
Abstract
Introduction
According to the United States (US) Census Bureau's 2017 National Population Projections, by 2030 the last of the baby boomer generation will be older than 65; turning 65 at a rate of 10 000 individuals each day. By 2030, this will represent twenty percent of the US population. 1 The United States is headed toward an end-of-life-care crisis. The number of patients with some combination of aging, frailty, dependence, and multiple chronic conditions continues to rise, resulting in increasing pressure on the US health system. 2
Palliative care teams improve medical-psycho-social issues in individuals with serious life-threatening diseases. There is clear evidence of the improved quality of life,3,4 decreased hospital lengths of stay,5–8 and reduced healthcare costs.3,5–8 End-of-life discussions held before the last 30 days of life are associated with less aggressive care and greater use of hospice. 9 Patients do feel that the emergency department (ED) is an appropriate place to have goals-of-care (GOC) discussions. 10 Additionally, this is a skill that can be taught. 11
There is an opportunity to incorporate these elements of palliative care by approaching the patient and documenting GOC while the patient is present in the ED.
Most patients want to die at home; however while 70% of patients report that they wish this, only 30% do.12,13 Goals of care documentation (Physician Orders for Life-Sustaining Treatment (POLST)/GOC note/advanced directive) may be hard to find in the medical record,14–18 and completion rates of advanced directives of elderly adults are low. 19 When the forms are not present, the default is full code/full treatment resulting in unwanted care near the end of life.
In 2016, Academic Emergency Medicine published a white paper on the research needs of shared decision making, palliative care, and end-of-life care in the ED.20–22 They identified key research questions including Which ED patients are likely to benefit from a GOC conversation and how can they be rapidly identified? What are the most effective interventions to promote in the ED, such as physician and nurse palliative education? What outcome measures should be evaluated to assess the integration of palliative care within the ED? 22 This research paper addresses some of these questions.
Barriers to GOC conversation in the ED include lack of physician time,23,24 lack of training, concerns about legal ramifications, feelings that a GOC discussion should only be held by the primary care physician, and discomfort having the conversation.23–27 By having specially trained staff in the ED to conduct and document GOC conversations, we hypothesize that it would remove barriers to GOC discussions emergency physicians face. At the time of study design, no similar research had been identified in review of the literature.
We hypothesized that embedding an ED RN in the ED who is trained in GOC conversations would:
Increase GOC documentation. Decrease overall ED/hospital/intensive care usage. Increase the length of time on both palliative care and hospice services. Be well received by patients/healthcare surrogates, as shown by high patient satisfaction scores.
Methods
Study Design and Setting
This retrospective and prospective, observational convenience sample pilot study was conducted over a six-month period, February 2016 to August 2016, in a single urban community ED with an annual patient volume of roughly 95 000. The study was unblinded. Patients acted as their own controls, comparing various hospital use metrics in the 12-month preindex visit to the 12-month postindex visit.
Sample Selection
Emergency Department Goals-of-Care Registered Nurses (ED GOC RNs)
For this study, 4 current ED RNs were selected to work additional shifts as ED GOC RNs. The ED GOC RN position was posted on the internal digital job board and interested ED RNs applied. ED RN selection criteria included a minimum of 3 years of EDRN experience, current employment within the ED, and passing a selection interview. They functioned as extra staff within the ED whose focus was only on having GOC discussions.
Once selected, the ED GOC RNs received 7 h of training which covered: how to conduct a GOC conversation, discussion of how to complete a POLST form, how to document the GOC conversation within the electronic medical record (EMR) in Epic, and how to identify appropriate study candidates. Additionally, trainees met with local palliative and hospice agency representatives.
Patients
Enrollment in the study was limited to patients aged 18 years and greater AND English speaking AND not pregnant AND having at least one of the 4 medical conditions:
Congestive heart failure with an ejection fraction of 40% or less. Metastatic cancer. Chronic Obstructive Pulmonary Disease on home oxygen. Chronic kidney disease stage III or greater.
