
Abstract
Background
Nurses play an important role in palliative care, and high-quality assessment tools can help standardize palliative-related nursing behaviors, but there are no such tools in China.
Objective
This study aimed to revise, cross-culturally adapt, and validate the Palliative Nursing Care Quality Scale (PNCQS) to provide an effective tool that can help nurses in mainland China assess the quality of palliative care.
Methods
This study involved a 2-steps process. First, the PNCQS was translated, back-translated, and cross-cultural adapted using Brislin's translation model. Second, a cross-sectional study was used to evaluate the reliability and validity of the revised scale. From January to February 2023, 367 nurses engaged in palliative care-related nursing from 3 tertiary A general hospitals were surveyed with the revised scale. The evaluation methods used in this study included item analysis, test-retest reliability, internal consistency, criterion-related validity, content validity, and construct validity.
Results
The PNCQS-Chinese included 20 items. In this study, the item-total correlation coefficients ranged from 0.67 to 0.83 (P < .01), and the critical ratio value of the items was 12.10 to 23.34 (P < .01). The scale-level content validity index was 0.98, and the item-level content validity ranged from 0.86 to 1.00. The total Cronbach's α and test–retest reliability of the scale were 0.96 and 0.79, respectively. Factor analysis of 20 items extracted 1 factor, and the contribution rate of cumulative variance was 60.03%.
Conclusions
PNCQS-Chinese shows acceptable validity and reliability for assessing the quality of palliative care-related nursing in mainland China.
Introduction
Palliative care (PC) aims to improve the quality of life for end-stage patients and their families. This goal can be achieved by controlling pain discomfort symptoms, alleviating physical and psychological suffering. 1 With the rapid progress of modern healthcare systems, the quality of dying has gained widespread attention. 2 By the end of 2020, the population of individuals aged 60 and above in China had increased to 264 million, 3 as well as a notable increase in the prevalence of chronic noncommunicable diseases, such as cardiovascular diseases and cancer.4,5 Consequently, there is a growing demand for PC services in China.6,7 However, the resources of PC services in mainland China remain limited. 8 Firstly, this situation can be ascribed to the impact of Chinese traditional culture, rendering it arduous for individuals to relinquish life-saving measures and embrace PC support.9,10 Furthermore, hospice wards usually do not carry out examinations and operations, which does not bring much economic benefits to hospitals and results in relatively lower wages for staff. 11 Additionally, medical staff in hospice wards frequently confront death, leading to heightened psychological burdens. 12 Therefore, there is still a shortage of places for professional PC in China, and most terminal patients are still treated in general hospitals.6,13 Consequently, the responsibilities of PC are borne by some departments of many hospitals, such as the intensive care unit (ICU) and oncology department. Some nurses in these departments will undergo professional training to undertake PC while engaged in nursing work. 11 Ning et al 14 proposed that PC should be the basic skill for medical staff in departments providing medical care to end-stage patients. Notably, as a group in a special stage of disease, dying patients have posing challenges to medical institutions and staff. 6 Improving the quality of life of patients in the terminal stage and assisting their families in coping with the death of their loved ones is a problem that requires increased attention from medical staff in general hospitals.
Quality assessment is an essential element in the evaluation of the worth of medical services, including PC, as it aids managers in identifying deficiencies in quality and furnishes valuable insights for the formulation of future strategies. 15 According to Mularski et al, 16 the primary domains for evaluating the quality of PC encompass symptom management, patient satisfaction, interpersonal dynamics, decision-making and care planning, continuity and communication, family burden and well-being, as well as the quality of the dying process and end-of-life experience. A study indicated that nurses undertake various roles in the PC process, such as disease observers, professional caregivers, multidisciplinary team coordinators, and educators. 17 Moreover, nurses and patients’ families communicate closely, therefore, they can easily identify the physical, psychological, and social problems faced by patients and their families.18,19 In summary, nurses play crucial roles in establishing professional PC teams. 20 Thus, assessing the quality of PCs provided by nurses is critical to improving the quality of patient care. The European Association for Palliative Care recommends various measurement tools to assess PC services: these tools should assess the needs of patients and their caregivers.21,22 In China, however, recent empirical studies on the quality of palliative nursing care are scarce, 8 and a unified and standardized tool is still being explored and improved. Currently, the main quality assessment tools related to PC include the McGill Quality of Life Questionnaire, 23 the Questionnaire Quality from the Patient's Perspective for Palliative Care, 24 and the Palliative Care Self-Reported Practices Scale (PCPS). 25 However, the above scales do not assess the ability of clinical nurses to care for dying patients in mental care, grief counseling, social continuity support, and multidisciplinary team care. Given the importance of nursing staff, it is obvious that the above tools for assessing the quality of PC nursing are not comprehensive.
The Palliative Nursing Care Quality Scale (PNCQS), developed by Zulueta-Egea et al 26 in 2020, was designed and validated by professional nurses and nurses working in palliative settings, including hospital, hospital support, social health, and home support. The primary aim of the PNCQS is to comprehensively assess the quality of palliative nursing care. This assessment encompasses the management of patients’ disease symptoms and the provision of psychological support by nurses to patients and their families. Additionally, it involves meeting the needs of families and primary caregivers, promoting active involvement of patient caregivers in the care process, establishing therapeutic relationships with patients and their families, offering moral support, and ensuring the continuity of care. The scale has been introduced in Turkey and applied to oncology clinics, ICUs, and PC clinics, where it exhibited favorable psychometric properties. 27 Professional scale assessment can promote continuous self-reflection, enhancement, and optimization of PC quality among PC practitioners. Considering the inherent advantages of the PNCQS and its capacity to guide nurses in delivering exceptional end-of-life care, this study aimed to introduce the PNCQS to measure nursing staff engaged in PC-related nursing within Chinese hospitals, thereby establishing a dependable measurement tool for future assessments of PC quality in China.
