
Abstract
Background
In 2019, a termination of pregnancy (TOP) service was established in Ireland following a landmark change to the constitution. Under Section 12 of the Health Act, TOP is permitted without restriction until 12 + 0 weeks’ gestation.
Methods
Retrospective review of inpatient medical TOP under Section 12 between 1 January 2019 to 31 December 2022 in a single tertiary maternity hospital in Ireland. Anonymised data from eligible cases was obtained from electronic healthcare records.
Results
The final cohort included 149 individuals. Gestational age (>9 + 0 weeks’) was the primary indication for hospital TOP (81.2%) with over 44% of the cohort at >11 + 0 weeks’ gestation. Misoprostol was administered within the recommended 24–48 h from mifepristone in 75.2% of cases. After one course of the medication regime, 9.4% of individuals required additional doses of misoprostol to complete the termination. Haemorrhage with blood loss >500 ml occurred in 4.2% of cases, with no other major/significant complications reported.
Conclusion
This is the first reported review of the efficacy and complications of the newly established Irish TOP service. Findings highlight the importance of timely access to care given the strict legal gestational cut-off. Variations in practice, specifically in timing of medication administration, were also shown.
Keywords
Introduction
In 2018, following a national Referendum, a landmark change to the Constitution enabled the introduction of legislation of termination of pregnancy (TOP) services in Ireland. Prior to this reform, access to TOP was limited to situations where there was a risk to the pregnant individual's life due to either physical or mental illness (Goverment of Ireland, 2013). As of the 1 January 2019, TOP was permitted under four specific circumstances, each outlined in a respective section of the legislation (Goverment of Ireland, 2018):
Without restriction until 12 + 0 weeks’ gestation (Section 12). Until foetal viability in the context of a significant risk to the life or health of the pregnant individual (Section 9). Until foetal viability in an emergency posing a risk to life or health of the pregnant individual (Section 10). Without gestational limitation in the presence of a foetal condition where the foetus is predicted to die within 28 days of birth (Section 11).
Annual reports from the Department of Health have shown that 98% of TOPs each year are performed under Section 12 of the Act, thus accounting for the majority of service provision (Department of Health, 2019, 2020, 2021, 2022b).
To provide TOP care under Section 12, a national freely accessible public service was established with a designated care pathway to direct points of access. Individuals seeking a TOP before 12 weeks’ gestation, otherwise known as an early TOP, contact a helpline or website (www.myoptions.ie), which provide non-directive counselling with signposting to all options including antenatal support and local service options. The initial consultation (visit one) is with a community-based general practitioner provider who makes an assessment about whether the TOP can be conducted in the community or whether a referral for ultrasound or to secondary care services is required. A 3-day waiting period is legally mandated from visit one until visit two, when the TOP can then be prescribed in the appropriate setting (National Women and Infants Health Programme, 2023).
The framework for the new service is outlined in the Model of Care: Termination of Pregnancy Services published by the Irish Health Service Executive (National Women and Infants Health Programme, 2023). It utilises an integrated model of care between community-based primary care providers and maternity hospital-based obstetricians and gynaecologists. Within this framework, general practitioners provide medical TOPs in the community to individuals without medical comorbidities who are less than 10 weeks’ gestation; while obstetrician and gynaecologists provide medical TOPs in secondary care settings between 10 + 0 to 12 + 0 weeks’ gestation, all surgical TOPs, and care for individuals with medical comorbidities preventing community TOP. Thus, individuals that meet the criteria for referral to secondary care have their TOP as inpatients in the hospital setting and are required to stay in hospital until delivery of the pregnancy. Clinical guidelines regarding early TOP provision have been published by the Irish Institute of Obstetricians and Gynaecologists (IOG), the Irish College of General Practitioners (ICGP), and the National Women and Infants Health Programme (NWIHP), and have served to establish the standard of care (Boyd et al., 2022; Institute of Obstetricians & Gynaecologists, 2018; Quality & Safety in Practice Committee, 2021).
The World Health Organisation Abortion Care Guideline 2022 provides an international clinical standard for TOP services and has emphasised the need to provide high-quality care, rather than solely safe TOP care (World Health Organization, 2022). However, there is still a need to determine the quality indicators that are associated with improved health and experience outcomes (Darney et al., 2019). In the current literature, indicators of access/availability and service provision, such as provider availability and financial access, are most commonly measured, whereas indicators of outcomes, such as adverse events or TOP completion, are underreported (Filippi et al., 2021). To evaluate TOP services, valid and standardised indicators of quality of care on both individual and population levels must continue to be established.
This study provides an overview of the first four years of inpatient TOP service provision carried out under section 12 at a single tertiary maternity unit in Ireland. We sought to establish the standard of care provided, review procedures and complications, identify areas of improvement, and inform future resource allocation.