Procedures
ED GOC RN
An ED GOC RN was physically available in the ED from 9:00 AM to 5:30 PM, Monday through Friday. The ED GOC RN would review the ED tracking board to identify patients who met the inclusion criteria. This typically included a brief chart review to go over a patient's medical history. The ED GOC RN then contacted the patient's primary ED RN to see if the patient had had his/her workup initiated (ie, bloodwork draw, an intravenous catheter placed) and was awaiting results. It was important that the ED GOC RN not impede the patient's workup. If the patient was awaiting results, the patient or surrogate was then approached for possible study inclusion (Figure 1). Once enrolled, a standardized questionnaire was used (Figure 2). The questions chosen had been validated in numerous other studies and are used widely throughout the palliative care community.11,28
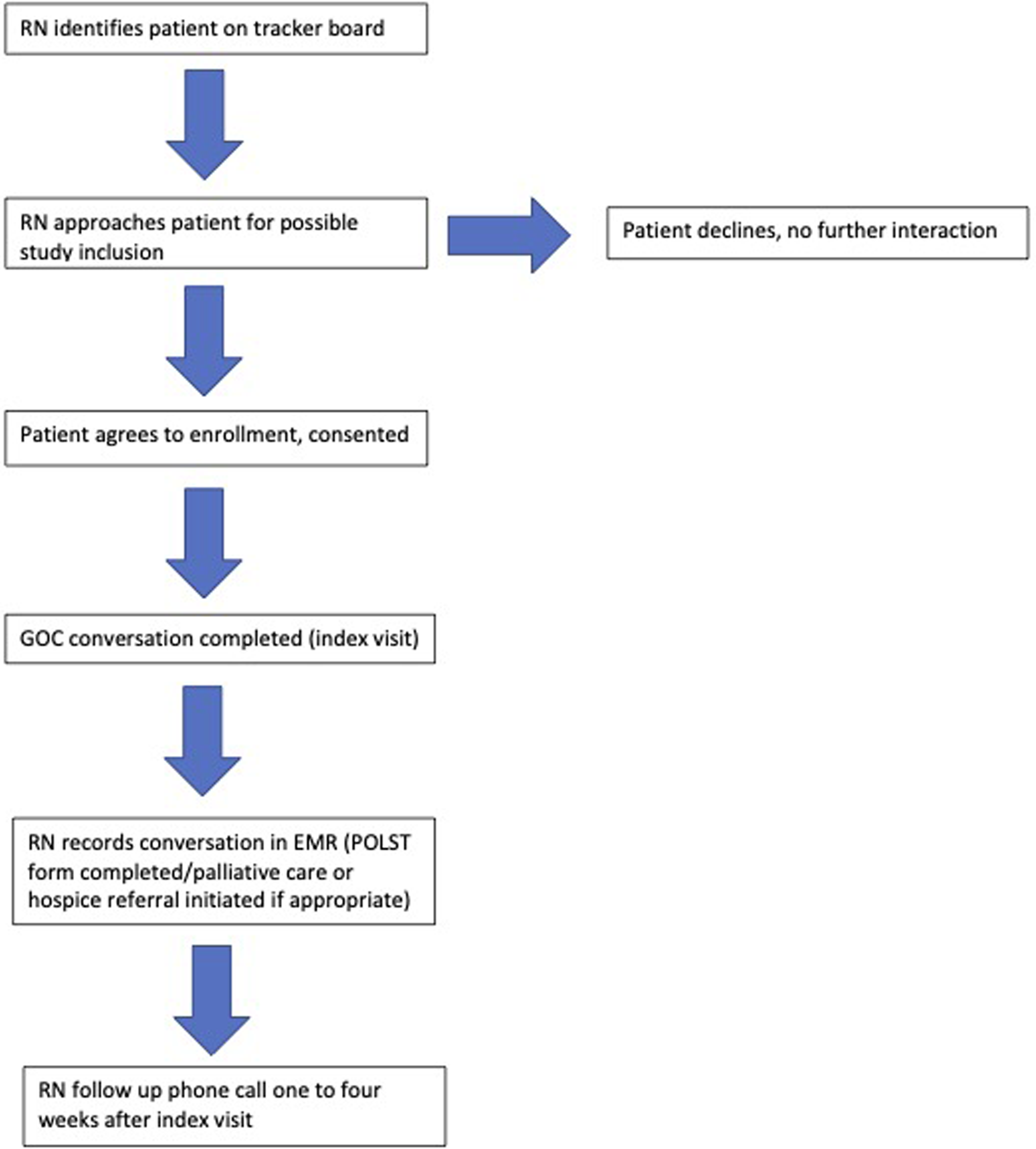
Study participant flowchart.
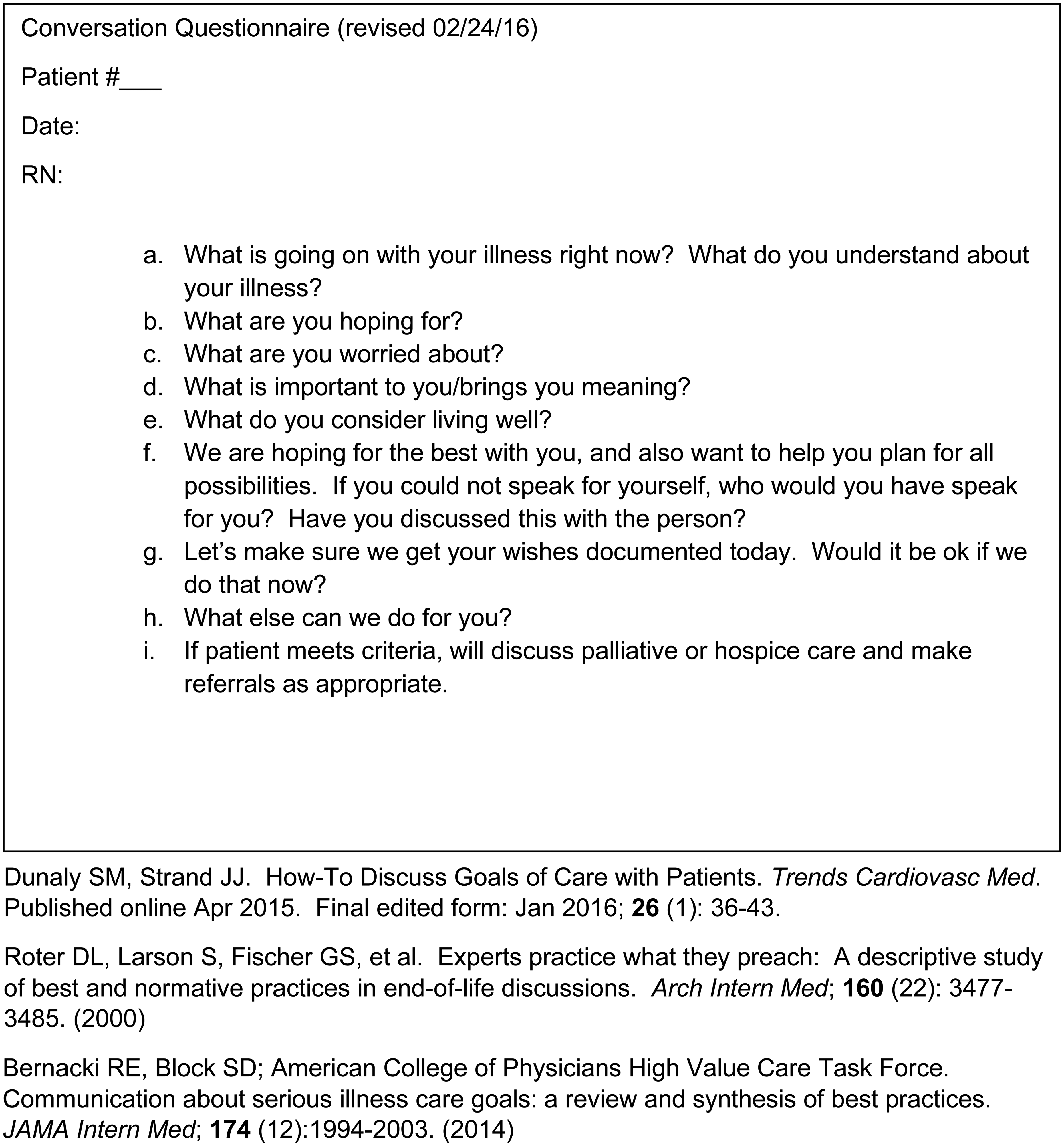
Goals of care question template.
This discussion was documented in the patient chart under the note title of “Goals of Care” to facilitate easy searching by other medical practitioners. If appropriate, a POLST form was filled out with the patient, confirmed, and signed by either the ED physician or given to the patient to be taken back to the primary care physician to review and sign. When possible, the conversation was held in the presence of the patient's family members.
A follow-up phone call was made to the patient between 1 and 4 weeks after the conversation to assess satisfaction with having the GOC conversation in the ED (Figure 3). It was not known at the time of the phone call if the patient was alive or dead. A maximum of 3 separate attempts were made to reach the patient or surrogate.

Patient follow-up phone call satisfaction questionnaire.
Data Analysis
Once a patient was enrolled, the goals of the care conversation were documented in his/her chart. Patient/surrogate satisfaction with the conversation was assessed via phone call and was gauged on a five-point Likert scale: 1 = Strongly disagree; 2 = Disagree; 3 = Neither agree nor disagree; 4 = Agree; 5 = Strongly agree (Figure 3).
The ED visit during which the patient was enrolled along with the ensuing hospitalization was considered the index visit. The index visit was the measurement for the 12-month prior and post periods. The data were captured from the EPIC electronic medical record system.
Patients were enrolled from February to July 2016. A retrospective chart review was completed for the 12 months preceding the index visit, looking at several metrics. These same metrics were monitored for the 12 months following the index visit. These metrics were:
