
Abstract
Introduction
The most intensive use of health care services by patients occurs in their final months of life.1,2 This period of increased health care use is also associated with increased transitions to different care settings. Regrettably, not all transfers or transitions are positive experiences for patients and their family caregivers. Each of these transitions may pose a potential threat to continuity of care and patient safety. 3
Transitions to new care settings are stressful for patients with advanced illnesses. Transferring patients at the end of life (EOL) has been shown to lead to increased suffering and decreased quality of life (QOL) in the final weeks or months of life. 4 Reasons for negative transition experiences include: the physical transfer itself, distress due to new and unfamiliar settings and providers, inability to address patient needs and level of communication. 5
Challenges in communication during transitions can occur between transition teams who may also lack sufficient coordination and effective processes to carry out the transition. 6 Patients with poor quality transfers are more likely to feel unsupported, unheard, and struggle with feelings of abandonment, guilt, and uncertainty. 7
Previous research has focused on the perceptions of the health care team during care transitions near the end of life. 8 The aim of this qualitative study was to explore the experience of transition to a PCU near the EOL from the patient and family caregiver perspective.
Methods
Setting and Participants
This qualitative study took place at a hospital based PCU in Toronto, Canada. Our 19 bed PCU admits patients with life limiting illnesses in their last 3 months of life. Research ethics board approval was granted by the Research Ethics Board at West Park Healthcare Centre and Salvation Army Toronto Grace Health Centre.
To be included in the study, patient participants required a Palliative Performance Scale (PPS) score of 30% or higher and the capacity to participate in a discussion about their transition experiences as determined by the physician investigators. While our preference was to interview patients, a family caregiver could participate if they were actively involved in caring for the patient and had knowledge of the patient's care transitions. Some interviews were completed jointly with the patient and their family caregiver. In instances where the patient was unable to participate in the interview due to a decline in their condition, the family caregiver was interviewed alone.
