
Abstract
Pregnancy loss prior to fetal viability is a common experience for women worldwide – 1 in 4 pregnancies end in miscarriage. Increased recognition of the impact of such loss has put the issue of statutory leave in this context on the policy and legislative agenda in an increasing number of jurisdictions. This article seeks to help inform these debates by presenting the findings of a comparative study of jurisdictions which have introduced such leave. From this, the article identifies two main approaches: leave based on the sick leave model and leave based on the compassionate leave model. The article argues that both models have strengths and limitations. What works in each individual jurisdiction will depend, among other factors, on the way in which the jurisdiction in question addresses the issue of leave more broadly. However, regardless of the model adopted, the article argues that some form of statutory leave for miscarriage and other pregnancy loss should be introduced on the basis that such leave serves to reinforce the equality agenda, provides a chance for care and recovery following pregnancy loss, and serves an important expressive and educative goal in ensuring better understanding of the impact of pregnancy loss on those who experience such loss.
Keywords
Introduction
Pregnancy loss prior to fetal viability (referred to in this article as early pregnancy loss) is a common experience for women worldwide. While many jurisdictions make provision for statutory leave where the pregnancy loss takes place during the later stages of pregnancy, such leave is less common where pregnancy ends pre-viability. This means that women who need to take leave in such situations have to fall back on sick leave, insofar as this leave is available in their jurisdiction. This issue has received relatively limited attention, partly because it falls between employment law and health law and partly because, despite the prevalence of early miscarriage, there is a lack of discussion of miscarriage in the public domain. 1 Its incidence and associated factors are poorly understood by general populations2,3 and pre-viability pregnancy loss/early pregnancy loss has traditionally been rendered invisible and its consequences ignored. 4
Recently, however, there has been greater recognition of the impact of early pregnancy loss. 5 As part of this, some employers now offer employees an entitlement to leave following early pregnancy loss. 6 More attention is also being paid to the possibility of introducing statutory leave following such pregnancy loss. 7 At the time of writing, jurisdictions considering the introduction of statutory leave include Canada; 8 England, Wales and Scotland; 9 Ireland; 10 Northern Ireland; 11 and Gibraltar; 12 as well as states and provinces including Alberta,13,14 Nova Scotia, 15 Catalunya, 16 and Oregon. 17 Other jurisdictions, including Australia and New Zealand, have recently introduced statutory leave. This article provides a comparative analysis of existing statutory leave for early pregnancy loss in high income countries 18 and identifies some of the common questions that arise in providing for leave in this situation.
To do this, the article begins in Part I by placing this kind of statutory leave in context - exploring the impact of early pregnancy loss on women and their partners and looking in outline at the other forms of statutory leave which may be available following early pregnancy loss. It then presents the case for the introduction of specific leave for early pregnancy loss. In Part II, the article sets out the findings of a comparative study of statutory leave for early pregnancy loss in high-income countries. 19 This has two roles: first, it establishes where statutory leave provisions currently exist and secondly, it allows for an analysis of how the matter is addressed in the applicable legislation. The article identifies two broad approaches which can be taken to this kind of leave and presents the advantages and disadvantages of each.