Number of ED visits Length of index ED visit Number of hospitalizations Duration of hospitalizations Number of intensive care unit admissions Duration of ICU stay Time on palliative care service Time on hospice service Patient/surrogate satisfaction with having a GOC conversation in the ED POLST form completion status Duration of GOC conversations
Statistical Analysis
Data was abstracted from the electronic medical record, Epic (Verona, Wisconsin), by a data analytics specialist, using Tableau (Seattle, Washington). Data abstracted was confirmed with a randomized manual chart review by 2 separate people. Acquisition of palliative and hospice enrollment data was attempted by manual chart review of every enrolled patient by the primary investigator (PI). The PI identified the index visit and then looked through the following 12 months of the patient's record to identify if and when a patient was enrolled in either service.
Continuous data were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR). Categorical data were presented as proportions. The number and the length of stay of ED visit/hospitalization/ICU admissions in pre- and postperiod were compared by the paired Wilcoxon signed rank test with continuity correction. Patients who died during the index ED/hospital stay were excluded from the study analysis beyond the initial rate of GOC documentation in the EMR and POLST completion in the ED on the index visit.
Based on the survival time after the index visit, 4 analysis cohorts were generated: (A) all enrolled patients; (B) patients who survived 1 week past the index visit; (C) patients who survived 1-month postindex visit; (D) patients who survived 12 months postindex visit (to the study's end). Patient demographics were reported for cohorts B and D. Duration of GOC conversations, and completion of POLST forms were reported for cohort A. Patient satisfaction ratings of ED GOC conversations were reported for cohorts C and D. Emergency Department/hospital/ICU usage was analyzed for cohort D.
Statistical analysis was conducted using R3.5.1 software (R Foundation for Statistical Computing, Vienna, Austria). Significance was set at P < .05.
Results
Characteristics of Study Subjects
A total of 133 patients were approached for study inclusion. Thirty-eight declined participation. Of the 95 enrolled patients, one withdrew after 1 month, and 10 died during the index ED visit/hospitalization (day of conversation). Of the 84 patients surviving 1 week past the index visit (both admitted and discharged), 12 (14.3%) died within 1 month, and 38 (45.2%) died within 1 year, thus not completing the 12-month postindex visit monitoring period. Data analysis was limited to the 46 patients who survived the entire 12-month postindex visit period (Figure 4).