Convenience sampling was used, with a maximum variation sampling approach to elicit a fuller picture of the range of palliative care transition experiences. 9 We attempted to recruit participants with a range of demographic and treatment experiences. Translation services were made available during the interviews, with one participant using this service.
The physician and social worker investigators (DS, KW, BL, JM) recruited patient and family caregivers to the study and a research associate trained in qualitative interview techniques conducted the interviews.
Data Collection
In person interviews were conducted with 24 participants, and telephone interviews were conducted with 5 participants. Fourteen patients participated either alone or with their family caregiver and 15 family caregivers participated alone without the patient present. The research associate (KA) conducted all of the interviews between July 13, 2018 and January 24, 2020.
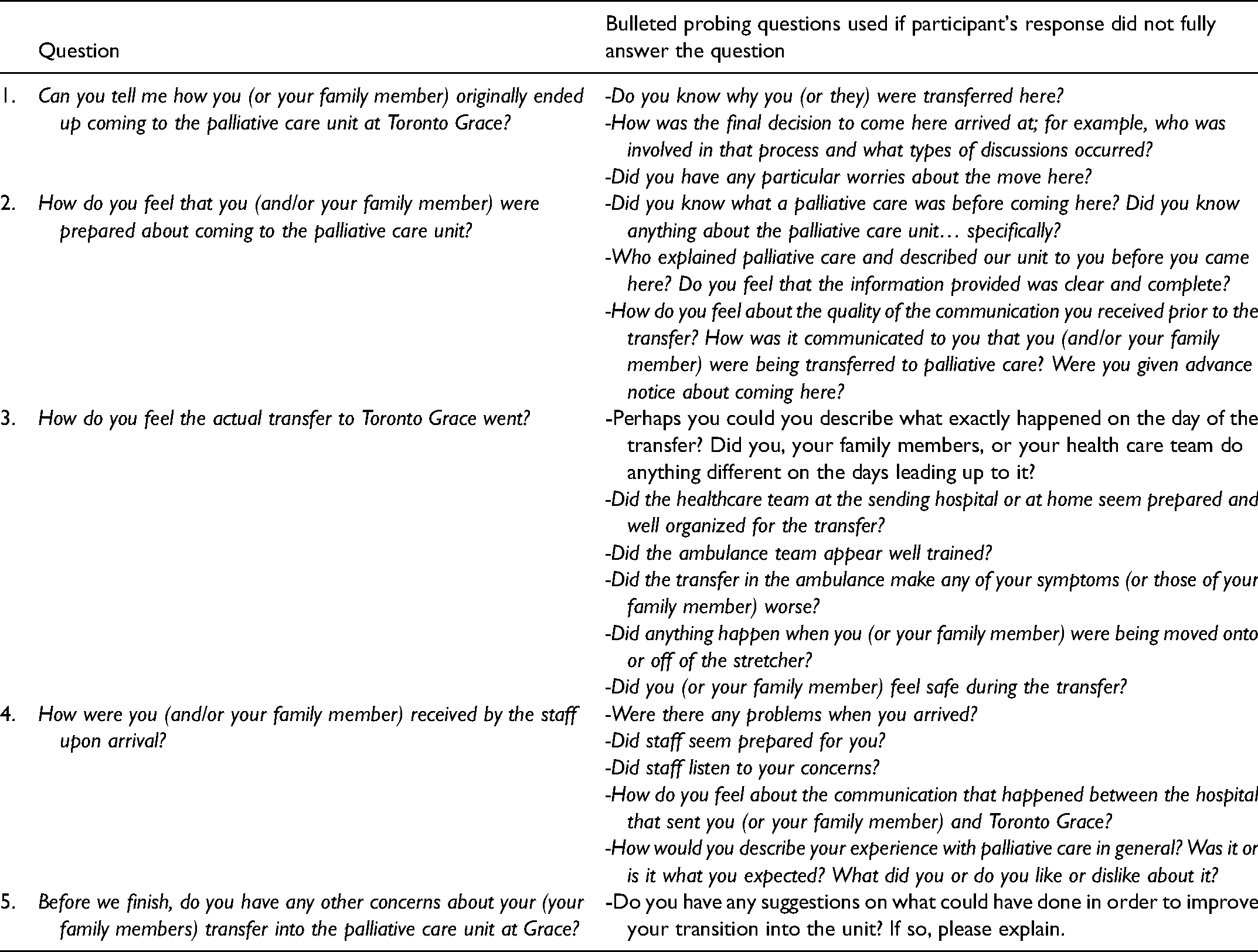
While an interview guide (Table 1) was developed to ensure discussion of general aspects of transition related experiences, a semi-structured interview approach was used to encourage broad discussion of participants’ transition related experiences.
Interview Guide Questions.
All of the interviews were audio recorded and later transcribed verbatim; these transcripts were then imported into NVivo 11, a software package that was used to assist in management, organization and selective retrieval of the qualitative data during the data analysis process.
Data Analysis
Interpretive description was the overriding approach used to analyze the transcripts to better understand the experiences and impact of the participant experiences. 10 The approach was inductive and iterative. Transcripts from the interviews were read multiple times and text was coded descriptively. 11 Codes were then grouped and categorized according to the key themes. An iterative process of constant comparison was applied wherein themes were generated, continually tested and revised based on new readings and interpretations of the original transcripts. 12 Sampling was continued until thematic saturation was reached.