Methods
A retrospective review was conducted of all inpatient medical TOP procedures under Section 12 between 1 January 2019 to 31 December 2022 in a single large (>7000 births) maternity hospital. Individuals either self-presented to the emergency department or were referred by a community-based TOP provider within the catchment area of the Ireland South Women and Infants Directorate, which encompasses four counties (Cork, Kerry, Waterford, and Tipperary) spanning 176 km2. Referrals were made if the criteria for a community TOP were not met or in the context of an ongoing pregnancy after early medical TOP in the community setting.
Initially, hospital TOP provision in this unit was an ad-hoc service with a limited number of consultants providing care in conjunction with an interim TOP midwife coordinator. Following the appointment of both a clinical consultant lead in TOP and a dedicated TOP midwife coordinator, standardisation of service was possible, with the introduction of regular clinics and clinical pathways for admission. Medical TOPs were carried out as per the national clinical guidelines with a regime consisting of oral mifepristone, which was administered at the second outpatient clinic visit, and buccal misoprostol, which was administered on the gynaecology ward following admission to hospital 36 h later. One round of the regime consists of one dose of 200 milligrams of mifepristone and up to five doses of misoprostol. An initial loading dose of 800 micrograms of misoprostol is given, which is then followed by up to four 400 micrograms doses administered at 3 hourly intervals until delivery. All medications were prescribed using pre-populated care plans in the electronic health chart to ensure standardisation. Unsuccessful or incomplete TOPs were managed either with additional doses of buccal misoprostol, manual removed of pregnancy tissue, or surgical TOP.
TOPs that were conducted under Section 12 in the hospital setting were identified from the hospital registry. Cases were excluded if individuals were managed as outpatients or opted for primary surgical management, so that the cohort reflected cases who had inpatient medical TOP. Additionally, cases were excluded if the medical TOP occurred during the cyberattack in May 2021, which affected the electronic healthcare records (Moore et al., 2023). Anonymised data were extracted from the electronic healthcare records and transcribed into a dataset on Excel. Various data points were recorded encompassing sociodemographic characteristics, obstetric characteristics, and details of the medical care provided, such as timing between mifepristone and misoprostol administration, timing from the first dose of misoprostol to delivery of the products of conception, resultant complications and their management, duration of stay in hospital, counselling and provision of contraception, and access to non-directive counselling with a social worker.
Descriptive statistical analysis was completed using SPSS Software (version 29.0.1.0 (171)). Ethical approval was obtained from the Clinical Research Ethics Committee (ECM 4 (t) 22/02/2022) of the Cork teaching hospitals.
Results
Cohort
In total, 164 cases were identified from the hospital registry. The following cases were excluded: incomplete data (primarily because of the May 2021 cyberattack (n = 3)), not electing to continue with medical TOP following secondary care clinic consultation (n = 3), outpatient medical TOP (n = 6), and primary surgical TOP (n = 3). This yielded a final cohort of 149 individuals undergoing primary inpatient medical TOP (n = 42 (2019), n = 34 (2020), n = 34 (2021), n = 39 (2022)) (Figure 1).
There was a relatively even distribution of nulliparous (76/149; 51.0%) and multiparous individuals (73/149; 49.0%). Of the multiparous individuals, 30.1% (22/73) had had a prior caesarean section. The majority of individuals were residents in the county of the hospital where the TOP was performed (121/149; 81.2%) and had a TOP between 9 and 11 weeks’ gestation (68/149; 45.6%). The primary indication for hospital-based TOP was gestational age (121/149; 81.2%), with other indications including medical comorbidities preventing community TOP, unsuccessful medical TOP in the community, and the individual's request. Further information on cohort demographics and obstetric characteristics are reported in Table 1.
Sociodemographic characteristics, pregnancy history, and current pregnancy characteristics of TOP cases (2019–2022).