Part I: Early pregnancy loss in context
This article is concerned with pregnancy loss prior to fetal viability and so we must begin by defining viability. While one might expect that the definition of viability would be uniform, there is in fact quite significant variation among jurisdictions. Moreover, in jurisdictions where the point of viability is legally defined, the legal definition may be different to the medical understanding of the term. 20 In ‘lay’ language, viability means the ability of the fetus to survive outside of the womb. 21 In medical terms, viability may be defined by gestational age and/or by fetal weight. 22 The World Health Organization uses a definition based on fetal weight, setting this at less than 500 grammes, which is broadly equivalent to 22 weeks’ gestation. 23 Definitions of viability based on gestational age range from 20 to 28 weeks of gestation, depending on the jurisdiction/geographical region. 24 In part, this variability reflects the fact that the point of viability changes as neonatal survival rates increase with improved technology. This can be illustrated by two examples from high-income countries. In the United States in 1989–90, the estimated survival rate for infants born at 23 weeks’ and 25 weeks’ gestation was 15% and 59% respectively, while by 2013–15, survival rates for the same stages of gestation were 49% and 88%, respectively. 25 In the Republic of Ireland, in 2014 the survival to discharge rates of infants born at 23 weeks and 25 weeks was 19% and 72%, respectively, 26 and in 2020, survival rates for the same gestational age were 25% and 78%, respectively. 27 Because in many jurisdictions fetal viability is a relevant factor in determining access to abortion, the variation may also reflect political or social factors. 28
A pre-viability pregnancy may come to an end for a number of reasons, including miscarriage, 29 ectopic 30 or molar 31 pregnancy, and termination of pregnancy. For the general population, the idea of early pregnancy loss is probably most frequently equated with first trimester miscarriage. It is estimated that globally approximately 23 million miscarriages occur every year and that the pooled risk of experiencing miscarriage is 15.3%. 32
Impact of early pregnancy loss
Regardless of the reason for the loss, early pregnancy loss has an impact on a range of people. This impact can be physical (for women), psychological and economic. Physical effects include bleeding and pelvic pain, which can continue for a number of days/weeks. Where there are complications, physical impacts can be significantly increased and can include hospital admission for management of miscarriage. Taking Ireland as an example, there were 50,538 hospitalisations for early miscarriage between 2005 to 2016. 33 In the same time period, a total of 12,098 women were hospitalised due to ectopic pregnancy. 34 More recent data from England records 33,352 inpatient admissions in respect of miscarriage, ectopic and molar pregnancies in 2021–22 (a slight increase on the previous year). 35 Management of miscarriage may involve a range of procedures, including surgical procedures such as D&C (dilation and curettage) to remove tissue (sometimes described as the retained products of conception) from the uterine wall. Recurrent miscarriage is also associated with long-term health problems, including increased risk of cardiovascular disease and venous thromboembolism. 36 Medical termination of pregnancy may result in cramp-like pain, heavy bleeding, or haemorrhage; while surgical termination of pregnancy could result in (rare) complications such as cervical injury, or infection. 37
Psychological impacts of pregnancy loss may vary depending on individual circumstances. Women and their partners will often experience immediate and intense feelings of grief and loss. 38 These feelings of grief may also be experienced by other family members, and in situations of surrogacy or planned adoption, grief can be experienced by the intended parents. There are also longer-term psychological impacts. A literature review published in the Lancet found clear evidence of an increased risk of depression, anxiety and suicide among women who had experienced a miscarriage. 39 Women may also experience post-traumatic stress disorder for a significant time following a miscarriage or ectopic pregnancy. 40
Finally, pregnancy loss may have an economic impact on the woman and possibly her partner, both in terms of associated medical or counselling costs and, depending on the conditions of employment, because of the need to take leave from work. There is also evidence that, even where women and their partners can take leave, this economic impact creates a pressure to return to work before feeling able to do so. 41
For some women and their partners, the impact of the miscarriage is exacerbated by the fact that miscarriage is poorly understood by both the general public and by healthcare providers. 42 These misconceptions can lead to self-blame and isolation for women and may also result in lack of understanding or sympathy in clinical healthcare providers. 43 In the Independent Review of Pregnancy Loss in England, the authors explain that, with early pregnancy loss, the usual pregnancy care pathway often disintegrates, leading to confusion, lack of information and choices. 44
Generalised statutory leave provision
Two forms of general statutory leave provision may be available to someone who has experienced early pregnancy loss. These existing forms of statutory leave also provide two models for the framing of leave following early pregnancy loss.
The first of these is sick leave, which is statutorily provided for in most jurisdictions worldwide. 45 Depending on the jurisdiction, sick leave entitlement may be paid or unpaid. In the United States, for example, the Family and Medical Leave Act 1993 (which applies only to employers with more than 50 employees) allows an employee who has a ‘serious health condition’ (which explicitly includes ‘[a]ny period of incapacity due to pregnancy, or for prenatal care’) to a period of leave of up to 12 weeks duration in every 12 months. 46 While the employee's job is statutorily protected during this leave, the leave itself is unpaid (unless the employer includes paid sick leave in the employee‘s work benefits package).