Results
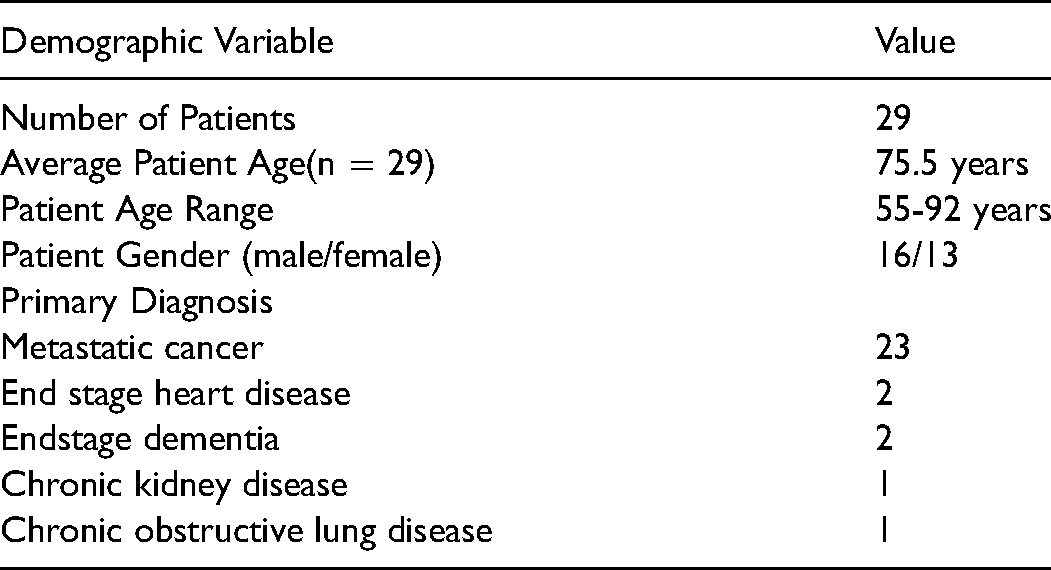
Interviews ranged in length from 12–125 minutes with the average semi-structured interview lasting 47 minutes. Of the 15 family caregiver participants, 8 were spouses, and 4 were adult children. The remaining 3 were an adult grandchild, niece and daughter-in-law. A profile of participant study patients, is summarized in Table 2. Patient demographic information is used in the table regardless of whether the patient or the family caregiver participated in the interview.
Patient Characteristics.
Themes
After qualitative analysis of the transcripts, the following 5 themes were identified:
Most participants described feeling informed about what to expect in terms of their health care when coming to the PCU. They reported having their health related questions adequately addressed by the team at the receiving PCU. Some participants, however, were still unclear about the nature of palliative care and, in some cases, about their illnesses and prior treatment details.
While many participants appreciated the prompt availability of a PCU bed and acknowledged the challenges of health care resource allocation, some participants described the quick transition as stressful.
Numerous participants raised concerns about communication. They reported they were not in a mental or emotional state to fully understand the information when it was provided and some identified that being given written material helped them to process information at their own pace.
“what would be extremely helpful is not only sit down and talk to the families when they’re transitioning into palliative… but you give them something to take with them. So that in a moment of calm they can read and know that some things [referring to loved ones symptoms and behaviour] are normal. Do you know what I mean?”(P16)
Others suggested it would have been helpful to include the whole family during discussions as a way to improve palliative care understanding for all. They stressed that too much responsibility was implicitly placed upon the family member who happened to be in attendance at these discussions and some worried that their lack of medical knowledge made them less suited to relay information to the rest of the family. As one participant explained,
“…what they[doctors] don’t understand is that I still have to go to my family and explain it all to them and I don’t work in palliative care and I don’t work in nephrology. I don’t work in any of the things that are affecting her to be palliative …. like I don’t deal with this and I don’t know how to explain to a family member”. (P29)
While inpatient palliative care relieved family caregivers of many of the practical challenges of providing patient care at home, some reported not being prepared for the new challenges that occurred. Some family caregivers shared feeling guilty transferring their loved one into inpatient palliative care, especially if they had wanted to die at home. Some spousal caregivers also struggled with being home alone for the first time. “We were married for 52 years you know and always together…so for me to be at home alone is sad.” (P26)
2.
Many patient participants identified having an advocate as essential during the transition and emphasized both family members and health care professionals as fulfilling this role.
Family participants felt they and other caregivers played a vital part in influencing their loved one's transition. They provide emotional and spiritual support, and also offered significant informational support and guidance. Many caregivers played a central role in navigating the health care system for patients and in making key inquiries, decisions and arrangements for them, owing to their diminished health status. Patients described how this unburdened them and made them more confident about the transition. “My kids are very hands on, involved in every step of my care. They spoke to the oncologist even when I wasn’t around… They explained what palliative care was to me even before I knew to ask … The amount of attention that my kids have given this has given me confidence. They are not leaving me to ride this out by myself.” (P6)
While patient participants appreciated the support, they also expressed concerns about the additional burden placed upon their families and the sacrifices being made. “I knew she would be upset… So she doesn’t come by at all because we keep her from knowing. Because she wouldn’t be able to handle it.” (P23)
The very decision to enter palliative care was often described as being motivated by the desire to take pressure off friends or family members. Some participants identified their lack of social support while in palliative care reflected a conscious choice not to burden others by informing them of the status of their condition.