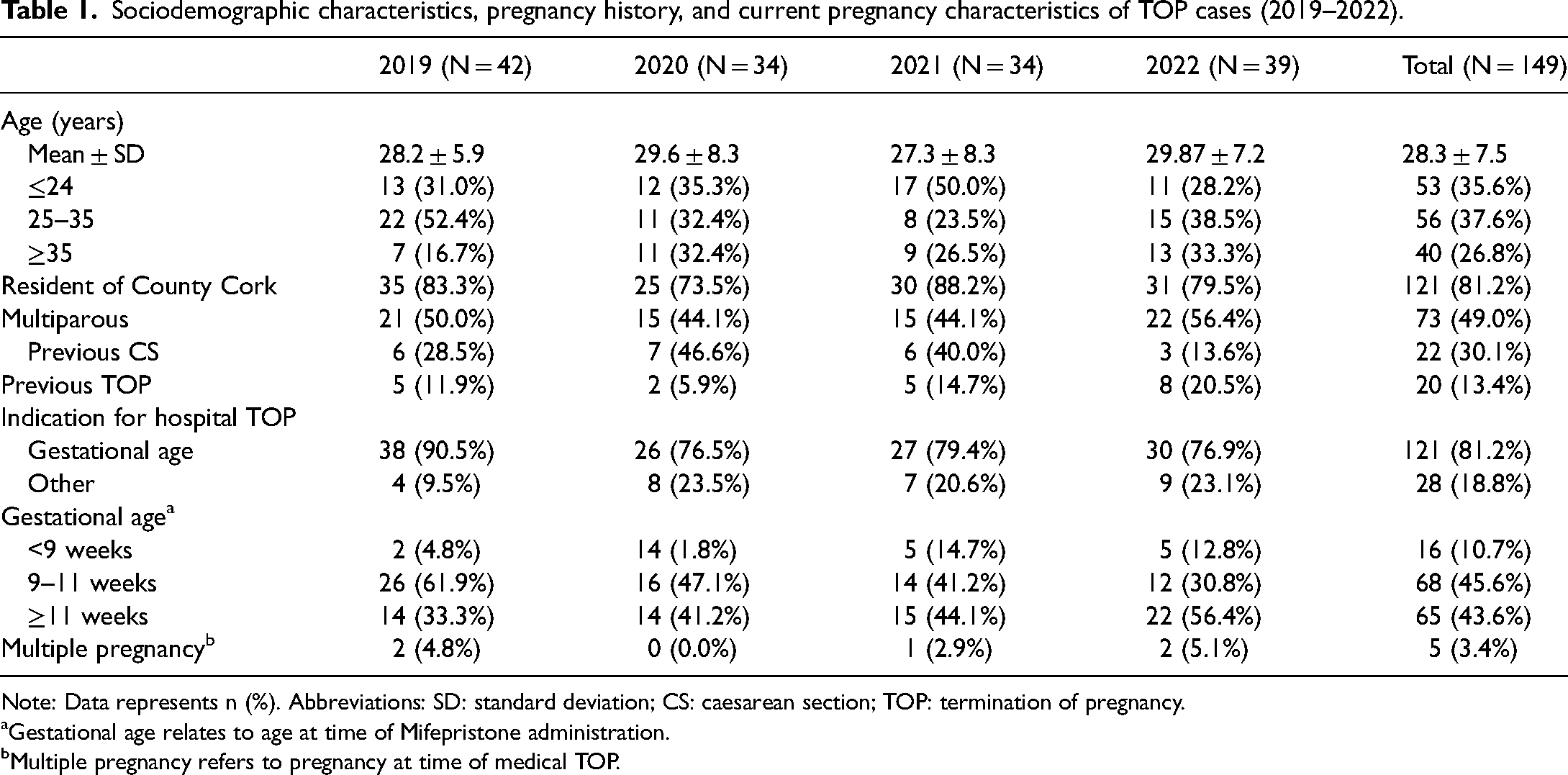
Note: Data represents n (%). Abbreviations: SD: standard deviation; CS: caesarean section; TOP: termination of pregnancy.
Gestational age relates to age at time of Mifepristone administration.
Multiple pregnancy refers to pregnancy at time of medical TOP.
Service overview including multidisciplinary team involvement, contraception provision, and duration of hospital stay.