In Europe, the European Social Charter states that all workers and their dependents have the right to social security. 47 All Member States of the European Union allow for sick leave and provide some degree of compensation for income lost through social security benefits. However, because the operation of sick leave and social security benefit are within the competence of European Union Member States, there is quite significant variation across the Member States. 48 In most States, the period of the sick leave and the duration of sickness benefits are aligned (although some provide for additional unpaid sick leave). 49 The scope of payment/benefits available depends on two main factors: the person's employment status and the extent of their social security contributions.
Some categories of workers (state employees and, depending on their employment contracts, some other salaried employees) will have a period of entitlement to sick pay (i.e., payment by their employer). Depending on the arrangement, sick pay may be part or all of the worker's salary. These workers may also be entitled to sickness benefit if the worker's sick pay entitlement is not of sufficient duration. For other workers, the only source of compensation available to them will be sickness benefit. This will be calculated either as a fixed rate of previous earnings or as a flat-rate amount. 50 The position regarding workers who are self-employed varies, with some Member States requiring that self-employed workers take out compulsory insurance to cover this kind of situation and others making no provision in this respect. 51 For workers on hourly contracts, and workers in the ‘gig’ economy (i.e., workers whose pay is based on completion of tasks), both sick leave and sickness benefit may be limited or non-existent. The duration of both sick pay and sickness benefit varies substantially across Member States. In Ireland, for example, the legal minimum entitlement to paid sick leave is five days 52 while some other Member States provide for sick pay for up to two years. 53 The duration of sickness benefit also varies depending on the jurisdiction and on the social security contributions which the worker has made. 54 The second form of leave which is potentially available is sometimes described as compassionate leave and sometimes as bereavement leave. This kind of leave is statutorily provided for in some jurisdictions and even where this is not the case, some employers include this kind of leave in employees’ work benefits package. There is no EU mandate for compassionate leave, although this kind of leave might be seen as being in line with the EU Work-Life Balance Initiative, most recently given legal force in Directive 2019/1158 on work-life balance. 55 Where compassionate leave is statutorily provided for, the basis for the leave and its nature and duration vary substantially across jurisdictions. In Ireland, for example, there is no statutory entitlement to any bereavement leave. Other examples include France, 56 Spain, 57 Malta 58 and Portugal, 59 all of which provide varying degrees of statutory bereavement leave, with length of leave typically depending on the degree of relation to the deceased.
Both of these forms of leave (to the extent that they exist) may be available in respect of early pregnancy loss. Sick leave (and sickness benefit) will be available to someone experiencing the physical or psychological effects of early pregnancy loss (subject to medical certification). The above bereavement leave models do not include early pregnancy loss explicitly, and so such leave does not generally fit within the ambit of these schemes. However, as we will see in Part II, several jurisdictions have employed an expanded form of the bereavement leave model to provide for leave in these circumstances.
In countries without explicit pregnancy loss leave (at the time of investigation), some quantitative or mixed-methods studies have examined what type of leave participants did take following their early pregnancy loss. An Australian study 60 found that the most common types of leave taken (across pregnancy losses of all gestations) were compassionate/bereavement leave (62%), sick or carers’ leave (42%), and annual leave (19%). An Australian study on early pregnancy loss 61 found that women mostly took sick leave (39%) or annual leave (19%) following their loss. An Irish study 62 found that sick leave was most common (78%), followed by unpaid leave (15%) and annual leave (12%).
The case for specific leave following early pregnancy loss
In considering the case for specific leave, two aspects of this policy choice must be separated. The first is whether such leave should be provided and the second is where the cost of such leave should lie, and specifically, whether this should be borne by employers or through the social security system. We will look at each aspect in turn.
Although generalised sick leave is likely to be available to women in cases of early pregnancy loss, this has some limitations. Most significantly, where sick leave (and/or sick pay/sickness benefit) is limited in duration, women who use their sick leave to address early pregnancy loss will have less sick leave available for other forms of illness, or may have already used their sick leave entitlement prior to the early pregnancy loss. For some women, this will not be an issue either because they will not require sick leave for other reasons or because the statutory schemes in their jurisdiction are sufficiently generous. For some women, however, this will constitute a significant disadvantage. Other possible limitations of generalised sick leave include the need for medical certification which may limit availability (depending on the medical professional) and the fact that such leave does not apply to partners who may also be experiencing loss and grief.
