
Abstract
Introduction
The influx of critically ill and rapidly deteriorating patients during the early COVID-19 pandemic led to an increased pressure for physicians to determine a patient's goals of care (GOC). 1 Physicians had to identify which patients would require, benefit, and want invasive measures to maximize the resources available for patient care. GOC conversations highlight the patient's values and goals. They ensure that physicians are both aware of and respectful of a patient's wishes if serious illness or death were to occur. GOC conversations sometimes incorporate, though do not always lead to, determination of code status. 2 In academic hospitals, internal medicine (IM) residents routinely have GOC conversations with patients as a component of their consultation.
Medical residents have described limited formal teaching, inexperience, and discomfort with GOC conversations.3,4 They have identified prognostic uncertainty, and lack of rapport between themselves and the patient or patient's family as barriers. 3 More senior physicians have identified prognostic uncertainty, language discordance, lack of rapport with patient and family, and reliance on a surrogate decision maker5–7 as barriers to effective GOC conversations. Proactive identification of GOC reduces the aggressiveness of care in future scenarios.8,9 Further, more comprehensive GOC discussions lead to better concordance between the prescribed and the patient's desired GOC. 10 Aiming to provide goal-concordant care is a priority for the National Academy of Medicine and can be used as a quality indicator. 11 Therefore, effective GOC conversations are essential to patient-centered care models, particularly when critical illness arises—as in the setting of COVID-19.
The COVID-19 pandemic required rapid restructuring of hospitals and wards across the world to accommodate patients with COVID-19. 12 Many acute care hospitals mandated changes in routine processes of patient care to avoid and reduce in-hospital transmission of COVID-19, including universal masking,13,14 visitor restriction policies,15,16 and extra precautions for aerosol generating medical procedures (AGMP).17–19 Training programs also had to adjust to the increasing numbers of patients while mitigating risk.20,21 At the academic hospitals affiliated with the University of Toronto where the authors practice, this involved redeploying residents to the IM clinical teaching units, establishment of COVID-19 teams, and a restructuring of resident call to separate daytime and nighttime shifts. During the first wave of the pandemic, the City of Toronto reported 250/100 000 population cases. 22 This is in comparison to New York City—the epicenter at that time—which reported 2263/100 000 population cases. 23
The rapid institutional changes and evolving medical knowledge made practicing medicine during the first wave of COVID-19 exceptionally uncertain—particularly with respect to patients’ illness trajectory, prognosis, and treatment plans. This is in contrast to later waves of COVID-19 when therapeutics,24,25 vaccine development,26–28 and variant strains 29 altered the illness trajectory of patients with COVID-19 to that with less morbidity and mortality. IM residents had to navigate this uncertainty while still early in their medical training—offering them less experience and confidence in their skillset. The experience of conducting GOC conversations from the perspectives of IM residents during a global pandemic, particularly one with significant morbidity and mortality as the first wave of the COVID-19 pandemic, is less explored. Understanding how IM residents learned and conducted GOC conversations, as well as the barriers and facilitators to GOC conversations during these constraints may more starkly elucidate areas of improvement in the educational approach to training residents to conduct GOC conversations. This qualitative study seeks to understand how the early COVID-19 pandemic impacted residents’ GOC conversations.
Methods
Setting and Participants
This study was conducted at a large, urban academic center in Toronto, Ontario, Canada. Recruitment occurred via purposive and convenience sampling. IM residents were invited by e-mail to participate in the study if they (1) cared for patients with COVID-19 during the first wave of the pandemic and (2) were active medical residents in the Core Internal Medicine Program at the University of Toronto during the 2019-2020 academic year. Three rounds of emails were sent for recruitment, and individuals who met the inclusion criteria were asked to participate. In Canada, residents are classified by their post-graduate year (PGY) level, that is, a resident in PGY1 would be in their first year of residency. Participation in the research study was completely voluntary.