Methods
Study Design
The present study was conducted in 2 distinct phases: (1) The translation, back-translation, and cross-cultural adaptation of the PNCQS; (2) a cross-sectional study to assess the psychometric properties of the PNCQS-Chinese. The translation of the PNCQS was conducted in accordance with Brislin's translation model while adhering to the established guidelines for the process of cross-cultural adaptation of self-report measures.28,29
Setting and Participants
From January to February 2023, nurses from 3 tertiary A general hospitals in XX Province were selected as participants through a nonprobabilistic convenience sampling. The inclusion criteria were: (1) Engagement in clinical nursing work in the ICU or oncology clinic for more than 6 months; (2) having the experience of caring for dying patients in the past 6 months; and (3) having a registered license to practice as a nurse. The exclusion criteria were: (1) Nurses who discontinued their participation midway through the survey; (2) nurses who were absent during the investigation due to sick leave, maternity leave, or other circumstances. The sample size calculation method was based on the international questionnaire design principles and psychological measurement principles, which recommend that the sample size should preferably be 5 to 10 times the number of items. 30 Moreover, the sample size of reference exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) should be at least 100 and 200 cases, respectively.30,31 Considering that PNCQS contains 20 items and a 10% loss to follow-up rate, a minimum of 330 nurses were required for this study.
Measurement Instruments
The general information questionnaire: Based on a review of relevant literature26,27 and group discussion, the research team developed a questionnaire including variables such as age, gender, education level, marital status, department, PC training experience, and job tenure.
The PNCQS, developed by Zulueta-Egea et al 26 in 2020, has 20 items and 1 dimension. Items are rated on a 5-Likert scale from 1 = never to 5 = always, and the total score range from 20 to 100, with higher scores indicating better quality of PC provided by nurses. In the initial study, the scale demonstrated a Cronbach's α coefficient of 0.94.
The PCPS was developed by Nakazawa et al 32 in 2010, and introduced to China by Zhao et al in 2021. 25 The scale is a self-assessment tool that nurses and other professionals can use to assess their performance during PC practice. The scale contains 18 items, and items are scored on a 5-point Likert scale from “never” to “always”.
Development Process of the Research
Step 1: Revision and Cross-Cultural Adaptation
Translation: The language of the scale in the initial study was Spanish. The researchers contacted the original author by email and obtained the approval of the PNCQS (in English). We believe that adopting the original author as the translator and rendering PNCQS into a broader English rendition could potentially enhance the semantic equivalence of the Chinese version of the scale. Additionally, maintaining communication with the author ensures the translation's professionalism. After that, the scale was translated according to Brislin's translation model 33 using the specific steps: (1) Forward translation: a nurse from the oncology unit (with a master's degree, the College English Test-6 certificate, and had received PC-related training) collaborated with a doctor specialized in ICU (with a doctoral degree and had experienced studying abroad). Their collaboration aimed to adapt the language used in the study to align with the language-expression habits in mainland China, obtaining PNCQS-1 and PNCQS-2; (2) Comprehensive comparison: professor with a doctoral degree, 4 years experience of studying abroad, and expertise in PC conducted a comprehensive comparison of PNCQS-1 and PNCQS-2, identifying and rectifying any inconsistencies to form PNCQS-3; (3) Back translation: PNCQS-3 was translated into PNCQS-4 and PNCQS-5 by 2 professionals, one of whom is a nurse with a master's degree with 3 years of PC nursing experience, and the other is a bilingual translator (a long-term translator) who had never seen the scale. Finally, the translation team convened a discussion session to compare PNCQS-4 and PNCQS-5, analyzed, and revised contentious elements per China's national circumstances. At last, the PNCQS-6 was established to enhance cultural congruence.
Expert panel: In order to assess the appropriateness and consistency of the content of the PNCQS-6, experts were invited to assess the pertinence, suitability, and linguistic clarity of each item in relation to the research topic. The selection criteria for experts encompassed the following: (1) At least 5 years work experience in the field of PC-related nursing; (2) familiarity with the development and application of measurement tools; (3) willingness to participate in this research. Almanasreh et al 34 suggested that an odd number of group members should be involved in the expert panel on the content validity, and that at least 3 experts should be involved. Eventually, 7 experts were invited. The panel comprised 2 associate professors of nursing, both of whom had doctoral degrees and expertise in scale localization processes and methods, as well as a track record of publishing relevant papers. Additionally, a chief nurse and a deputy chief physician with rich clinical management experience were selected. It also comprises 3 nurses who are also involved in the translation process, including 2 with a master's degree and one with a bachelor's degree (who has obtained a professional PC-training certificate). A questionnaire was used at this stage to evaluate the relevance of each item to the test topic. The questionnaire was assessed using a 4-point Likert scale, which ranged from 1 (indicating irrelevance) to 4 (indicating high relevance). Experts evaluated the questionnaire items for content consistency, readability, and language appropriateness based on their understanding of the concept of PC and their expertise. Experts were required to provide explanatory notes in cases where the experts deemed it necessary to make modifications.
Pretests: In order to ensure the comprehensibility and appropriateness of the revised PNCQS-6 for the intended population, a sample of 30 nurses with experience in PC nursing was selected for a face-to-face questionnaire survey. Participants were instructed to indicate any questions they found difficult to comprehend during the response process and provide suggestions for improving unclear sections. An item on the scale was re-evaluated or revised if 20% of the participants found it unclear. Ultimately, the version of the PNCQS-Chinese was established.