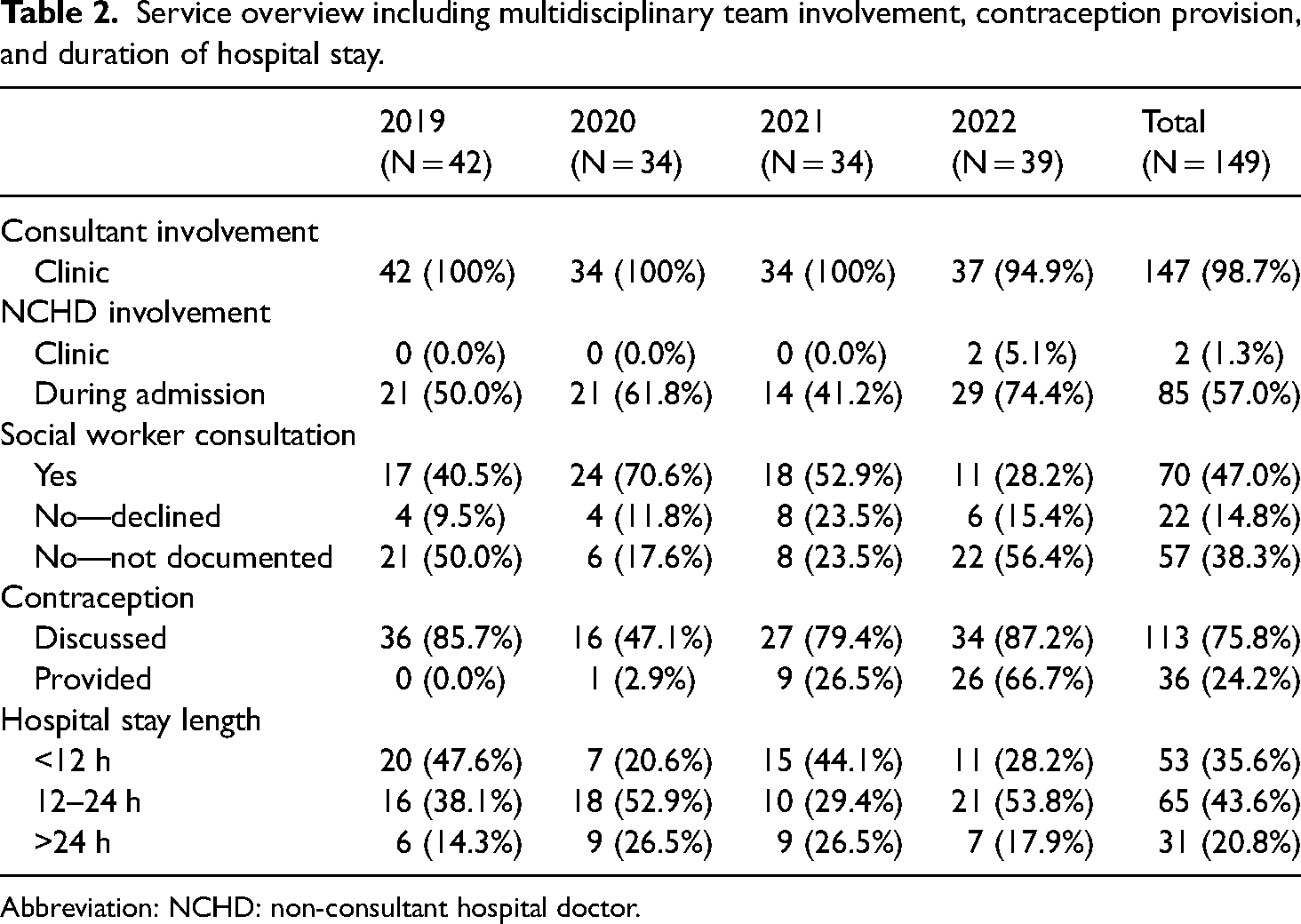
Abbreviation: NCHD: non-consultant hospital doctor.
Medications administered as part of medical TOP regime.
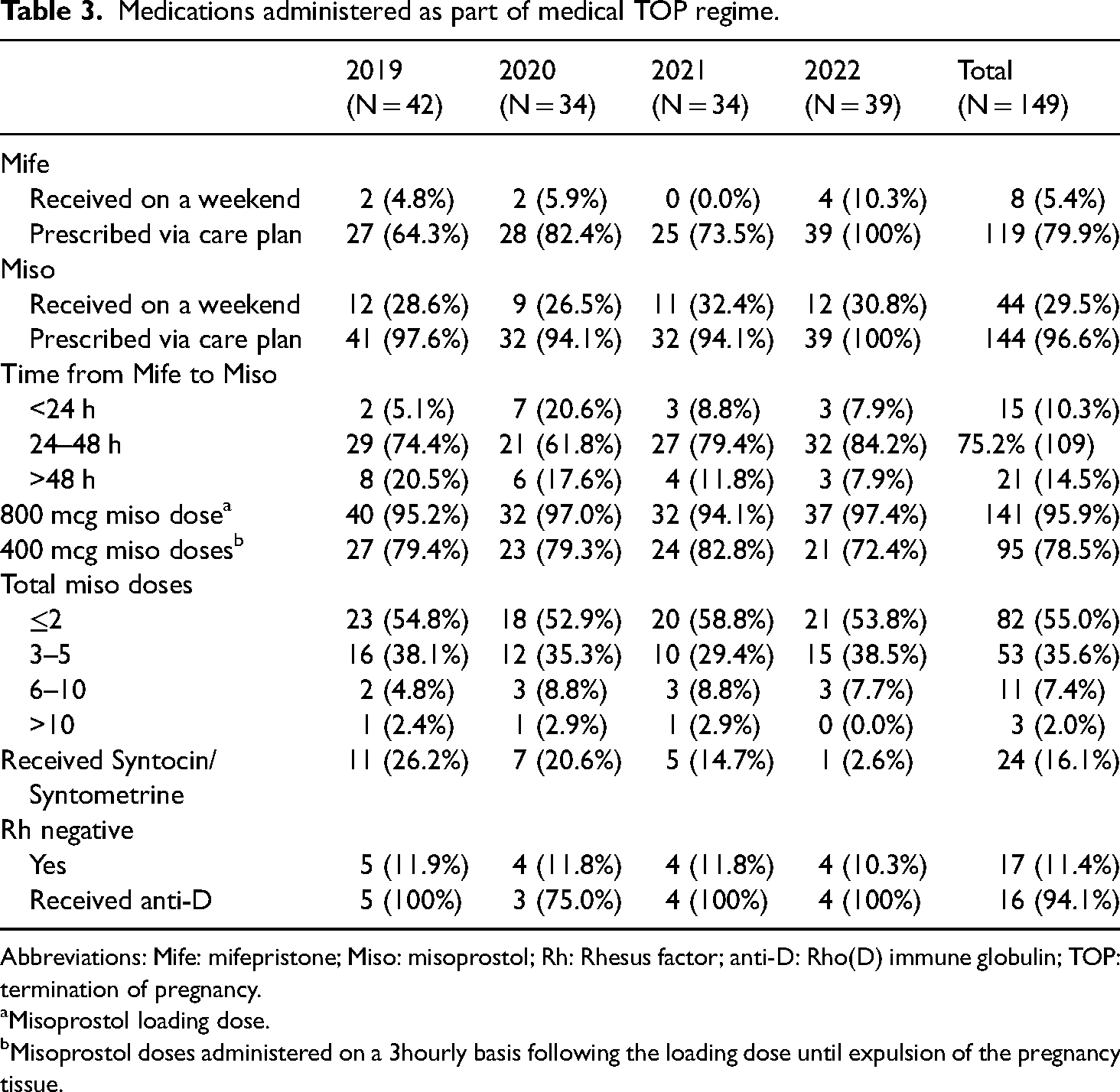
Abbreviations: Mife: mifepristone; Miso: misoprostol; Rh: Rhesus factor; anti-D: Rho(D) immune globulin; TOP: termination of pregnancy.