Data Collection
A semi-structured interview guide (Appendix 1) was established based on existing literature and reflexivity 30 of the 2 authors. Interviews were completed with the primary author (AL) via the online platform Zoom and memos were recorded after each interview. Interviews were then transcribed verbatim using the online transcription software company ‘Rev’ (www.rev.com). Automated transcripts were proofread by the primary author (AL) to ensure accuracy. The study was conducted using a constructivist grounded theory (CGT) approach,31,32 with data collection and analysis occurring concurrently and iteratively. CGT was chosen due to its flexibility and inductive approach to the data collected. CGT allows for the construction of a theory in an area where another theory does not exist, which the authors felt was appropriate as this scale of a global pandemic had not previously been encountered by IM residents.31,32
Data Analysis
Both authors (AL and NA) independently proceeded with line-by-line open coding of the transcripts to identify codes, which were subsequently grouped into themes. Analysis occurred simultaneously with data-collection, using an iterative, constant comparison approach. The authors met regularly to review codes and themes. The interview guide was iteratively modified throughout the research process to address identified themes. Four questions were added to the original interview guide to further explore new themes that emerged with participants. These include questions 5, 8, 9, and 12 (Appendix 1). Interviews were conducted until no new themes were identified. All participants received and signed an approved consent form prior to participating in the study. Participants received a $15 Amazon Gift Card for their participation.