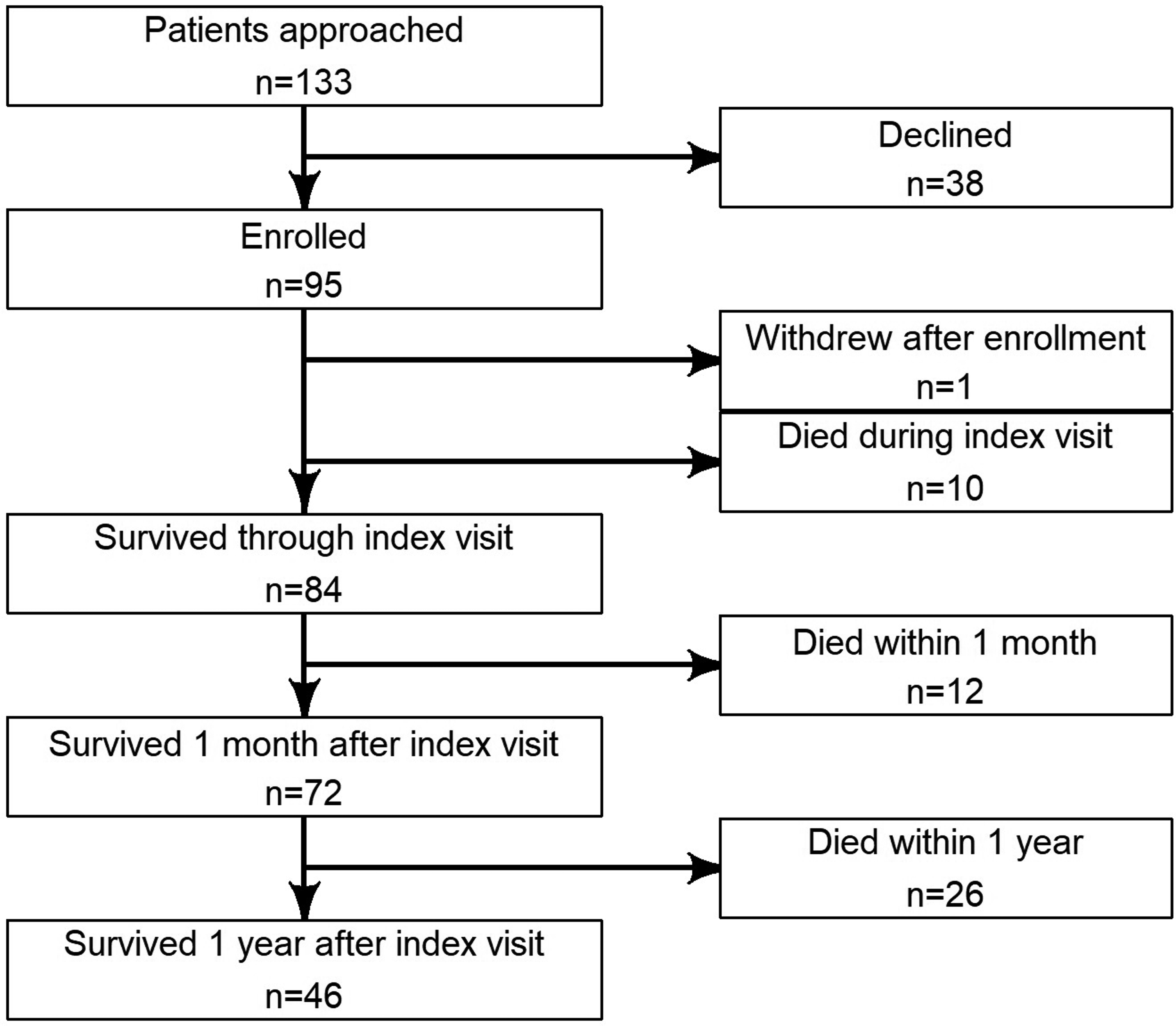
Patient enrollment flowchart.
Demographics for the survival to study's end group were: mean age of 72 years, ± 11 years; 46% female; 94% Caucasian (The study hospital is sited in a predominantly Caucasian area.). The majority of patients were on Medicare or a combination of Medicare plus secondary insurance (92%). The breakdown of the 4 inclusion criteria groups is as follows: 30% COPD, 20% CHF, 46% CKD stage III or greater, and 4% cancer (Table 1).
Patient Demographics.