Step 2: Evaluation of the Psychometric Properties of the PNCQS-Chinese
1. Item analysis
The critical ratio (CR) and correlation coefficient methods were used in this study. The CR method indicates the degree of reflection of various respondents. First, the total score for each item on the scale was computed, and the total score was arranged in descending order. The top 27% and bottom 27% of scores were classified as high and low scores, respectively. The independent sample t-test was conducted to compare the disparities between the high-low score group. Items exhibiting no statistical significance or with a CR value below 3.00 were eliminated from the analysis.
35
The degree of correlation was ascertained by calculating the correlation coefficient between each item and the total score of the scale. Items with a correlation coefficient below 0.40 or lacking statistical significance were excluded.
36
2. Reliability analysis 3. Validity analysis
Internal consistency, as measured by Cronbach's α, was used to assess the homogeneity and inherent correlation among items. The Cronbach's α coefficient of the removed item was analyzed simultaneously. If the Cronbach's α coefficient does not increase significantly upon deleting any item, no items need removal.
37
Test-retest reliability was used to evaluate the stability and consistency over time.
38
During data collection, a separate test-retest team was set up to check the test-retest reliability, including 60 nurses, who were investigated again 3 weeks later using electronic questionnaire under the same measurement conditions. For accuracy, we excluded nurses who rotated or studied in the department during test-retest intervals to ensure that the measurement conditions were as consistent as possible. If the correlation coefficient between the total scores of the 2 measurements exceeded 0.70, indicating a favorable level of test-retest reliability.
This study used content validity to assess the adequacy of items and appropriateness of content within the questionnaire. After the translation phase, a panel of 7 experts in PC was invited to evaluate the relationship between the items of the PNCQS-Chinese and the total scale. The item content validity index (I-CVI) for each item was determined by having the experts assign a score ranging from 1 to 4, reflecting the perceived importance level of the item content. Higher scores indicated greater significance of the item content. The I-CVI was calculated by dividing the count of experts who were assigned an item score of 3 or 4 by the total count of experts involved in the evaluation. The scale content validity index average (S-CVI/Ave) of the scale was determined by averaging the I-CVI values, which were typically ≥ 0.78. Additionally, the S-CVI/Ave was reported to be 0.90.
34
Construct validity concerns the inherent properties of the tool, which can be measured through EFA and CFA, 39 EFA, which is performed by principal component analysis and maximum variance rotation method, 40 should be used when the Kaiser-Meyer-Olkin (KMO) value is > 0.60 and the Bartlett spherical test is statistically significant (P < .05). The final selected factor and item must satisfy the requirements of factor of feature root ≥ 1 and factor load value ≥ 0.40. A cumulative explanatory variability of more than 40.0% of common factors is considered acceptable. CFA is used to evaluate model fit and is considered to fit well when the following criteria are met: chi-square degree of freedom ratio (χ2/df) ≤ 3.00, root mean square value of approximate error (RMSEA < 0.08), comparative fit index (CFI) > 0.90, incremental fit index (IFI) > 0.90, and Tucker-Lewis index (TLI) > 0.90. 31
Criterion-related validity: The method of concurrent validity, a form of criterion validity, was adopted to assess the extent to which a novel instrument aligns with established measures or gold-standard benchmarks simultaneously. 40 The Chinese version of PCPS was used as the reference scale for evaluation. 25 Pearson correlation test was used to assess the relationship between PNCQS-Chinese total score and PCPS scale.
Known-Group validity was assessed in this study by dividing the subjects into groups based on age, gender, education, marital status, department, PC training experience, and job tenure to determine if there were statistically significant differences in the total score of PNCQS-Chinese among these groups.
Data Collection
Data collection for this study involved the utilization of a general information questionnaire developed by the researchers, as well as the PNCQS-Chinese. The online electronic questionnaires were constructed using the Questionnaire Star Platform. The primary objective of the study was clearly stated on the home page of the questionnaire, and the participants rights to informed consent and privacy were protected. After obtaining the approval of the relevant hospital departments, the investigation team will distribute the questionnaire to eligible qualified nurses. The collected questionnaires were meticulously reviewed and filtered by 2 researchers, who excluded those with abnormal responses and missing data. The average time to complete the questionnaire is about 5 minutes.
Statistical Analysis
Two individuals conducted data integration to ensure the accuracy of the statistical questionnaire information. Statistical analysis was performed using SPSS (Version 26.0), and CFA was conducted using AMOS (Version 28.0). The function to identify repeated entries in SPSS was used to eliminate duplicate questionnaires. The skewness and kurtosis test results indicated conformity with a normal distribution. 41 Quantitative data was represented using the mean and standard deviation (SD), and qualitative data was summarized using frequency and percentage. Descriptive analysis, independent t-tests, and ANOVA were used to explore the characteristics and distribution of PNCQS-Chinese.
Ethical Considerations
This study obtained approval from all participating institutions and the ethics committee of the hospital where the research group was situated (QYFY WZLL 26722). We informed respondents of the purpose of the survey in the questionnaire and ensured that the survey was performed according to their preferences.
