
Abstract
Context
Incorporation of a palliative care approach is increasingly needed in primary care and nursing home care because most people with a life-limiting illness or frailty live there.
Objectives
To explore patients’ and relatives’ experiences of palliative care at home and in nursing homes.
Methods
Generic qualitative research in a purposive sample of patients with an estimated life expectancy of <1 year, receiving care at home or in a nursing home, and their relatives. Data is collected through semi-structured interviews and thematically analyzed by a multidisciplinary research team.
Results
Seven patients and five relatives participated. Three essential elements of palliative care and their contributing factors emerged: 1)
Conclusion
In both primary care and nursing home care, patients and relatives expressed the same essential elements of palliative care. They emphasized the importance of being recognized as a unique person beyond their patient status, receiving honest and clear information aligned with their preferences, and having care organized to ensure continuity. Adequate competence and skills are needed, together with a care organization that enables continuity to provide safe and person-centered care.
Keywords
Introduction
When a patient is faced with a life-limiting illness or frailty, the prioritization of a patients care shifts towards the quality of life and end-of-life considerations. 1 Patients confronted with life-limiting illness, prefer to stay at home or a home-like surrounding.2,3
In the Netherlands (NL), 41% of individuals with palliative care needs die at home, and 27% in nursing homes. 4 Home care is provided by general practitioners (GPs), district nurses (DNs) and nurse assistants. 5 Other paramedical professionals can support and treat patients at home.6,7 As multiple care-organizations are involved, multiprofessional consultation is not regulated. PATZ groups (palliative care at home) are available, in which professionals can collaborate on a voluntary basis. 8 When patients are unable to stay at home due to intensive care needs, nursing home care is available where care is primarily provided by nurse assistants, supported by nurses, in collaboration with physicians and other professionals. 9 Multiprofessional consultations are held for every patient at least twice a year. 10
Palliative care aims to improve the quality of life and dying through management of physical and psychological symptoms and social and existential concerns. 1 Assessment and management should be considered as a multidimensional experience in all four dimensions and is provided through an interprofessional collaboration of health care professionals (HCPs). 11 Patients’ and relatives’ values, wishes and needs should be the basis on which decisions are made. 11
Recognition and treatment of symptoms,12,13 the associated communication,12,14 as well as guidance in shared decision-making and psychological, social, and spiritual support, are essential for patients and relatives to experience good palliative care. 12 In practice, palliative care is often inadequate for patients cared for at home and in nursing homes as care is not integrated or integrated too late, symptoms and concerns are not recognized or uncharted, and many symptoms remain under or over-treated.15-18 Patients and relatives often experience deficiencies in palliative care competence, collaboration, percon-centered focus and access to HCPs.19-22 There is room for improvement, specifically in addressing the needs of patients andrelatives.15,23 A clear understanding of the experiences is essential for optimal palliative care in practice and integral to the quality of care,24,25 taking into account several patient characteristics, such as age, gender, educational level, place of residence and patients’ diagnosis, who have an effect on how care is experienced.26-29 The aim of this study is therefore to explore the experiences of patients and relatives with palliative care at home and in nursing homes.
Methods
Design
A generic qualitative study was conducted using inductive thematic analysis to explore the experiences of patients and their relatives with daily palliative care practices. 30 The study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) for reporting. 31
Participant Selection
A purposive sample of patients with an estimated life expectancy of less than one year who received care at home or in a nursing home were eligible for this study. If the patient could not be interviewed or was already deceased, the primary contact person (referred to as 'relatives') was interviewed. Maximum variation was sought with respect to sex, age, education, place of residence, and patients' diagnoses. The exclusion criteria were cognitive impairment and language barrier for both patients and relatives. Participants were identified and recruited through nursing homes, DNs and GPs in the central region of the NL.