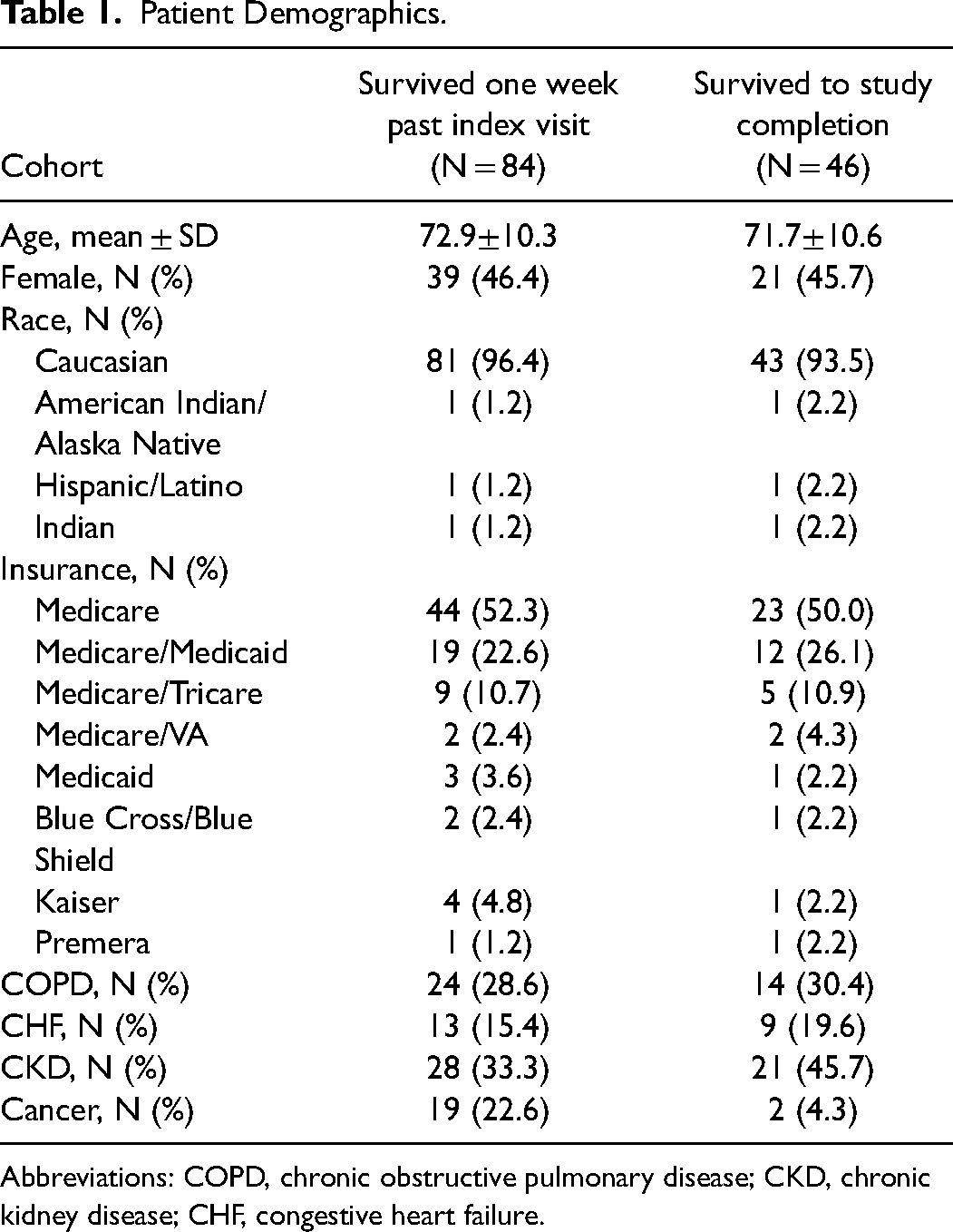
Abbreviations: COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; CHF, congestive heart failure.
Patients with cancer had the highest mortality rate of those enrolled in the study. Of the patients who survived the week following the index visit, 23% carried a cancer diagnosis, but only 2/19 survived to the end of the study as compared to 14/24 for COPD, 9/13 for CHF, and 21/28 for CKD (Table 1).
GOC Conversations
The total number of GOC conversations held was 94. All of these patients had their wishes recorded in their EMRs. Using the corrected population of 84 patients (those surviving the week following the index visit), the mean ED conversation time was 48.9 min. The length of GOC conversation time varied widely, from 17 to 90 min, primarily due to patients’ interest in discussing their goals of care. Some patients had prior experience discussing their GOC and therefore had shorter conversations. Most conversations were 1 h or less in length: 15 to 30 min for 35 conversations (41.7%), 31 to 60 min for 30 conversations (35.7%), and 61 to 90 min for 19 conversations (22.6%).
Physician's Orders for Life-Sustaining Treatment (POLST) Completion
In the all-enrolled group, 35 had preindex visit POLST forms completed, 35 completed the form during the index visit, 4 updated their current form, and 24 declined form completion.
Of those surviving the week following the index visit, 29 had a POLST form completed before their index visit, 34 patients filled one out in the ED with the ED GOC RN, 3 patients updated their current POLST, and 21 patients declined to complete a POLST.
Limiting POLST completion data to those who survived to the study's end, 12 had a preindex visit completed POLST form, 20 patients completed a POLST form on the index visit, 1 updated the current POLST form, and 14 declined ED POLST completion (Table 2).
Physician Orders for Life-Sustaining Treatment (POLST) Form Completion Status.