Misoprostol loading dose.
Misoprostol doses administered on a 3hourly basis following the loading dose until expulsion of the pregnancy tissue.
Overview of complications occurring during/after inpatient admission for medical TOP.
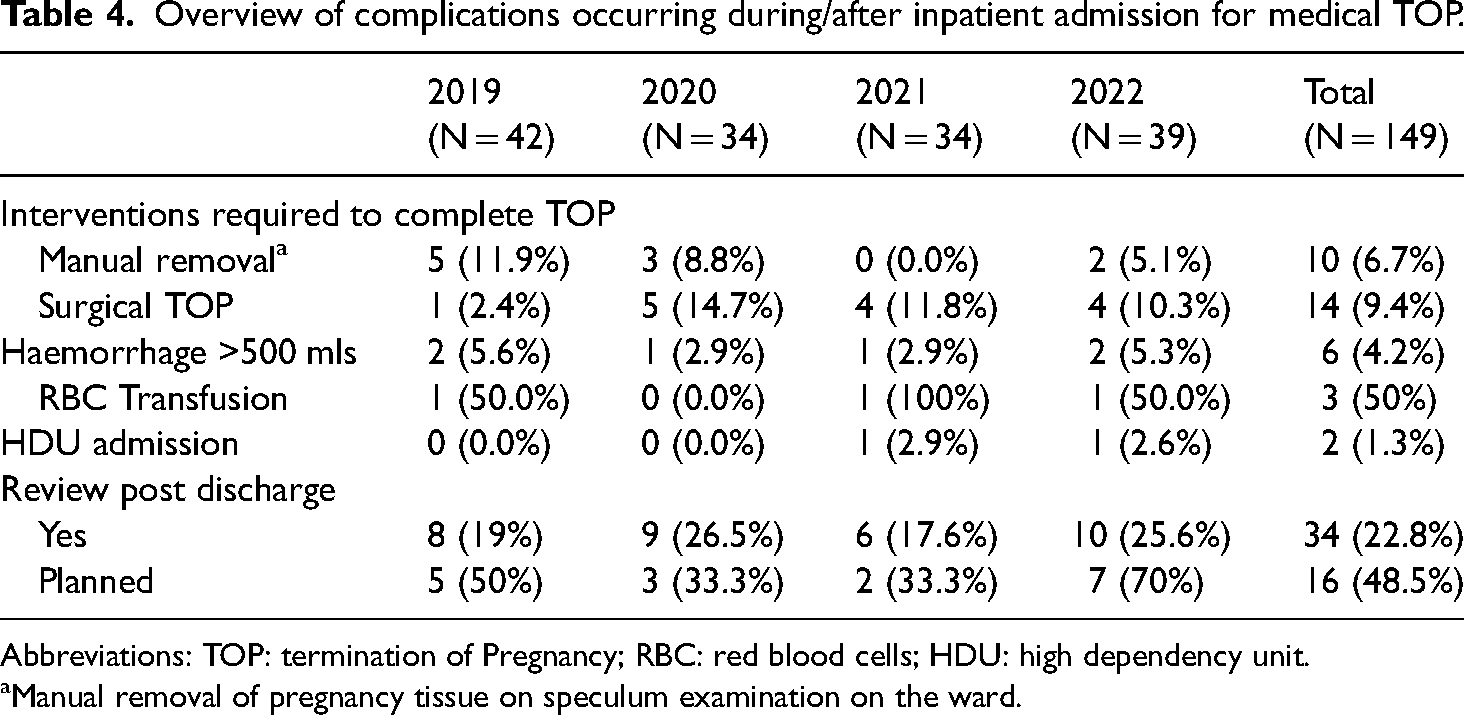
Abbreviations: TOP: termination of Pregnancy; RBC: red blood cells; HDU: high dependency unit.
Manual removal of pregnancy tissue on speculum examination on the ward.