Results
Revision and Cross-Cultural Adaptation
During the stage of revision and cross-cultural adaptation, the study collated and revised the questions raised by various nursing experts and the questions raised by 30 nurses on the items of the scale during the preinvestigation. Experts recommended that the phrasing of each component should maintain consistency and adopt a first-person perspective, thereby enabling the respondents to fully immerse themselves in the given context. For instance, examples such as “I conduct a comprehensive evaluation of the pain” and “I provide the necessary measures for the symptom management” were suggested. The original content of item 10 on the scale was “Use active listening and silence for nonjudgmental understanding of the feelings.” However, the words “active listening” and “silence” were regarded as conflicting concepts when translated into Chinese. This is because experts believe that active listening should contain appropriate responses, so they should not be juxtaposed with “silence.” Finally, this study modifies the item to “I know how to actively engage in effective listening, comprehend the emotions, thoughts, and convictions of patients and/or families, while refraining from passing judgment.” Likewise, item 18 “Ask open and specific questions to support the patient in his/her decision making or final wishes.” During the preinvestigation, some nurses responded that they did not know how to distinguish between “open questions” and “specific questions.” Therefore the expert committee reconvened to discuss it again. Experts believe that A and B in Chinese refers to the part where the concepts of A and B overlap, while A or B encompasses not only the overlap of the 2 concepts but also the concept itself. In this scale, “open questions” and “specific questions” should be understood in relation to “or” rather than “and.” Therefore, we changed “and” to “or.” We changed “ensure” to “focus” in Item 19 because the experts believed that many nurses are not powerful enough as they are not managers. “ To ensure that coordination between all team members and the different levels of care” may be challenging for a nurse without a position to achieve. All items were considered to be retained, and the contents of each item reflected the quality of care in PC.
Participant Characteristics
A total of 367 samples were included in the data analysis, comprising individuals aged 22 to 45 years (mean age: 31.47 ± 5.62). Among these samples, 45 cases (12.26%) were male, while 322 (87.74%) were female. Furthermore, 165 (44.96%) participants were recruited from the ICU, and 202 (55.04%) from the Oncology Clinic. Additionally, 96 (26.16%) nurses reported receiving training in PC (Table 1).
General Characteristic of the Participants (N = 367).
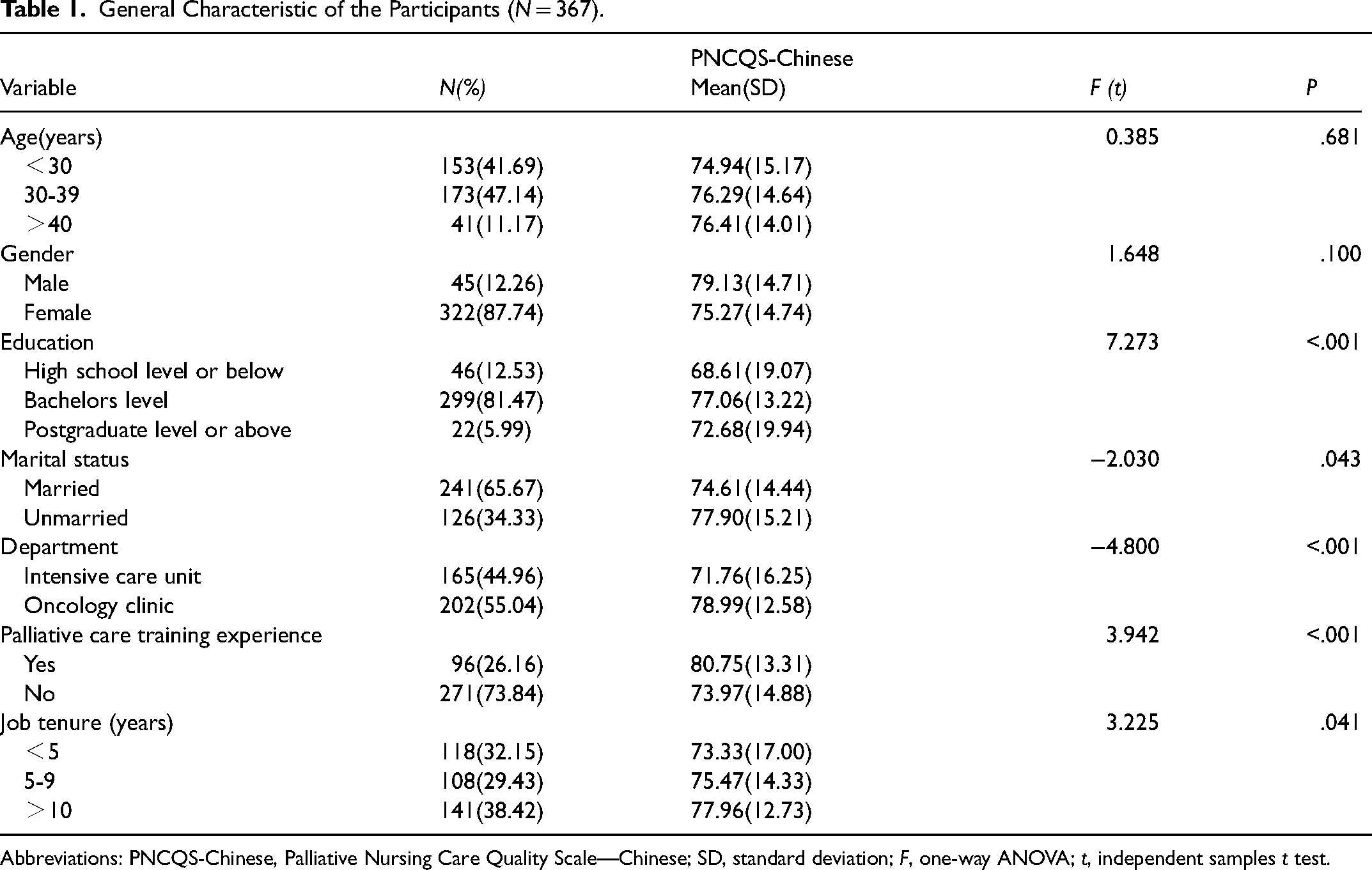
Abbreviations: PNCQS-Chinese, Palliative Nursing Care Quality Scale—Chinese; SD, standard deviation; F, one-way ANOVA; t, independent samples t test.
Item Analysis
The findings indicate that the critical value of CR for each item ranged from 12.10 to 23.34 (P < 0.01), surpassing the minimum standard of 3. Furthermore, the correlation coefficient between the score of each item and the total score of the scale ranged from 0.67 to 0.83, with all coefficients exceeding 0.40. Consequently, it is recommended to retain all items (Table 2).