Ethical Considerations
This study was reviewed and approved by the University of Toronto Research Board (REB Protocol #39743). At the time of the study, AL was a General Internal Medicine subspecialty resident at the University of Toronto. NA was a general internist, clinician educator, and site program director for the core internal medicine training program at the University of Toronto.
Results
Eleven residents participated in the interviews (Table 1). Residents were consistently able to distinguish between code status and GOC, defining the former as the “terms of particular components of resuscitation such as CPR, intubation, or advanced level of care like ICU level of care, vasopressors,” (P6) and the latter as “about philosophy of care, values, what type of person someone is and what they see themselves doing after this diagnosis” (P10). We identified 3 overarching components of the residents’ experience including: self-described process of conducting GOC conversations, education around GOC conversations, and conduction of GOC conversations during the COVID-19 pandemic.
Demographics of the Participants Between October and December 2022.
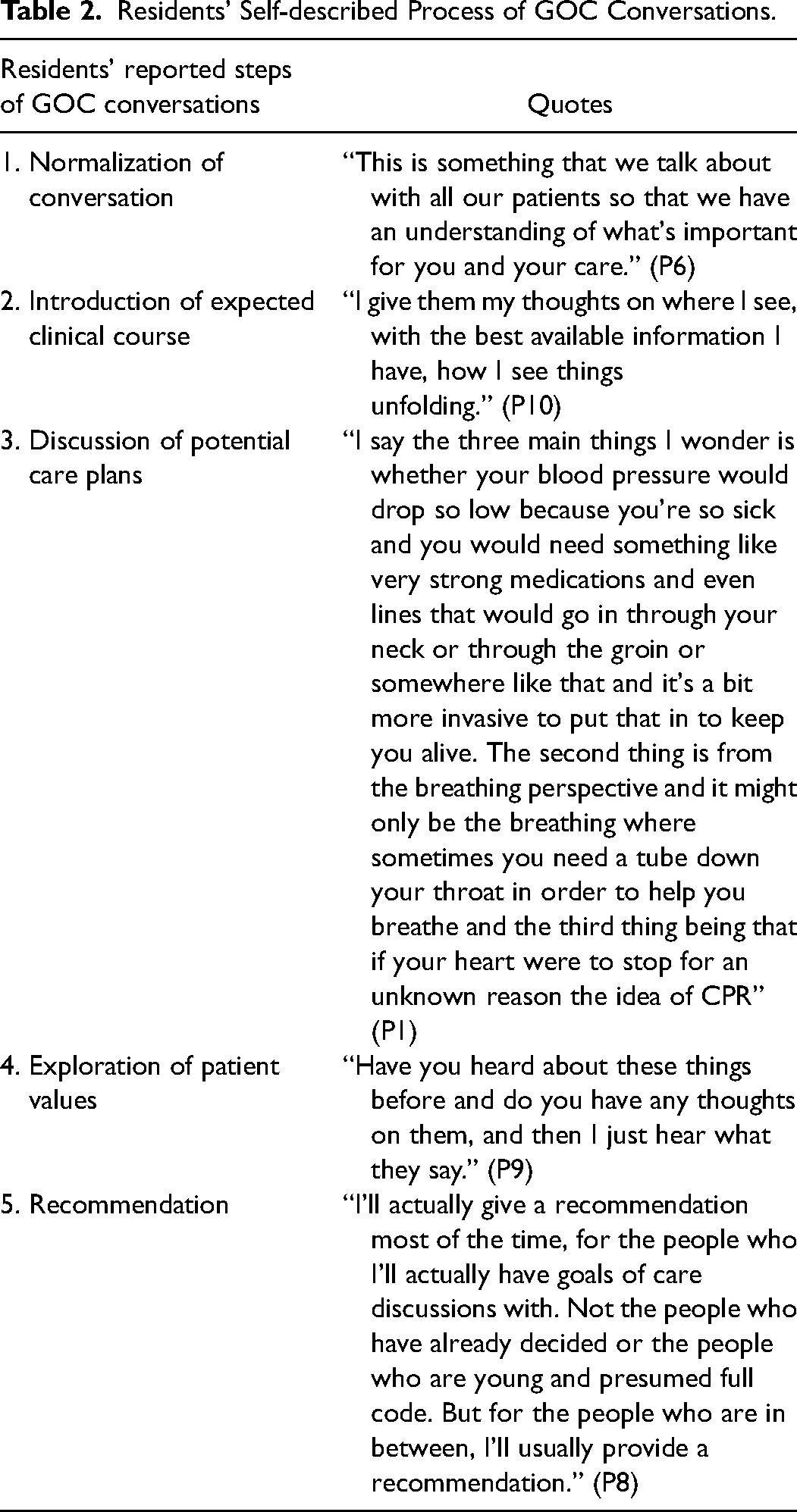
Process of Conducting GOC Conversations