Services overview
Individuals attended for consultation in the TOP clinic with a consultant obstetrician and gynaecologist prior to proceeding with medical TOP. Additional services utilised during these consultations included ultrasonography, optional counselling with a social worker, and/or interaction with a midwife TOP coordinator. Just under half of individuals opted for non-directive counselling with a social worker (70/149; 47.0%), while the remaining individuals either declined this (22/149;14.8%) or had no documentation stating it had been offered (57/149; 38.3%). Service provision with respect to pre-admission/clinic encounters were primarily consultant-led (147/149;1.3%); however, non-consultant hospital doctors (NCHD) involvement primarily occurred on a ward level (85/149; 57.0%). Contraception was discussed during the majority of pre-admission/clinic appointments (113/149; 75.8%); however, uptake and/or provision of contraception prior to discharge was low (36/149; 24.2%) with most individuals recommended to follow-up with their primary care practitioner. Provision of contraception improved each year (0/42; 0% in 2019, 1/34; 2.9% in 2020, 9/34; 26.5% in 2021, 26/39; 66.7% in 2022) (Table 2).
Medication
Pre-populated care plans for prescribing the medical TOP regime were available within electronic healthcare charts to reduce the risk of prescribing errors. In this cohort, these electronic care plans were used to prescribe misoprostol (144/149; 96.6%) more often than mifepristone (119/149;79.9%). The use of care plans for mifepristone prescribing improved each year (27/42;64.3% in 2019, 28/34;82.4% in 2020, 25/34; 73.5% in 2021, 39/39; 100% in 2022). Misoprostol was administered within the recommended 24–48 h of mifepristone administration in the majority of cases (109/149; 75.2%). Most instances occurring outside of this time period were due to delays in timing from mifepristone administration to admission to hospital, likely due to staff and bed shortages. The loading dose of misoprostol was appropriately administered to almost all individuals (141/149; 95.9%), and this remained consistent across the four years. Subsequent doses of misoprostol were appropriately administered within the advised timeframe of every 3 h (95/149;78.5%). The majority of medical TOPs required less than five doses of misoprostol to be complete (135/149; 90.6%). Syntocinin/syntometrine was administered routinely to assist completion of uterine evacuation and/or treat acute haemorrhage in a small proportion of cases (24/149;16.1%). This is despite it not being in the routine care plan as it's use is only indicated in the treatment of acute haemorrhage in the national guidelines. There were 17 rhesus negative individuals in the cohort (11.4%) and all but one, appropriately received anti-D immunoglobulin as is recommended by the British Society for Haematology for the prevention of haemolytic disease of the foetus and newborn (Qureshi et al., 2014) (Table 3).
Complications
In cases of ongoing pregnancy or incomplete TOP, whereby there is retained pregnancy tissue, following completion of one round of the medical TOP regime, one of the following treatment options were provided: additional doses of misoprostol were administered (14/149; 9.4%), pregnancy tissue was manually removed on speculum examination on the ward (10/149; 6.7%), or a surgical TOP was performed (14/149; 9.4%). There were no instances (0/149; 0%) of acute surgical complications in individuals who required surgical TOP with respect to cervical injury or uterine perforations, and all cases appropriately received antibiotic prophylaxis as per the national guidelines. Two individuals in the cohort required high dependency unit level care for one-on-one monitoring following significant blood loss. Six individuals had an estimated blood loss greater than 500 ml, of whom three received a red blood cell transfusion. A medical review following discharge from the hospital was sought by 34 individuals (34/149; 22.8%), of which 48.5% were scheduled clinic appointments (16/34) and the remaining were unplanned presentations by individuals to the emergency department (18/34; 52.9%). Presentations for emergency review were primarily due to concerns regarding infection or heavy/irregular vaginal bleeding. We were unable to determine any relationship between complications and patient variables (e.g. gestational age, medication administration) due to the small sample size (Table 4).
Discussion
This study provides an overview of medical TOP provision at a large maternity hospital over a 4-year period since inception of the Irish TOP service. A review of this nature is particularly important due to the short period between legislation approval (December 2018), service development, and service implementation (January 2019). Internationally, the Irish service is unique in that 90% of terminations are community based; therefore, this study provides a unique insight into an integrated model of termination care.
In this study, inpatient medical TOPs were provided to 149 individuals, and the primary indication for referral to a secondary care setting was gestation greater than or equal to 10 weeks’. There were variations in consultant versus NCHDs involvement, and practice, specifically with respect to timing of medication administration. A small, number of complications were observed, providing insight into areas for improvement.
More than 44% of the hospital-based cohort had a gestation greater than 11 + 0 weeks’; thus, highlighting the importance of timely access to care and the limitations placed by the mandatory 3-day waiting period in the context of the strict 12 + 0 week's gestation cut-off (National Women and Infants Health Programme, 2023). Recent work both in Ireland and internationally has identified the negative impact this restriction has on individuals, who carry the burden of wait times, miscalculation of gestation, and failed procedures (Center for Reproductive Rights, 2021; Conlon et al., 2022; Joyce et al., 2009; Rowlands, 2015). Mandatory wait periods have been shown to directly result in delays, which further supports the Irish National Women's Council and World Health Organisation's recommendation that the enforced waiting period be removed to ensure timely access to terminations (Kennedy, 2021; Rowlands and Thomas, 2020; World Health Organization, 2003).