Psychometric Properties of PNCQS-Chinese.
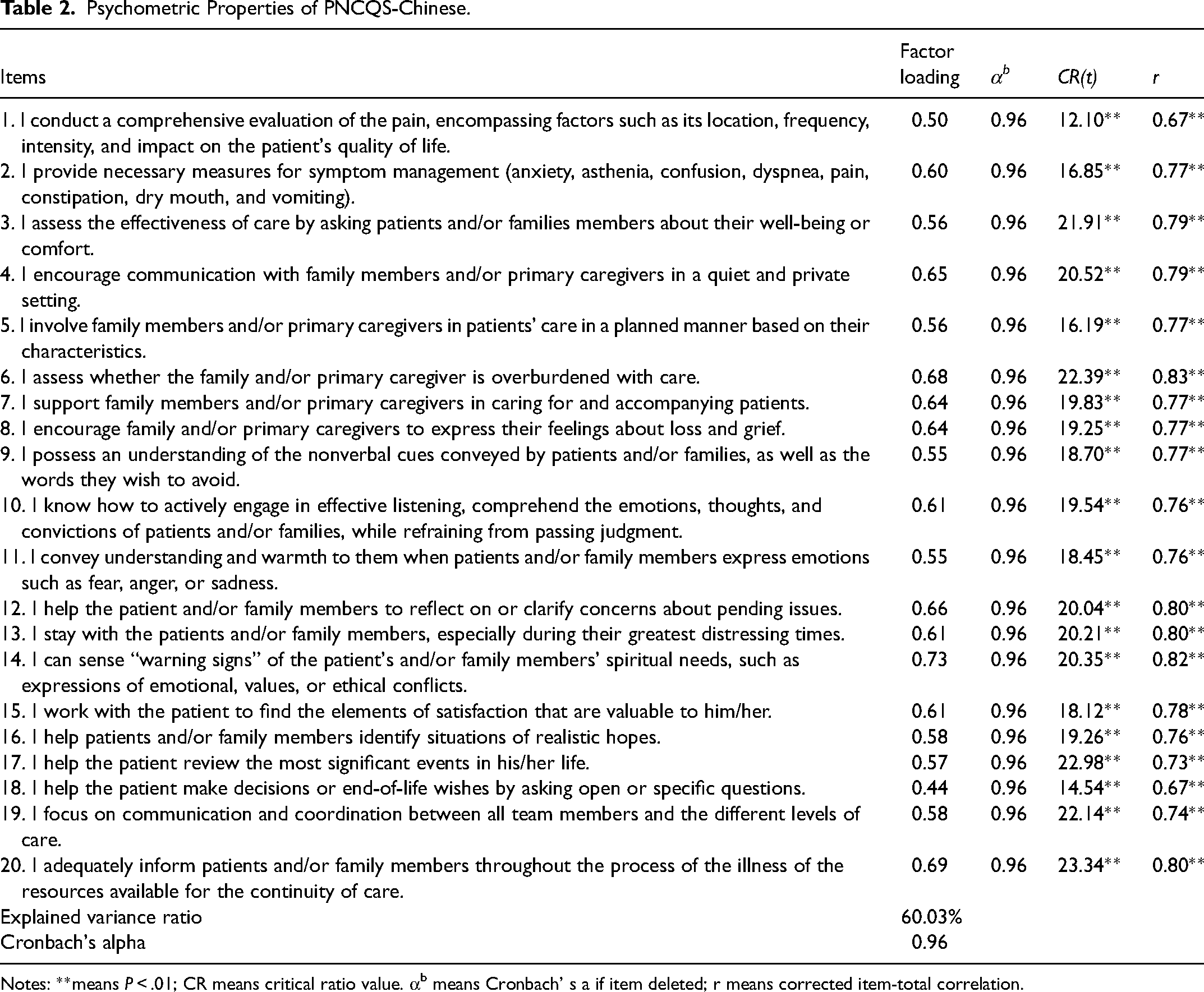
Notes: **means P < .01; CR means critical ratio value. αb means Cronbach’ s a if item deleted; r means corrected item-total correlation.
Reliability Analysis of PNCQS-Chinese
The Cronbach's α coefficient for PNCQS-Chinese was found to be 0.96. Deleting each item did not significantly increase the Cronbach's α coefficient, indicating that no entry should be deleted (Table 2). Following a 3-week interval, the scale was readministered to 60 clinical nurses who completed the initial questionnaire. However, 6 nurses dropped out of our survey, and 1 nurse did not complete the questionnaire. Consequently, the analysis was conducted on 53 questionnaires. Ultimately, The retest reliability coefficient was 0.79.
Validity Analysis of PNCQ-Chinese
Content validity: After consultation with 7 experts in PC-related nursing, the I-CVI of the Chinese version of PNCQS was 0.86 to 1.00, and the S-CVI/Ave was 0.98.
Structural validity analysis results: A total of 152 samples were randomly selected from 357 questionnaires to conduct EFA. The findings indicated that the Chinese version of PNCQS had a KMO value of 0.96 and Bartlett's spherical test value of 3314.49, with a significance level of P < .01, satisfying the requirements for factor analysis. Principal component analysis and the maximum variance orthogonal rotation method were used to extract a single common factor. The standardized load values of the factor model ranged from 0.44 to 0.73, all exceeding the threshold of 0.40. No violations of estimation occurred, and the cumulative variance contribution accounted for 60.03%. The specific factor loadings can be found in Table 2. Based on a sample size of 215, the CFA yielded an optimal model fit, as evidenced by the fit indices χ2/df = 2.267, RMSEA = 0.077, CFI = 0.912, TLI = 0.901, and IFI = 0.913 (Figure 1).
