI: 1.01–1.06); moderate/severe or worse cognitive impairment (OR = 1.7; CI: 1.63–1.77); diagnoses of cancer (OR = 8.91; CI: 8.75–9.08), HIV (OR = 1.94; CI: 1.65–2.28), renal failure (OR = 1.45; CI: 1.41–1.49), congestive heart failure (OR = 1.40; CI: 1.37–1.44), and COPD (OR = 1.18; CI: 1.16–1.21); increased health instability (OR = 5.04 CI: 4.93–5.15); polypharmacy (ie, 2-4 medications OR = 1.12; CI: 1.06–1.17; 5-8 medications OR = 1.11; 95% CI: 1.06–1.17; and 9 + medications OR = 1.13; CI: 1.08-1.19).
Discussion
This study showed that, even after controlling for personal, social, functional, and clinical factors, home care clients aged 85 + years, persons living with dementia, those with mental illness, members of a linguistic minority, and persons living in rural areas have reduced odds of having recognized palliative needs. These findings, while largely consistent with the literature, help to further illustrate disparities faced by some groups receiving home care in Canada.
Older age (ie, ≥ 85 years) has previously been associated with worse symptom control and poorer PC quality.9,23 Some have suggested that discrimination may play a role. 24 For example, providers may see death as expected among the very old, who are then de-prioritized for PC. It is known that fewer persons with dementia receive palliative care in Canada in spite of increased mortality compared to those without dementia. 25 This study supports that, and found that presence of a dementia diagnosis remained associated with decreased odds even after controlling for impairments in communication and cognition. Further investigation into the structural barriers that play a role in reduced recognition of palliative needs, which includes receipt of palliative care services, is needed. Additionally, there was significant overlap in terms of these two underserved groups in this study; just over half (51.5%) of persons living with dementia were aged 85 + years. While the adjusted model took membership in each group into account, further research examining the compounding impact of membership in both of these groups (ie, interaction effect) on recognition of palliative needs, as well as other relevant outcomes, is warranted.
This study also showed that persons with mental illness have decreased odds of having recognized PC needs. Some have suggested that a lack of a robust social support system23,24 and poor integration of psychiatric and PC services26–28 may lead to this group being underserved in terms of PC. This study did find that fewer persons with mental illness were married and more had never been married. Further investigation into their informal support networks, as well as the status of their informal helpers, is needed.
Persons belonging to a linguistic minority also had decreased odds of recognition of palliative needs. A recent scoping review highlighted that language discordance between palliative care providers and recipients negatively impacts access to and the quality of PC, as well as advance care planning. 13 Language discordant health care also acts as a barrier to PC referral, satisfaction, and assessment.29,30 Being part of a linguistic minority implies being part of a minority group; further research should employ an intersectional lens to enhance understanding of PC inequities faced. 31
Interestingly, the present study found that those living in rural areas had marginally higher odds of having palliative needs recognized. There are many rural and remote communities in Canada that are underserviced or lack PC and hospice coverage entirely. 32 The Canadian Atlas of Palliative Care (2024) has recommended setting clear benchmarks to expand community-based service capacity in rural and remote areas. This study found that, after controlling for other characteristics, living in a rural area was associated with a 1% increase in the odds of having recognized palliative needs; it was associated with a 58% increase in the unadjusted model. This finding may be explained by the presence of one or more PC access facilitators in the rural communities, for example, telemedicine,33–35 multidisciplinary collaborative practices,36–37 and providers working alongside rural communities to meet their needs.38,39
Many personal, social, functional, and clinical characteristics were significantly associated with recognition of palliative needs in the adjusted model. For example, females were less likely to have palliative needs recognized, which has been reported in articles reviewed by Wong & Phillips (2023). 40 Further qualitative and quantitative researches should incorporate an intersectional lens to provide nuance to experiences and inequities. Not surprisingly, diagnosis of cancer was the strongest predictor of having recognized needs. While advances have been made, PC remains largely centered around cancer care.9,12,41 Nicholson and colleagues (2023) also describe the historically cancer-focused provision of PC and structural inequities that result from this. 42 Under this cancer-centered provision, diseases with uncertain trajectories and complex management are underserved. In accordance with this notion, the present study found that increasing levels of multimorbidity were associated with lower odds of recognized palliative needs. Other chronic conditions were associated with increased odds of recognized palliative needs, albeit not to the extent of a cancer diagnosis. The under-recognition of palliative needs among persons with multimorbidity, dementia, and advanced age becomes especially problematic when considering that multimorbidity and prevalence of dementia are expected to rise.9,12,42,43 As such, an approach focused on early and holistic identification of needs not only at the onset, but throughout the illness trajectory is needed.12,44