Residents described their GOC conversation in 5 steps (Table 2) with few aligning their conversations with an evidence-based framework. Some residents, but not all, provided recommendations to patients during their GOC conversations. Those who provided recommendations often assumed this strategy following a palliative care or critical care rotation where they saw the technique role-modelled by senior physicians. Most GOC conversations eventually merged into a decision about code status.
Residents’ Self-described Process of GOC Conversations.
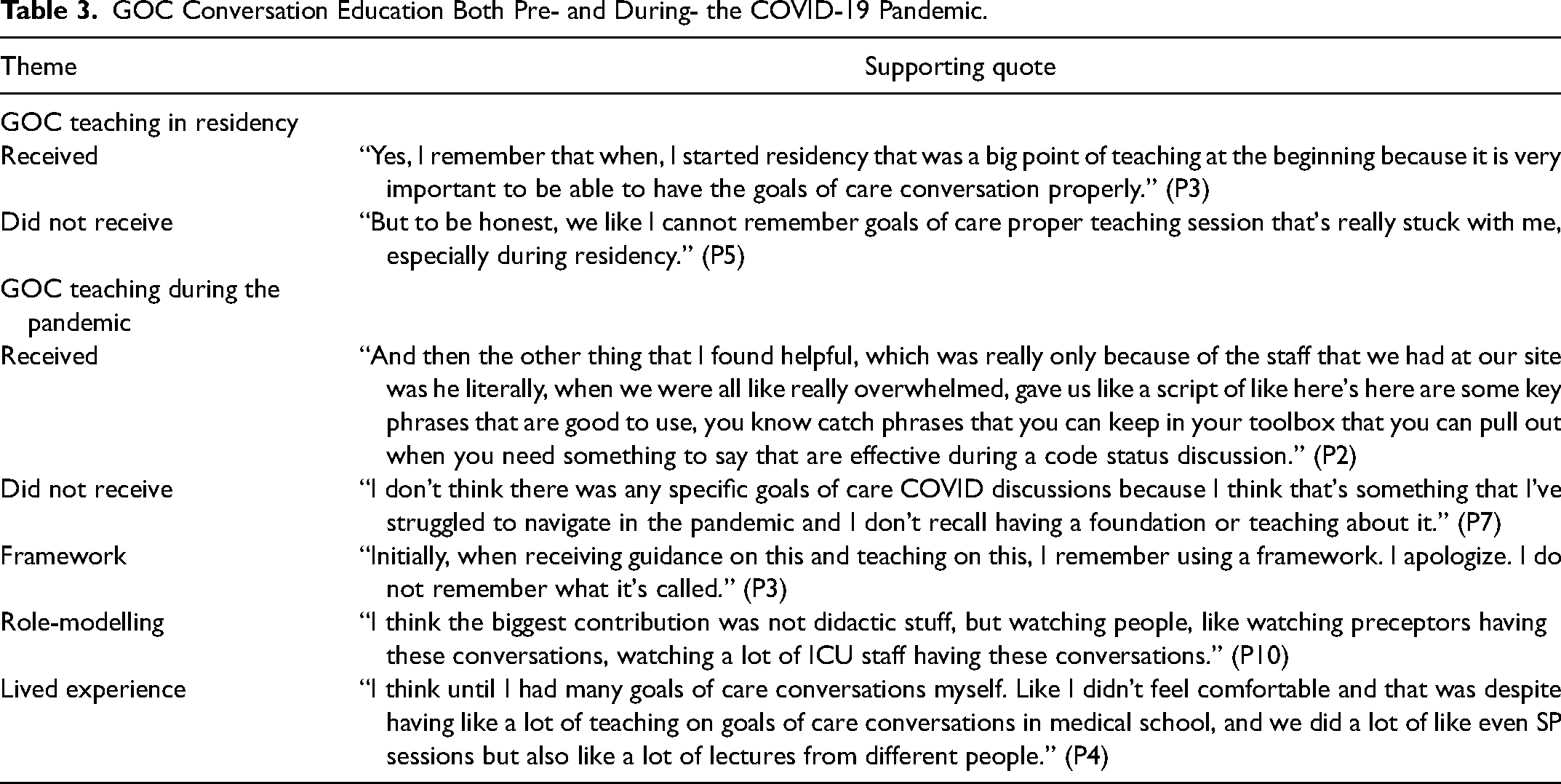
GOC Teaching
Residents reported limited didactic teaching with respect to GOC conversations (Table 3). The education reportedly received by residents were mixed, with some reporting no teaching at all during their residency to some reporting pandemic-specific teaching where they received both written and/or verbal instruction as well as a “script” to guide GOC conversations. They reported relying heavily on role-modelling from more senior physicians to enhance their own GOC conversations. Residents reported honing their GOC conversations via self-practice and a “trial and error” approach.
GOC Conversation Education Both Pre- and During- the COVID-19 Pandemic.
GOC Conversations During the COVID-19 Pandemic
Residents described several barriers to their GOC conversations during the COVID-19 pandemic (Table 4). They emphasized the urgency to have GOC conversations, most often at the time of admission, rather than deferring GOC conversations for stable patients. Residents described the potential for rapid deterioration in patients with COVID-19 as the main reason for more urgent GOC conversations.
Identified Themes and Supporting Quotes on How COVID-19 Affected Resident's GOC Conversations.