An argument for specific leave following early pregnancy loss may be grounded in both equality and health and wellbeing norms. From an equality perspective, while not denying that the emotional impact of early pregnancy loss may be broader, such loss has a more direct and immediate impact on women and pregnant people. As identified above, even though women who experience early pregnancy loss may be able to utilise generalised sick leave, they are nonetheless placed in a disadvantaged position with respect to men. This therefore raises questions regarding equality and non-discrimination.
At an international level, the elimination of discrimination against women is a requirement under Art. 11(1) of the United Nations Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) 63 and the elimination of discrimination on a range of grounds, including sex, is a requirement under C111 of the International Labour Organization, 64 Art. 2 of which requires States Parties to ‘promote by means appropriate to national conditions and practice, equality of opportunity and treatment in respect of employment and occupation.’
Within Europe, the right of workers to ‘equal opportunities and equal treatment in matters of employment without discrimination on the grounds of sex’ is protected under the European Social Charter. 65 Additionally, in the European Union, equality and non-discrimination are recognised as foundational values, protected by the Treaty on the European Union, 66 the Treaty on the Functioning of the European Union 67 and the Charter of Fundamental Rights of the European Union. 68 An extensive legislative programme has been adopted to deliver on these values. Of particular relevance to the discussion here is the Equal Treatment Directive as it applies to working conditions, including pay. 69 It is arguable that the loss of the sick leave entitlements which have been used up because of having to take leave for early pregnancy loss constitutes discrimination under the Directive. 70 However, in the absence of a ruling by the Court of Justice of the European Union, this cannot be assumed, and so legislative provision for leave is required to provide the necessary certainty.
From a health and well-being perspective, we are now seeing greater recognition of the physical and emotional impact of early pregnancy loss, including in the workplace. Although studies are still limited,
71
a scoping review conducted by Meunier et al concluded that it was ‘reasonable to assume that the reasons for returning to work will significantly affect the experience of a person returning to work’. They continue: Thus, their experience will be different depending on whether they return to work because they want to resume their professional responsibilities or because they feel under pressure, guilty, judged, or potentially penalized, in financial terms or in terms of career advancement.
72
If the arguments in favour of early pregnancy loss leave are accepted, the question then arises as to who should fund such leave: the employer or the state through social security benefits? This question is beyond the scope of this article, although we suggest that the appropriate answer will depend, among other factors, on the ways in which costs are borne in respect of other forms of employment-related leave, including maternity leave. A relevant factor in this regard may be the need to ensure that employers are not burdened with the costs of the leave such that they respond by conscious or unconscious discrimination in hiring women. 76
Part II: Legislating for early pregnancy loss leave
The comparative study of statutory leave for early pregnancy loss was conducted in two stages. In the first stage, we sought to establish how many high-income jurisdictions make provision for this kind of leave and then we engaged in a close analysis of the relevant measures that exist.
Stage 1
At stage 1, we focused on the 81 high-income countries 77 as identified by the World Bank. The lead author undertook extensive internet searches including government information websites, international reports on maternity and related leave, and original legislation. Search terms included ‘miscarriage’ ‘maternity’ ‘leave’ etc., and the name of the country. Where multiple sources of information were available for each country, these were cross-referenced to ensure accuracy of information. These searches were conducted between October and December 2022. Information was available for 80 78 of 81 countries included in the World Bank high-income country list (accessed October 2022).
Through this process, countries were identified as providing statutory leave in the case of pregnancy loss before the point at which viability is defined in that country (if such a definition existed). It was found that nine countries categorised as high-income provide statutory leave in the case of pregnancy loss before viability: Australia, 79 Iceland, Macau, New Zealand, Panama, Portugal, Puerto Rico, South Korea, Taiwan and the Canadian province of Québec. While the study was focused on high-income countries, the study also identified several low-middle income countries which appear to make provision for leave for early pregnancy loss. These countries are: Brazil, Columbia, China, India, Indonesia, Nicaragua, Mauritius, the Philippines, and Vietnam. Given the limits of the study, we were unable to subject these countries to further analysis.