3.
Patients’ ability to come to terms with being near the end of life affected their transition to PCU. Several spoke of having accepted and even embraced this final part of their lives. Accepting that they were going to die allowed them to reflect fondly on their life. They described setting aside anger and resentment regarding their condition, past setbacks and grievances, and expressed gratitude for the things and people around them as well as the time they had left. “I try to keep my mind on how to be the best I can in going out you know. Not resent anybody. Not be angry or, or disappointed. I have had a good life, a good career, a good education and piles and piles of good friends so that’s where I am at.” (P30)
A few participants expressed anger over their condition and regrets over life situations or personal behaviors, such as smoking, that may have contributed to their illnesses. Some continued to focus on physical recovery, the future and things they had yet to experience or achieve. “Palliative care is about waiting to die. …And I mean that’s not what I am waiting for. I am waiting to get standing and get in motion and get going back home. ..They [the healthcare team] suggested [palliative care] but it’s not my plan.”(P25)
“I felt apprehensive about coming here because the one thing I absolutely dislike is having to give up my independence … I accept [death] as part of life but the fact that I cannot get up and go to the toilet or to go and have a wash without having a nurse help me that upsets me.”(P6)
Often participants felt disempowered which was a challenging part of their transition to PCU. “… I felt quite insulted because I considered myself an adult woman and I know that places like this have to have their rules and regulations, [but] I don’t get dinner when I say I am hungry. I don’t get breakfast when I say I am hungry… I just thought, he [doctor] must have thought I was awfully stupid not to realize that I would not be…in charge.” (P1) 4.
Many participants described that their greatest struggle was the uncertainty about when they or their loved one would die. “The thing that needs to be improved is the way they (prognosticate)…how much time the person has. I feel like that is so severely different in each place you go…I think because they don’t know they just say a number and the family kind of calculates their whole life around that number.” (P29)
“…It appeared that my husband was…very close to the end and then he kind of rallied and was a little better. And so we [my children and I] were anxious because we couldn’t stay … And the medical people…said, we really don’t know…it could be tomorrow…” (P3)
Many mourned the potential loss of care relationships they had made in the PCU setting. They compared their current PCU environment to the environments they were expecting to be transferred to(often perceived as less favorable). “I think I will will myself to die. No, I don’t want to do that at all [go back home or to other facility]. It scares me and I don’t know where they would put me. I don’t know what kind of care I’d get. You can’t replicate this so don’t move me please. That’s how strongly I feel about it…”(P13)
5.
Most patient and family participants recounted how their actual transfer to PCU went smoothly. However, some participants experienced issues related to coordination and continuity of care. Last minute procedures, such as catheter removal or medical procedures needing to be completed could complicate the transfer, leading to tension between participants and transferring facility staff. For example, one participant described how she was told to meet the ambulance attendants for her husband's discharge at a specific time, only to be left waiting for hours due to delays which were not communicated to her. She reflected on this negative experience. “I sit there all day ….and I talked to the lady and the lady said they are going to come …. If they know they are not going to be on time they should tell you… it’s wasting your time and you sit there waiting and waiting, and waiting.”(P2)
In order to address issues with coordination during the transfer, some participants suggested that the receiving PCU could play a greater role in communicating with the facility transferring the patient prior to the actual transfer.
Factors that lead to anxiety on arrival to the unit included not getting the room they felt they had initially been promised, concern about medications and whether all relevant information had been transferred. One participant suggested a more transparent process by which family could confirm the multitude of prescriptions, and medical information that a patient typically acquired from multiple facilities would be helpful.
Others spoke about the loss of relationships during the transfer process, they lamented how longstanding and meaningful relationships with earlier health care providers, such as the oncology teams and home care providers, were lost when the patient entered a PCU.