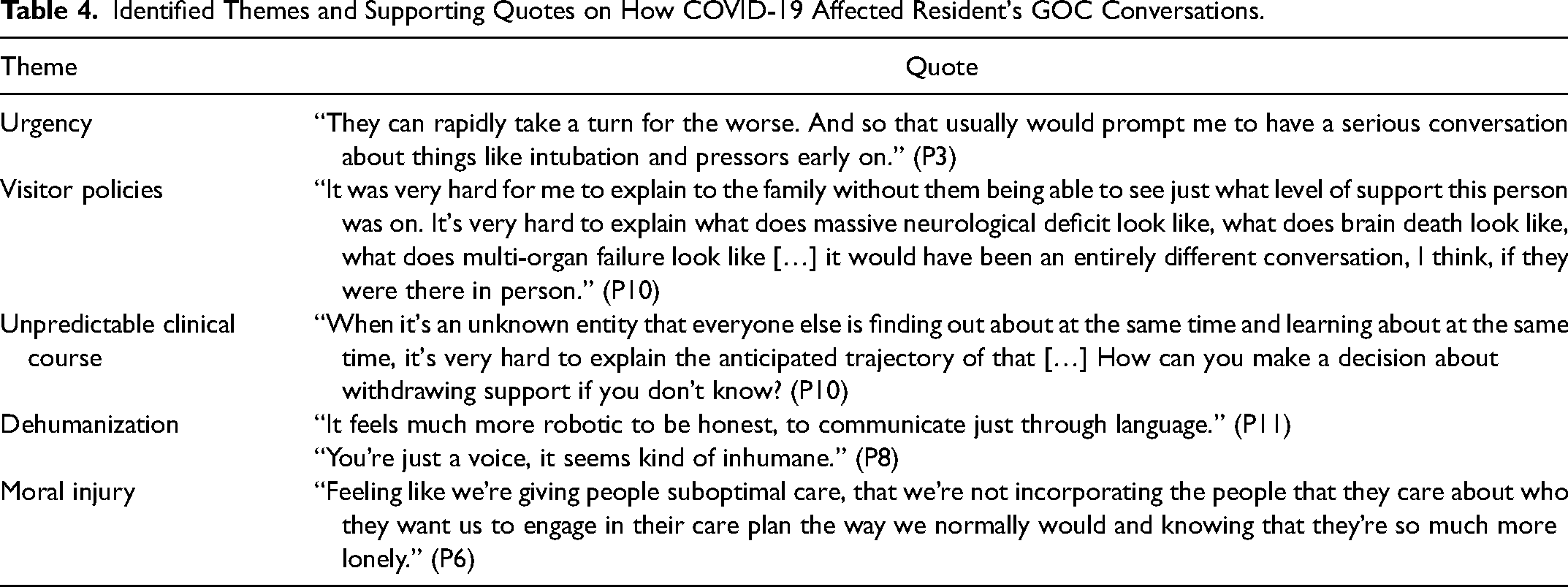
Residents adapted steps 2, 3, and 4 (Table 2) of their conversation specifically to the COVID pandemic. Introduction of clinical course (step 2) required expression around the limited knowledge of COVID-19. Discussion of potential care plans (step 3) and exploration of patient values (step 4) was challenged by restrictive visitor policies. Many GOC conversations were had via telephone due to the visitor restrictions. Residents found that verbal descriptions alone were insufficient in describing both the severity of illness as well as invasiveness of potential interventions. Residents also found it challenging to establish a therapeutic rapport with patients’ loved ones over the phone given the lack of non-verbal cues.
Residents described a sense of dehumanization and feeling as if they were “just a voice” (P8) to patients’ loved ones when discussing GOC. The inability to effectively communicate with patients’ support systems limited residents’ ability to adjust a patient's code status despite worsening clinical status. For some residents, it was unclear that the current invasive therapeutics were within the patient's GOC, and/or that the patient would be accepting of the unintended consequences or long-term sequelae of more invasive measures. Residents therefore expressed uncertainty about whether they were providing goal-concordant care. Because of this, residents described a sense of moral distress.
Discussion
Our study brings to light an important tension: even though residents regularly conduct GOC conversations, they often feel ill prepared to do so with resulting consequences both for patient care and for the residents themselves. This tension is uniquely highlighted in this study completed during the early COVID-19 pandemic where uncertainty was pervasive. Lack of experience with a poorly understood contagion with a high level of morbidity and mortality at the time in addition to the variable clinical presentation, absent therapeutic interventions, and unpredictable illness trajectory heightened the need for skill in GOC conversations. Despite the uncertainty, residents adapted their GOC conversations to both the novel illness and systemic barriers with limited formal instruction in attempts to provide goal-concordant and patient-centered care.