Stage 2
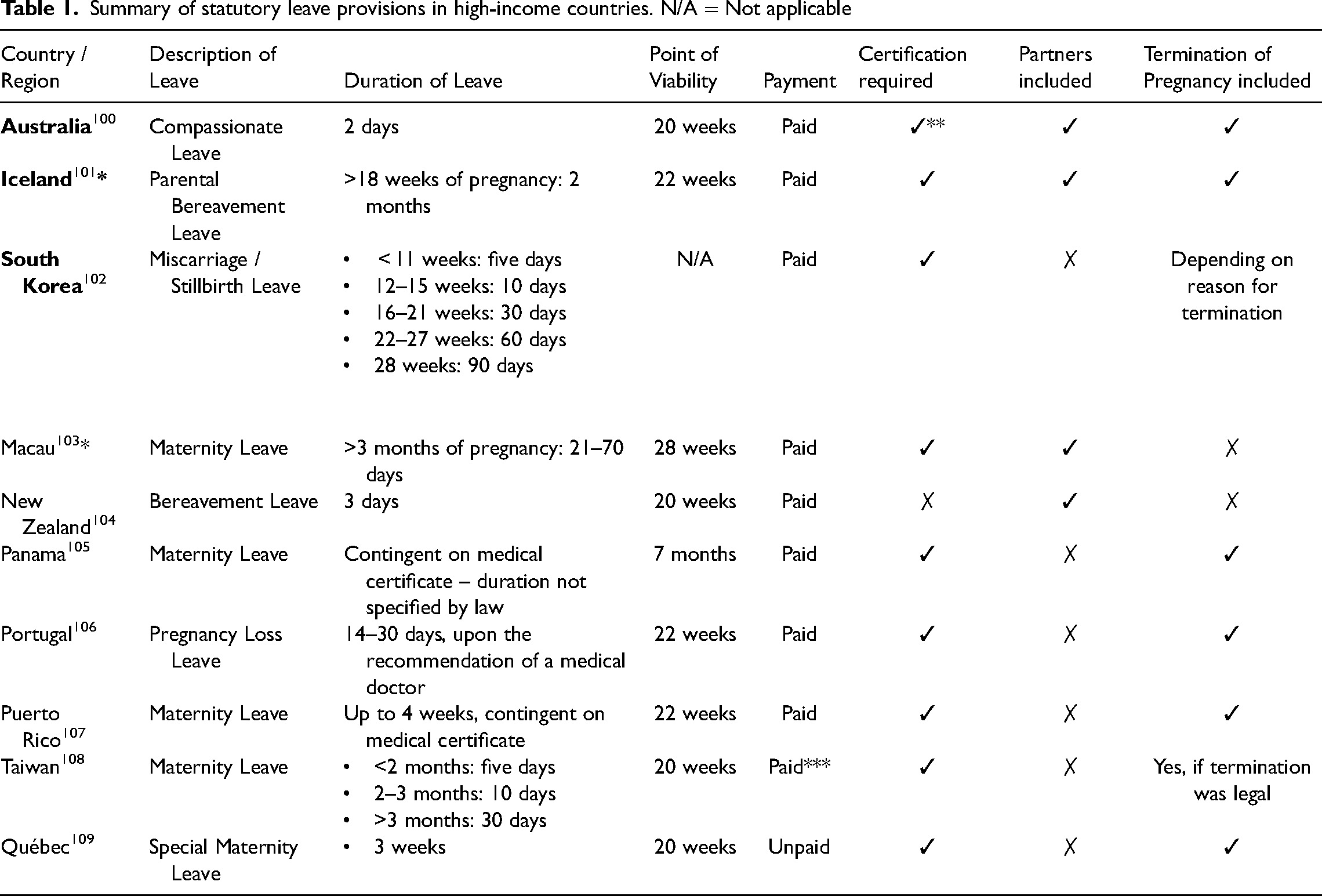
Having established the high-income countries which had applicable legislation, we then sourced this legislation and analysed it on the basis of the following criteria: description of the type of leave (e.g., bereavement leave, miscarriage leave); length of leave; eligibility requirements for taking this leave; and whether this leave was paid or unpaid. In addition to a textual analysis, key informants were sourced and contacted to verify findings and share information about legislation in their country that was not available online. Typically, these key informants included those working in the target country and specialising in obstetrics/midwifery, research in pregnancy loss, or workers’ rights. The findings of Stage 2 are summarised in Table 1.