Data Collection
Data were collected between May and October 2019 through semi structured interviews by one researcher (KK) at participants’ preferred locations. A topic list (supplementary material 1) was developed based on the Netherlands Quality Framework for Palliative Care, 11 and scientific literature. A multidisciplinary team of experts and one pilot interview, not included in the analysis, validated the topic list. The topics covered were: experienced care, identification of multidimensional symptoms and concerns, decision-making, communication with HCPs, continuity of care, the burden on relatives, and care recommendations. All interviews began with a broad opening question: 'How are you doing now, and what was the last period (last month) like for you?' to build rapport. Non-verbal expressions were noted in memos. After each interview, a methodological report was written consisting of 1) a brief description of the participant, 2) description of interview location and environment, 3) the course of the interview, 4) reflections on the questionnaire, and 5) other information. Member checks occurred during the interviews by summarizing the participants' responses. Data collection and analysis alternated, allowing for adjustments to the topic list as new insights emerged. Data collection continued until saturation was reached on the main themes. 32 All interviews were audio-recorded, transcribed verbatim, and anonymized. In addition, respondents’ demographic information was collected.
Data Analysis
A thematic analysis was performed following the method described by Braun and Clarke. 30 The data were analyzed within a research team to ensure research triangulation, comprising of an epidemiologist with qualitative research training (KK), a senior qualitative researcher (EdG), a nurse practitioner in palliative care and palliative care consultant (GH), and a senior researcher who is an oncology nurse (ST). After the initial three interviews, meaningful segments were identified through open coding independently by two researchers (KK and EdG). The findings were discussed, and preliminary codes were established. Subsequently, new participants were purposively included. This process repeated after the subsequent three interviews. After initial coding of the first six interviews, a consensus-based coding tree of main and subcategories, was developed by the research team. Subsequently, axial coding was conducted using NVivo 12. 