The geographical inequality in TOP service provision in Ireland is another challenge faced by individuals in accessing care at an earlier gestation. One in four of our cohort had to travel outside of their county of residency as TOP services were not available to them locally. It is well established that proximity directly influences access to TOPs, and that individuals that have to travel have TOPs at later gestational ages (Doran and Nancarrow, 2015; Sethna and Doull, 2007). This places an avoidable burden on individuals and has been shown to disproportionately affect marginalised communities (Sethna and Doull, 2007). To address this disparity, service provision continues to be expanded and by January 2024 17 of the 19 maternity units in Ireland will offer termination care (Department of Health, 2023). Additionally, a blended model of care integrating remote consultations, which was temporarily implemented during the COVID-19 pandemic, has been approved as permanent. This will allow individuals seeking a TOP to opt for one of the two mandatory consultations to be conducted over the phone or virtually (O’Regan, 2023). In order to further eliminate geographical barriers to care and support individual autonomy, consideration can also be made to providing community medical TOPs between 10 and 12 weeks’ gestation as is recommended by the World Health Organization and is established in other countries (Director-General Health and Social Care, 2020; World Health Organization, 2022). However, limitations when applying this model of care to the Irish setting apply due to the strict 12 week gestation cut-off, which could leave individuals without further treatment options in the event of an unsuccessful community TOP in this crucial time frame. Additionally, the safety and the individual's seeking a TOP's perspective regarding acceptability of this has yet to be evaluated in Ireland and is an area for potential future research.
Within the current Irish termination service infrastructure, a limited portion of healthcare professionals participate in service provision raising concerns regarding the sustainability of the service (Donnelly and Murray, 2020; O'Shaughnessy et al., 2021). Our study found that service provision is primarily consultant-led with limited participation from doctors in training. While the legislation accepts conscientious objection (Goverment of Ireland, 2018), limited exposure to termination care has been found to perpetuate both staffing issues and a knowledge gap due to a lack of clinical experience (Leitao et al., 2022). This is also highlighted by the NICE 2019 Guideline on ‘Abortion Care’, which emphasised the importance of integrating practical exposure to TOP in the core curriculum of healthcare providers to support the sustainability of termination services (O'Shea et al., 2020). Efforts must also be made to create a national TOP curriculum across Irish medical schools, which at present is lacking, to ensure standardization of TOP education and thus subsequent knowledge among clinicians. Lastly, when addressing the sustainability of the service, consideration is to be made to integrating midwifery and nurse-led care, which has been shown to be safe, effective, and associated with greater satisfaction from individuals seeking TOPs (World Health Organization, 2022).
The variation in care provided with respect to medication administration demonstrates the need to standardise care within the newly established service. Of the cohort, 25% did not receive misoprostol within 24 to 48 h from mifepristone administration as per the clinical guidelines, and 4.1% did not receive the correct misoprostol loading dose (Institute of Obstetricians & Gynaecologists, 2018). This may have contributed to the discrepancy in efficacy observed; the published efficacy rate following one round of the medical TOP regime is 98% (Gatter et al., 2015); however, we noted that 9.4% of our cohort required supplemental doses of misoprostol upon completion of one round of the medical regime (i.e. up to five doses). In response, clinical pathways have been created with set days of admission to ensure appropriate staffing and early ward admission times to ensure bed availability, and clinical care algorithms were established to ensure a consistent approach to management. The use of clinical pathways has been shown to reduce variation in protocol implementation and has been identified as a crucial element in quality improvement (Lavelle et al., 2015; Panella et al., 2003). This was further evident by the increase in the provision of contraception following the implementation of clinical pathways, which included designated TOP midwife coordinators and a clinical lead, in addition to the launch of a nationally funded long acting contraception scheme (Department of Health, 2022a).
The low complication rates observed are in keeping with the international literature that shows that early medical TOPs are safe and complications are infrequent (Chen and Creinin, 2015; Kruse et al., 2000). Haemorrhage requiring blood transfusion was the most significant complication seen in our cohort. Studies in developed countries have shown that haemorrhage requiring surgical management or blood transfusion is a rare complication of early medical TOPs, and the risk increases with advanced gestation (>49 days) (Kruse et al., 2000; McKinley et al., 1993). Furthermore, the requirement for individuals between 10 and 12 week's gestation to be inpatients until delivery allows for the identification and swift management of complications such as unsuccessful and incomplete TOPs, which in Ireland carry a significant burden on the individual due to the strict legal gestation cut-off. Insight into this is provided by the additional interventions required to complete the TOP in this study; however, it is difficult to ascertain whether these interventions were required or occurred as a result of over treatment in the medical setting, and thus further research is needed. Lastly, the number of unplanned medical reviews following discharge provides insight into minor complications such as mild endometritis as reviews were primarily due to concerns regarding infection and/or bleeding secondary to same. However, further research is needed to further evaluate minor complications including those that are conservatively managed.