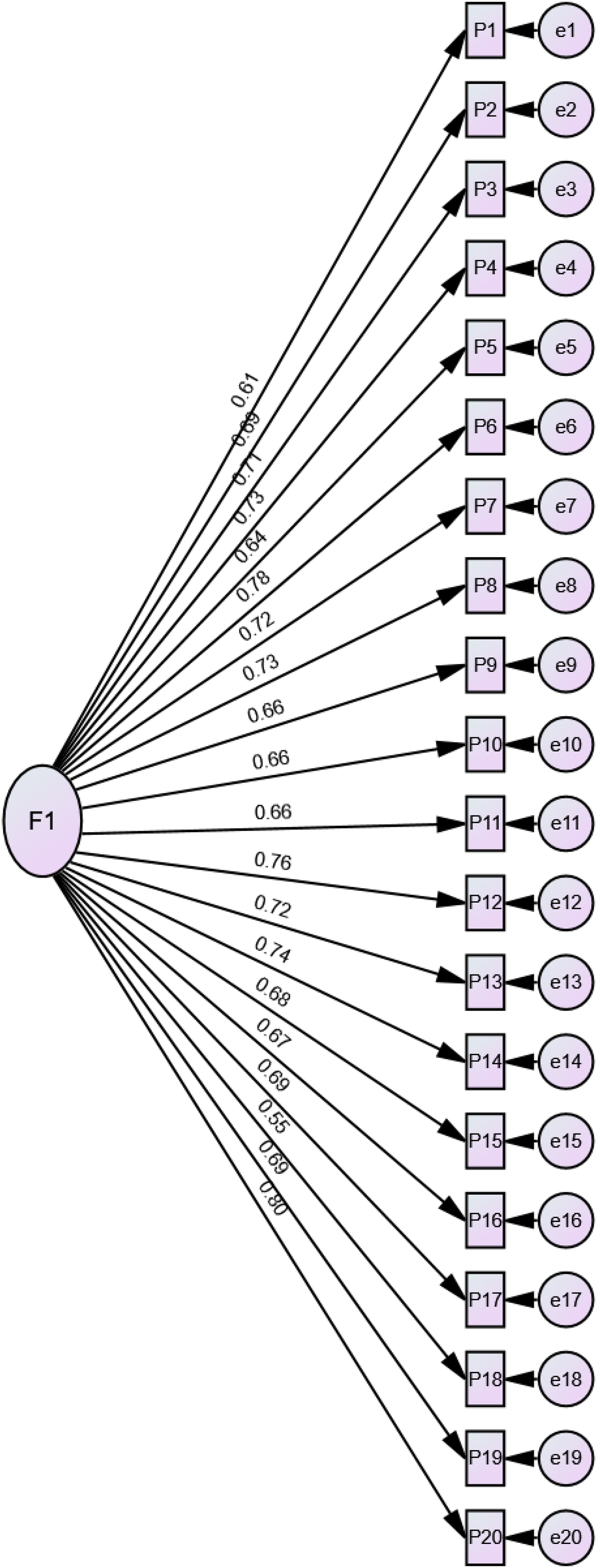
Construct validity. Standardized estimates: χ2/df = 2.267,RMSEA = 0.077,CFI = 0.912,TLI = 0.901,IFI = 0.913. Abbreviations: RMSEA, root mean square value of approximate error; CFI, comparative fit index; TLI, Tucker-Lewis index; IFI, incremental fit index.
Criterion-related validity: The results showed that the total scores of PNCQS-Chinese and PCPS were positively correlated (r = 0.77, P < 0.05), which was greater than 0.60. 40
Known-Group Validity: The findings of the study indicate that the average PNCQS-Chinese scores of nurses involved in this study were significantly different in terms of education, marital status, department, PC training experience, and job tenure (P < .05) (Table 1).
The Score of PNCQS-Chinese and Comparison with the PNCQS-Original
The mean total score of PNCQS-Chinese was 75.74 (SD:14.77). Using the independent sample t-test to compare the scores of the items of PNCQS-Chinese and PNCQS-Original showed that the average scores of each item in the PNCQS-Original were higher than PNCQS-Chinese scores (t = 2.47 to 8.19, P < .01) (Table 3). The largest gap was in question 5: “I involve family members and/or primary caregivers in patients’ care in a planned manner based on their characteristics.”
Comparison Between PCCQS-Chinese and PCCQS-Original.