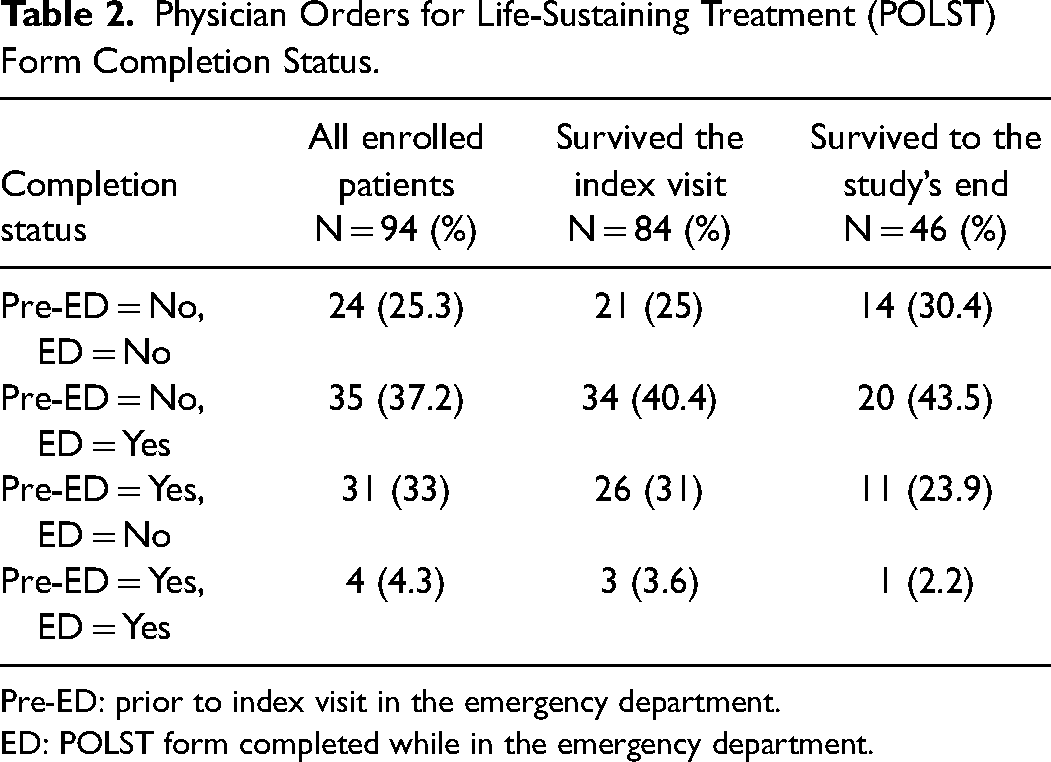
Pre-ED: prior to index visit in the emergency department.
ED: POLST form completed while in the emergency department.
Patient Satisfaction With ED GOC Conversation
We reached 50% of the study population with the follow-up phone call. Patients were asked to rate their experience with the ED-based conversation from 1 to 5, with 5 as very satisfied with having the GOC conversation in the ED.
Among those surviving the week following the index visit, 44 were contacted (52%). 39/44 (88.9%) rated the experience 5/5, 2/44 (5%) rated the experience 4/5, and 3/44 patients (7%) could not recall the ED GOC conversation (Table 3).
Patient Satisfaction Rating With Emergency Department Goals of Care Conversation.
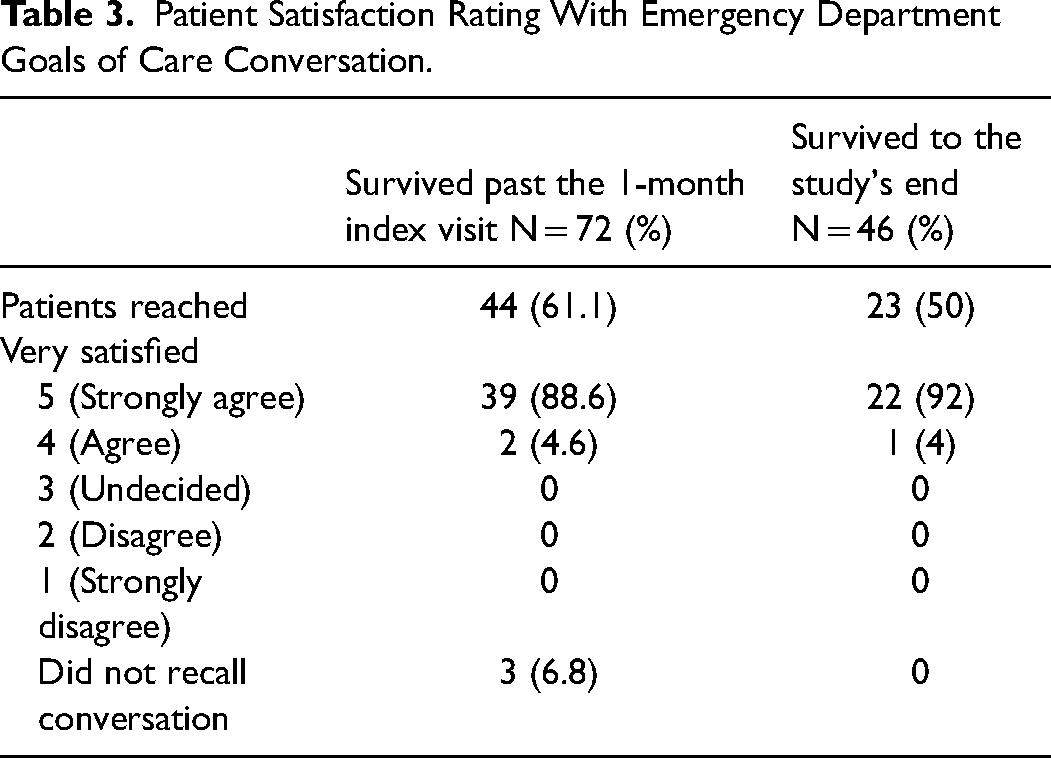
In the survival to the study's end cohort, 23 (50%) were reached for a satisfaction survey. 22/23 (95.7%) rated the experience 5/5; 1/23 rated it 4/5 (4.3%) (Table 3).
ED Visits and Hospital or ICU Admission
In the survival to the study's end cohort, ED visits decreased, the mean changed from 4.3 visits in 12 months preindex to 3.0 postindex and the median was 3.0 (IQR: 2.0-4.8) visits in 12 months preindex and 2.5 (IQR: 1.0-4.0) postindex (P = .028). The number of hospital admissions and length of hospital stays were similar in the prior- and postperiod (Table 4).