One unique finding in our study is the suggestion that moral distress experienced by trainees providing end-of-life care may begin with GOC conversations. Resident moral distress related to end-of-life care has previously focused on the provision of care or treatments at the end of life that were felt to be either futile or harmful for the patient.33,34 The COVID-19 pandemic may have contributed to this finding as residents worried that their conversations with patients and their loved ones were limited by medical knowledge about COVID-19 and communication barriers resulting from the institution of restrictive visitor policies. 34 Residents described a sense of dehumanization and difficulty developing rapport with patients’ loved ones when having GOC conversations conducted virtually. Admitted patients were often left to have high-stakes conversations and make critical decisions without the support of their loved ones at bedside. This led to the concern that patients and their loved ones had limited ability to understand the extent of illness, resulting in the delivery of potentially goal-discordant care.
Our study also identified barriers that should be considered in education paradigms beyond the COVID-19 pandemic. Prognostic uncertainty and limited ability to advise potential care plans are known barriers, particularly for more junior residents. The ability to understand and predict illness course is limited during the earlier years of training. Further, despite more permissive visitor policies later in the pandemic, many GOC conversations may still be completed over the phone for a variety of reasons—consider distance or mobility issues of the substitute decision maker. Conversations conducted over the phone or via video conference are unique in that individuals lose non-verbal cues on both sides of the conversation. 1 Communication guides 35 have suggested verbally acknowledging emotion to convey compassion as a core skill in conducting GOC conversations over the phone. 36 Lastly, the ability to have effective conversations in a time of clinical urgency is important in the setting of any rapidly deteriorating patient.
A Conceptual Model to Teach GOC Conversations
Given our findings, it is imperative that trainees are provided with a strong educational foundation to navigate challenging GOC conversations. When exceptional circumstances arise, it is important that they can root their actions in the fundamentals. We propose a conceptual model (Figure 1) to ground GOC education based on our study: formal teaching of a validated GOC framework,37–39 positive doctor role modelling by a senior physician, and experiential learning.