Discussion
Transitions to different care settings are common for patients in the final months of life. Participants we interviewed felt
Some participants who reported a less positive transition experience expressed feeling overwhelmed by the amount of information presented to them. It is interesting that some participants would have preferred having more family members and friends involved in discussions about care decisions especially considering the emphasis on health care information not being shared outside the patient's immediate circle of care. An unintended consequence of strict adherence to privacy regulations is that some patients may feel overwhelmed at having to understand detailed and voluminous information themselves or with only one family member. Wilson describes similar communication complexities such as strict information privacy concerns and avoidance of difficult conversations that can lead to transition difficulties. 6
Some participants expressed a feeling of fear about the transition and others reported a feeling similar to “giving up” which has been recognized previously as a common theme for patients transitioning to palliative care. 16 These findings suggest a need for improvement in communication between the health care team, patients, and their families with an emphasis on reframing hope and the idea of palliative care.
Some participants also reported feeling unable to fully consider palliative care transition decisions because of time constraints imposed by the clinical team or the greater health care system. They shared feeling pressured to take the first bed available even if it was not the preferred choice for them, leading to feelings of unpreparedness and frustration. This is significant as the perception of lack of choice and flexibility in considering individual wishes has been identified as one of the major stressors in a transition to PCU and is a known fear for patients in the dying process.7,17,18
Our findings support the importance of ensuring the circle of care extends to families who may themselves be experiencing transition related stress; for example, adjusting to the absence of loved ones at home, feelings of guilt, and emotional struggles all of which are highlighted in our study and have been reported previously.13,21,22 Some family stressors may not be apparent to health care providers but may be significant to the patient-family unit's ability to cope with the transition. Families have additional burdens that they must navigate outside of hospital. These challenges felt primarily by the patient-family unit, have a direct impact on patient satisfaction with the transition to PCU. This is significant as a commonly feared aspect of dying for patients is anxiety for their family. 23
We were surprised to find that a significant source of stress for participants was uncertainty surrounding what would happen if their condition improved or stabilized and patients needed to be either transferred from the PCU to another care facility or discharged home. Discharges are unusual as most patients die on the PCU. It was interesting to find that participants’ fears of leaving the PCU were similar to those that they experienced when arriving; for example, fear about changes in care, decreased choice, feelings of abandonment and being “put somewhere”. This reinforces the likelihood that anxiety about care transitions near the end of life is universal regardless of the physical location that the patient is transitioning to.
It has been suggested that each transfer is a threat to
Limitations
While yielding important insights into the participants’ experiences during transition, our study has some limitations. We included only those patients whose PPS scores were 30% or higher and who were or had family members who were able to participate in a complex conversation. In excluding other patients, we may have missed important information unique to less well patients. The inclusion of caregivers as participants may have had the unintended consequence of over emphasizing the experiences of those patients whose families were more present and involved.
Given the short survival and changing condition of some of the patients, more caregivers’ opinions were recorded than the patients themselves. This may have resulted in the experience and opinions of caregivers being overemphasized.
Conclusion
Our study contributes to previous research on care transitions near the end of life by examining the transition experience from the perspective of both patients and their family caregivers. Semi structured interviews were carried out from which five themes were identified; Being prepared, Feeling supported, Coming to terms with end of life issues, Dealing with uncertainty, and Continuity of care. Our findings highlight the need for clear and iterative communication especially about topics such as prognostication, declining clinical status, and decision making that involves patients and their family caregivers. Consideration of ways to optimize patient experience in these domains will help health care teams to better facilitate and improve patient care and satisfaction with these transitions.
Footnotes
Acknowledgments
We are grateful for the generous support of the patients and family caregivers who shared their time and experiences with us in carrying out this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from the Toronto Grace Health Centre to conduct this research.
Ethical Approval
Approval for this study was granted by the West Park Healthcare Centre- Salvation Army Toronto Grace Health Centre Research Ethics Board.
Informed Consent
Informed consent was obtained from all study participants.
Trial Registration
Not applicable, because this article does not contain any clinical trials.