Emergency Department Visits/Hospitalizations/ICU Stay in 12 Months Pre- and Postindex Visit for Patients Who Survived to the Study's End (46 Patients).
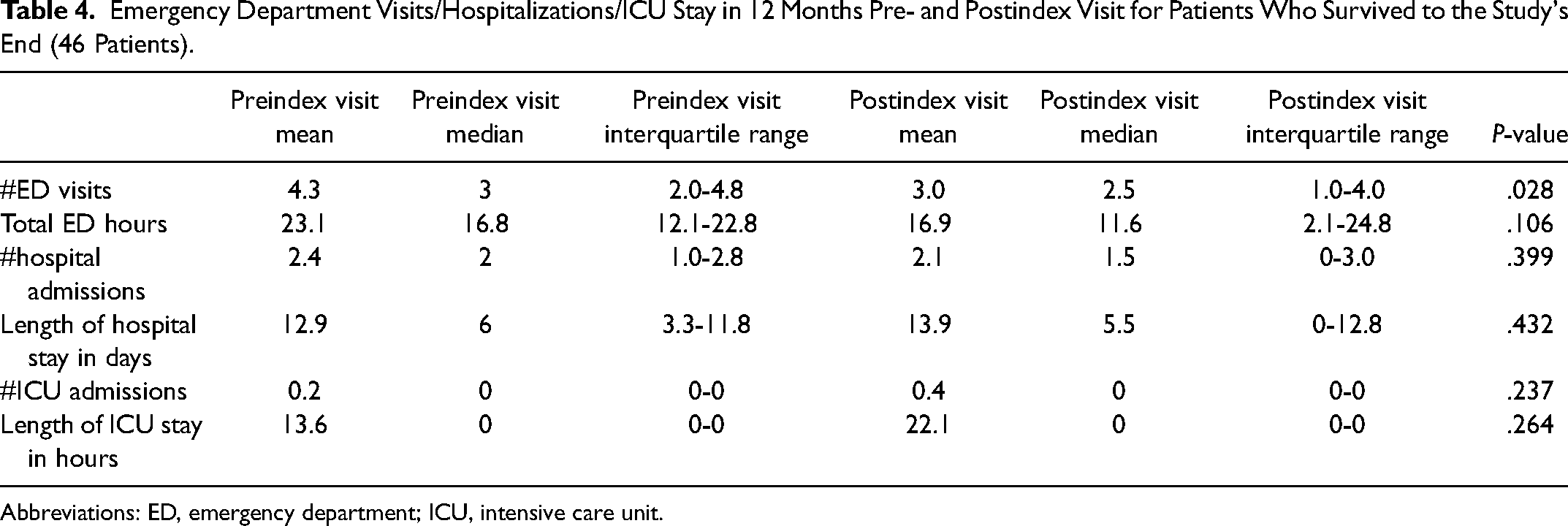
Abbreviations: ED, emergency department; ICU, intensive care unit.
ED length of stay could not be analyzed because of an extended period of in-patient boarding within the ED that occurred during the study period. This artificially lengthened patient ED length of stay.
Hospitalizations were similar with a median preindex rate of 2.0 (IQR: 1.0-2.8) hospitalizations/patient to a postindex rate of 1.5 (IQR: 0-3.0) hospitalizations/patient (P = .399). Total inpatient hospitalization days in the 12-month pre- and postindex period were similar, with a median of 6.0 to 5.5 total days (IQR: 3.3-11.8; P = .423) (Table 4).
There were 11 ICU admissions in the preindex period and 17 in the postindex period (P = .237). The length of ICU stay was longer in the postindex visit period, increasing from a total of 625 to 1017 h for all 46 patients (P = .264) (Table 4).
Midway through the study, one of the only 2 area palliative care organizations closed and we were unable to access their data/records. We were unable to ascertain how long patients had been on palliative care service, and whether they had transferred to another organization, and had difficulty obtaining accurate hospice service admissions and length of stay data. Thus, we were unable to analyze our hospice and palliative care data.
Discussion
All enrolled patients (100%) had their GOC recorded in their EMRs. One-third presented to the ED on the index day with a POLST already completed, so we were able to increase the number of patients with a completed POLST by another 1/3. That is, 50% of the patients without a POLST on arrival to the ED left with a completed POLST. Ideally, every patient enrolled would have completed a POLST form at the time of their GOC conversation, but some patients needed more time to reflect on their wishes and discuss them with their families before they felt comfortable committing their decision to paper.
ED patients were very satisfied with the GOC conversation and comfortable being approached in the ED. We were able to reach approximately half of the patients for the follow-up phone survey. Of those contacted, 95% rated the conversation as 4/5 or 5/5. Care was taken with respect to when the GOC was initiated. Our nurses waited until the patients had been in the ED for at least an hour, all the bloodwork had been obtained, and the patient was awaiting results. The nurse would then speak with the patient's primary ED nurse to make sure “now is a good time to come by.”
There have been prior studies on GOC conversations taking place in the ED. One adapted the brief negotiation interview to an 11-min intervention and found increased receptivity to the discussion as well as in POLST forms at 6 months. 29 Another used ED-nurse-initiated serious illness conversations as a means to prime the patient for further GOC discussion with their primary provider. 30 What is unique and innovative about this current study is that we demonstrated that patients could be approached about GOC leading to a completed POLST during that visit in the ED.