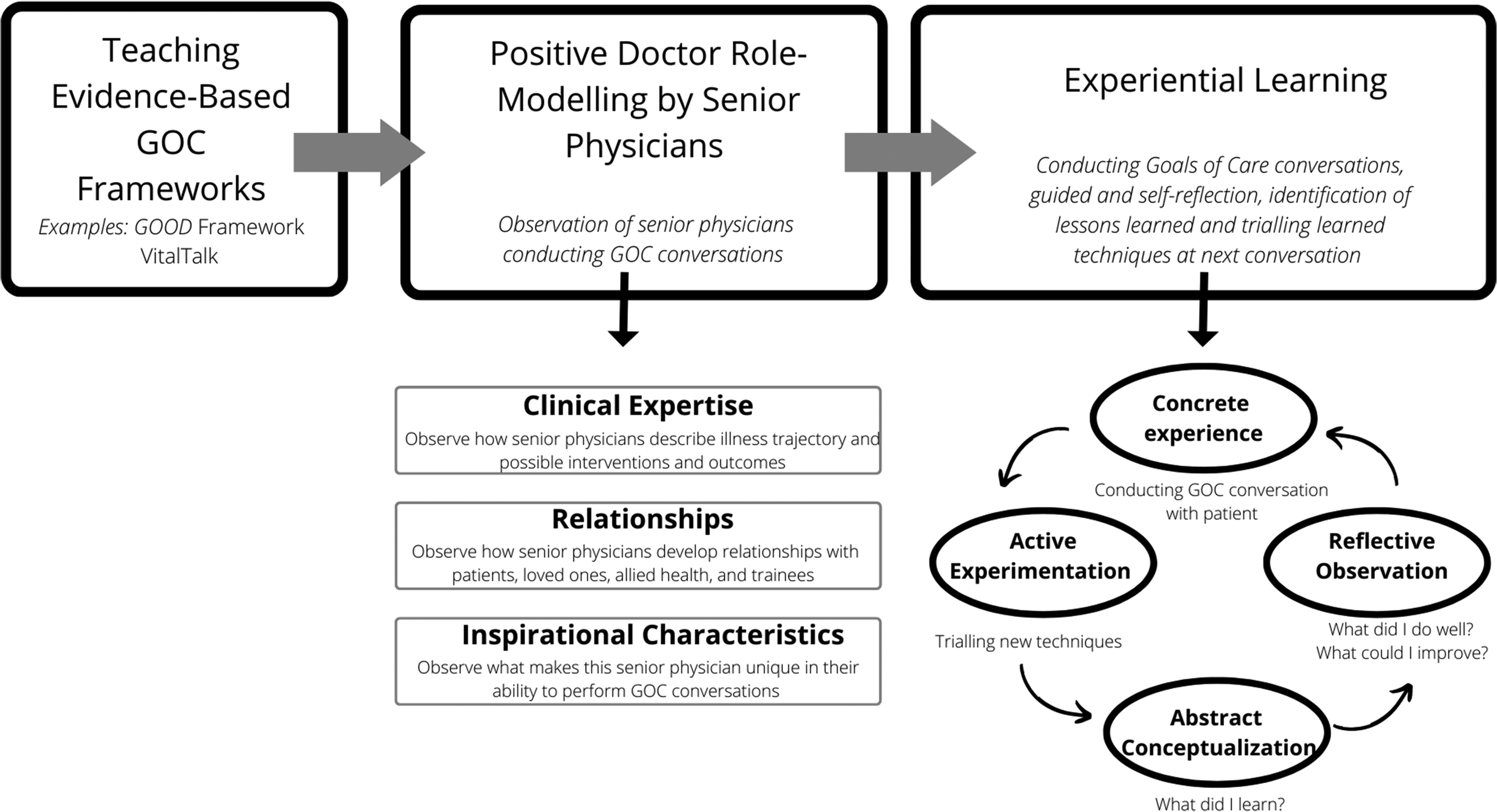
A conceptual model for teaching GOC conversations.
In this study, most residents reported that they did not use a formal framework for GOC conversations. Residents nonetheless described a consistent process of completing GOC conversations. The authors felt that this implied a framework that is “passed down” via informal teaching or an implicit reliance on a framework that may have been taught earlier in their medical training. Nonetheless, several serious-illness conversation guides such as VitalTalk, 39 REMAP, 38 and GOOD 37 exist, and should be incorporated into residency training at an early stage. Just as residents are taught guidelines and evidence-based frameworks for the treatment of other conditions (ie, sepsis, GI bleed), they should also be taught evidence-based approaches to GOC conversations. Such frameworks can provide a foundation for residents to build upon when approaching GOC conversations.
Residents in our study also described relying heavily on positive doctor role-modelling and experiential learning to hone and develop comfort completing GOC conversations. The hidden process of positive doctor role modelling described by Passi and Johnson40,41 notes an “exposure phase” whereby trainees observe professional attitudes by more senior physicians. They outline how trainees observe and subsequently integrate clinical decision making, professional attitudes, and relationship-building techniques into their desired practice. Prior studies have demonstrated how residents who have completed a critical care rotation or palliative care rotation42,43 noted observing senior physicians complete GOC conversations and subsequently felt more confident in their own abilities. Further, residents who had seen recommendations role-modelled by more senior physicians were more likely to provide a recommendation which is welcomed by family members and patients as part of the shared decision-making process. 43 Positive doctor role-modelling of GOC conversations by senior physicians with observation by residents, particularly early in their training, may increase the comfort and skill of residents as they navigate potentially challenging conversations.