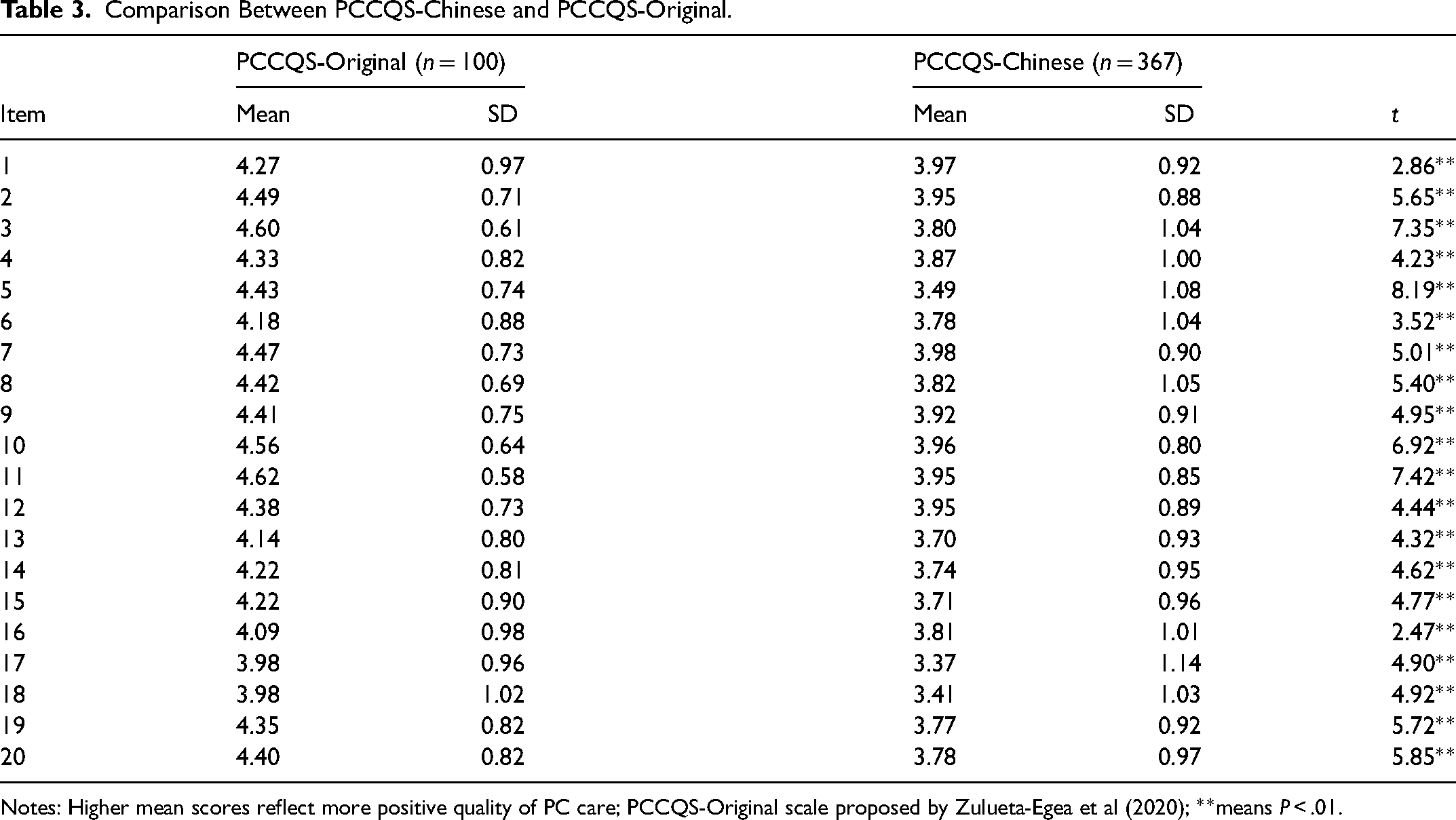
Notes: Higher mean scores reflect more positive quality of PC care; PCCQS-Original scale proposed by Zulueta-Egea et al (2020); **means P < .01.
Discussion
Based on the findings of the intercultural adaptation process guide.28,29 This study conducted a series of rigorous procedures, including positive translation, back translation, cultural debugging, and predictive testing, to develop the Chinese version of the PNCQS scale. Similar to the PNCQS-Original scale, the PNCQS-Chinese consists of 1 dimension and 20 items. The PNCQS-Chinese focus on assessing clinical nurses involved in PC nursing, and the scale effectively measures 5 aspects of PC quality: Control and relief of symptoms, family or primary caregiver, therapeutic relationship with patients and their families, spiritual support, and continuity of care. Besides, PNCQS-Chinese has adjusted slightly to enhance clarity and align with cultural norms. Therefore, the scale possesses scientific rigor and cultural appropriateness within the Chinese context.
Psychometric Properties of the PNCQS-Chinese
The results indicated that the value of CR for each item of the PNCQS-Chinese scale ranged from 12.10 to 23.34, with a statistically significant difference (P < .01). This suggests that each item on the scale demonstrates good discrimination and can assess the quality of PC nursing to some extent. Additionally, the correlation coefficients between the scores of each item and the total score ranged from 0.63 to 0.83 (all P < .01), surpassing the threshold of 0.40, indicating that all items effectively evaluate the quality of PC provided by nurses. Consequently, all the items were retained for further analysis. Reliability analysis showed that the Cronbach's α coefficient of the PNCQS-Chinese scale was 0.96, indicating substantial internal correlation and consistency among the scale items. The observed discrepancy compared to the original version (0.91) and the Turkish version (0.92) can be attributed to the characteristics of the participants, as the study population for these 2 versions encompassed a broader range of choices. Additionally, it is important to note the significant disparity in job responsibilities between nurses employed in PC professional institutions and those engaged in PC-related nursing work in general hospitals. 19 This disparity may result in greater differences in choosing questionnaire answers. Furthermore, the PNCQS-Chinese had a test-retest reliability exceeding 0.70, suggesting a notable level of stability and dependability for the scale, consistent with the Turkish national version. 27 Consequently, it can be inferred that the PNCQS-Chinese demonstrates substantial discrimination and reliability.
Regarding validity analysis, the I-CVI of PNCQS-Chinese ranged from 0.86 to 1.00, while the S-CVI/AVE was 0.98, all surpassing the minimum threshold, suggesting a substantial level of concordance between the scale's measured content and the intended content. The extracted single-factor structure from EFA accounted for the total variance, aligning with the original version's hypothesis. Furthermore, the CFA further supports the results of the EFA, as evidenced by the attainment of desirable fitting indices (χ2/df = 2.267, RMSEA = 0.077, CFI = 0.912, TLI = 0.901, and IFI = 0.913). 31 The criterion-related validity results demonstrated a strong correlation between the PNCQS-Chinese and the established valid Chinese version of PCPS, indicating a high level of validity for the PNCQS-Chinese assessment. 40 Additionally, variations in the total scores of PNCQS-Chinese across different demographic factors such as education, marital status, department, PC training experience, and job tenure further confirm the satisfactory validity of the PNCQS-Chinese test within known groups.