This study had both strengths and weaknesses. It was based on high-quality population-level data on home care clients across multiple Canadian provinces and territories, thereby painting an accurate picture of recognition of palliative needs of underserved groups across the country. While the study was able to examine a number of different underserved groups, there are others that were not examined. Other groups, such as persons experiencing homelessness, racialized individuals, indigenous people, 9 and persons with intellectual and developmental disabilities are also known to be underserved in palliative care.45,46 It should be noted that information on homelessness was not available, but will become available as jurisdictions transition from the RAI-HC to its updated version, the interRAI Home Care (interRAI HC). 15 Identification of persons with intellectual and developmental disabilities will also become possible in the update to the interRAI HC. Future work should not only further delve into the experiences and outcomes of groups reported in this study, but also consider other underserved groups. This study aimed to examine the impact of membership in an undeserved group on recognition of palliative needs, and considered several personal, social, functional, and clinical characteristics that are known to play a role. The goal was not to develop a full model predicting recognition of palliative needs. In the future, analyses should consider additional factors, as well as interaction terms to better understand the compounding impact of certain factors on recognition of palliative needs. Finally, this study looked at recognition of palliative needs, which included but was not limited to receipt of a palliative approach or palliative care services. As such, we do not know if the individuals identified as having recognized palliative needs actually received related care. Future research should also look at service utilization and outcomes over time.
However, the study positions itself well to fill a gap in research and information on underserved populations and the recognition of palliative needs. Additionally, the study uses high quality, population-level data where all variables are based on a validated instrument (the RAI-HC). The study also features a comprehensive analysis that considered variables across the personal, social, functional, and clinical domains.
Conclusion
This study showed that the palliative needs of some groups of home care clients are less likely to be recognized. As such, they may not be receiving the care they need and that would optimize their quality of life. Specifically, persons with mental illness, dementia, linguistic minorities, and those 85 + years of age had lower odds of recognized palliative needs despite adjusting for sociodemographic, clinical, and functional factors. Future work on promoting earlier identification and awareness of palliative needs is needed. This includes the early identification of persons who could benefit from a palliative approach to care to improve experiences and health outcomes. Future work should also consider an intersectional lens to examine experiences and outcomes especially within underserved groups. This will be an important step to provide a nuanced understanding of how risk factors interact within underserved populations.
Footnotes
Acknowledgements
Production of this document has been made possible through a financial contribution from Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
Ethical Considerations and Consent to Participate
The present study involved secondary analysis of anonymized data. Therefore, ethics approval is not required according to the Tri-Council Policy Statement 2022 Article 2.4B. An exemption was obtained from the Lakehead University Research Ethics Board.
Consent for Publication
Not applicable
Author Contributions
AB: Analyses, and paper writing
NW: Help with paper writing, assisted with analyses
LM: Conceptualized and designed the study, guided analyses, and assisted with paper writing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Canada,
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data are made available to interRAI Fellows (Martin) for research use under an existing license agreement interRAI has with the Canadian Institute for Health Information; note that the agreement is for research only, not commercial use. Students working under the supervision of an interRAI Fellow can apply for free access to the data but are subject to terms of use. As part of interRAI's agreement with the Canadian Institute for Health Information, the data may not be transmitted to third parties; therefore, the data used in this study cannot be made available to others. Those interested in using the data can apply directly to the Canadian Institute for Health Information for access.