Lastly, residents can then build upon a validated framework and techniques learned via positive doctor role-modelling through experiential learning to hone their skills with GOC conversations. Experiential learning as described by Kolb 44 identifies a cycle with 4 main components: concrete experience (GOC conversation with patient), reflective observation (consider the efficacy of the conversation), abstract conceptualization (what could be better?), and active experimentation (try new techniques to improve conversation). Kolb's theory of experiential learning allows residents to continuously practice and enhance a single skill, in this case, GOC conversations, in different contexts and adapt and improve their performance in the skill. We argue that this is the final step for residents to become comfortable and apt at conducting effective GOC conversations.
Limitations
Limitations of this study include a single urban, academic center and only IM residents, many of whom were more junior in their training and may not have received focused palliative care or critical care training yet. Further, the residents who participated in this research study primarily discussed their experiences with the first wave of COVID-19 and their experiences may have evolved as our understanding of COVID-19 has improved, potentially impacting recall of their early experience.
Our study was also limited by low resident participation. Participants primarily consisted of PGY2s and 4s, with no PGY3s. PGY1s at the time of the study were ineligible to participate given that they would not have been in residency during the first wave of the COVID-19 pandemic. The lack of PGY3 participants means that we did not examine the experiences of those at the intermediate level of IM residency training. Nonetheless, thematic saturation was reached by 11 participants, speaking to the universality of themes even by those at the beginning and nearing the end of their IM training. By the time the initial interviews were completed, we had already entered the third wave of the pandemic, at which point illness understanding and potential treatments for COVID-19 were emerging. Further interviews at this time were felt to represent a radically different experience from the uncertainty of the first wave and thus were not pursued.
Recruitment from other Canadian sites was not sought, as the experience in Toronto differed vastly from that across the province due to larger case counts, hospital admissions, and resulting systems and residency program restructuring. At this academic center, COVID-19 patients were abundant but did not overwhelm the healthcare system nor did the volumes significantly limit care due to resource constraints. The experiences of residents in more resource-limited locations outside of Toronto and/or higher volume of patients with COVID-19 may have added additional themes that were not identified in our research study.
Conclusion
This study uses the experience of IM residents to describe how GOC conversations were affected by the early waves of the COVID-19 pandemic. We found that uncertainty around illness prognosis, restrictive visitor policies, and insufficient education around GOC conversations impacted the residents’ ability to have effective GOC conversations which may have caused feelings of moral distress in some residents. We thus present a conceptual model to ground GOC conversation education. Further research should evaluate the implementation and outcomes of our conceptual model in practice. This should include both education surrounding conversations conducted in person as well as virtually (via phone or video conference). Another area of interest may research how GOC conversations beyond the COVID-19 pandemic may contribute to resident moral distress.
Footnotes
Prior Presentations
University of Toronto, GIM Research Day 2021—May 28, 2021. International Conference for Residency Education 2021—October 21, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HoPingKong Centre for Excellence in Education and Practice, University Health Network for sponsoring the authors and this study. Nadine Abdullah is supported by an award from the Mak Pak Chiu and Mak-Soo Lai Hing Chair in General Internal Medicine, University of Toronto.
Appendix 1: Interview Guide
Please read the following to the participant:
Thank you for agreeing to take part in this study. I will be asking you several questions. In order to protect your privacy and the privacy of others, please do not mention any names or any personal information that can identify you or patient during the interview.
Please state your year of training and residency program.
Demographics: age, gender.
Please describe your clinical experience with COVID-19 during your residency. How did your clinical rotations change with the COVID-19 pandemic? Were you involved in admitting patients or completing the initial consultation for patients with suspected or confirmed COVID-19? What changes were made to your hospital during the COVID-19 pandemic?
Examples include AGMP, visitor policies, PPE etc. In your opinion, can you please describe the difference between code status and goals of care conversations?
Which conversations are you more commonly having? Did you receive any teaching about having goals of care conversations during the pandemic?
If so, what did this teaching in entail? Please describe your process in having goals of care conversations. Do you have a framework that you use? Do you provide recommendations for GOC? Have any of the changes made during COVID-19 affected your goals of care conversations? Were there any factors that influenced how urgently you had GOC conversations? Have you ever experienced moral distress that related to a patient's GOC?