Quality of Palliative Nursing Care in China
Research conducted by Yin et al 42 demonstrated that translating the scale into multiple languages can facilitate the comparison of cross-cultural outcomes and help correct the gap in PC quality. This study found that the average total score of PNCQS-Chinese was 75.74 (SD:14.77), which is higher than that of the Turkish version, which was 64.74 (SD:10.66). 27 This discrepancy may be attributed to the exclusion of certain items in the Turkish version of PNCQS. Furthermore, the results of this study revealed that the scores for all items in PNCQS-Chinese were significantly lower than those in PNCQS-Original. 26 Two factors potentially contribute to these disparities. First, the distinct progression of PC may be influenced by the disparities between Chinese and Western cultures. Chinese and Western cultures exhibit a compassionate approach toward end-of-life care and emphasize the provision of humane support.43,44 However, it is imperative to acknowledge the substantial variations in the perceptions of dying, death, and the afterlife across countries and nations. 45 Besides, the psychological, social, and spiritual requirements of individuals nearing the end of their lives also exhibit significant disparities. Consequently, providing care and support in this context necessitates an approach and an appreciation for national and cultural distinctions. The second aspect pertains to the survey population, specifically the deficiency of standardized PC knowledge training and qualification certification among most nurses in China. 11 This deficiency results in disparate service capabilities among employees and nonstandardized service content. The 2015 Quality of Death Index was established through comprehensive research and interviews conducted with over 120 PC experts worldwide. 46 The rankings encompassed various factors such as hospitals and hospice environments, staffing levels and competencies, affordability of care, and quality of care. China's ranking of 71st out of 80 countries, 46 coupled with the reported challenges of sluggish PC integration and an increasingly ageing population, raises significant concerns. Given the vast size of China's population, this discovery is particularly disconcerting, prompting us to acknowledge the presence of certain obstacles in the advancement of PC within the country, this is also consistent with our research results.
In addition, we found that the higher the job tenure, the higher the quality of PC for nurses who had received PC training and worked in oncology departments, consistent with the original and Turkish versions. 27 The professional proficiency of nurses improves as they accumulate more years of experience, enabling them to address the psychological needs of patients and their families better and foster effective teamwork.19,47 Consequently, a higher PC score is achieved. The higher level of PC among oncology nurses compared to ICU nurses may be attributed to the critical condition of patients in the ICU and the influence of the visiting system. 48 ICU nurses may prioritize direct patient care by focusing on symptoms while potentially overlooking the needs of family members. 49 Zulueta-Egea et al's 26 study highlights that the PNCQS-Original assessment places greater emphasis on patient and family aspects rather than treatment-related factors, such as symptom management. Hence, it is plausible to assert that the level of person-centered care provided by nurses in the oncology department may be superior. However, it is noteworthy that in the Turkish version of the test, 27 the findings indicate a higher quality of PC among nurses in the oncology department compared to those in the PC clinic. In the future, we can conduct further investigation and comparison in China to further explore the phenomenon.
Limitation
The limitations of this study mainly include 2 aspects. First, the questionnaire was not assigned to the general population but only to specific subgroups that can mainly obtain PC quality-related resources, which is consistent with the limitations of the original scale. This is also related to the phrasing of certain items, such as “I will focus communication and coordination between all team members and the different levels of care.” Some members of the general population may also need to provide PC, but they may be individuals rather than in groups. So the PNCQS-Chinese is not suitable for measuring the quality of PC in the general population, it is specifically designed for use in hospital settings. In the future, the items can be supplemented and improved to apply to a wider range of people. Second, this study only conducted questionnaire verification for PC-related nursing workers in general hospitals, which is based on the national conditions of the mainland. However, with the development of PCs in China, this study should be further extended to professional PC staff to verify the questionnaire.
Conclusions
Nurses are significant in delivering PC to individuals with terminal illnesses, especially in departments with many end-stage patients, such as geriatrics, oncology, emergency departments, and ICUs. The caliber of PC directly impacts the well-being of patients and their families. Establishing nursing quality assessment instruments serves as the foundation for associated research. The Chinese adaptation of the PNCQS demonstrates commendable reliability and validity among Chinese nurses, meeting the psychometric standards. The advantage of the Chinese version of PNCQS lies in its reduced number of items, explicit item content, and succinct scoring method, making it a more efficient self-evaluation scale. The scale can assess the nursing quality of nurses engaging in PC-related within Chinese general hospitals. Additionally, self-evaluation can facilitate nurses’ introspection and advancement in hospice care, continuously enhancing the nursing quality provided to terminally ill patients.
Footnotes
Acknowledgements
The authors would like to thank the research institutions and leaders for their permission, and thank you to all the nursing workers who are willing to participate in this questionnaire. Additionally, we express our sincere gratitude to the original author of PNCQS, for promptly and patiently addressing our inquiries during the course of our research. Their invaluable assistance has greatly contributed to the meticulous evaluation and enhancement of the Chinese rendition of PNCQS, for which we are immensely appreciative.
Author Contributions
| Criteria | Author initials |
|---|---|
| Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; | Yubiao Gai, Qingwei Liu, Meng Zhang |
| Involved in drafting the manuscript or revising it critically for important intellectual content; | Yubiao Gai, Qingwei Liu |
| Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content; | Yubiao Gai, Qingwei Liu, Meng Zhang, Xiaojing Guo, Yuchen Zhang, Tong Qin,Ying Wang |
| Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. | Yubiao Gai, Qingwei Liu, Meng Zhang, Xiaojing Guo, Yuchen Zhang, Tong Qin, Ying Wang |
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The support for this study comes from the Medical and Health Research guidance Fund of Qingdao, China in 2022 (grant number: 2022-WJZD198).