33 In the analysis of the ninth interview, no new themes or additional meanings emerged. To ensure data saturation, three additional interviews were conducted. Demographic data were summarized using Microsoft Office Excel, version 2016. 34
Ethical Considerations
This study was conducted following the principles of the Declaration of Helsinki 35 and the General Data Protection Regulation. 36 The Utrecht Medical Research Ethics Committee classified this study as exempt from the Medical Research Involving Human Subjects Act (WAG/mb/19/010 438). All participants received written and verbal information and informed consent was obtained before each interview.
Results
Participants Characteristics
Participants Characteristics (n = 12).
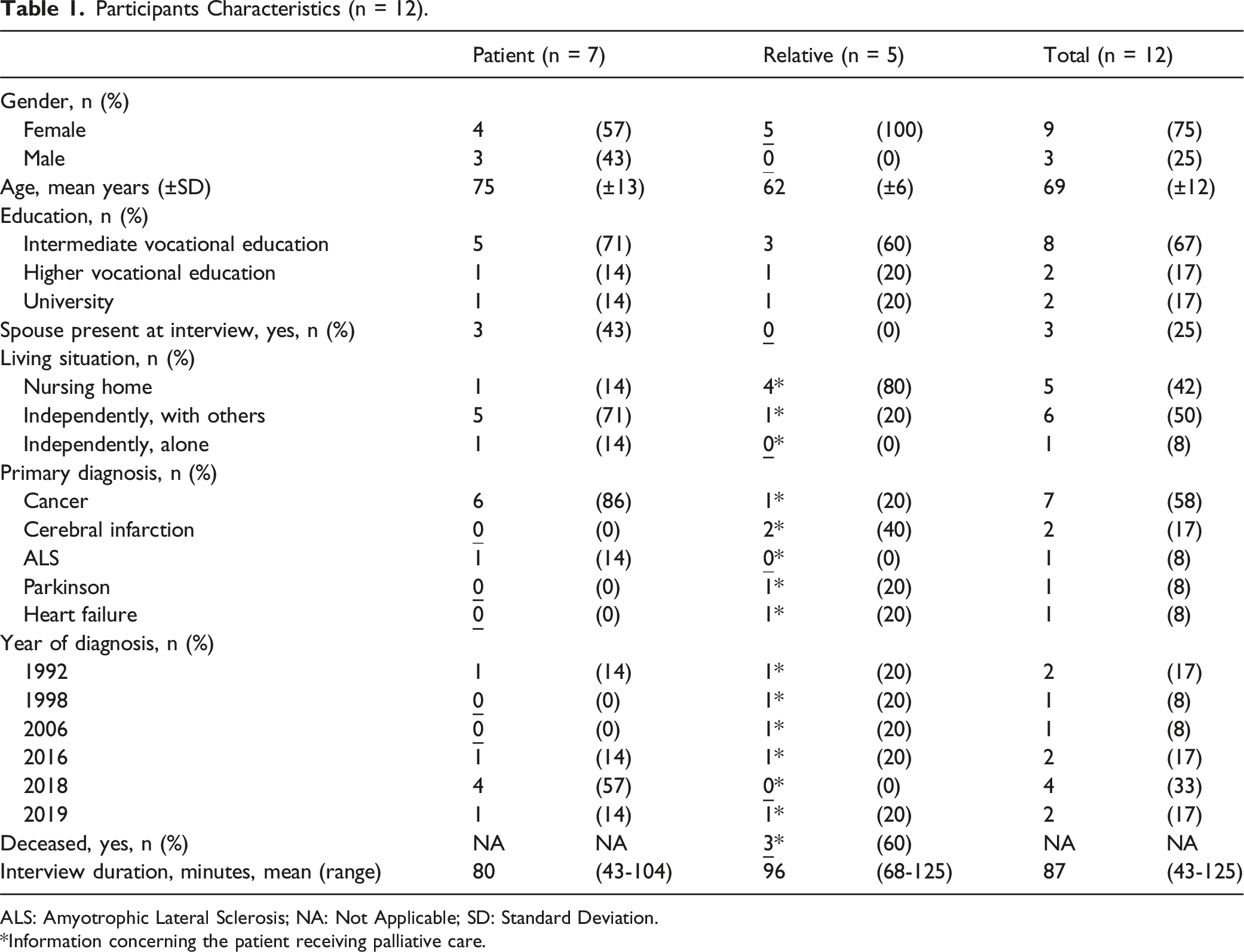
ALS: Amyotrophic Lateral Sclerosis; NA: Not Applicable; SD: Standard Deviation.
*Information concerning the patient receiving palliative care.
Essential Elements of Palliative Care
Initially, all participants stated to be satisfied with the care provided and were hesitant in sharing of and reflecting on undesired experiences. Undesired situations often stemmed from inappropriate interactions with specific HCP. Participants linked these experiences primarily to inadequate education/training, workload, staff and financial shortage, and bureaucracy.
Quotes per Identified Theme.
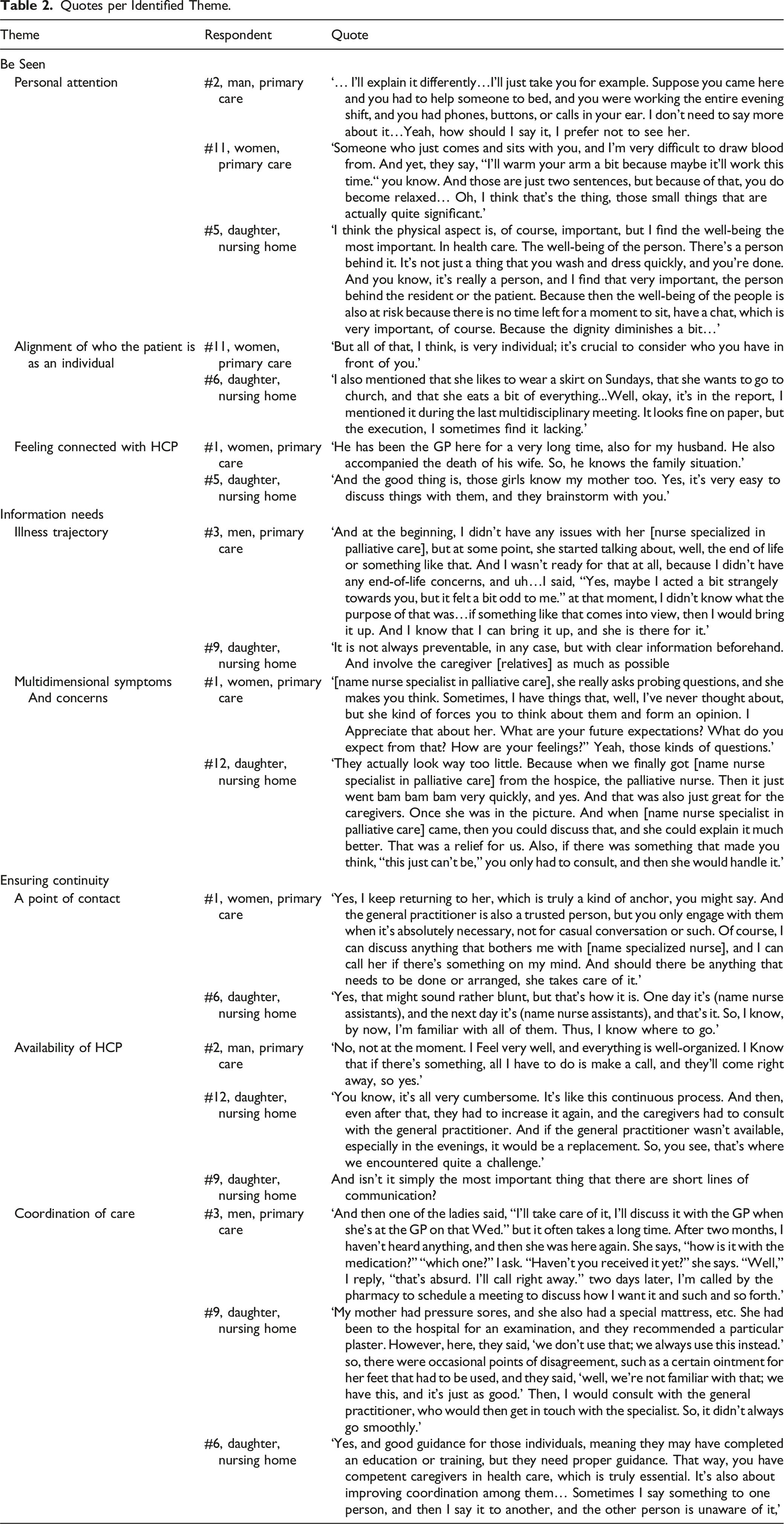
Essential Element 1: Be Seen
The most outstanding essential is ‘be seen’, which refers to the feeling of being seen as a person rather than the illness through personal attention, alignment to who the patient is as a person and feeling connected.
Personal Attention
All participants expressed a need for empathy. The HCPs’ attitude and communication competencies are vital. Further, this need manifests in HCPs being present in the moment, listening attentively, and conveying that they are not in a hurry. This is crucial in routine care but extends to engaging in conversations, sitting with the patient, stopping by, and remembering details previously discussed. Participants value HCPs who exhibit warmth, empathy, understanding, and genuine interest, and make patients feel that their concerns matter, taking them seriously and treating them as equals in the conversation.