Having an in-depth GOC conversation and recording it in the EMR takes time that ED doctors and APPs lack.20,22–26 This study demonstrates that with proper training, nurses (and presumably other trained allied professionals) can have these conversations in the ED. The mean conversation duration was 47.5 ± 19.5 min. Some were shorter at 15 to 20 min because the patient already had a POLST form which the ED GOC RN reviewed and updated. For some patients, this was a first-time discussion and took more time. This conversation is best had by someone dedicated to this role without concurrent clinical duties in the ED.
Our population was elderly and sick. We chose diagnoses that were likely to cause death within the next 1 to 2 years. A minority of the patients had a completed POLST form which is similar to other studies.19,31
ICU admissions are often used as a measure of aggressive treatment for patients at end of life. A total of 20% to 30% of patients at end of life are admitted to ICU. 32 It has been reported that end-of-life patients who are in possession of treatment-limiting POLSTs are associated with significantly lower rates of ICU admission. 33 In this study, total time in the ICU increased, though it was not statistically significant. This is contradictory to what would be expected, and there are insufficient data to determine the cause or whether this trend is real. It does bring up the issue that having the POLST is only helpful to the patient if it is easily found by the treating ED team, and if the wishes are tightly followed.
Inpatient hospitalizations had no significant changes. It was essentially flat at 2 hospitalizations/patient/year. Once the patients were admitted, their hospital stays were not any shorter. There was a decrease in the number of ED visits postindex visit.
As a patient's illness progresses, one would have expected an increase in ED visits and hospitalizations. This suggests we may be seeing a decrease in hospital use among our population. Without a more in-depth chart review, it may be that some of these patients transferred to a palliative or hospice organization after their index visit.
We are unable to comment on whether the ED GOC conversation led to increased hospice or palliative care service enrollment due to insufficient data.
We recommend the next step be a larger randomized trial. Future study design should take into consideration patients with a diagnosis of cancer with metastasis with respect to intervention times and study duration. These patients were ill, and most of them died before the completion of their 12-month postconversation interval.
The need to have and record these conversations is only growing as the population ages, living longer with much more complex medical conditions.1,2 These conversations require a specific skill set that can be learned.10,11 It is rare that an in-patient palliative care team will be able to meet the ED demand. The embedded ED GOC nurse represents one way to get ahead of this issue. It is already challenging to find a completed POLST form within the EMR in a timely fashion.13–17 Standardization of the conversation and location in the medical record would be a dramatic improvement. This is a billable conversation and can theoretically support the position. Recent changes to Medicare now allow one to bill for the conversation.34,35 The revenue generated would cover the cost of the RN or social worker. With ED-embedded social workers already available, perhaps this is a learnable skill that can be added to their role if the ED RN is not an option.
Limitations
The sample size is small. It was a convenience sample, there was no randomization, and patients could choose not to participate. As we don’t know any characteristics of that nonparticipation group, there may be biases in the patient group who consented to take part or those who chose not to participate. A significant number of patients were lost to follow-up. Almost half the study population died before reaching the study's end. Most patients whose inclusion criterion was cancer with metastases died before the end of the study (2 survived to the end of the study) (Table 1). Patients enrolled may have been more comfortable having a GOC discussion and generally less likely to use ED/hospital with increasing frequency as their disease worsened. This could have biased the ED/hospital usage data. The ED GOC RNs were in the ED from 9 AM to 5 PM, Monday through Friday. We don’t know how patients would react to being approached if they arrived in the ED in the evenings, on weekends, or overnight. Additionally, our population was primarily Caucasian, and our results may not be generalizable to other groups. DNR/DNI forms require a physician’s signature. The RN can have a GOC conversation with a patient, but there is still time required from a physician for the advanced directives to be signed. While we reported a high rate of POLST forms being signed in the ED, it can be inferred that this was a direct result of the GOC conversation, but this study was not designed to demonstrate a causal relationship between the 2.
Conclusion
In summary, the US population is aging rapidly 1 and living longer with serious illnesses. 2 These patients are presenting to the ED with increasing frequency. Waiting for ED patients are a potential missed opportunity to be approached about GOC. The majority do not have advanced care directives. 18
This novel study demonstrates that trained individuals can approach patients about GOC in the ED and that this leads to a significant number of completed POLST forms. Patients are receptive to and highly satisfied with these encounters. These conversations can take place during an ED stay while patients await test results without interrupting patient care. These discussions can be billed under Medicare, so it is possible that a financially viable model can be developed.34,35
Footnotes
Acknowledgments
This work was supported by the Clinical Transformation Council, Providence Regional Medical Center Everett, Washington. Support from Anne Pau, senior clinical analyst, (Providence Regional Medical Center Everett, Washington) for initial data acquisition and preliminary statistical analysis. Grant acquisition, staffing, and logistical support from Julie Zarn, BSN, RN, NE-BC (Providence Regional Medical Center Everett, Washington). A big thank you to Dr. Joanne Roberts and Dr. Enrique Enguidanos for helping to bring this project to completion.
Author Contributions
Suzanne Bigelow, primary investigator, study conception and design, lead author. Ron Medzon, contributor, drafting of article. Mari Siegel, contributor, drafting of article. Ruyun Jin, biostatistician, drafting of article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was reviewed, approved by, and had oversight provided by our system institutional review board, Providence St. Joseph Health Human Research Protection Program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Providence Clinical Transformation Council.