Summary of statutory leave provisions in high-income countries. N/A = Not applicable
Summary of statutory leave provisions in high-income countries. N/A = Not applicable
While all the jurisdictions identified above provide some form of statutory leave for early pregnancy loss, there is considerable variation both as regards the length of leave and the requirements to be met before such leave is allowed. In almost all jurisdictions analysed the statutory leave is paid, usually by employers. In broad terms, jurisdictions approach the statutory leave in one of two ways: the first reflects the compassionate/bereavement leave model, while the second reflects the sick leave model.
Australia and New Zealand provide examples of the first approach. Both jurisdictions already had an established statutory right to bereavement leave, and so it was relatively straightforward to fit leave following early pregnancy loss into this framework. In Australia, the Sex Discrimination and Fair Work (Respect at Work) Act 2021 amended the Fair Work Act 2009 to extend the entitlement to compassionate leave to include an entitlement to leave following a miscarriage. 80 The leave in question is for two days and it is available to both the woman and her spouse or de facto partner. The leave is paid by the employer at the employee's base pay rate except for ‘casual employees’ 81 who are entitled only to unpaid leave. 82 Miscarriage is defined to mean a ‘spontaneous loss of an embryo or fetus before a period of gestation of 20 weeks’. 83 Thus, the leave is not available in situations of termination of pregnancy. To access the leave, an employee must give notice to their employer as soon as is practicable and must advise of the expected duration of the leave. 84 If required to do so by the employer, the employee must also provide evidence that would satisfy a reasonable person of the cause for the leave (in this case the miscarriage). 85
The New Zealand legislation adopts a broadly similar format although there are some noteworthy differences of detail. The Holidays (Bereavement Leave for Miscarriage) Amendment Act 2021 extends the entitlement to bereavement leave under the Holidays Act 2003 to include situations of miscarriage and stillbirth. 86 ‘Miscarriage’ is defined as ‘the end of a pregnancy in the first 20 weeks of pregnancy other than as a result of abortion services provided in accordance with the Contraception, Sterilisation and Abortion Act 1997’. 87 The duration of the leave is three days and it is paid by the employer at a rate equivalent to the employee's relevant daily pay or average daily pay. 88 The leave may be available to all employees who have completed six months current continuous employment with the employer. 89 The leave entitlement applies to the woman; to her spouse or partner; and to a former spouse or partner who would have been the biological parent of the child; as well as to someone who has undertaken to be the primary carer of the child and their spouse or partner. 90 To access the leave, the employee must inform their employer of their intention to take the leave as early as possible. 91 However, unlike the position in Australia, the employer does not have an entitlement to require the provision of evidence of the reason for the leave.
This model of leave primarily addresses the emotional impact of early pregnancy loss. In so doing, it adopts a relational approach, with the New Zealand legislation in particular recognising that the experience of grief is not just felt by the woman who has directly experienced the loss. A key strength of the model is its accessibility; the fact of the miscarriage is sufficient to ground the entitlement to leave. However, there are limits to this approach. The most obvious is the duration of the leave, which is likely to leave most women who experience an early pregnancy loss having to rely at least in part on sick leave. The other limit is the blanket omission, in both jurisdictions, of women who have had terminations. This seems to presume that women who have terminated a pregnancy do not experience grief or loss. Yet, there is strong evidence that for some women (and their partners), termination of pregnancy is a source of loss and grief.92,93 The omission of termination from the legislation serves to reinforce abortion stigma which in turn has been shown to increase feelings of post-abortion grief.94, 95 Furthermore, some women experiencing spontaneous miscarriage do not experience emotional or psychological impacts, just the physical effects of the loss.