Alignment to Who the Patient is as an Individual
It is crucial for participants that care is tailored to the individual and aligns with the patient’s identity. To achieve this, HCPs must delve into the person behind the patient. This involves knowing the patient’s preferences, such as their food and music choices, their interests, and their personality. When this personalized approach is not integrated into care and systematically incorporated, participants feel that their autonomy and voice are not respected.
Feeling Connected with HCPs
Participants emphasized on the importance to feel connected with the HCPs by developing a relationship that goes beyond a purely professional connection and involves a genuine bond where they know each other well. This connection impacts the participants' emotional state, trust, and the quality of interactions. A consistent team of HCPs contributes to fostering these personal connections.
Essential Element 2: Information Needs
Information needs refers to the need for a proactive approach with means of information on illness trajectory and multidimensional symptoms and concerns.
Illness Trajectory
Participants require comprehensive information about their illness trajectory, by means of professional expertise, clear expectations for different scenarios, explanations for the care process, and guidance on what questions and wishes they can express. It is essential for this guidance to commence from the outset of the trajectory and to adapt continuously to the needs and preferences of the patient or relative. Conversations about illness, dying, and death often do not occur until the patient’s condition deteriorates or the terminal phase is identified and is influenced by the patient’s or relative’s ability to accept the illness. Relatives require additional guidance from HCPs on how to support their loved ones through the illness trajectory. This includes information about what is considered normal, how the illness presents itself, and what the dying process entails.