This is the first study to report on the complications of early inpatient medical TOPs in Ireland. The current data reflect a single unit's experience and highlights the need for standardised and systematic data collection on a national level for adequate and deeper understanding of TOP service provision, ensuring its sustainability and continuous improvement towards best recommended practice.
Conclusion
Medical TOPs before 12 weeks’ gestation conducted in the hospital setting are both efficient and safe. This 4-year study is the first reported review of the efficacy and complication rates of the newly established service. We advocate for policy reform to remove the 3-day waiting period, expansion of the TOP services to provide care to rural communities, and additional training to ensure a sustainable service.
Flow chart depicting final cohort numbers. Abbreviations: MTOP: Medical Termination of Pregnancy, STOP: Surgical Termination of Pregnancy.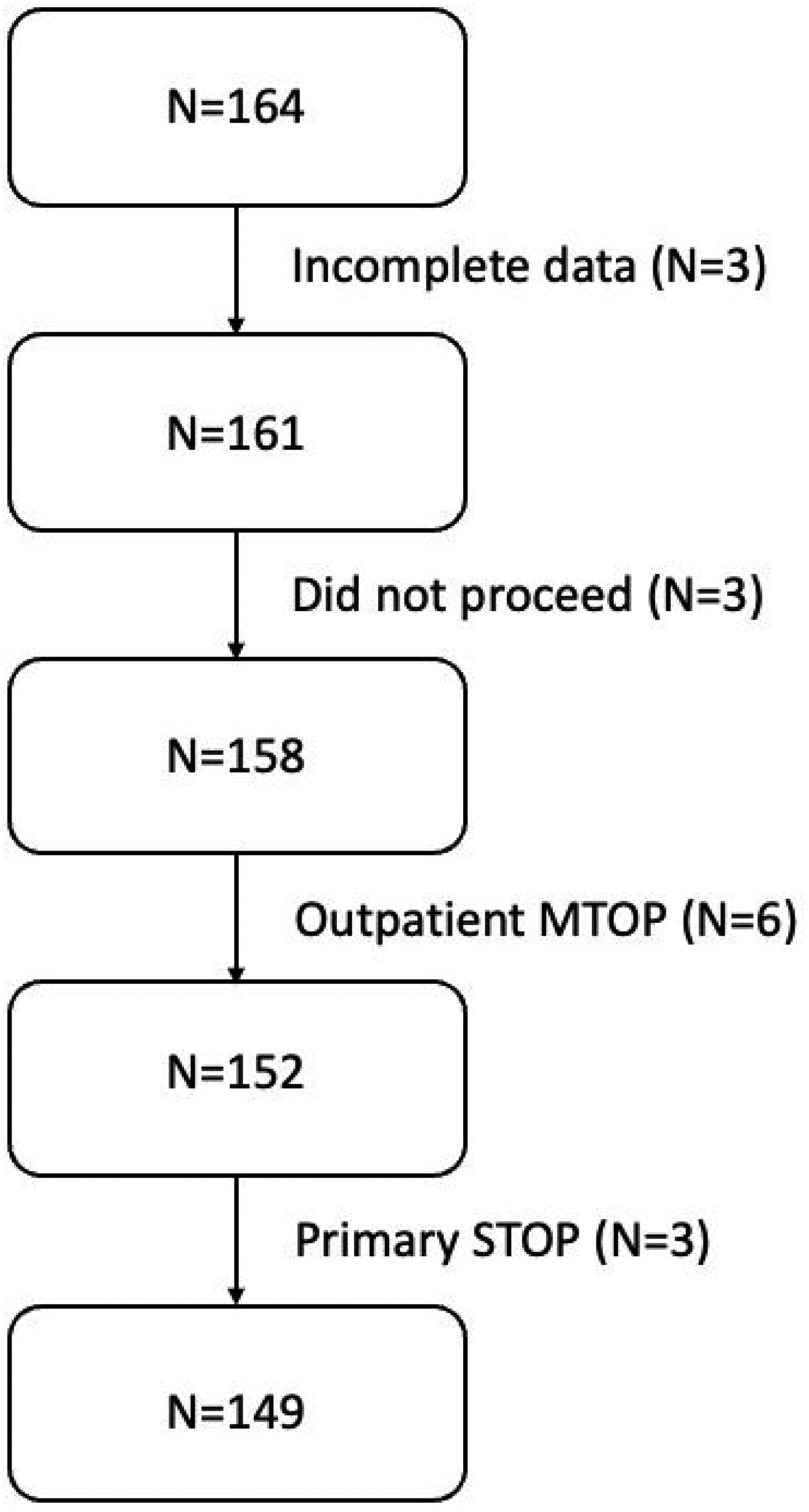
Footnotes
Acknowledgements
This work has been presented at the 17th European Society of Contraception and Reproductive Health Congress, the Cork University Maternity Hospital Audit Day, and the National Perinatal Epidemiology Centre Research Day.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.