The second model of leave is more focused on the physical impact of pregnancy loss and operates in a similar way to sick leave. Under this model, leave is typically available only to the woman who has directly experienced the pregnancy loss and the leave requires medical certification. Taiwan and South Korea provide broadly similar examples of this kind of leave. In Taiwan, for example, the woman is entitled to five days’ leave if the pregnancy loss occurs in the first two months of gestation; one week of leave if the loss occurs between two and three months; and four weeks’ leave if the pregnancy loss takes place between three months and 20 weeks. 96 However, employees are entitled to paid leave (which is financed by employers) only if the pregnancy loss takes place after three months. If the pregnancy loss takes place before three months, the employee has to fall back on their pay entitlements under sick leave. This leave entitlement also arises where the pregnancy has been terminated, although termination of pregnancy in Taiwan is lawful in only a limited range of circumstances. 97
Another version of this kind of leave, which applies in Portugal, Panama and Puerto Rico, allows for potentially longer leave for the woman, but this is entirely dependent on medical evaluation of need. The Panama Labour Code allows for leave for pregnancy loss, but leaves the length of the leave to be determined by the medical professional based on the employee's needs. 98 The Puerto Rican Labour Code is more restrictive. Under this, an employee who has a miscarriage or termination which produces the same medical effects as childbirth is entitled to a period of leave which may extend up to eight weeks. 99 The evaluation of whether the pregnancy loss meets this criterion must be made by a medical professional.
Although the sick leave model tends to focus more on pregnancy loss as a physical occurrence, in most jurisdictions where it operates, the leave also allows some time for emotional recovery and expresses a societal recognition of the impact of pregnancy loss. Its most obvious limitation is that it fails to recognise that the emotional consequences of pregnancy can extend beyond the woman. In some iterations, this approach is also heavily dependent on authorisation by medical professionals and, as the Lancet Review recognised, there is still quite considerable lack of understanding of the impact of early pregnancy loss among medical professionals.
Conclusion
Increased recognition of the impact of early pregnancy loss has put the issue of statutory leave in this context on the policy and legislative agenda in an increasing number of jurisdictions. This article has argued in favour of the introduction of statutory leave, leaving open the question of whether such leave should be funded by employers or by the state. It has sought to help inform these debates by presenting the findings of a comparative study of jurisdictions which have introduced such leave. While there is a range of options, most can be broadly categorised as fitting within either a compassionate/bereavement leave model or a sick leave model. Both models have strengths and limitations. What works in each individual jurisdiction will depend, among other factors, on the way in which the jurisdiction in question addresses leave more broadly. Thus, a jurisdiction which already makes statutory provision for compassionate/bereavement leave may choose to include leave after pregnancy loss within this broader leave entitlement. A benefit of this approach is that it easily facilitates a relational approach recognising that the impact of early pregnancy loss may be wider than the effects experienced by the pregnant woman. For other jurisdictions, such pregnancy loss leave may fit more comfortably within sick leave entitlements. However, regardless of the nature of the leave, we suggest that the introduction of statutory leave for early pregnancy loss serves to reinforce the equality agenda, provides a chance for care and recovery following early pregnancy loss, and serves an important expressive and educative goal in ensuring better understanding of the impact on those who experience such loss.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the following key informants: Samantha Payne, CEO, Pink Elephants Network (Australia); Professor Francine de Montigny, Professor of Nursing and Family Sciences, University of Québec in Outaouais, (Québec); Leó Örn Þorleifsson, Director of Rights and Entitlements at the Directorate of Labour (Iceland); Representative from Labour Affairs Bureau (Macao); Robin Cronin, Research Midwife Specialist, University of Auckland (New Zealand); Mario A. Rognoni H., Associate Lawyer, Arosemena Noriega & Contreras (Panama); Judicial Assistant, Representative of the Judicial Council (Portugal); Mariela Rexach, Federal Litigator, Littler, San Juan (Puerto Rico); Eunkyung Shin, Director of Ministry of Health and Welfare (South Korea); Pei-Yuen Tsai, Associate Professor, Graduate Institute of Social Work (Taiwan)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was funded by the Department of Children, Equality, Disability, Integration and Youth, Ireland.