Multidimensional Symptoms and Concerns
Participants, especially relatives, require HCPs who can anticipate and outline scenarios for potential future care to prevent symptoms and undesirable situations. Moreover, participants highly value clarity regarding symptoms and interventions, leveraging the expertise of HCPs. This need intensifies as the patient’s condition deteriorates. In most cases, participants experienced a reactive HCP approach, with some being proactive by asking questions. Most HCPs have conversations with participants about advance directives but have less attention to additional proactive care agreements.
Furthermore, the emphasis of care is primarily placed on physical symptoms, aligning with participants' expectations. Support for psychological symptoms, and social and spiritual concerns is often sought within the family. One patient mentioned an HCP who monitored symptoms over time using a symptom diary, which was highly appreciated by the patient.
Essential Element 3: Ensuring Continuity
The last essential element for patients and their relatives is ‘ensuring continuity’ which refers to organizational aspects of care: single point of contact, availability of HCP, and coordination of care.
Single Point of Contact
All participants value a dedicated contact person to guide them through the course of illness. This professional, whom they trust and can confide in regarding their symptoms, concerns, and fears, should have palliative care expertise and be available to answer questions, provide support at every stage of the illness, and aid in preparing for future care. Most participants could not identify a contact person.
Availability of HCPs
The availability of HCPs means that participants can always reach out to an HCP, whether by phone, email or in person, for questions or consultations. Most participants appreciate regular consultations, even when the patient’s condition is stable. In addition, undesired situations are experienced with fluctuating personnel. Most participants expressed the need for more frequent contact with physicians or nurses who can coordinate care and treatment. Furthermore, the presence HCPs who are qualified to make informed decisions becomes particularly important as the illness progresses and becomes unstable.
Coordination of Care
Participants value HCPs support for practical aspects and stress the need for improved collaboration and communication across health care settings. They experienced issues in hospital-district teams and or GP and hospital-nursing home communication, mainly due to information loss and care plan disagreements. Internal collaboration challenges included inconsistent care plan communication, insufficient information during patient transfers, and unclear roles and responsibilities.
Discussion
This study explored the palliative care experiences of patients with a life-limiting illness at home and in a nursing home and their relatives. Three essential elements of palliative care emerged:
Patients and relatives in both settings perceived the same essential elements of palliative care. In a study on barriers to providing palliative care for patients at home or in nursing homes with HCPs we found that barriers differed within the settings; in primary care, mainly organizational barriers were identified whereas, in nursing homes, most barriers were related to care content. 37 ‘Be seen’, ‘information needs’, and ‘ensuring continuity’ seem to be preconditions for patients to live their lives, regardless of the environment, given the conditions of the palliative phase.
Our study highlighted the importance of how HCPs provide care. Undesired experiences were largely influenced by a specific HCP. As a result, patients depend on luck when it comes to the HCP attending to them at their bedside. 38 HCPs effectiveness can be shaped by care organization constraints like workload and staff shortages. However, it goes beyond time; patients and relatives acknowledge these challenges. The key factors lie in the attitudes and competencies of HCPs. To see a patient as a unique person stood out the most. Several other studies confirmed this importance. Studies in home care showed that palliative care patients preferred care that supported to ‘be seen as the person they had always been’, 3 and focus on the person was an element that patients and relatives considered essential. 21 Another study under palliative care patients in home, nursing homes and hospitals and their relatives showed that a ‘death in which one could maintain a connection with one’s previous identity’ was described a good death. 39 A conceptual framework to understand the patient experience, sets the person across the whole continuum, indicating that the patient and user of health care services is the same unique person they have been. 40 Other studies with patients in the palliative phase in various settings support our results as they identified the importance to feel safe in the place of care, 41 that palliative care focused on living a meaningful life, 13 and that palliative care included respect and empathy. 42 Furthermore, showing empathy, which involves perceiving a patient as a unique individual, and providing open and honest information is essential for effective communication, 43 which results in turn in favorable outcomes. A study by Westendorp et al showed that information that an HCP conveys with empathy is remembered better than information shared without empathy 44 ; which also enhances shared decision-making. Other studies revealed that empathic communication and providing specific prognostic information enables symptom control, guides decision-making and has an immediate effect on how the patient feels, on the satisfaction of patients, feelings of insecurity and fear, on the trust they have in HCPs, and on the future.43,45-47 However, patients often perceive communication with HCPs as ineffective.48-50 In our study on barriers in primary care and nursing homes, HCPs did not perceive barriers in communication with patients and relatives, which exposes the necessity of communication. 37 In addition, all three essential elements help HCPs to shape proactive palliative care. Patients and relatives who feel seen as a person, receive clear and honest information, and who have a single point of contact and HCPs that are available, may as well be more open about their symptoms and concerns, may be more willing to engage in conversation about (future)care needs, death and dying, 51 know what to expect which helps them to make well-considered decisions and positively influences symptom management.
Strengths and Limitations
A strength of this study is the inclusion of participants from both primary care and nursing home settings, providing a comprehensive understanding of essential palliative care elements among patients and relatives. Participants varied in gender, education, patients’ place of residence and patients’ diagnosis, providing a presentation of various experiences among a diverse group. The diversity in age was limited; younger patients might have other essential elements that are important to them due to an active family life and younger children. Mainly primary care patients and nursing home relatives were interviewed due to contextual constraints. Participants tended to express satisfaction with care rather than undesired experiences. Efforts to explore these experiences were challenging, possibly due to care dependency. A common strategy involved presenting a hypothetical undesired situation, prompting participants to share their own experiences. This strategy resulted in additional information on undesired situations, which was not spontaneous.
Implications
This study highlighted that the essence of palliative care is not always optimal. HCPs must be aware of their impact on patients' and relatives’ well-being simply on how they engage and communicate with them. Experiences of patients and relatives are highly influenced by their interactions with HCPs. An empathic attitude and competencies, especially on communication, are important in providing palliative care. To support HCPs in daily practice, education and training should focus on communication skills, with a special endorsement for nursing staff given their extensive interaction with patients and relatives. Further, incorporating an increased use of PROMS, such as the Utrecht Symptom Diary four dimensional (USD-4D),52,53 could help HCPs in their communication with patients and relatives and to really put the values, wishes and needs first.
Conclusion
Patients living at home and in nursing homes, along with their relatives, expressed the same essential elements of palliative care that matter to them. They emphasized the importance of being recognized as a unique person beyond their patient status, receiving honest and clear information aligned with their preferences, and having care organized to ensure continuity. HCPs should be aware of these essential elements and should use these insights as guidance for daily practice. Adequate competence and skills are needed, together with a care organization that enables continuity in order to provide safe and person-centered care.
Supplemental Material
Supplemental Material - Being Seen as a Unique Person is Essential in Palliative Care at Home and Nursing Homes: A Qualitative Study With Patients and Relatives
Supplemental Material for Being Seen as a Unique Person is Essential in Palliative Care at Home and Nursing Homes: A Qualitative Study With Patients and Relatives by Katrin Kochems, Everlien de Graaf, Ginette M. Hesselmann, and Saskia C. C. M. Teunissen in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
We thank all participants who took the time to share their experiences with us and all contact persons from nursing homes and PaTz groups who helped us with the recruitment. In addition, we thank the multidisciplinary team of experts for their help in validating the topic list and the patient by whom we could pilot-test the topic list.
Author Contributions
KK did the interviews and took part in the conception and design of the research, performed the data collection, took part in the data analysis, and drafted and critically revised the manuscript. EdG, ST and GH took part in the conception and design of the research, and data analysis and critically revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is part of the KWASA study (KWAliteit van zorg; SAmenwerken in signaleren en besluivormen in de palliatieve fase; Quality of care; Collaboration in signaling and decision making in the palliative phase), supported by the Netherlands Organisation for Health Research and Development [grant number 844001506]. The funding party did not take part in the conception and design, data collection, and analysis, nor in drafting or revising the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.